
Abstract
Background:
Clavicle fractures are common injuries in professional football. Surgical fixation of these injuries may lead to decreased nonunion rates, improved shoulder strength, and decreased residual functional impairment.
Purpose:
To determine (1) return-to-sport (RTS) rate in National Football League (NFL) players after clavicle fracture open reduction and internal fixation (ORIF), (2) postoperative career length and games per season, (3) pre- and postoperative performance, and (4) postoperative performance compared with control players matched by position, age, years of experience, and performance.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Publicly available records were used to identify players who underwent surgical treatment of a clavicle fracture while playing in the NFL. Demographic and performance data were collected for each player, and matched controls were identified. Control and case performance scores were calculated using a standardized scoring system. RTS was defined as playing in 1 NFL game after surgery. Comparisons between case and control groups at preoperative and postoperative time points were made using paired-samples Student t tests.
Results:
Seventeen surgeries (16 players) were analyzed. Fifteen players (94.1%) were able to RTS in the NFL at a mean 211.3 ± 144.7 days postsurgery; 7 (44%) returned within the same season as their injury and subsequent fixation. The overall rate of a player’s remaining in the NFL 1 year after surgery was 88.2%. Players who underwent surgery played in a similar number of games per season and had similar career lengths in the NFL as controls (P > .05). There were no significant (P > .05) differences between cases and matched controls presurgery and preindex. There was no difference (P > .05) in postoperative performance scores or games per season compared with preoperative scores or games per season for any position. Quarterbacks (n = 3, P = .049) and running backs (n = 5, P = .039) had significantly worse postoperative performance scores when compared with postindex matched controls.
Conclusion:
There is a high rate of RTS in the NFL after clavicle fracture ORIF. Players who underwent clavicle fracture ORIF played in a similar number of games per season and had similar career lengths in the NFL as controls. Quarterbacks and running backs had significantly worse postoperative performance scores when compared with postindex matched controls.
Keywords
Clavicle fractures are one of the most common upper extremity injuries in both contact and noncontact sports. 9 These injuries are a source of significant morbidity, accounting for up to 10% of all sports-related fractures. 19 Because of these factors, clavicle fractures are an important area for research in orthopaedics.
Clavicle fractures most commonly result from a fall onto the ipsilateral shoulder, making athletes prone to this injury. 21 The clavicle is prone to fractures as it is the only loadbearing bone that stabilizes the shoulder girdle. 17 The clavicle connects the axial skeleton to the upper extremity, contributes to the motion and stability of the upper extremity, and provides protection to the underlying neurovascular structures.
Most clavicle fractures are located in the midshaft (81%). Lateral (17%) and medial (2%) fractures are seen less frequently. 5,15,17,20 Closed clavicle fractures have historically been treated nonsurgically in the general population and in the National Football League (NFL), with low rates of nonunion and symptomatic malunion. 7,13 However, more recent studies have demonstrated the results of nonoperative treatment to be inferior with nonunion rates ranging from 15% to 20%, loss of shoulder strength ranging from 18% to 33%, and the presence of residual functional impairment 6 months after injury in up to 42% of patients. 7,11,16
Various orthopaedic procedures, such as ankle fracture open reduction and internal fixation (ORIF), Achilles tendon repair, and patellar tendon repair, can have a negative effect on postoperative performance, return to sport (RTS), and length of career in the NFL. 2,10 NFL players undergoing forearm fracture ORIF, ankle fracture ORIF, and tibial intramedullary nailing have wide-ranging RTS, at 96.3%, 78.6%, and 90.9%, respectively. 10 However, the RTS and postoperative performance after clavicle ORIF in NFL athletes has not been well established. Given the increasing revenue and popularity of the NFL, it is important to understand surgical outcomes in this patient population. This information could be valuable for both players and front office personnel in establishing realistic RTS goals and planning for career length and postoperative performance.
