
Abstract
Background:
Hamstring autograft is a common graft choice when performing ulnar collateral ligament reconstruction (UCLR).
Purpose/Hypothesis:
The purpose of this study was to survey Major League Baseball (MLB) team physicians and determine whether these physicians harvest the hamstring (semitendinosus or gracilis) from the drive leg (ipsilateral to surgical site) or landing leg (contralateral to surgical site) when performing UCLR on elite-level pitchers. The hypothesis was that the majority of surgeons harvest the hamstring from the drive leg when performing a UCLR.
Study Design:
Descriptive epidemiology study.
Methods:
Overall, 52 MLB team orthopaedic surgeons were sent the 5-question online survey. The survey assessed surgeon UCLR volume, surgical technique, which leg the hamstring graft was harvested from, the reasoning for choosing that particular leg, and whether the surgeon would change their practice if evidence showed the hamstring from one of the legs was more important than the other. The survey was sent out 5 separate times to maximize the response rate.
Results:
Forty (77%) MLB team physicians completed the survey. The largest number of surgeons (n = 16; 40%) performed between 5 and 14 UCLRs annually, while 6 (15%) performed more than 50 UCLRs annually. Most surgeons (n = 23; 57.5%) used the docking technique. Significantly more surgeons harvested the hamstring from the landing leg (n = 29; 72.5%) compared with the drive leg (n = 11; 27.5%) (P = .007). More surgeons cited the reason for their choice of leg as a belief that the hamstring they harvested plays less of a role in the ability of a pitcher to generate a forceful pitch (n = 25; 62.5%) than for logistical reasons in the operating room (n = 15; 37.5%); this difference was not statistically significant. Significantly more surgeons would change their practice (n = 35; 87.5%) if evidence showed the hamstrings from a specific (drive or landing) leg to be more active in the throwing motion compared with those who would not (P < .001).
Conclusion:
When performing a UCLR using hamstring autograft, the majority of MLB team physicians harvest the hamstring from the landing leg as opposed to the drive leg, as they believe the hamstring from the landing leg plays less of a role in generating a forceful pitch than that from the drive leg.
Keywords
Injuries to the ulnar collateral ligament (UCL) have become commonplace among elite-level and adolescent baseball pitchers. 3,6,11,12,15,26,34 While some pitchers are fortunate enough to return to sport (RTS) after a period of rest and rehabilitation, most pitchers who wish to RTS at a high level after sustaining such an injury require a UCL reconstruction (UCLR). 24,35 Studies have described many UCLR techniques that afford pitchers the ability to RTS at rates greater than 85%, although these studies have not found a specific technique to be superior to the rest. 3,5,10,12,16,36,44 While UCL repair with an internal brace has received recent attention with promising short-term results, the current standard treatment for baseball pitchers who wish to RTS is a UCLR. 3,7 –9,26
When performing a UCLR, several graft options for reconstruction include palmaris longus autograft, hamstring autograft, allograft, and others. 3,10,38 Studies have shown reliable RTS rates from each graft choice, with no superiority of one choice over another, although no randomized comparative trials exist. 3,13 When a patient does not have a palmaris longus tendon in either arm, the palmaris tendon appears small in size or damaged (torn, ossified, etc), or the patient is undergoing a revision UCLR, many surgeons choose to harvest a hamstring tendon (gracilis or semitendinosus) from either the ipsilateral leg or contralateral leg, similar to an anterior cruciate ligament reconstruction (ACLR). 1,28 The ipsilateral leg is commonly known as the drive or lag leg while the contralateral leg is known as the landing or lead leg.
Hamstring tendon harvest is a relatively benign procedure with low reported graft site complication rates in the ACLR literature, including injury to the infrapatellar branch of the saphenous nerve and wound dehiscence. 29,32,37 However, one complication that can have a long-lasting effect on patients is persistent hamstring weakness on the side of the harvest. While studies have shown varying amounts of hamstring regrowth after gracilis and semitendinosus harvest, some studies have shown persistent weakness in knee flexion at final follow-up. 2,27,40,42 Long-term follow-up has demonstrated essentially permanent atrophy of those muscles attached to the harvested tendons. 41 It is unclear whether this residual weakness has an effect on pitching mechanics in high-level baseball pitchers.
