
Abstract
Background:
The medial collateral ligament (MCL) is the most frequently injured ligament of the knee, but it infrequently requires surgical treatment. Current literature on MCL reconstructions is sparse and offers mixed outcome measures.
Purpose/Hypothesis:
The purpose of this study was to compare the outcomes of isolated MCL reconstruction and multiligamentous MCL reconstruction. Our hypothesis was that in selective patients, MCL reconstruction would significantly improve objective and subjective patient knee performance measures, those being baseline valgus laxity, range of motion, objective and subjective International Knee Documentation Committee (IKDC) scores, Tegner score, and Lysholm knee activity scores.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines and utilizing 3 computer-based databases. Studies reporting clinical outcomes of patients undergoing MCL reconstruction due to chronic instability or injury with mean follow-up of at least 2 years and levels of evidence 1 to 4 were eligible for inclusion. All relevant subject demographics and study data were statistically analyzed using 2-sample and 2-proportion z tests.
Results:
Ten studies involving 275 patients met our inclusion criteria. Of these patients, 46 underwent isolated MCL reconstruction while another 229 underwent reconstruction of the MCL in addition to a variety of concomitant reconstructions. Overall outcomes for all patients were significant for (1) reducing the medial opening of the knee (8.1 ± 1.3 vs 1.4 ± 1.0 mm; P < .001), (2) improving the patient’s objective IKDC score (1.2% vs 88.4%; P < .001), (3) improving the patient’s subjective IKDC score (49.8 ± 6.9 vs 82.4 ± 9.6; P < .001), and (4) improving the Lysholm knee activity score (69.3 ± 5.9 vs 90.5 ± 6.6; P < .001). No differences existed between concomitant reconstruction groupings except that postoperative Lysholm scores were better for MCL/anterior cruciate ligament reconstruction than MCL/posterior cruciate ligament reconstruction (94.3 ± 4.5 vs 84.0 ± 11.7; P < .001). Normal or nearly normal range of motion was obtained by 88% of all patients.
Conclusion:
The systematic review of 10 studies and 275 knees found that the reported patient outcomes after MCL reconstruction were significantly improved across all measures studied, with no significant difference in outcomes between concomitant reconstructions.
Keywords
The medial collateral ligament (MCL) acts as the primary biomechanical restraint to valgus laxity against valgus stress at 0° and, importantly, at 30° of knee flexion. 5,6 MCL injury often occurs when an acute valgus load is applied and may occur as an isolated entity or in combination with a spectrum of multiligamentous involvment. 5,6
MCL injuries are the most frequent ligamentous injuries of the knee and can have either contact or noncontact mechanisms. 5,6,10 The majority are isolated sprains that can vary in severity. As the severity of the injury increases, so does the likelihood of injury to other associated ligamentous structures. A widely accepted grading classification groups MCL injuries by the opening of the medial joint line with valgus force while the knee is in 30° of flexion. Laxity of 1 to 5 mm, 6 to 10 mm, or >10 mm in comparison with the opposite knee are defined as grade 1, 2, or 3 injuries, respectively. High-energy injuries resulting in MCL injury frequently damage other knee ligaments in conjunction with the MCL. 6,10 In patients sustaining a grade 3 MCL injury, nearly 78% of patients had an injury to another associated structure. 11 Approximately 95% of these concomitant MCL injuries involve the anterior cruciate ligament (ACL). 12
When evaluating treatment plans, isolated grade 1 and 2 MCL injuries are treated nonoperatively with bracing, while grade 3 injuries may require surgical intervention with a repair or reconstruction. 5,6 The use of a long-leg hinged knee brace, early weightbearing, valgus versus varus overall alignment, and proximal injury may be factors that portend successful nonoperative MCL treatment. 5,6,10,21 Surgical intervention is often considered when patients do not respond to the initial nonoperative measures or when patients have chronic, persistent valgus instability and instability complaints within the coronal plane. 