
Abstract
Background:
Anterior cruciate ligament (ACL) tear is the most frequent injury in alpine ski racing, and there is a high prevalence of ACL reinjury. Limited data exist on the concurrent pathology with primary ACL tears in elite alpine ski racers and the magnitude of injury progression after primary ACL reconstruction (ACLR).
Purpose:
To evaluate (1) the involvement of intra-articular and multiligament pathologies at the time of primary ACLR, (2) the subsequent progression in meniscal/chondral injuries, and (3) the occurrence of ACL reinjury in elite alpine ski racers.
Study Design:
Case series; Level of evidence, 4.
Methods:
Primary ACLR operative reports (n = 28) were obtained for 32 elite alpine ski racers along with the reports of 20 operative procedures that occurred subsequent to primary ACLR. Operative reports were evaluated to identify the presence/location of multiligament injury, meniscal tears, and chondral lesions.
Results:
At the time of primary ACLR, a majority of knees (82%; 23/28) demonstrated concurrent injury compared with isolated ACL tears; 32% of knees sustained multiligament injuries (9/28), and 8 involved the ipsilateral medial collateral ligament (MCL). Of the ACL-injured knees, 54% had chondral lesions, of which 73% were sustained in the lateral knee compartment, and 82% of meniscal tears (14/17) were complex in nature. Bilateral ACL tears were seen in 22% of the participants, and 28% underwent ACL revision. In the case of ACL revision or future meniscal/chondral surgery, 60% of meniscal tears and 80% of chondral lesions had worsened since the time of primary ACLR.
Conclusion:
Concurrent injury was common in this group of elite ski racers. Primary ACL tears were typically accompanied by lateral compartment chondral lesions and complex meniscal tears that worsened over time. ACL/MCL tears were the most common multiligament injury pattern.
Severe knee injuries account for more than one-third of the injuries suffered by elite alpine ski racers, and anterior cruciate ligament (ACL) tears are the most frequent diagnosis. 6,11 The percentage of alpine skiers who require ACL revision surgery (19%) is higher than other athletic and nonathletic populations, which ranges from approximately 2% in the general population to about 4% to 9% in young athletes. 2,23,26,31,32 Despite efforts to mitigate injury risk in alpine ski racing, ACL injury rates remain high. 13,34 Unlike in field sports, 33 there is no difference in ACL injury rates between male and female elite skiers. 6,11,34 The overall high risk for ACL tears in elite alpine ski racing and the finding of no sex-based differences may be due to the unique high-energy injury mechanisms that generate external abduction (valgus) and internal rotation forces on the knee. 5
While alpine ski racers who have undergone ACL reconstruction (ACLR) may succeed in returning to sport 14,34 compared with other athletic populations, 3 recent studies show that skiers after ACLR may have significant and persistent neuromuscular deficits. 18 –20 This suggests a requirement for more scientific research on the impact of ACL injuries in this population. 17 The long-term effects of ACL injury on the knee joint health of elite alpine ski racers remains unclear, yet ACL injury is known to increase the risk of developing early-onset knee joint osteoarthritis (OA) in young adults, 35 especially when the ACL tear occurs alongside injury to other knee structures such as the articular cartilage and menisci. 4,27 In fact, the concurrent pathology with ACL tears, including multiligament injuries, chondral lesions, and meniscal tears, are important determinants of outcome after ACLR. 8,16,22,29,36,39 The only study examining elite and professional alpine skiers, now more than 30 years old, showed a high prevalence of medial collateral ligament (MCL) injuries, medial meniscal tears, and only a small fraction of knees with chondral lesions. 15 However, since this study’s publication in 1987, there have been dramatic changes to ski equipment, faster skier speed, and the recent identification of high-energy ACL injury mechanisms specific to alpine ski racing. 5 Thus, it seems likely that the concurrent pathology with primary ACL tears in elite alpine ski racers may have evolved as well over the past 30 years.
Thus, the purpose of the present retrospective study was 3-fold: (1) to evaluate the concurrent pathologies, including meniscal tears, chondral lesions, and multiligament injuries, at the time of primary ACLR in elite alpine ski racers; (2) to evaluate the future state of the chondral lesions and meniscal tears; and (3) to evaluate the occurrence of ACL reinjury in elite alpine ski racers by reviewing postoperative reports obtained from surgeries that occurred subsequent to the primary ACLR.