Therefore, the purpose of this study was to survey Major League Baseball (MLB) team physicians and determine if these physicians harvest the hamstring from the drive leg or landing leg when performing a UCLR on elite-level pitchers. We hypothesized that the majority of MLB team physicians harvest the hamstring tendon from the drive leg when performing a UCLR on elite-level pitchers using a hamstring autograft.
Methods
We created a 5-question survey (Table 1) on the website SurveyMonkey (http://www.surveymonkey.com) and sent the survey to 52 MLB team orthopaedic surgeons. Surgeons were identified by team websites, Major League Baseball Team Physicians Association website (http://mlbtpa.org/index.php/team-physicians), and press releases. Only orthopaedic surgeons with a valid email address were included in this study. The team surgeons were determined by internet web searches. In 2016, the survey was sent out to the surgeons first on October 19 (round 1), and a reminder email was sent on November 3 (round 2), November 10 (round 3), December 7 (round 4), and December 21 (round 5) to those who had not yet completed the survey. The responses were kept confidential, and the data were organized via the SurveyMonkey web tool. We were blinded as to the surgeons’ names. The team physicians were instructed to respond to all relevant questions, and the survey was arranged such that the participant could not complete the survey without answering all the questions. Institutional review board approval was not necessary for this survey study.
Five-Question Survey Administered to Major League Baseball Team Orthopaedic Surgeons a
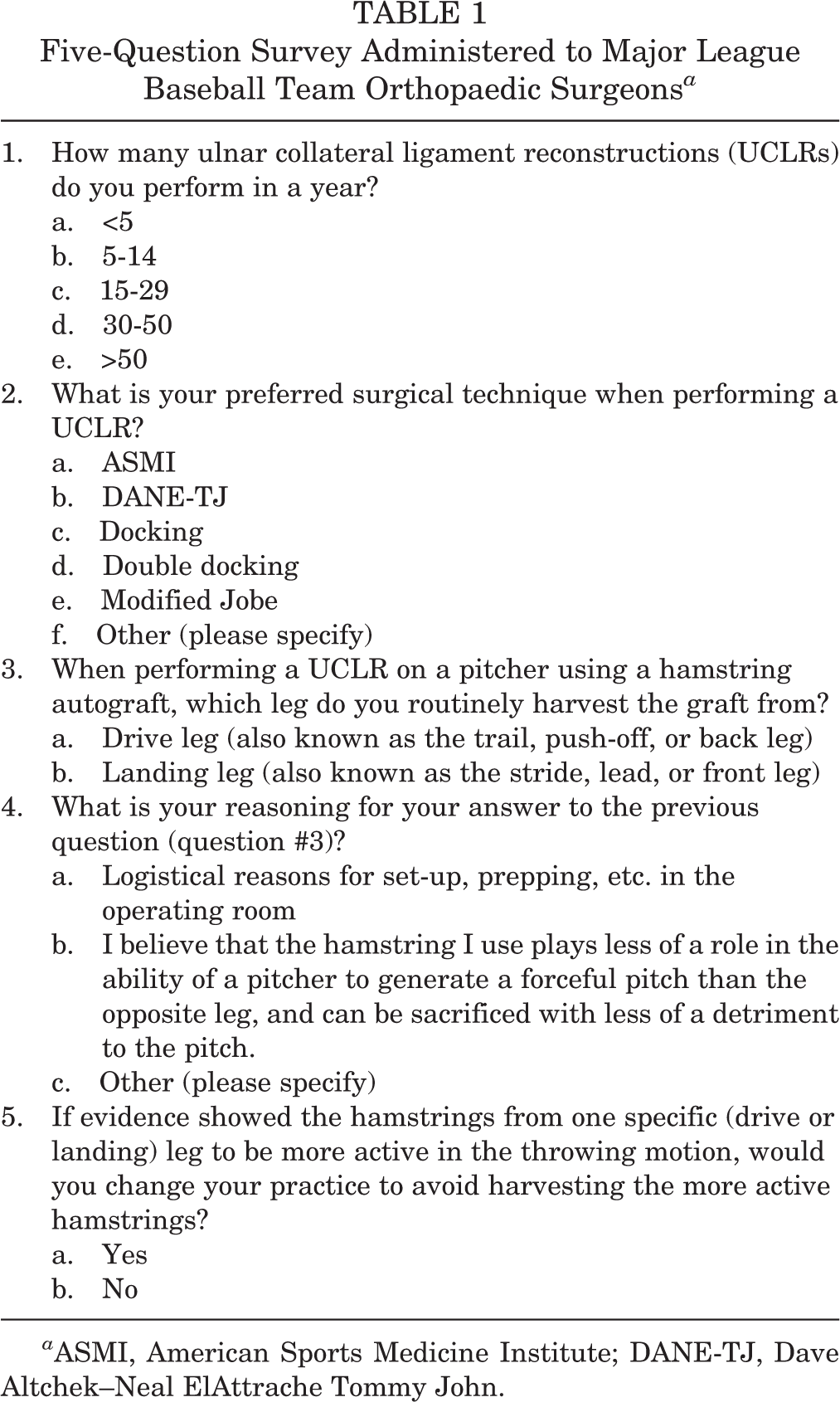
a ASMI, American Sports Medicine Institute; DANE-TJ, Dave Altchek–Neal ElAttrache Tommy John.
Statistics
Descriptive statistics were calculated. Chi-square and Fisher exact tests were used as appropriate, depending on cell populations to compare the distribution of responses to a null hypothesis of a random distribution. In addition, the distribution of responses of those surgeons who preferred the landing leg were compared with those who preferred the drive leg using chi-square and Fisher exact tests as appropriate, depending on cell populations.
Results
