
Abstract
Background:
Subcircumferential periosteal edema above the ankle joint is frequently present on magnetic resonance imaging (MRI) with syndesmosis injuries but has not been previously reported. Fluid height within the interosseous membrane also has not previously been shown to be associated with syndesmosis injury severity.
Purpose:
To investigate whether a new sign on MRI and measurement of the length of fluid within the interosseous membrane above the ankle may be used to enable identification of a syndesmosis injury and allow differentiation from lateral ligament injury.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Three groups of patients (those with an isolated syndesmosis injury [SI group], isolated lateral ligament injury [LLI group], and no injury [NI group]) who had an ankle MRI for another reason were identified from a patient notes database and the MRI scans retrieved. The scans were anonymized and independently assessed by 8 clinicians (surgeons and radiologists) who were blinded to the diagnosis. The maximum length of fluid above the ankle within the intraosseous membrane was measured for each patient. The presence or absence of distal anterior, lateral, and posterior tibial periosteal edema was recorded (broken “ring of fire”).
Results:
Measurement of the length of fluid above the ankle had excellent intraobserver reliability (intraclass correlation coefficient, 0.97; 95% CI, 0.93-0.99) but poor interobserver reliability. Fluid extended higher in both the LLI group (P = .0043) and SI group (P = .0058) than the NI group, but there was no significant difference between the LLI and SI groups (P = .3735), indicating that this measurement cannot differentiate between the injuries. The presence of the broken “ring of fire” around the distal tibia was significantly more frequent in the SI group when compared with both LLI and NI groups (P < .00001). The sensitivity of this sign is 49%, but when present, this sign has a 98% specificity for syndesmosis injury.
Conclusion:
The presence of tibial subcircumferential periosteal edema 4 to 6 cm above the ankle joint (the “ring of fire”) is highly suggestive of a syndesmosis injury. This new radiological sign can assist with early identification of such injuries. The measurement of height of fluid above the ankle within the interosseous membrane is variable and cannot differentiate severe ankle sprains from high ankle sprains involving the syndesmosis.
Keywords
Ankle syndesmosis injuries are a cause for delayed return to sport and are associated with ankle pain and long-term disability if the diagnosis is delayed or unrecognized. 8,20,24 The mechanism of injury and the presence of high ankle pain may alert the treating clinician to the presence of a syndesmosis injury rather than a “simple” lateral ligament sprain. 2,6,7,12,14,25,26 However, frequently, the history of injury and the clinical signs may be confusing. Plain radiographs may show instability of the syndesmosis in high-grade unstable injuries, but the most frequent injuries encountered in sports are the more subtle syndesmosis injuries (referred to as sprains by some authors). 4 Delay in appropriate treatment of these injuries may lead to long-term adverse sequelae. 1,3,10,11,13,17 –19,23
Injury to the anterior and posterior inferior tibiofibular ligaments (AITFL and PITFL, respectively) and the interosseous ligament (IOL) may be accurately identified on magnetic resonance imaging (MRI). 9,12,15,21,22 However, previous injuries to these ligaments with thickening and fibrosis demonstrated on MRI with associated edema proximally from the anterior talofibular ligament (ATFL) injury in a supination-inversion ankle injury may lead to uncertainty as to the presence of an acute syndesmosis injury requiring specific treatment. The presence of subcircumferential edema was noticed on MRI around the tibia 4 to 6 cm above the ankle joint in patients with a syndesmosis injury. We had not observed this in patients with injury only to the ATFL. We also observed significant edema or extrusion of joint fluid along the interosseous membrane proximal to the ankle joint. We considered this subcircumferential edema, which has not previously been described and which we termed the broken ring of fire (RoF), may be a diagnostic sign for syndesmosis injury, and measurement of the length of bleeding along the interosseous membrane may correlate with the presence of a syndesmosis injury and aid in the early recognition of such injuries.
The aim of this study was to assess whether identifying the broken RoF or measuring the height of bleeding into the interosseous membrane were useful signs in the early detection of a syndesmosis injury and whether they could help differentiate such injuries from lateral ligament injuries isolated to the ATFL.
Methods
MRI scans of patients with an isolated syndesmosis and isolated lateral ligament injuries were identified from a patient notes electronic database. All those with a syndesmosis injury (SI group) had a grade II injury according to the West Point Classification. 8 Diagnosis of syndesmosis injury was made by a combination of clinical examination (by a foot and ankle orthopaedic consultant surgeon) and MRI scan using traditional methods of diagnosing syndesmosis injury: edema and ligamentous disruption demonstrated on axial and coronal images. Those with an isolated lateral ligament injury (LLI group) had injury to the ATFL alone or ATFL and calcaneofibular ligament (CFL). A third group of patients were identified with no history of injury to the syndesmosis or lateral ligament complex (NI group). These patients underwent MRI scanning for unrelated conditions such as osteochondral lesion of the talus or Achilles tendon injury. Identifying features were removed from the scans, which were then randomly listed for review.
Imaging was performed in a number of centers. Although the imaging parameters were not completely standardized, axial imaging included either a short tau inversion recovery series (STIR) or proton density fat saturation (PDFS) of a T2-weighted image. The MRI scanners had a magnetic strength of 1.5 T. All sequences were able to identify edema, enabling the diagnosis of subcircumferential edema with confidence.
Eight clinicians (radiologists and surgeons) were blinded to the diagnosis and independently reviewed all scans. There were 2 fellowship-trained consultant orthopaedic surgeons, 1 musculoskeletal radiologist, 2 senior foot and ankle orthopaedic fellows, and 3 senior orthopaedic residents. All were asked to assess the axial imaging for the presence or absence of subcircumferential edema around the tibia in any of the slices between 4 and 6 cm proximal to the ankle joint having been shown examples of the RoF (Figure 1). They were also asked to measure the height of fluid (representing edema or joint fluid) above the ankle joint (Figure 2). The coronal view used to measure the fluid height was standardized to be in line with the center of the syndesmosis on the anteroposterior/lateral plane. The height was remeasured on 12 scans on a separate occasion to assess intraobserver reliability.