We hypothesized that at the time of primary ACLR, ACL tears would be accompanied by a greater proportion of lateral meniscal tears, lateral compartment chondral lesions, and multiligament injury involving the MCL compared with the other concurrent injuries. In addition, at the time of subsequent surgery after primary ACLR, we expected to find a significant number of skiers with a deterioration in their meniscal tears and chondral lesions.
Methods
Study Design
The retrospective study design was approved by a university research ethics board, and a search of a physical fitness testing database housed at a national sport training center was undertaken to identify skiers who competed for the Canadian Alpine Ski Team between 2000 and 2015. As the Canadian Alpine Ski Team conducted their annual physical fitness testing at the training center, the database contained a comprehensive record of Canadian national team alpine ski racers. A total of 137 skiers were identified in the database. After this search, current/former coaches, team physicians, and physical therapists were enlisted to identify the alpine ski racers who suffered an ACL injury during this period (n = 39) (Figure 1). These individuals were contacted to enlist their participation in the study and to verify their history of ACL injury.

Overview of the participant recruitment process.
Thirty-two athletes responded, provided informed consent, and completed a questionnaire to provide background information on their ACL injuries (males [n = 15]: time competing on national team = 8.5 ± 5.7 years, right limb dominant n = 13, left limb dominant n = 2; females [n = 17]: time competing on national team = 8.2 ± 4.0 years, right limb dominant n = 12, left limb dominant n = 1, no limb dominance n = 4). Limb dominance was defined as the preferred limb for kicking a ball. Of the 32 participants included in this study, 7 sustained bilateral ACL injuries, bringing the total number of knees with primary ACL injury to 39. At the time of a future ipsilateral ACL reinjury, 1 skier also sustained a contralateral ACL tear (ie, ipsilateral ACL reinjury/contralateral ACL injury). There were no bilateral primary ACL ruptures that occurred at the same time in this patient group. From these questionnaire data, we determined the following: (1) the date of primary ACLR, (2) limb (left or right) that was injured, (3) graft type, (4) name of the surgeon, (5) whether the reconstructed limb was revised or a contralateral ACL tear was sustained after the primary ACL injury, (6) date of eventual revision or contralateral ACLR after the primary ACL injury, and (7) name of the surgeon who performed the revision or contralateral ACLR. While annual physical fitness testing was performed at the same testing laboratory over the 15-year study period, the Canadian Alpine Ski Team program was not consistently centralized in the same geographic location. Thus, specific documentation was unavailable regarding more detailed postoperative care procedures, and the skiers did not follow a standardized rehabilitation program.
Six Canadian orthopaedic surgeons contributed surgical reports for primary ACLR procedures performed for 28 knees. This information included 4 reports for contralateral ACL surgeries. Surgical reports that occurred after the primary ACLR (future surgeries), including surgery for ACL revisions, meniscal tears, or chondral lesions, were obtained for 21 knees. For all knees without primary ACLR operative reports, questionnaire data were only used to obtain the date of the primary ACLR, the limb injured, and the graft type. In the event of missing operative reports subsequent to the primary ACLR, questionnaire data were used to determine whether an ACL revision or contralateral ACL injury was suffered and the date of the surgery. Patient questionnaire data were not used for assessing multiligament injuries, meniscal tears, or chondral lesions.
The data from the surgical reports were coded and transferred onto a spreadsheet (Microsoft Excel, version 15.24) by a researcher with medical knowledge. Additionally, a second researcher reviewed the operative reports independently to verify the accuracy of the data. In the event of discrepancies, the corresponding surgeon was contacted directly for verification. The primary ACLR surgery operative reports and operative reports that occurred after the primary ACLR were used to determine the following binary (yes/no) outcome measures: complete or partial tear of the ACL, and presence or absence of multiligament injury, meniscal tears, and chondral lesions. The location of the chondral lesions was classified as lateral compartment, medial compartment, and patellofemoral compartment. A modified Outerbridge rating system 28 was used to classify the severity of chondral lesions: grade 1 (softening and fibrillation), grade 2 (partial thickness defect with fissures on the surface that did not reach subchondral bone or exceed 1.5 cm in diameter), grade 3 (fissuring to the level of subchondral bone in an area greater than 1.5 cm), and grade 4 (exposed subchondral bone). Meniscal tears were classified according to the location (medial or lateral meniscus) and the tear type. Surgical reports that followed the primary ACLR were used to evaluate the presence of contralateral ACL tears or ACL revisions, the progression of meniscal tears, and the progression of chondral lesions.