10 There are 2 primary surgical treatment options available: reconstruction or repair of the damaged ligament. In the senior author’s (B.R.B.) experience at a level 1 trauma center, it is exceedingly unusual to repair/reconstruct the MCL, as nonoperative intervention remains an effective treatment modality. There are some concomitant ligamentous injuries that can create a much more difficult problem to manage, as patients with MCL, posterior oblique ligament (POL), and posteromedial corner (PMC) injuries can go on to develop anteromedial rotatory instability (AMRI). Although this is extremely rare, this would likely lead to earlier surgical intervention than someone who has an isolated injury to their MCL. Despite the senior author (B.R.B.) having conducted nearly 2500 prior ACL reconstructions, only 25 patients have required MCL reconstruction, with the method of injury, severity, and presence of concomitant damage acting as key factors. Therefore, this systematic review was undertaken to provide further insight into such an infrequent procedure. The aim of this study was to systematically evaluate the clinical outcomes of patients undergoing primary MCL reconstruction to offer clinical recommendations for the procedure. We hypothesized that the outcomes of MCL reconstruction significantly improve objective and subjective patient knee performance measures (those being baseline valgus laxity, range of motion, objective and subjective International Knee Documentation Committee [IKDC] scores, and Tegner and Lysholm knee activity scores), and that there exists significant difference in outcomes among the various concomitant reconstructions.
Methods
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines using a PRISMA checklist. Systematic review registration was completed using the PROSPERO International prospective registrar of systematic reviews (registration number CRD42016045508, dated August 9, 2016). On July 5, 2016, a comprehensive literature search by 2 independent reviewers was conducted of 3 computer-based databases: PubMed, CINAHL, and Cochrane Central Registrar of Controlled Trials. The use of medical subject headings (MeSH) in conjunction with keywords was employed to obtain a large inclusionary search result from 1990 to July 2016. Search results were limited to those in English. The electronic search algorithm, composed of MeSH and keywords found in the title/abstract was as follows: ((“Outcome Assessment (Health Care)”[Mesh]) OR (outcome OR outcomes)) AND ((“Arthroplasty”[Mesh]) OR medial collateral ligament) NOT shoulder[Title/Abstract] NOT elbow[Title/Abstract] NOT animal model[Title/Abstract] AND English[Language]. Selection for study inclusion was determined by reviewing the title and abstract of each study. A minimum mean follow-up of 24 months was required for inclusion. Studies were excluded if they were duplicates, on irrelevant topics such as total knee arthroplasty or ligamentous reconstructions that did not include concomitant MCL reconstruction, articles comprising only abstracts or review articles, and studies that only discussed MCL repairs. The reference lists of included studies were considered for inclusion of additional studies missed by the initial search.
Once relevant studies were identified, the full text of the studies was obtained and analyzed. Patients of interest in this systematic review underwent MCL reconstruction for chronic instability or injury. Study and subject parameters collected included (1) level of evidence; (2) year of publication; (3) interval from injury to surgery; (4) length of follow-up; (5) demographics such as age, sex, and affected extremity; (6) whether magnetic resonance imaging (MRI) was obtained; (7) number of subjects; (8) concomitant procedures; (9) complications; (10) rehabilitation techniques; (11) surgical techniques; and (12) surgical failures. Clinical outcome scores included residual valgus laxity; IKDC objective, subjective, and valgus scores; Lysholm and Tegner knee activity scores; and range of motion.
Statistical Analysis
Descriptive statistics were calculated, and data values were reported as mean ± standard deviation for continuous variables and percentage frequencies for categorical variables. Statistical data aggregated from the qualifying studies or those directly reported from individual studies with a P value <.05 were deemed significant. A publicly available calculator (http://in-silico.net/tools/statistics/ztest/) was used to calculate the z score and P values. The quality and bias of the study methodology was calculated using the Modified Coleman Methodology Score (MCMS). The MCMS consists of 15 quality evaluations with scores scaled to a range of 0 to 100, where 0 to 55 = poor, 55 to 69 = fair, 70 to 84 = good, and 85 to 100 = excellent. Power analysis was performed.