The purpose of this study was to determine (1) RTS rate in NFL players after clavicle fracture ORIF, (2) postoperative career length and games per season, (3) pre- versus postoperative performance, and (4) postoperative performance compared with control players matched by position, age, years of experience, and performance. We hypothesized that NFL players who underwent clavicle fracture ORIF would have (1) a greater than 90% RTS rate, (2) no significant difference in postoperative career length and games per season compared to matched controls, (3) no significant difference in postoperative performance compared with preoperative, and (4) no significant performance difference postoperatively when compared with matched controls.
Methods
Players in the NFL who sustained a clavicle fracture and underwent ORIF between August 2003 and December 2015 were evaluated (Figure 1). These players were identified through NFL team websites, publicly available Internet-based injury reports, player profiles and biographies, and press releases. The search was manually conducted by 2 orthopaedic surgery residents. Searches were performed for all NFL teams and players.

Flowchart illustrating application of exclusion criteria.
Information for all players identified was included in this study as it related to RTS rate. A player was deemed to have RTS if he played in any single NFL game after surgery. A player did not RTS if he did not play in any NFL game after surgery. Inclusion criteria were any NFL athlete on an active roster in the NFL prior to clavicle fracture. Players were included if they were found to have clavicle fracture ORIF as reported by at least 2 separate sources. Athletes who were injured and underwent procedures before completing their first NFL regular season were excluded. Players who sustained a clavicle fracture and underwent clavicle fracture ORIF in the 2015-2016 season were excluded from analysis because they had less than a 1-year opportunity to RTS. In addition, online reports that were conflicting, incomplete, or did not have a date of surgery were also excluded from the study (n = 0).
Demographic variables, including a player’s age, position, prior professional experience, and date of surgery, were recorded. Players were categorized by their positions, including quarterback (QB), running back (RB), tight end (TE), wide receiver (WR), offensive lineman (OL), defensive lineman (DL), linebacker (LB), defensive back (DB), kicker (K), or punter (P). Performance statistics were collected from www.pro-football-reference.com for each player identified before and after clavicle fracture ORIF (Table 1). Statistics were collected for regular season NFL games only, with preseason and playoff games excluded.
Variables Collected for Each Position

A control group was selected; 1 control player was selected per case player. Controls were matched to study cases based on position, age (±1 year), years of experience (±1 year), and performance data prior to the surgery date. Each control was given an index date (relative to career length), which matched the case player’s surgery date, to compare postoperative or postindex performance. For example, if a player underwent clavicle fracture ORIF 3 years into his career, the control’s index date was 3 years into his career.
Player statistics for cases pre- and postoperative and controls pre- and postindex were collected and aggregated. Each statistical category was divided by games played to account for discrepancies in number of games played per season. A player’s performance score was then calculated by using a previously published and standardized scoring system (Appendix) based on metrics important to the player’s specific position. 3,8,10 Statistics per game were used to calculate each performance score per game.
All players were included in RTS, games per season, and career length analysis. A Kaplan-Meier survivorship curve with “retirement” as the endpoint was constructed postoperatively for cases and postindex for controls. Positions without previously defined performance scores (punters, kickers, and offensive lineman) were excluded from performance score analysis. Comparisons between case and control groups and preoperative and postoperative time points were made using paired-samples Student t tests (in-silico; http://in-silico.net/tools/statistics/ttest), with significance set at P < .05.
Results
A total of 17 surgeries in 16 players were analyzed (Table 2). The mean age at surgery was 27.8 ± 3.9 years, and mean experience in the NFL at surgery was 5.2 ± 3.6 years. The running back position represented the largest proportion of players who underwent clavicle fracture ORIF, with 5 (29.4%) cases. One player fractured his contralateral clavicle within 6 months of initial surgery and RTS. He was counted as a single player (2 surgeries). Fifteen players after 16 surgeries (94.1%) were able to RTS in the NFL at an average of 211.3 ± 144.7 days. Seven of those players (44%) returned within the same season as their injury and subsequent fixation. The 1 player who did not RTS was released with an injury settlement after clavicle ORIF. During this same time frame (August 2003 to December 2015) there were 17 clavicle fractures in 17 players that were treated nonoperatively in the NFL.