Statistical Analysis
Descriptive statistics, including the group mean and standard deviation, were calculated for all continuous variables and reported as the mean value ± SD (RStudio, Version 0.99.902). The proportions of cases sustaining chondral lesions, meniscal tears, multiligament injuries, ACL revisions, and contralateral ACL tears were compared within the patient group using a chi-square test of proportions. A chi-square test of proportions was also used for within-group comparison of the number of skiers showing a progression in their chondral lesions and meniscal tears over time. A Yates continuity correction was used when required, and statistical significance was set at α = .05 using a 2-tailed design.
Results
Concurrent Pathology at Time of Primary ACLR
Of the 39 ACL tears identified through the questionnaire, 23 (59%) occurred on the left knee. Using the primary ACLR operative reports, 5 of 28 knees (18%) had only isolated tears and 23 of 28 (82%) knees had associated injury. A comparison of these 2 proportions showed statistically significant differences (P < .0001). Nine of 28 knees (32%) had multiligament injuries, including 1 posterior cruciate ligament (PCL)/ACL/MCL tear and 8 MCL tears (Table 1). Two grade 1 MCL tears were treated conservatively, and 6 were surgically repaired (grade 2, n = 1; grade 3, n = 5). Three knees had only chondral lesions, 5 knees had only meniscal tears, and 12 knees had both meniscal and chondral injuries. In total, 54% of knees (15/28) had chondral lesion(s). More chondral lesions occurred in the lateral compartment (11/15 knees) versus the medial compartment (4/15 knees) (P < .001) (Table 1). Seventeen of the 28 knees (61%) had meniscal tears at the time of the primary ACL surgery. Compared with single-dimension meniscal tears, there was a greater number of complex meniscal tears (ie, included a combination of at least 2 tears either in the vertical, horizontal, or radial direction) (P < .05) (Table 1). Eight meniscal tears were repaired, 8 tears were resected, and 1 meniscal tear was not treated.
Concurrent Injury at the Time of Primary ACL Reconstruction Surgery a
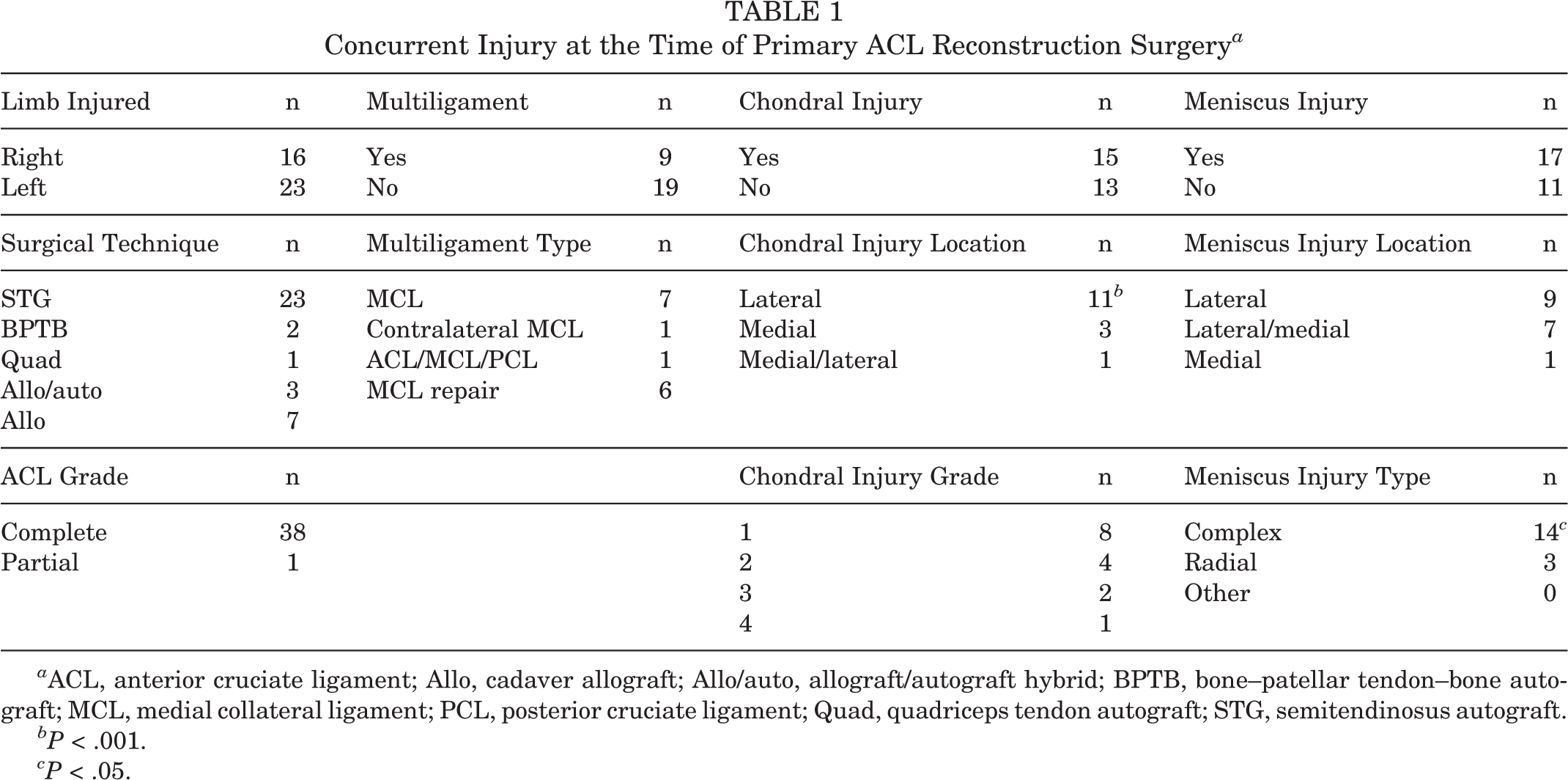