Results
After implementation of the inclusion/exclusion criterion, 10 publications (see the Appendix) were identified from 2005 to 2016, with a total of 275 patients undergoing MCL reconstruction who met our inclusion criteria (Figure 1). 3,8,9,15 –19,28,29 There were 46 isolated MCL reconstruction procedures and 229 cases with concomitant reconstruction, including the ACL, posterior cruciate ligament (PCL), and/or posterolateral corner (PLC). Seventy-one percent of patients underwent a diagnostic MRI. Table 1 demonstrates the breakdown of concomitant reconstructions, and Table 2 depicts the types of grafts utilized. Meniscal repair or meniscectomy was performed on 61 (22.2%) patients, while microfracture for a cartilage lesion was performed on 2 (0.7%) patients, with severe articular cartilage injury seen in an additional 2 (0.7%) subjects. The chosen fixation methods consisted of metal interference screws, bioabsorbable interference screws, EndoButton (Smith & Nephew), screw and washer, and staples, the most common being bioabsorbable interference screws (64%).

Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart. MCL, medial collateral ligament.
MCL Reconstructions and Accompanying Concomitant Reconstructions a

a ACL, anterior cruciate ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner.
Choices of Graft Tissue Used in Medial Collateral Ligament Reconstruction a

a Graft selection is separated into preferences by each study and the corresponding total quantities.
These patients (69% male/31% female) had a mean age of 34.3 ± 10.8 years (range, 14-64 years). A mean 15.4 ± 11.5 months (range, 0.3-216 months) from initial injury to surgical reconstruction was observed. The mean follow-up time was 33.3 ± 11.1 months (range, 15-151.2 months).
The medial opening was reported in 5 of 10 studies, and was 8.1 ± 1.3 mm preoperatively (grade 2) and 1.4 ± 1.0 mm postoperatively (grade 1) (P < .001). Preoperatively, 1.2% (1/82) of patients had an objective IKDC grade of A or B (reported in 2 of 10 studies), whereas 88.4% (221/250) patients had a grade of A or B postoperatively (P < .001) (reported in 8 of 10 studies). The mean subjective IKDC preoperative score, reported by 4 of 10 studies, was 49.8 ± 6.9, with a postoperative mean of 82.4 ± 9.6 (P < .001). Patients also made significant improvements in their mean Lysholm knee activity scores, with preoperative values of 69.3 ± 5.9 and postoperative values of 90.5 ± 6.6 (P < .001), as reported by 5 of 10 studies. All studies reported that the vast majority of patients (88%) were able to return to normal or nearly normal range of motion, where abnormal was defined in the studies as a loss of extension greater than 6° or a loss of flexion greater than 10°. Of the 33 patients reporting a deficit in range of motion postreconstruction, only 27.2% experienced a loss in extension as opposed to 75.7% that lost at least 10° of flexion.
Where available, these same values were statistically compared between concomitant procedures and graft choices. All comparisons, including graft choices, had a significance of P > .05 except Lysholm knee activity scores between MCL/ACL reconstruction (94.3 ± 4.5) and MCL/PCL reconstruction (84.0 ± 11.7) (P < .001). A sample size of 592 patients was needed to detect a difference in IKDC objective grade A or B between ACL + MCL and PCL + MCL groups, with a power of 0.8 and P = .05. A post hoc power analysis for this outcome in the current study with the current sample size revealed a power 0.24. The reconstruction success rate was 98.2%, with 5 surgical failures being reported. Three of these failures, defined as postoperative objective IKDC scores of C or D, occurred within the MCL/PCL cohort. The 2 other failures were due to an MCL femoral insertion failure and an undescribed failure necessitating revision to pull the graft from the femoral tunnel. Complications included 5 infections ranging from superficial wound infections to 1 case of septic arthritis, 2 patients requiring knee stiffness release, 1 patient with a medial hematoma delaying wound healing, 4 patients reporting pain that was alleviated by the eventual removal of both screw and washer, and 2 patients reporting residual medial laxity.