Example of the broken “ring of fire” (red arrow). Axial T2-weighted fat-saturated magnetic resonance image from a patient in the syndesmosis injury (SI) group.

Measurement of height of fluid within syndesmosis (red arrow and lines). Coronal T2-weighted fat-saturated magnetic resonance image from a patient in the syndesmosis injury (SI) group.
Statistical advice was sought from the Department of Biostatistics, Eastman Institute, University College London, UK, and statistical analysis was performed using SPSS software (SPSS Statistics for Windows, version 22.0; IBM Corp). A pilot study was performed with 9 scans in each group, and a subsequent power study concluded that a minimum of 18 patients would be required in each group with a power of 80% and alpha value 0.05.
The presence/absence of the RoF was analyzed using the chi-square test as well as the sensitivity, specificity, and positive/negative predictive values. Reliability testing was performed on measurements of the height of fluid above the ankle using intraclass correlation coefficients (ICCs) on the 12 scans that underwent repeat testing. This result was interpreted according to Cicchetti 5 (Table 1). The Kruskal-Wallis test was used to assess differences in the distributions of height, with the null hypothesis (H0) stating that there is no difference in the heights between the groups with an alpha level of 0.05 and a critical value of 5.99147. The Mann-Whitney U test for nonnormally distributed data was used to assess differences between the distributions of each group, with a significance level of P < .05.
Qualitative Ratings of Agreement Based on ICC Values a

a Table adapted from Cicchetti. 5 ICC, intraclass correlation coefficient.
Results
A total of 98 suitable scans were identified and included in the study: 22 in the SI group, 31 in the LLI group, and 45 in the NI group.
Assessment of the Ring of Fire
Subcircumferential edema of the distal tibial periosteum was named the broken RoF.
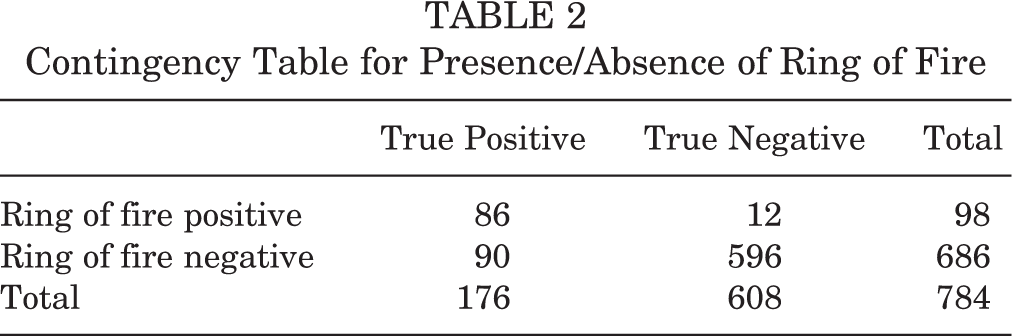
The results of the presence or absence of the RoF are summarized in Table 2. The RoF was present more frequently in those with a syndesmosis injury than without (P < .001) and significantly more frequently than in those with a lateral ligament Injury (P < .001) (Table 3). Although the RoF had a sensitivity of predicting a syndesmosis injury of 49%, it had a false positive rate of 1.4% in the NI group and 2.8% in the LLI group. Overall, it had a specificity of 87%, with a negative predictive value of 98% and a positive predictive value of 88%.
Contingency Table for Presence/Absence of Ring of Fire
Chi-Square Results for Ring of Fire a