a ACL, anterior cruciate ligament; Allo, cadaver allograft; Allo/auto, allograft/autograft hybrid; BPTB, bone–patellar tendon–bone autograft; MCL, medial collateral ligament; PCL, posterior cruciate ligament; Quad, quadriceps tendon autograft; STG, semitendinosus autograft.
bP < .001.
cP < .05.
ACL Revisions, Contralateral ACL Injuries, and Progression of Chondral/Meniscal Injury
Seven of the 32 participants (22%) sustained bilateral ACL tears (total number of knees with primary ACL tears: n = 39). The mean time to the contralateral ACL injury was 3.6 ± 2.8 years (median = 2.3 years). Twenty-eight percent (11/39) of knees underwent an ACL revision. Seven skiers had a single ACL revision, and 4 skiers had 2 or more ACL revisions. ACL revision operative reports were obtained for 8 knees. The mean time to the first ACL revision was 3.3 ± 2.2 years (median = 2.3 years). At the time of ACL revision, 63% of knees (5/8) demonstrated new meniscal tears, and chondral lesions had worsened in 63% of knees (5/8). Of the 39 knees, 15 (38%), including 3 knees with ACL revision, underwent a subsequent surgery for meniscal tears or chondral lesions. Operative reports were obtained for 13 knees.
The mean time to the subsequent surgery was 4.7 ± 5.4 years (Table 2). At the time of the subsequent surgical procedure, 62% (8/13) of the meniscal tears had worsened. Seven skiers who had meniscal repairs or resections performed at the time of primary ACLR went on to have subsequent meniscal surgery. The meniscal tears of 3 patients with resection at the time of primary ACLR had worsened, and 2 were unchanged. The tears of the 2 patients with meniscal repairs at the time of primary ACLR were unchanged. The proportion of knees with worsening chondral lesions (11/13) was greater than the number of chondral lesions that had remained the same since the primary ACL surgery (2/13) (P < .01) (Table 2). Ten knees were identified with grade 3 or 4 chondral lesions compared with 3 at the time of primary ACLR. One patient who presented with a high-grade partial ACL tear, complete PCL tear, and complete MCL tear underwent a primary PCL/MCL reconstruction followed by ACLR and MCL revision 13 months after the accident.
State of Articular Cartilage and Menisci at the Time of Future Surgeries After the Primary ACL Reconstruction a

a ACL, anterior cruciate ligament.
bP < .01.