Surgery and RTS Data by Position a
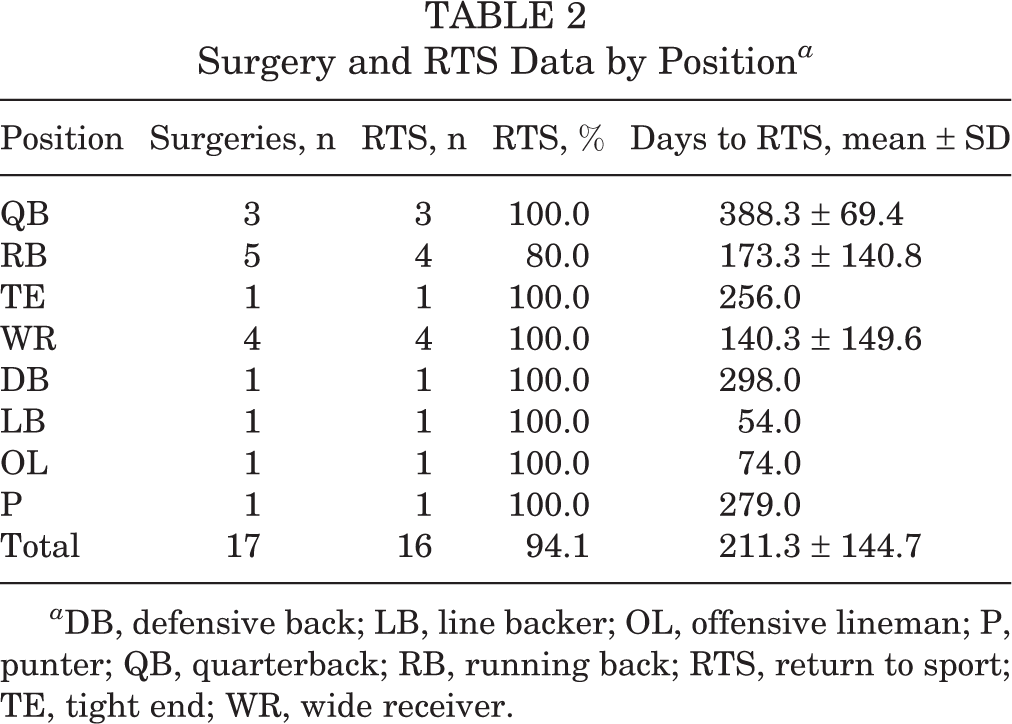
a DB, defensive back; LB, line backer; OL, offensive lineman; P, punter; QB, quarterback; RB, running back; RTS, return to sport; TE, tight end; WR, wide receiver.
One player (6.25%) returned to play in less than 6 weeks. An additional 5 players (31.25%) returned to play between 6 and 12 weeks, and the remaining 10 players (62.50%) returned after 12 weeks. Of the 10 players who RTS after 12 weeks, 70% were out of season when they were expected to return. The average RTS was 53.4 days for players who RTS during the same season.
The overall 1-year survival rate of players undergoing clavicle fracture ORIF was 88.2% (Figure 2). Players in the control group had similar career lengths in the NFL (3.0 ± 1.9 years) compared with players who underwent clavicle fracture ORIF (2.6 ± 1.4 years; P = .350) (Table 3). Players in the control group played in a similar number of games postindex (11.4 ± 3.9 games per season) compared with games postsurgery for those who underwent clavicle fracture ORIF (11.6 ± 4.4 games per season; P = .804). No players changed positions on RTS after clavicle fracture ORIF.
