
Abstract
Background:
Idiopathic frozen shoulder (nontraumatic) is commonly encountered in patients between the ages of 35 and 60 years in general orthopaedic practice. While the prevalence of frozen shoulder among the general population is estimated to be between 2% and 4%, a significantly higher prevalence of 10% to 22% has been reported in patients with diabetes mellitus. Since diabetic patients are more prone to develop frozen shoulder than nondiabetics, the question arises as to whether patients diagnosed as having idiopathic frozen shoulder are at greater risk to develop diabetes mellitus and should be routinely screened for this condition.
Purpose:
To compare the prevalence of diabetes mellitus and prediabetes among patients diagnosed with idiopathic frozen shoulder who are not known to have either diabetes mellitus or prediabetic conditions with that of an age-matched group from the general population.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients at a shoulder clinic with a diagnosis of idiopathic frozen shoulder were asked to participate in the study if they were aged between 35 to 60 years and had no known previous diagnosis of diabetes mellitus or prediabetic conditions. These patients underwent a 2-hour oral glucose tolerance test. According to their fasting and 2-hour plasma glucose levels, patients were diagnosed as normal glucose tolerance, prediabetic, or diabetic. Findings were matched with the prevalence in an age-matched general population.
Results:
Fifty patients completed the test. Four patients with idiopathic frozen shoulder (8%) were found to be prediabetic. No patient was found to be diabetic. All 4 patients reported a history of diabetes in their parents or siblings.
Conclusion:
Patients diagnosed with idiopathic frozen shoulder who are 60 years or younger and are not known diabetics have a similar probability of having diabetes or prediabetes to an age-matched population. No routine diabetic workup is warranted specifically for these patients.
Frozen shoulder is commonly encountered in patients between the ages of 35 and 60 years. 8 It may arise spontaneously without an obvious predisposing cause, or it may be associated with a variety of local or systemic disorders. The diagnosis of idiopathic frozen shoulder (IFS) is based on the recognition of the characteristic features of pain and global limitation in passive range of motion of the shoulder, in the absence of other focal shoulder pathology such as glenohumeral joint arthritis or rotator cuff tears. 5,8,13,14
While the prevalence of IFS among the general population is considered to be between 2% and 4%, 3,14 a significantly higher prevalence of 10% to 22% has been reported in patients with diabetes mellitus. 2,8,13,15 Because diabetic patients are more prone to develop frozen shoulder than nondiabetics, the question that arises is whether patients diagnosed as having IFS are at greater risk to develop diabetes. A review of the literature has found only 1 study that is related to this issue. 16
The oral glucose tolerance test is a glucose loading test that can detect abnormal glucose metabolism that has not yet revealed itself clinically as diabetes mellitus. 1,12 It is a “stress test” for the glucose metabolism and is considered the best method to detect prediabetic states. Patients with glucose intolerance (abnormal glucose metabolism) are considered to be prediabetics, with a significant probability of becoming diabetics in the future. 7,12 Changes in life habits of prediabetic patients have shown a reduction of 50% in the development of diabetes. 12
Since early diagnosis of diabetes and prediabetes (glucose intolerance) have been shown to reduce the risks of future disease-related complications, 12 the significance of early diagnosis of these conditions is clear. Therefore, if IFS can be shown to be associated with probable future emergence of diabetes, routine evaluation for prediabetes should be performed for these patients.
The question for the treating physician is if a diagnosis of IFS should be an indication for prediabetes screening. Consequently, we focused on patients who had no other indications for diabetic screening. Therefore, we did not include in this study female patients with gestational diabetes, which is a known predisposition for the development of diabetes, 6 patients who take diabetogenic medications, or patients older than 60 years because of the very high prevalence of prediabetes in the general population of that age (around 50%). 5
Our objective was to determine whether the diagnosis of IFS is an indication to screen for diabetes.