Discussion
This study provides current and updated data on the concurrent pathology with ACL tears in an elite alpine ski racing population. At the time of primary ACLR, a high proportion of combined ACL injuries (82%) were observed compared with isolated ACL tears (18%). The proportion of skiers with just isolated ACL tears in this study is lower than reports from other athlete populations, which range from 28% in American football to 44% in team handball. 12 More than half (61%) of the present group of skiers had meniscal tears at the time of primary ACLR. In a general nonathletic population, the prevalence of meniscal damage with ACL tears is 34% to 51%, 7,8,21,23 and it is 41% to 51% in recreational skiers. 10,30 We observed that a high percentage of meniscal tears (82%) were complex and also involved the lateral meniscus. This finding contrasts with an earlier report by Higgins and Steadman, 15 perhaps the only published study that evaluated the concurrent pathology with ACL tears in elite/professional alpine ski racers, in which only peripheral meniscal tears were observed, and medial meniscal tears outnumbered those found in the lateral meniscus. We observed, however, only a single isolated medial meniscal tear. The percentage of complex meniscal tears in this group of elite skiers was also higher than in recreational alpine skiers, where the reported prevalence is less than 10%. 10,12 This finding is of concern, as meniscal injuries occurring with ACL tears are known to accelerate the progression of knee joint OA. 8,22,24,29,35,36
Articular cartilage lesions were found in 54% of the skiers at the time of primary ACLR, which also appears elevated compared with the 15% to 47% reported for the general population. 7,16,21 –23,25 The majority of the current group of elite ski racers (73%) sustained lateral compartment chondral injuries with their ACL tears. This is consistent with the literature showing that acute ACL tears coincide predominantly with lateral compartment tibiofemoral injury. 7,22 The greater prevalence of lateral compared to medial compartment chondral lesions is also consistent with the injury patterns observed in recreational alpine skiers. 9,30 However, the study conducted by Higgins and Steadman 15 in 1987 with elite/professional skiers reported articular cartilage injuries in just 10% of athletes. Our findings, including a high prevalence of lateral compartment injuries to both the meniscus and the articular cartilage, suggest marked developments in the injury patterns associated with primary ACL tears in high-performance ski racers, which may be due to the substantial changes in ski equipment and increased skier speeds over the past 30 years. 5 These factors contribute to unique high-energy injury mechanisms in modern-day alpine ski racing that result in combined tibial internal rotation/valgus loading of the knee joint and likely anterior subluxation of the tibia. 5,30
In the current study, 32% of the skiers sustained a multiligament injury along with their ACL tear, and all but 1 injury involved the ipsilateral MCL. ACL/MCL tears are less prevalent in the general population (8%-13%) than in this group of elite ski racers, 21,23 and alpine skiers may be 1.9 times more likely to suffer ACL/MCL injuries compared with soccer players. 12 The present findings are consistent with data from nonelite alpine skiers showing that ACL/MCL injuries occurred in 31% to 38% of all ACL injuries. 10,30 However, the percentage suffering ACL/MCL injury is lower than reported by Higgins and Steadman 15 who noted that 80% of high-performance alpine skiers suffered ACL/MCL injury. Nevertheless, the ACL/MCL injury appears to remain a common multiligament injury pattern among top-level alpine ski racers. The unique injury mechanisms in skiing involve equipment risk factors such as the lever arm of the ski, a stiff boot restricting ankle range of motion, and neuromuscular factors (eg, aggressive quadriceps contraction) that culminate in high knee valgus/shear loading and altogether likely contribute to the greater occurrence of ACL/MCL injuries in elite alpine skiers. 5,30
In the present study, 28% of the knees underwent ACL revision surgery, and 4 knees (13%) required multiple revisions. Of the 32 overall skiers, 7 (22%) suffered an ACL tear to the contralateral limb. The scientific data on ACL revisions and contralateral ACL injuries in elite alpine ski racers is limited. 34,37 Pujol et al 34 found that 30% of elite alpine ski racers with ACLR suffered contralateral ACL injury, whereas the prevalence of ipsilateral reinjury was 19%. A study evaluating collegiate-level alpine ski racers reported that 22% underwent ACL revision surgery. 37 Both these reports, along with the findings of the present investigation, are limited by the retrospective study design. Nevertheless, the prevalence of bilateral ACL tears and ipsilateral ACL reinjury in this group of elite alpine ski racers is high compared with the general population, where ACL revision surgery consequent to reinjury is performed in less than 4% of patients. 