A conflict of interest was reported in 1 study (10%) and was absent in the remaining 9 studies (90%). The majority of studies (90%) were level 4 evidence. Mean study quality, as evaluated by MCMS, was 41.3 (poor).
Discussion
A comprehensive review of the current literature revealed only 275 patients who underwent MCL reconstruction in the past 11 years, emphasizing the fact that MCL reconstructions are exceedingly uncommon procedures. Given the infrequency with which MCL reconstructions are performed and the lack of clinical evidence surrounding the results of these procedures, the aim of this study was to report quantitative outcomes of MCL reconstruction and to compare these outcomes across the most common concomitant reconstructions. All but 1 of our study hypotheses were confirmed, as objective clinical outcomes, including valgus laxity, range of motion, objective and subjective IKDC scores, and Lysholm scores were significantly improved after MCL reconstruction. The data were not sufficient to comment on Tegner knee activity scores. A significant difference between concomitant procedures and graft choices was found among only 1 outcome variable comparing MCL/ACL reconstruction and MCL/PCL reconstruction, leaving no statistical conclusions available to be made.
The incidence of MCL injuries has continued to increase over the past several years as a result of growing participation in sports such as skiing, ice hockey, and football, all of which involve valgus forces to the knee. 5,21 With the rising prevalence, knowledge of current, effective prevention and treatment modalities becomes increasingly significant. Some studies have shown that prophylactic bracing confers reduced risk for MCL injury to football linemen, while others have shown no benefit, specifically to skill players. 1,2,10,20,24 Regardless of preventative practices, these injuries still occur frequently. Once a patient sustains an MCL injury, nonoperative management, MCL repair, and MCL reconstruction are all viable options for treatment. With appropriate nonoperative treatment, grade 1 and 2 injuries often heal in a matter of weeks, while grade 3 injuries may require a year or longer. 27 Reconstruction or repair of the MCL is a relatively uncommon procedure, as nonoperative treatment is often successful at returning the patients to their prior level of function.
Currently, the majority of MCL literature focuses on nonoperative treatments, including bracing and physical therapy, as nonoperative treatment has shown to be largely successful, with long-term nonoperative outcomes often on par with early reconstruction in the MCL/ACL cohort. 5,6,10,13 This demographic is one commonly seen in the clinical setting, as nearly 95% of concomitant MCL injuries include the ACL. 12 In this review, only 70.0% (159 knees) of concomitant procedures were MCL/ACL reconstructions, lower than the reported 95% due to the inclusion criteria of certain studies focusing on predetermined ligament groupings. However, many studies included in this review did describe an initial attempt to manage MCL injuries with nonoperative treatment prior to surgery. Surgical intervention in these patients was considered only after the patients had failed nonoperative treatment.
Failure of nonoperative treatment can result in debilitating, persistent medial instability, secondary dysfunction of the ACL, weakness, and osteoarthritis. 14 Thus, patients with chronic valgus laxity who have failed a course of nonoperative treatment or who have suffered multiligamentous knee injuries are the most frequent candidates for surgical correction. 5,6,10 The indication for MCL reconstruction compared with MCL repair is based on the remaining quality of the native ligament and the length of time since the injury. 21 A ligament beyond repair requires reconstruction with an autograft or allograft. In this review, the most common surgical indications were chronic laxity due to repeated injury and/or failure of nonoperative treatment.
When MCL reconstruction is indicated in multiligamentous knee injuries, one must decide whether to fix all ligaments concomitantly or in a staged fashion. It is possible that surgical reconstruction of any concomitantly injured cruciate ligaments would sufficiently correct a patient’s medial laxity so as to avoid MCL reconstruction, further complicating the surgical decision-making process. 13,27 Since the MCL is made of 2 components, an anterior and a posterior, this phenomenon can occur in the face of a normal or near-normal valgus stress test at full extension and would indicate an intact posterior MCL. 25 Previous studies have found that when the ACL is reconstructed early, there are often no significant differences in outcomes between subsequently reconstructing the MCL and opting for nonoperative treatment. 13 Nonetheless, MCL reconstructions are frequently performed concomitantly with cruciate ligament or other ligament reconstructions, as was observed in this review.