A total of 40 (77%) MLB team physicians responded to the survey. The majority of surgeons (n = 16; 40%) self-reported the performance of between 5 and 14 UCLRs annually, while 6 (15%) performed >50 UCLRs annually (Figure 1). Most surgeons (n = 23; 57.5%) performed UCLR using the docking technique, with 3 using the modified docking/docking plus technique (Figure 2).

Responses to “How many ulnar collateral ligament reconstructions (UCLRs) do you perform in a year?”

Responses to “What is your preferred surgical technique when performing a UCLR?” ASMI: American Sports Medicine Institute; DANE-TJ: Dave Altchek–Neal ElAttrache Tommy John; UCLR, ulnar collateral ligament reconstruction.
Significantly more surgeons harvested the hamstring from the landing leg (n = 29; 72.5%) than the drive leg (n = 11; 27.5%) (P = .007). Overall, most surgeons cited the reason for their choice of leg as a belief that the hamstring they harvested plays less of a role in the ability of a pitcher to generate a forceful pitch than the opposite leg (n = 25; 62.5%) rather than for logistical reasons in the operating room (n = 15; 37.5%); however, this difference was not statistically significant (P = .155). When responses were separated out based on which leg the surgeon harvested the hamstring from, more surgeons who harvested the hamstring from the landing leg did so because of a belief that the landing leg plays less of a role in generating a forceful pitch (21/29, 72%) while surgeons who harvested the hamstring from the drive leg did so more commonly for logistical reasons such as operating simultaneously on the arm and leg (7/11, 64%), although this difference was not statistically significant (P = .065) (Figure 3). There were no significant differences in technique between those surgeons who preferred the drive leg (8/11, 73% docking and modifications and 3/11, 27% Jobe and modifications) over the landing leg (21/29, 72% docking and modifications and 8/29, 28% Jobe and modifications) (P > .999); nor were there any significant differences in case volume between those surgeons who preferred the drive leg (4/11, 36% <15 UCLRs per year and 7/11, 64% ≥15 UCLRs per year) over the landing leg (17/29, 59% <15 UCLRs per year and 12/29, 41% ≥15 UCLRs per year) (P = .293).

Comparison of responses to why surgeons choose to harvest the leg from the landing leg versus the drive leg based on which leg they harvest their graft from.