Methods
This study was approved by a university hospital institutional review board. The study cohort consisted of patients from a hospital shoulder clinic who were diagnosed with IFS by 2 of the authors (O.S., C.M.). Patients were asked to participate in the study if they met the following inclusion criteria: age 35 to 60 years, absence of shoulder pathology in a shoulder radiograph and absence of a full-thickness rotator cuff tear in an ultrasound examination, as well as no known previous diagnosis of diabetes mellitus or (for women) previous diagnosis of gestational diabetes. Patients were excluded if they used diabetogenic medications (steroids), had other known hormonal issues, had rheumatoid diseases, or were previously diagnosed with shoulder pathology (fracture, full-thickness rotator cuff tear, glenohumeral arthrosis, or any history of shoulder surgery). IFS was diagnosed on the basis of an insidious onset of painful global limitation of shoulder motion in the absence of shoulder pathology in standard shoulder radiographs and the absence of a full-thickness rotator cuff tear in an ultrasound examination. The global limitation of shoulder motion included limitation in flexion and internal rotation as well as external rotation limitation of more than 50% compared with the contralateral shoulder. 3,13
Fifty-nine patients were asked to participate in this study, of whom 51 (88%) agreed. After signing informed consent, patients underwent a 2-hour glucose tolerance test. After an overnight fast, a venous blood sample was drawn, then 75 g of glucose mixed in water were taken orally by the patient. Two hours later, an additional venous blood sample was taken. Blood samples were cooled during the time of the procedure and were then sent for glucose-level analysis. Fasting as well as 2-hour post–glucose loading results were documented for each patient. Overall, 50 patients completed the test successfully. In 1 patient, technical mishandling of the blood samples led to erroneous analysis. According to the plasma glucose levels, patients were diagnosed as normal glucose tolerance, prediabetic (impaired fasting glucose and/or abnormal 2-hour glucose tolerance), or as diabetic. Table 1 presents the values used to diagnose these conditions. 12
Classification of Glucose Intolerance According to Glucose Levels a
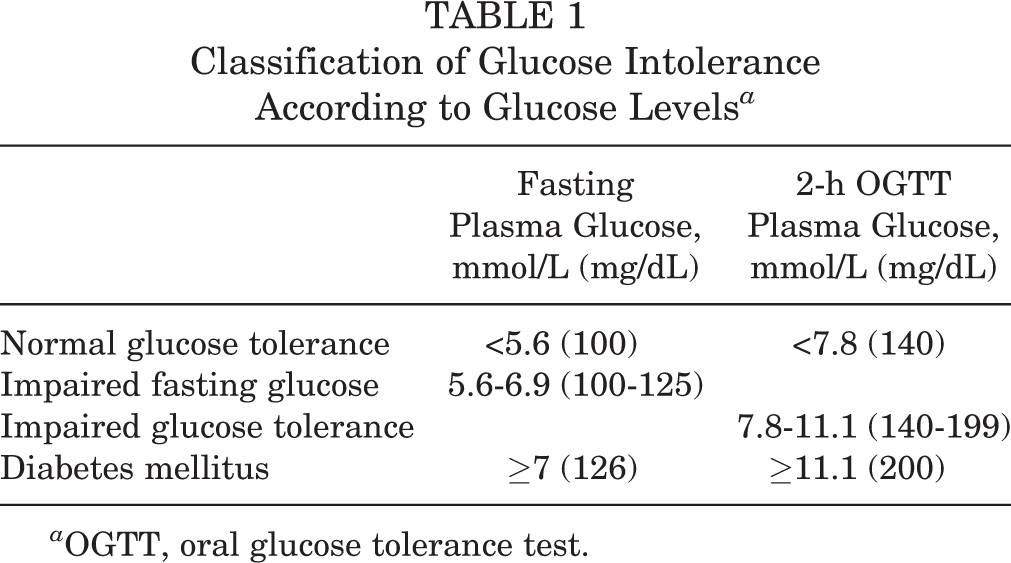
a OGTT, oral glucose tolerance test.
The sample size was calculated on the basis of the prevalence of impaired glucose tolerance in patients with IFS found in a previously published study (48% of patients 16 ) and in an age-matched general population (15% of patients 7,12,17 ). The percentage of prediabetic patients in this study was compared with previously published reports of the prevalence of prediabetes in the general, age-matched population using a 1-sided chi-square test. Univariate analysis was conducted, and differences were considered significant at P ≤ .05.
Results
There were 27 female and 23 male study participants. All patients were white, and all patients were members of health maintenance organizations (HMOs). Their mean age was 51 years (range, 36-60 years; SD ±5.4). The dominant hand was involved in 19 patients (39.6%). Five patients (10%) reported a prior history of frozen shoulder affecting the contralateral shoulder. Twenty-one patients (42%) reported a family history of diabetes in their immediate family (parents, siblings). The mean body mass index (BMI) was 25.3 kg/m2 (range, 18.8-34.5 kg/m2; SD ±7.9).