At a mean 33 months postsurgery, this systematic review found that there was significant improvement in the outcomes of patients undergoing MCL reconstruction, as measured by the medial knee opening, both objective and subjective IKDC scores, Lysholm knee activity scores, and range of motion. Comparison across varying concomitant procedures, including isolated MCL reconstruction, MCL/ACL reconstruction, and MCL/PCL reconstruction, found that postoperative Lysholm activity scores of MCL/ACL reconstructions (94.3 ± 4.5) were significantly higher than those of the MCL/PCL reconstructions (84.0 ± 11.7) (P < .001). A multitude of variables, including surgical technique, rehabilitation procedures, and the anatomic relationship of the ligaments, could account for this discrepancy.
Differences in reconstruction techniques were evident between the reviewed studies. Common techniques included isolated anatomic reconstruction of the superficial MCL (sMCL) or combined reconstruction of both the sMCL and POL. Two studies introduced new techniques. 3,29 One comprised an anatomic reconstruction of the sMCL and PCL using a single femoral tunnel, while another described a tibial inlay technique specifically tailored for the MCL. The studies reviewed included a variety of graft choices, with hamstring autograft, quadriceps tendon autograft, Achilles allograft, and hamstring allograft all previously reported as viable options, with no definitive evidence to support 1 graft or technique over another. 21,27 Graft selection often stems from the extent of the injury and the graft availability. An allograft is typically recommended in multiligamentous injuries, as it eliminates graft site morbidity, reduces dissection time, and decreases postoperative pain and stiffness. 22 However, allografts introduce an added cost and carry a risk of disease transmission. 22 If an autograft is chosen, the hamstring tendons, either ipsilateral or contralateral, are readily available and easily harvested. The grafts most used by the surgeons of the reviewed studies were Achilles tendon allografts and semitendinosus tendon autografts. Two studies reported the implementation of different grafts: a tibialis anterior tendon allograft and a nondescript allograft. The senior author (B.R.B.) uses an Achilles allograft for chronic medial instability, while the majority of total patients included in this review received a semitendinosus autograft.
In addition to the chosen grafts and techniques, fixation methods also varied among the included studies. These fixation methods consisted of metal interference screws, bioabsorbable interference screws, EndoButton screw and washer, and staples. It has been well established that fixation methods are essential to limit graft loosening and residual instability. 26 Current literature for Achilles allografts in particular recommends the use of metal interference screws for fixation at the proximal end in conjunction with optional EndoButton fixation. 23 The distal allograft is commonly secured with staples, while screw-and-washer constructs are sometimes used in osteopenic patients. 23 Reconstruction using semitendinosus autograft often follows a similar method of fixation. However, novel methods such as an adjustable-loop suspensory fixation have been introduced for femoral fixation. 7 Nonetheless, this study found the most common fixation method was interference screws, with bioabsorbable more common than metal.
With the overwhelming majority of concomitant MCL injuries occurring in association with ACL injuries, it is important to note that combined reconstruction of the MCL and ACL is associated with an increased prevalence of postoperative arthrofibrosis. 4,11,12 This suggests that staging the reconstructive procedures may provide beneficial outcomes for patients with regard to knee range of motion. 4 While concomitant injury to the ACL was extremely common, there were other concomitant ligamentous injuries included in this study. It should be understood that injuries to the MCL, PMC, and POL can produce AMRI, and will require earlier surgical intervention to prevent valgus laxity and hyperextension. The surgical treatment for each patient must be tailored to the specific injury pattern, as no single algorithm can encompass all injury patterns and all patient factors. Further investigations into which method best improves outcomes and reduces arthrofibrotic complications are required, as this study lacked a sufficient quantity of patients and comparable outcome parameters to meaningfully compare patient outcomes between isolated MCL reconstruction and MCL/ACL reconstruction.