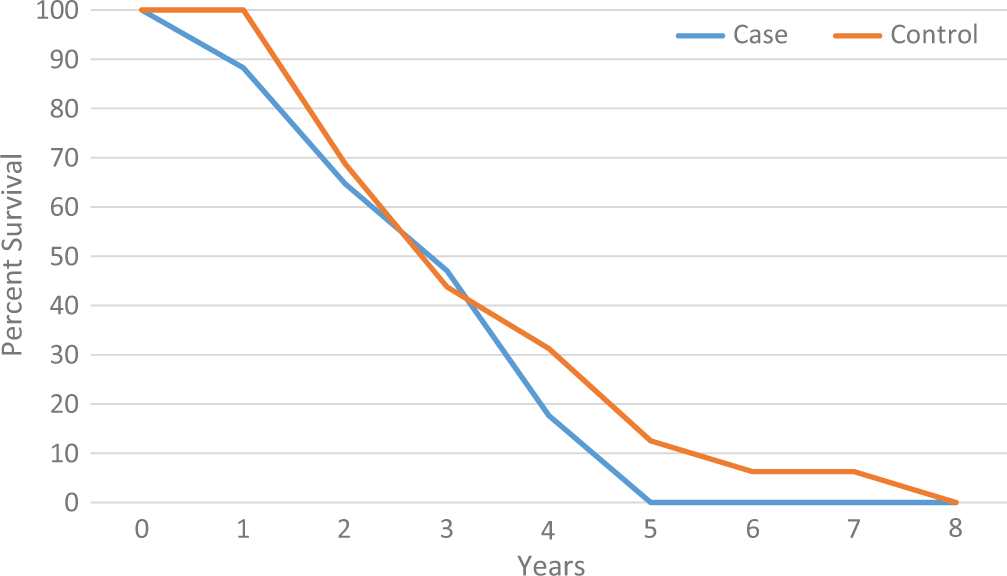
Kaplan-Meier survival analysis for cases and controls. Zero (0) signifies year of surgery for cases and index year for controls.
Games Per Season and Career Length Postsurgery and Postindex for Cases and Controls a

a DB, defensive back; LB, line backer; OL, offensive lineman; P, punter; QB, quarterback; RB, running back; TE, tight end; WR, wide receiver.
There were no statistically significant (P < .05) differences in demographic, performance, and games per season data between cases and matched controls presurgery and preindex (Tables 4–6). There was no significant difference in postoperative performance scores or postoperative games per season compared with preoperative for NFL players who underwent clavicle ORIF (Tables 7 and 8; Figure 3). Quarterbacks (P = .049) and running backs (P = .039) had significantly worse postoperative performance scores when compared with postindex matched controls (Table 9 and Figure 3).
Age and Experience for Each Position at Time of Surgery (for Cases) and Index Time (for Controls) a
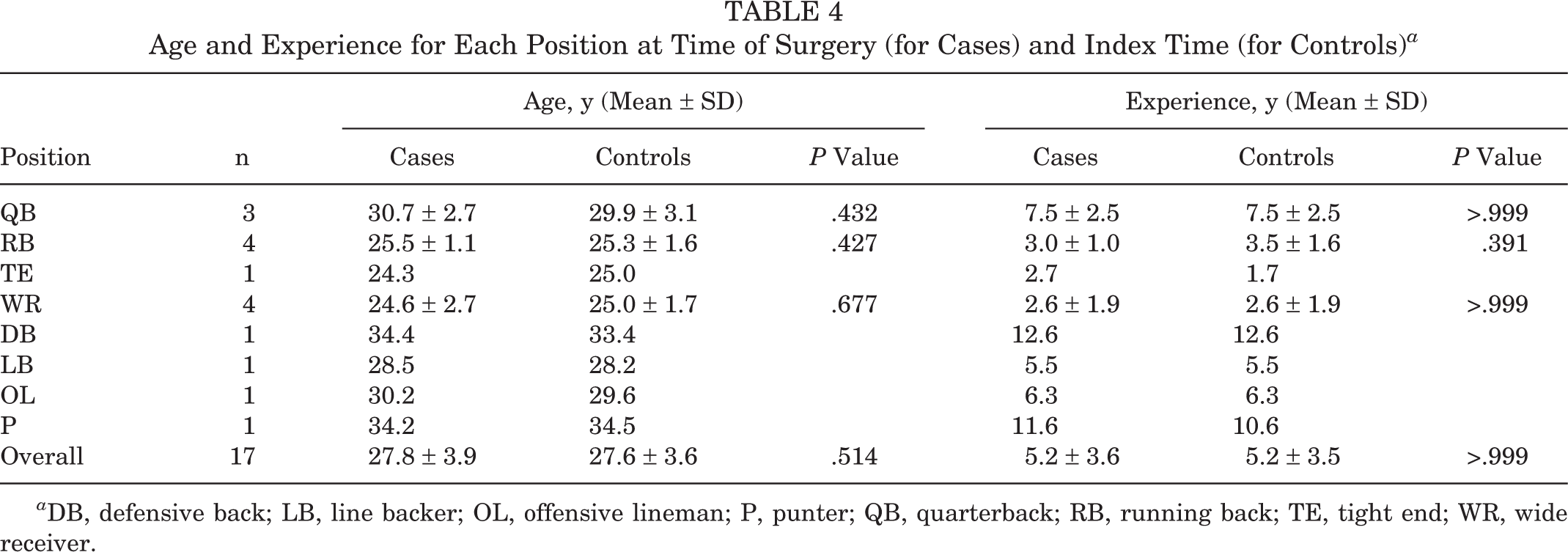
a DB, defensive back; LB, line backer; OL, offensive lineman; P, punter; QB, quarterback; RB, running back; TE, tight end; WR, wide receiver.
Preoperative and Preindex Performance Scores for Cases and Matched Controls a

a DB, defensive back; LB, line backer; OL, offensive lineman; P, punter; QB, quarterback; RB, running back; TE, tight end; WR, wide receiver.
Mean Games per Season Pre- and Postsurgery for Cases and Mean Games per Season Preindex for Controls a

a DB, defensive back; LB, line backer; OL, offensive lineman; P, punter; QB, quarterback; RB, running back; TE, tight end; WR, wide receiver.
b Student t test comparing case pre- and postsurgery games per season.
c Student t test comparing case presurgery and control preindex games per season.
Pre- and Postsurgery Performance Scores by Position for Cases and Postindex Performance Scores for Matched Controls a

a DB, defensive back; LB, line backer; QB, quarterback; RB, running back; TE, tight end; WR, wide receiver.
b Student t test comparing pre- and postsurgery performance scores.
c Student t test comparing postsurgery and postindex performance scores.
d Statistically significant difference (P < .05).