Mean glucose fasting level was 4.5 mmol/L (range, 2.8-6.0 mmol/L; SD, ±0.7), and mean 2-hour glucose level was 5.5 mmol/L (range, 3.8-10.8 mmol/L; SD, ±1.5). Four patients were diagnosed with prediabetes in this study. There was 1 patient with an impaired fasting glucose of 6 mmol/L. Three patients (6%) had abnormal 2-hour glucose levels of 8.3, 9.6, and 10.8 mmol/L and were therefore diagnosed as having impaired glucose tolerance. The patient with impaired fasting glucose was a male aged 49 years, and the other 3 patients with impaired glucose tolerance were women aged 49 years (1 patient) and 57 years (2 patients). BMI data of these 4 patients were similar to those of the entire group (range, 20.0-31.3 kg/m2, mean ± SD, 26.0 ± 5.6 kg/m2). All 4 patients reported a family history of diabetes in parents or siblings. No patient was diagnosed with diabetes. Table 2 presents the P values found when the percentage of prediabetic patients in this study was compared with previously published reports of the prevalence of prediabetes in a general, age-matched population. No statistically significant differences were found in this comparison.
Prevalence of Glucose Intolerance in Different Populations With Similar Ethnicities and Age Group to the Present Study

aP value was calculated between the study described and the current study.
Discussion
This study prospectively evaluated the prevalence of diabetes and prediabetes in patients diagnosed with IFS who did not have a prior diagnosis of diabetes or prediabetes. We found 4 of the 50 patients in this study (8%) to have prediabetes. We have found no case of diabetes in these patients.
To compare the prevalence of prediabetes in our study group with the general, age-matched prevalence, we used previously published reports. As diabetes and prediabetes prevalence vary between different ethnic groups, 1,17 we compared our data with groups of similar ethnicities 7,9,11,17 and similar age categories. Table 2 presents the prevalence of glucose intolerance in these populations. The rate of prediabetes in our study group (8%) was within the range found in similar age-matched populations. Therefore, the prevalence of diabetes and prediabetes in patients with IFS who are not known diabetics or prediabetics was similar to that of an age-matched population.
This study included patients aged 60 years or younger and excluded patients with prediabetic conditions such as gestational diabetes. We did not include patients older than 60 years for 2 main reasons. First, the high frequency of prediabetes and diabetes among people older than 60 years in the general population makes people in this age group already prone to diabetic conditions. 5 Second, IFS is less common in patients older than 60 years. Since our study question was to evaluate the need for diabetic screening in patients diagnosed with IFS, we decided to focus on the bulk of such patients, who are not already at high risk for diabetes and prediabetes due to their age.
Our results differ from a previously published study that investigated the same question. 16 In that study, Tighe and Oakley 16 examined a subpopulation of 52 patients who had IFS without a previous diagnosis of diabetes or prediabetes. Using a 2-hour glucose test, these authors found a prevalence of 3.8% for diabetes and 48% for prediabetes in this group and concluded that patients with frozen shoulder should be routinely screened for diabetes. 16 The different findings of these 2 studies can be explained by 2 factors: The quality of the medical surveillance of the study populations prior to the study may differ. In the current study, all participants were members of HMOs. Higher HMO member ratio in the study population may yield better basic health surveillance and prediabetes and diabetes detection. Another difference may be a function of inclusion criteria. Tighe and Oakley 16 included a significant number of patients in the seventh and eighth decade, an age group that was excluded from this study. Patients older than 60 years have significantly higher prevalence of both diabetes and prediabetes. 17 Since most patients with IFS are younger than 60 years, the older patient subset in the study by Tighe and Oakley 16 may represent a skewed population with a higher prevalence of diabetes and prediabetes. Race and BMI range were not stated in their study and may also be possible explanations for the difference observed between the results of the 2 studies. In addition, the prevalence of obesity, a risk factor for diabetes, varies between different geographic locations and could also potentially explain the differences between the studies.
A weakness of this study is the lack of an in-study control group. This may have led to an inaccurate estimation of prediabetes in the general, aged-matched population. However, the rate of patients with prediabetes in this study was relatively small, both absolutely and in comparison with a relevant similar population. Therefore, this should not affect the implication of our results.
Another weakness of our study is that all patients were white, and no patients were severely obese (BMI >35 kg/m2); therefore, our findings may not be generalizable to all populations. Finally, the “control” populations that we used were from reports published 17 to 33 years earlier. It is possible that the incidence of impaired glucose tolerance has increased in some of the populations (eg, the United States, England) along with an increased incidence of obesity.
It has been recommended by some that patients diagnosed with IFS should undergo a full diabetic workup to screen them for prediabetes if they are not known to be diabetics. 4,10,16 This is based on the significantly higher incidence of frozen shoulder among the diabetic population, which leads to the assumption that IFS may be a prediabetic condition. Our study findings do not support this view. Based on our study results, we conclude that newly diagnosed patients with IFS who are 60 years or younger and are not known diabetics or prediabetics have a similar probability of having diabetes or prediabetes to their age-matched population. Therefore, no routine diabetic workup is warranted specifically for these patients.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Committee on Research Involving Human Subjects, Hebrew University-Hadassah Medical School.