a LLI, lateral ligament injury; NI, no injury; SI, syndesmosis injury.
Assessment of Height of Fluid in the Interosseous Membrane
The distribution of the height measurements is summarized in Table 4. Intraobserver reliability testing resulted in an ICC of 0.97 (95% CI, 0.93-0.99), representing excellent reliability for the measurement of height. However, for interobserver reliability, the ICC was 0.49 (95% CI, 0.21-0.75), indicating only fair reliability between observers (Table 5). The Kruskal-Wallis test demonstrated that H0 failed to exceed 5.99, and therefore, the null hypothesis was accepted and there was no significant difference between groups. The data were checked for normality, and there was a nonnormal distribution with skew to the right. The Mann-Whitney U test demonstrated a significant difference in height between both the LLI and SI groups when individually compared with the NI group (P = .0043 and P = .0058, respectively) but no difference in height between the SI and LLI groups (P = .3735).
Measurement of Height for All Groups, in mm a

a LLI, lateral ligament injury; NI, no injury; SI, syndesmosis injury.
Reliability Testing for Measurement of Height of Fluid in Syndesmosis a

a ICC, intraclass correlation coefficient.
Discussion
The most important finding of this study is that the presence of the broken RoF sign on MRI may alert the clinician to the possibility of a syndesmosis injury and may be helpful in differentiating this high ankle sprain from the more common isolated lateral ligament injury. This may be considered as a diagnostic sign as it has a high specificity, although its absence does not exclude a syndesmosis injury since it has a sensitivity of only 49%. This has similar sensitivities and specificities as the Segond fracture has to anterior cruciate disruption. 10 We suggest that the broken RoF only occurs when there has been sufficient trauma to disrupt part of the intraosseous membrane, which leads to bleeding proximally and circumferentially around the tibia. We conclude that this does not occur when the ATFL or CFL are injured in isolation. We recommend that scans are assessed for this sign 4 to 6 cm proximal to the ankle joint to reduce the likelihood of a concomitant ankle capsular injury giving a false positive sign. We would suggest all ankle imaging extends to this level. It is noted that the maximum height of fluid extension into the syndesmosis in the NI and LLI groups was 34.1 and 32.6 mm, respectively, reinforcing our opinion that observation of the RoF should be sought above 4 cm. When this new sign is identified on a scan, its specificity should alert the clinician to the possibility of syndesmosis injury so that careful clinical assessment may be made as to the stability of the injury and appropriate management commenced.
Measurement of the height of edema/extrusion of joint fluid within the syndesmosis, although reproducible within observers, appears open to individual interpretation and it does not appear to be reliable. This variation between observers means that it is not an accurate method of assessment for syndesmosis injury. Fluid extruded proximally within the interosseous membrane in both the LLI and SI groups, which we presume is due to bleeding from the AITFL/ATFL injury or joint fluid from an associated capsular tear. Although the maximum height was 34 mm in the LLI group and 59 mm in the SI group, there does not appear to be a threshold above which this measurement is significant. In addition to the unacceptable variability between observers, measurement of this height cannot be used to differentiate a syndesmosis from isolated lateral ligament injury, as no significant difference between these groups could be demonstrated.
The limitations of this study include its retrospective nature and that although the patient notes indicated the diagnosis of isolated grade II syndesmosis injury, only some patients underwent arthroscopic confirmation of this diagnosis. Although the observers were shown examples of the RoF sign and measurement of the fluid height was demonstrated, it could be argued that further experience after feedback from these data could improve the interobserver reliability. Nussbaum et al 16 demonstrated that the length of tenderness on palpation along the anterior aspect of the interosseous membrane is associated with a longer recovery after syndesmosis injury. It would have also been interesting to have clinical follow-up data to see whether the height of fluid correlates with a poorer outcome.
Conclusion
The presence of subcircumferential periosteal edema around the tibia 4 to 6 cm above the ankle joint (the broken “ring of fire”) is highly suggestive of a syndesmosis injury. This new radiological sign can assist with early identification of such, especially in recurrent injuries. The measurement of the height of the fluid above the ankle within the interosseous membrane is variable and cannot differentiate severe ankle sprains from high ankle sprains involving the syndesmosis.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was waived by the Fortius Clinic.