Limitations
Although we attempted to locate each study measuring outcomes from MCL reconstruction, the search design did not include studies in a language other than English and did not include gray literature. This may have introduced a selection bias. The overall quality of the included studies also draws our findings into question, as 90% were level 4 studies lacking control groups, with a poor average MCMS score. This is an inherent limitation of the systematic review, as we are limited to data from already published articles. Furthermore, several studies focused on 1 or 2 specific concomitant procedures, while others chose to investigate a diverse conglomerate of differing concomitant procedures. Within these differing studies, the measured outcome variable also differed. This generated some concern in the data analysis of the qualifying patients, as certain variables may have only been recorded across 3 or fewer studies. Additionally, given the infrequency of the surgical procedure, a mean sample size of 27.5 patients does not appropriately lend itself for robust data analysis. These factors contributed to this review being underpowered. Moreover, the exact timing of surgery for the various types of concomitant injuries could not reliably be determined, as this was not separated out in the individual studies that were included. Hence, the time from injury to surgical intervention for some of the MCL injuries with concomitant injuries to the PLC, PMC, POL, and so forth may have been much sooner, but the timing for these groups could not be isolated. Postoperative rehabilitation, a factor that may influence measured outcomes during follow-up, was not homogenous and often varied by the preferences of the surgeon and the type of concomitant procedure conducted. There were some aspects of the physical examination and injury patterns that were not reported in the individual articles and therefore could not be analyzed in our review. This adds in the possibility of a reporting bias.
Conclusion
The systematic review of 10 studies and 275 knees found that the reported patient outcomes after MCL reconstruction were significantly improved across all measures, those being baseline valgus laxity, range of motion, objective and subjective IKDC scores, and Lysholm knee activity scores, with no significant difference in outcomes between concomitant reconstructions.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.R.B. receives research support from Arthrex, ConMed Linvatec, DJ Orthopaedics, Ossur, Smith & Nephew, and Tornier and receives publishing royalties from SLACK Inc.
Appendix
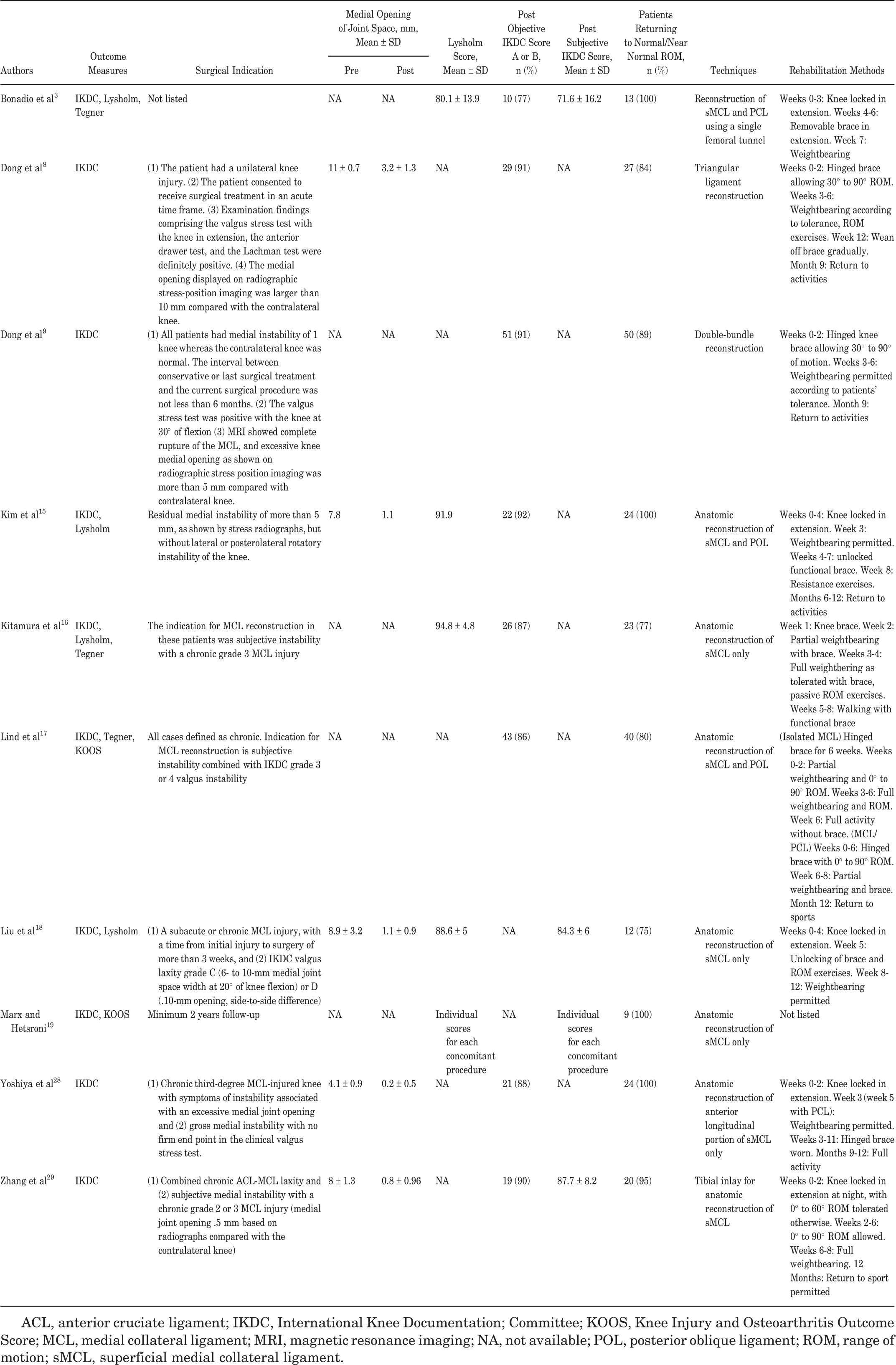