Listing of Case Players and Individual Performance Scores Pre- and Postsurgery a
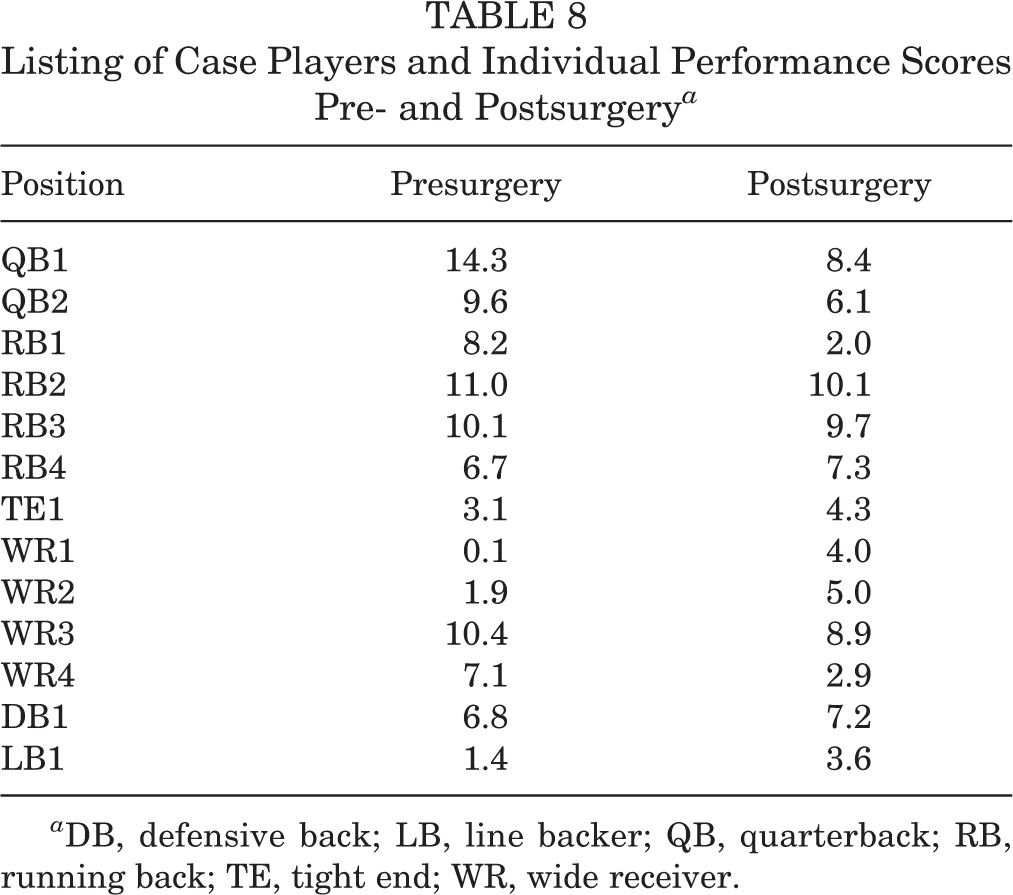
a DB, defensive back; LB, line backer; QB, quarterback; RB, running back; TE, tight end; WR, wide receiver.

Performance scores by position before and after surgery compared with controls pre- and postindex. ▪ = Significant difference between postsurgery and postindex performance scores. DB, defensive back; LB, line backer; QB, quarterback; RB, running back; TE, tight end; WR, wide receiver.
Postoperative and Postindex Performance Scores for Cases and Matched Controls a
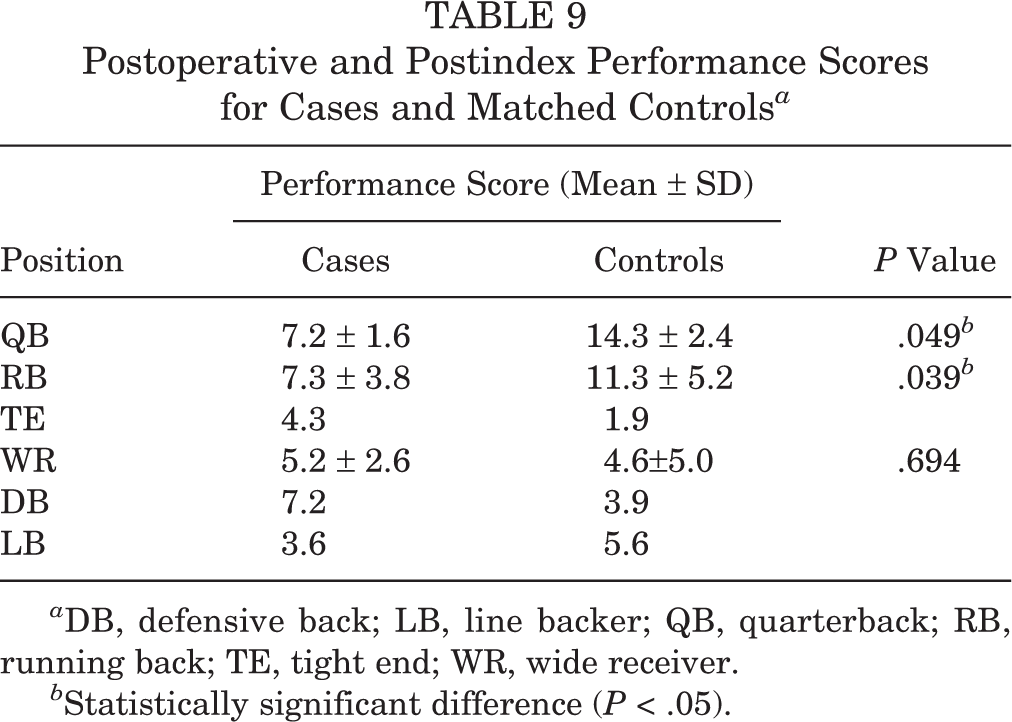
a DB, defensive back; LB, line backer; QB, quarterback; RB, running back; TE, tight end; WR, wide receiver.