Significantly more surgeons would change their practice (n = 35; 87.5%) than would not (n = 5; 12.5%) to avoid harvesting the more active hamstring if evidence showed the hamstrings from a specific leg (drive or landing) to be more active in the throwing motion (P < .001). Although not statistically significant, those surgeons who preferred the drive leg were no more likely to change their practice if evidence showed that hamstrings from a specific leg were more active in the throwing motion (10/11, 91%) compared with surgeons who preferred the landing leg (24/29, 83%) (P > .999).
Discussion
It has been well documented that the number of UCLRs performed in both elite and adolescent baseball pitchers is rising. 3,14,15,26 As the number of UCLRs continues to increase, it is important to determine how to optimize this procedure to afford pitchers the best chance at returning to sport at the same or higher level as before surgery. Because no clinical data exist on the importance of the hamstring tendons of the drive leg and landing leg in the baseball pitch, the expert opinion of MLB team physicians who perform UCLR on the most elite baseball pitchers and are most familiar with high-level pitching mechanics may provide the highest level of evidence available. Our hypothesis was incorrect, as the majority of MLB team physicians (72.5%) harvested the hamstring tendon from the landing leg when performing a UCLR using hamstring autograft as opposed to the drive leg.
Hamstring autograft has recently gained popularity as a viable graft choice when performing a UCLR in adolescent as well as elite-level athletes. 10,34 The gracilis, as well as the semitendinosus, have both been used as graft options for UCLR, although typically only 1 tendon is harvested when performing a UCLR as opposed to an ACLR, in which both tendons are commonly harvested. 32 Multiple studies have reported encouraging results when performing a UCLR with hamstring autograft. 3,34 Erickson et al 13 performed a study in which the authors compared palmaris longus autograft, hamstring autograft, and allograft as graft choices in UCLR to determine if differences in outcomes (RTS rate, clinical outcomes scores, and reoperation rates) existed between grafts. These authors found no significant difference in clinical outcome scores (Kerlan-Jobe Orthopaedic Clinic, Timmerman-Andrews), RTS rates, reoperations, or complications between graft choices. However, it is currently unclear which leg the hamstring graft should be harvested from in a baseball pitcher to minimize any effect the graft harvest may have on the pitching motion.
Harvesting the hamstring tendons leads to minimal acute graft site morbidity, such as leg soreness and the possibility of numbness in the distribution of the infrapatellar branch of the saphenous nerve. 32 However, a more significant issue with harvesting the hamstrings is persistent knee flexion weakness as well as weakness in internal rotation. 27,39,43 Konrath et al 27 reviewed 20 patients who underwent an ACLR using hamstring autograft and found that knee flexion, extension, and internal rotation strength were significantly lower in the leg where the hamstring had been harvested compared with the contralateral limb (all Ps <.05). The authors also noted that only 35% of patients showed regeneration of both the gracilis and semitendinosus on magnetic resonance imaging. Similarly, Tashiro et al 43 found significant knee flexion weakness after hamstring harvest for ACLR. Hence, the residual weakness present in the leg from which the graft was harvested may affect the pitcher’s throwing motion, as motion analysis studies have shown significant lower-extremity muscle activity during the pitching motion. 4 Therefore, mitigating this effect by harvesting the hamstring graft from the leg that contributes less to the overall pitch is imperative.
While a significant amount of research has focused on upper-extremity mechanics as it relates to the overhand pitch, much less attention has been paid to the lower extremity. 17 –23 However, the limited data that are available have shown significant muscle activation in the lower extremities during the baseball pitch. 4,25,31,45 These studies have found that, in pitching, ground reaction and braking forces are significant; and significant torques pass through the hip and knee that are created and balanced by the hamstrings, suggesting that these muscles are important for pitch velocity, command, and control. 4,25,31 Furthermore, Montgomery and Knudson 33 found that pitch speed could be increased by increasing the pitcher’s stride length, something that can be directly related to hamstring strength.