| Medial Opening of Joint Space, mm, Mean ± SD | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Authors | Outcome Measures | Surgical Indication | Pre | Post | Lysholm Score, Mean ± SD | Post Objective IKDC Score A or B, n (%) | Post Subjective IKDC Score, Mean ± SD | Patients Returning to Normal/Near Normal ROM, n (%) | Techniques | Rehabilitation Methods |
| Bonadio et al 3 | IKDC, Lysholm, Tegner | Not listed | NA | NA | 80.1 ± 13.9 | 10 (77) | 71.6 ± 16.2 | 13 (100) | Reconstruction of sMCL and PCL using a single femoral tunnel | Weeks 0-3: Knee locked in extension. Weeks 4-6: Removable brace in extension. Week 7: Weightbearing |
| Dong et al 8 | IKDC | (1) The patient had a unilateral knee injury. (2) The patient consented to receive surgical treatment in an acute time frame. (3) Examination findings comprising the valgus stress test with the knee in extension, the anterior drawer test, and the Lachman test were definitely positive. (4) The medial opening displayed on radiographic stress-position imaging was larger than 10 mm compared with the contralateral knee. | 11 ± 0.7 | 3.2 ± 1.3 | NA | 29 (91) | NA | 27 (84) | Triangular ligament reconstruction | Weeks 0-2: Hinged brace allowing 30° to 90° ROM. Weeks 3-6: Weightbearing according to tolerance, ROM exercises. Week 12: Wean off brace gradually. Month 9: Return to activities |
| Dong et al 9 | IKDC | (1) All patients had medial instability of 1 knee whereas the contralateral knee was normal. The interval between conservative or last surgical treatment and the current surgical procedure was not less than 6 months. (2) The valgus stress test was positive with the knee at 30° of flexion (3) MRI showed complete rupture of the MCL, and excessive knee medial opening as shown on radiographic stress position imaging was more than 5 mm compared with contralateral knee. | NA | NA | NA | 51 (91) | NA | 50 (89) | Double-bundle reconstruction | Weeks 0-2: Hinged knee brace allowing 30° to 90° of motion. Weeks 3-6: Weightbearing permitted according to patients’ tolerance. Month 9: Return to activities |
| Kim et al 15 | IKDC, Lysholm | Residual medial instability of more than 5 mm, as shown by stress radiographs, but without lateral or posterolateral rotatory instability of the knee. | 7.8 | 1.1 | 91.9 | 22 (92) | NA | 24 (100) | Anatomic reconstruction of sMCL and POL | Weeks 0-4: Knee locked in extension. Week 3: Weightbearing permitted. Weeks 4-7: unlocked functional brace. Week 8: Resistance exercises. Months 6-12: Return to activities |
| Kitamura et al 16 | IKDC, Lysholm, Tegner | The indication for MCL reconstruction in these patients was subjective instability with a chronic grade 3 MCL injury | NA | NA | 94.8 ± 4.8 | 26 (87) | NA | 23 (77) | Anatomic reconstruction of sMCL only | Week 1: Knee brace. Week 2: Partial weightbearing with brace. Weeks 3-4: Full weightbering as tolerated with brace, passive ROM exercises. Weeks 5-8: Walking with functional brace |