b Statistically significant difference (P < .05).
Discussion
The purpose of this study was to determine (1) RTS rate in NFL players after clavicle fracture ORIF, (2) postoperative career length and games per season, (3) pre- versus postoperative performance, and (4) postoperative performance compared with control players matched by position, age, years of experience, and performance. We hypothesized that NFL players who underwent clavicle fracture ORIF would have (1) a greater than 90% RTS rate, (2) no significant difference in postoperative career length and games per season compared with matched controls, (3) no significant difference in postoperative performance compared with preoperative, and (4) no significant performance difference postoperatively when compared with matched controls.
The first study hypothesis was confirmed with a high (94.1%) RTS rate. The remaining hypotheses were partially confirmed in that the postoperative career length and postoperative games per season were not significantly different, no position had a significant difference in postoperative performance, and quarterbacks and running backs had significantly worse postoperative performance when compared to matched controls.
Two previous studies in recreational and amateur athletes demonstrated an RTS rate of 94% and 100% for players who underwent clavicle fracture ORIF. 12,18 The RTS rate from these prior studies is similar to the results of the present study, with an RTS rate of 94.1% in 16 NFL athletes. However, the study by Meisterling et al 12 had an average RTS of 83 days, and the study by Ranalletta et al 18 had an average RTS of 68 days. The RTS time from these studies was shorter than the results of the present study, with an average RTS of 211 days. The faster RTS was likely secondary to these studies, which included multiple sports in addition to football, where RTS is not as dependent on a fully united clavicle fracture as riding sports, soccer, and skiing. It is unknown in the present study when a player was “cleared” to RTS as opposed to when his first game was played postsurgery. Of the 10 players who RTS after 12 weeks, 70% were out of season when they were expected to return. Therefore, the mean RTS was likely higher than it would have been if the players were not in the offseason. This is also exaggerated by the short NFL season compared with other sports. The average RTS was 53 days for players who RTS during the same season.
Another study by Morgan et al 13 looked at the evolving management of clavicle fractures in NFL athletes. Of the 6 players treated with ORIF of their clavicle fracture, 50% were able to RTS within the same season. This is similar to the present study, in which 44% (7/16) of players returned within the same season as their injury and subsequent fixation.
These prior studies did not look at performance scores for specific position groups and did not compare the outcomes of clavicle fracture ORIF against matched controls. By using controls that were matched for age, NFL experience, and performance, the current study was able to improve performance data comparisons for case players against controls at the same junction of their career. By simply comparing a player with himself, rapid improvements (or regressions) in performance that are prevalent among similar players in the league may otherwise not be accounted for.
The offensive skill positions represented the largest proportion of players who underwent clavicle fracture ORIF, with 13 (81.3%). We hypothesize that the increased incidence of clavicle fractures within these position groups is likely due to getting tackled and driven into the ground onto the shoulder. On the contrary, defensive players are typically doing the tackling and are better able to control their bodies to avoid direct impact on the shoulder when they reach the ground.