2,23 Young female athletes appear to be at an increased risk for ACL revision (5%-25%) 2,32 and contralateral ACL injury 31,32 compared with the general population, but the prevalence is still lower than seen in the present athlete group and compared with others who have evaluated ACL reinjury in alpine ski racers. 34,37 The average time to the contralateral injury and revision surgery was 3.6 and 3.3 years, respectively, but the data were skewed toward shorter time duration (median time to contralateral ACL tear = 2.3 years; median time to ACL revision = 2.3 years). Consistent with other reports, it seems that the first few years after primary ACLR represent a period of increased vulnerability for ACL reinjury. 27,32
In the present study, 38% (15/39) of knees underwent a subsequent surgery for either chondral lesions or meniscal tears at a mean time of 4.7 years after primary ACLR. At the time of surgery for ACL revision or meniscal/chondral injury, 80% of the chondral lesions had worsened since the primary ACLR. While only 11% of the knees had grade 3 or 4 chondral lesions at the time of primary ACLR, 50% of knees had a grade 3 or 4 chondral lesion at revision. Furthermore, 60% displayed a worsening of their meniscal tears from the time of primary ACLR. The progression of chondral lesions and meniscal tears after ACL revision surgery is a crucial factor related to knee health, including early onset of knee OA. 1,8,24,29,35,39,40 In a group of 109 nonathletes, 29% presented with a grade 3 or 4 cartilage loss, and 59% with medial meniscus tears at the time of ACL revision surgery. 1 A study comprising 1205 patients found that 59% had signs of abnormal articular cartilage and menisci at the time of ACL revision surgery, which negatively affected patient-reported outcomes at the time of ACL revision surgery. 39 Based on the present data, it seems that a deterioration in meniscal tears and chondral lesions should be expected in elite alpine ski racers after primary ACLR, along with an elevated prevalence of severe articular cartilage degeneration, compared with previous reports. Nevertheless, it seems that a high percentage of elite alpine ski racers may surpass their preinjury performance level after ACL injury. 14 However, in the present study we were unable to obtain pre- and postinjury performance data.
There are challenges with studying elite alpine ski racers, such as working with small sample sizes. Nevertheless, this type of investigation is important given the high prevalence of ACL tears among this athlete population. 6,11 While small sample sizes are an inherent problem of studying elite athlete populations, such investigations are deemed essential for sport-specific injury prevention efforts. 38 An additional limitation of the present study was the inability to control for a standardized rehabilitation protocol after primary ACLR. Finally, the use of the questionnaire assessment may have introduced a recall bias. We accounted for this bias by only using questionnaire data to determine surgical occurrences and the limb that was injured and to identify the specific graft type. All other parameters of interest related to the study objectives were determined through analysis of the available operative reports. Despite these limitations, this study provides current and unique data on the associated pathology with primary ACL tears in elite alpine ski racers, while also addressing the progression of related knee injuries. The present findings may be important for clinicians who want to predict the progression of concurrent injuries with ACL tears in elite alpine ski racers and to devise suitable timelines for safe return to sport to protect skiers against reinjury and/or further injury progression.
Conclusion
A higher prevalence of combined chondral, meniscal, and ligament injuries versus isolated ACL tears were observed in this group of alpine ski racers compared with reports in the scientific literature comprising other athletic or nonathletic populations. Complex meniscal tears were the most prevalent comorbidity, and a significantly greater proportion of lateral compartment chondral lesions were observed compared with medial compartment lesions. The progression of meniscal tears and chondral lesions appeared to be more severe in the present group of alpine ski racers compared with other athlete groups.
Footnotes
Acknowledgment
The authors acknowledge support from Own the Podium and the Canadian Sport Institute Calgary.
One or more of the authors has declared the following potential conflict of interest or source of funding: The Alberta Innovates Health Solutions, the Killam Laureates, the Canada Research Chair Programme, and the Killam Foundation provided funding for this research.
Ethical approval for this study was obtained from the Conjoint Health Research Ethics Board at the University of Calgary (Ethics ID: REB14-2270_MOD1).