| Lind et al 17 | IKDC, Tegner, KOOS | All cases defined as chronic. Indication for MCL reconstruction is subjective instability combined with IKDC grade 3 or 4 valgus instability | NA | NA | NA | 43 (86) | NA | 40 (80) | Anatomic reconstruction of sMCL and POL | (Isolated MCL) Hinged brace for 6 weeks. Weeks 0-2: Partial weightbearing and 0° to 90° ROM. Weeks 3-6: Full weightbearing and ROM. Week 6: Full activity without brace. (MCL/PCL) Weeks 0-6: Hinged brace with 0° to 90° ROM. Week 6-8: Partial weightbearing and brace. Month 12: Return to sports |
| Liu et al 18 | IKDC, Lysholm | (1) A subacute or chronic MCL injury, with a time from initial injury to surgery of more than 3 weeks, and (2) IKDC valgus laxity grade C (6- to 10-mm medial joint space width at 20° of knee flexion) or D (.10-mm opening, side-to-side difference) | 8.9 ± 3.2 | 1.1 ± 0.9 | 88.6 ± 5 | NA | 84.3 ± 6 | 12 (75) | Anatomic reconstruction of sMCL only | Weeks 0-4: Knee locked in extension. Week 5: Unlocking of brace and ROM exercises. Week 8-12: Weightbearing permitted |
| Marx and Hetsroni 19 | IKDC, KOOS | Minimum 2 years follow-up | NA | NA | Individual scores for each concomitant procedure | NA | Individual scores for each concomitant procedure | 9 (100) | Anatomic reconstruction of sMCL only | Not listed |
| Yoshiya et al 28 | IKDC | (1) Chronic third-degree MCL-injured knee with symptoms of instability associated with an excessive medial joint opening and (2) gross medial instability with no firm end point in the clinical valgus stress test. | 4.1 ± 0.9 | 0.2 ± 0.5 | NA | 21 (88) | NA | 24 (100) | Anatomic reconstruction of anterior longitudinal portion of sMCL only | Weeks 0-2: Knee locked in extension. Week 3 (week 5 with PCL): Weightbearing permitted. Weeks 3-11: Hinged brace worn. Months 9-12: Full activity |
| Zhang et al 29 | IKDC | (1) Combined chronic ACL-MCL laxity and (2) subjective medial instability with a chronic grade 2 or 3 MCL injury (medial joint opening .5 mm based on radiographs compared with the contralateral knee) | 8 ± 1.3 | 0.8 ± 0.96 | NA | 19 (90) | 87.7 ± 8.2 | 20 (95) | Tibial inlay for anatomic reconstruction of sMCL | Weeks 0-2: Knee locked in extension at night, with 0° to 60° ROM tolerated otherwise. Weeks 2-6: 0° to 90° ROM allowed. Weeks 6-8: Full weightbearing. 12 Months: Return to sport permitted |
ACL, anterior cruciate ligament; IKDC, International Knee Documentation; Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; MCL, medial collateral ligament; MRI, magnetic resonance imaging; NA, not available; POL, posterior oblique ligament; ROM, range of motion; sMCL, superficial medial collateral ligament.