Prior studies have also failed to comment on performance and RTS differences between position groups after clavicle fracture ORIF. There was no significant difference in performance between cases and matched controls presurgery and preindex. The wide receivers improved their performance scores postoperatively, as did their corresponding controls postindex. This finding indicates that clavicle fracture ORIF may not have a significant influence on the development and performance of these players.
On the other hand, the performance of quarterbacks and running backs decreased postoperatively, while performance of their corresponding controls improved postindex. This represented a performance score difference of 7.1 per game for quarterbacks and 4.0 per game for running backs. Extrapolated over a 16-game season, this would lead to a score difference of 113.6 and 64.0 for quarterbacks and running backs, respectively. Using the performance score, quarterbacks had 2000 fewer yards passing and 8 fewer passing touchdowns per season, and running backs had 400 fewer yards rushing and 4 fewer rushing touchdowns per season compared with matched controls. These are clearly both clinically and statistically significant results.
One possible explanation for the significant difference in performance for quarterbacks is the involvement of their dominant throwing arm (n = 3) leading to increased pain and decreased range of motion and negatively affecting their throwing mechanics. This may also contribute to the longer length of time for RTS, with quarterbacks needing an average of 388.3 days. Further studies are needed to assess the biomechanical effect of clavicle ORIF on throwing motion.
Limitations
There were limitations to this study. The use of publicly available data to identify clavicle fracture ORIF was prone to selection, reporting, and observer bias. However, this method of data acquisition has been used in multiple previous studies. 1,4,6,8,14 Additionally, the use of public data limits the ability to obtain the severity of the injury and the exact surgical procedure being performed. In this study, career length was not adjusted for “time missed” for players who underwent surgery. Their time in the league was in fact longer than reported; however, the number of seasons they spent playing (ie, career length) after surgery was accurate. Inherent to this type of study, there were multiple unknown confounding variables, such as presurgical course and no direct physical contact or medical records access to corroborate diagnosis. In addition, the specific fracture pattern, surgical approach, technique, and implant, among other surgical variables, could not be determined. Other limitations included the absence of patient-reported outcomes, the small number of participants, incomplete follow-up and career length for players still in the NFL, and inability to compare offensive linemen or specialists with performance scoring. Also, we were unable to compare clavicle fracture ORIF to nonoperative treatment of clavicle fracture in NFL athletes.
Conclusion
There was a high rate of RTS in the NFL after clavicle fracture ORIF. Players who underwent clavicle fracture ORIF played in a similar number games per season and had similar career lengths in the NFL as controls. Quarterbacks and running backs had significantly worse postoperative performance scores when compared with postindex matched controls.
Footnotes
Declaration of Conflicting Interests
One or more of the authors has declared the following potential conflict of interest or source of funding: P.C.M. is a paid presenter for Vericel and receives research support from DePuy and Arthrex. J.D.H. receives research support from DePuy Synthes and Smith & Nephew, is a paid consultant for NIA Magellan and Smith & Nephew, and receives publishing royalties from SLACK Inc.
Ethical approval was not sought for the present study.
Appendix Calculation of Player Performance Scores

| Position | Performance Score Formula |
|---|---|
| Quarterback | (Passing Yards ÷ 25) + (Passing Touchdowns × 4) + (Rushing Yards ÷ 10) + (Rushing Touchdowns × 6) |
| Running back/wide receiver/tight end | (Receiving Yards ÷ 10) + (Receiving Touchdowns × 6) + (Rushing Yards ÷ 10) + (Rushing Touchdowns × 6) |
| Defensive players | (Tackles) + (Assists ÷ 2) + (Sacks × 4) + (Passes Defended) + (Interceptions × 5) + (Interceptions/Fumbles Returned for Touchdowns × 6) + (Forced Fumbles × 3) + (Fumbles Recovered × 2) + (Safeties × 2) |