While the focus of the pitch is often the shoulder and elbow, a significant amount of the force necessary for velocity creation is generated in the legs and trunk and is then transferred up the body into the shoulder, elbow, and finally the ball. 4,25,30,31 The lower extremities are also important for balance and braking and may therefore be important for command and control. Therefore, loss of hip extensor and knee flexor power may not be trivial for an elite pitcher. As a result, appreciating which leg is more important to the overhand pitch and therefore which leg is optimal for hamstring autograft for a UCLR may lead to better postoperative outcomes. No current literature exists regarding this dilemma.
The results of the current study showed that significantly more MLB team orthopaedic surgeons harvest the hamstring for a UCLR from the landing leg. Furthermore, of the team orthopaedic surgeons who harvested the hamstring from the landing leg, the majority (72.4%) of them did so because they believe the landing leg is less important to the overhand pitch than the drive leg. Conversely, of the team orthopaedic surgeons who harvested the hamstring from the drive leg, the majority (63.6%) did so for logistical purposes in the operating room. Such logistical reasons can include operating simultaneously on the leg and elbow, inability to prep and drape contralateral extremities due to the size of the operating room, and others. Hence, only 10% of the surgeons surveyed believe the hamstrings from the landing leg are more important in generating a forceful baseball pitch (meaning only 4 surgeons responded that they would harvest the hamstring from the drive leg because they believed the hamstrings from the landing leg are more important in the baseball pitch). This is an important finding, as it shows that a majority of surgeons who care for elite-level baseball athletes believe the hamstrings of the drive leg to be more important than the hamstrings of the landing leg. While further studies evaluating muscle activation of the hamstrings of both legs during the baseball pitch are necessary to definitively answer this question, the expert opinion of MLB team physicians can help guide surgeons performing UCLR on baseball players in the interim.
Limitations
As with any survey study, this study has several limitations. These results are level 5 evidence and represent the opinions of team physicians from a single sport. While these physicians take care of athletes from all sports and have expertise in multiple areas, the questions were only aimed at baseball pitchers. Hence, the results may not be translatable to females, softball pitchers, athletes in other overhead sports, and others. There is the small possibility that a survey respondent clicked the wrong answer choice accidentally. This survey did not address all possible technique variables (whether the gracilis or semitendinosus was harvested) or rehabilitation protocols. Furthermore, although an exhaustive search was performed to locate all MLB team physicians, there are some who may have been missed.
Conclusion
When performing a UCLR using a hamstring autograft, the majority of MLB team physicians harvest the hamstring from the landing leg as opposed to the drive leg, as they believe the hamstring from the landing leg plays less of a role in generating a forceful pitch than the hamstring from the drive leg.
Footnotes
One or more of the authors has declared the following potential conflicts of interest or source of funding: J.R.D. receives royalties from Arthrex and Oakstone Publishing, is a paid consultant for Arthrex and Theralase, and has stock/stock options in Theralase and Topical Gear. B.R.B. is a team physician for the Chicago White Sox; receives research support from Arthrex, ConMed Linvatec, DJ Orthopaedics, Ossur, Smith & Nephew, and Tornier; and receives publishing royalties from SLACK Inc. G.P.N. is a physician for the Chicago White Sox, receives royalties from Innomed and SLACK Inc, is a paid consultant for Tornier, receives research support from Tornier, and has stock/stock options in Zimmer. N.N.V. is a team physician for the Chicago White Sox; receives research support from Arthrex, Arthrosurface, DJ Orthopaedics, Ossur, Smith & Nephew, Athletico, ConMed Linvatec, Miomed, and Mitek; has stock/stock options in Cymedica, Minivasive, and Omeros; is a paid consultant for Minivasive, Orthospace, and Smith & Nephew; and receives royalties from SLACK Inc, Smith & Nephew, and Vindico Medical-Orthopedics Hyperguide. C.S.A. is the head team physician for the New York Yankees, receives royalties from Arthrex, is a paid consultant or Athrex, has stock/stock options in At Peak, receives publishing royalties from Lead Player, and receives research support from Major League Baseball and Stryker. A.A.R. is a team physician for the Chicago White Sox; receives royalties from Arthrex and SLACK Inc; is a paid consultant for Arthrex; is a paid presenter or speaker for Arthrex; and receives research support from DJO Surgical, Ossur, and Smith & Nephew.
Ethical approval was not sought for the present study.