
Abstract
Background:
Gluteal tendinopathy is a common cause of lateral hip pain, and existing conservative treatment modalities demonstrate high symptom recurrence rates. Autologous tenocyte injection (ATI) is a promising cell therapy that may be useful for the treatment of gluteal tendinopathy.
Purpose:
To investigate the safety and effectiveness of ATI, specifically in patients with chronic recalcitrant gluteal tendinopathy.
Study Design:
Case series; Level of evidence, 4.
Methods:
Twelve female patients with a clinical and radiological diagnosis of gluteal tendinopathy were recruited. Patients demonstrated a mean duration of symptoms of 33 months (range, 6-144 months), had undergone a mean 3.2 prior corticosteroid injections (range, 2-5), and had failed to respond to existing conservative treatments including physiotherapy and injections. In an initial procedure, tendon cells were harvested from a needle biopsy of the patella tendon and propagated in a certified Good Manufacturing Practice (GMP) laboratory. In a secondary procedure, a single injection of 2 mL autologous tenocytes (2-5 × 106 cells/mL) suspended in patient serum was injected into the site of the pathological gluteal tendons under ultrasound guidance. Patients were assessed pre- and postinjection (3, 6, 12, and 24 months) using the Oxford Hip Score (OHS), a visual analog pain scale (VAS), the Short Form–36 (SF-36), and a satisfaction scale. Magnetic resonance imaging (MRI) was undertaken at 8.7 months (range, 6-12 months) postinjection.
Results:
Molecular characterization of autologous tendon cells showed a profile of growth factor production in all cases, including platelet-derived growth factor α, fibroblast growth factor β, and transforming growth factor β. The OHS (mean, 24.0 preinjection to 38.9 at 12 months [14.9-point improvement]; 95% CI, 10.6-19.2; P < .001), VAS (mean, 7.2 preinjection to 3.1 at 12 months [4.1-point improvement]; 95% CI, 2.6-5.6; P < .001), and SF-36 (mean, 28.1 preinjection to 43.3 at 12 months [15.2-point improvement]; 95% CI, 9.8-20.5; P < .001) significantly improved to 12 months postinjection, sustained to 24 months. Eight patients were satisfied with their outcomes. Significant MRI-based improvement could not be demonstrated in the majority of cases.
Conclusion:
ATI for gluteal tendinopathy is safe, with improved and sustained clinical outcomes to 24 months.
Keywords
Greater trochanteric pain syndrome (GTPS) is a term used to define the clinical condition of greater and peritrochanteric hip pain and tenderness, 12 –14,17,23,28 affecting 10% to 25% of the general population. 18,23,28 While previously reported as trochanteric bursitis, gluteus medius and/or minimus tendinopathy is now accepted as the most prevalent pathology in those with pain and tenderness over the greater trochanter. 11 Histological changes in tendinopathy include decreased and disorganized collagen production, deposition of adipose tissue, vascular hyperplasia characterized by an absence of polymorphonucleocytes, variation in cell populations, and disruption of the extracellular matrix. 29 Apoptosis and autophagic tendon cell death occurs in more severe cases, 3 and increased cell death rates in chronic lateral epicondylitis and rotator cuff tendinopathy indicate that the healing process is suppressed by a lack of cellular components. 24 The depleted cell population and reduced collagen synthesis accelerate collagen deterioration, compromising the ability of the tendon to maintain structural integrity. 29
Conservative treatments for gluteal tendinopathy may include rest, anti-inflammatory medication, ice and/or heat, physical therapy, shock wave therapy, ultrasound, and local corticosteroid injections. 8,15,22,28 However, a high symptom recurrence rate at 1 year has been demonstrated for all conservative treatment modalities in primary care, 18 and patients frequently undergo multiple courses of nonoperative treatment with only temporary pain relief. 19 Autologous tenocyte injection (ATI) is a novel cell therapy that has shown restoration of functional tendon cells in animal studies. 4,5 Clinical and radiological improvement was documented in a single case report employing ATI for rotator cuff tendinopathy, 26 while significant clinical and radiological improvement was reported in a pilot study investigating ATI for chronic lateral epicondylitis, 24,25 demonstrating a sustained reduction in pain and improvement in function to 4.5 years postinjection in patients who had failed nonoperative treatment. 24,25 The aim of this pilot study was to investigate whether ATI is safe and effective in more troublesome patients with clinical and radiological diagnoses of gluteal tendinopathy who had failed to respond to other nonsurgical treatments. We hypothesized (1) that ATI is safe and well tolerated by patients and (2) that patients will demonstrate a significant clinical improvement sustained to 24 months postinjection.
Methods
Participants
The first 12 patients (all female) that fit the below inclusion/exclusion criteria were offered ATI as part of this pilot trial, all recruited from a single orthopaedic surgeon’s (G.C.J.) practice, with none refusing treatment. All patients had symptomatic gluteal tendinopathy and had previously undergone unsuccessful attempts at nonoperative measures, including image-guided steroid injections into the greater trochanteric bursa (n = 12; mean, 3.2 injections; range, 2-5), platelet-rich plasma (PRP) (n = 4), and physiotherapy (n = 12). After failure of other nonoperative measures, patients were clinically assessed by a consultant orthopaedic surgeon and underwent magnetic resonance imaging (MRI) to confirm the diagnosis of gluteal tendinopathy as well as ensure the absence of a high-grade partial- or full-thickness gluteal tendon tear. Patients were excluded if they had undergone previous hip and/or gluteal repair surgery, had hip osteoarthritis, and/or received steroid injections within the preceding 3 months. The mean age of patients was 52.6 years (range, 41-67 years), with an average duration of symptoms of 33 months (range, 6-144 months) (Table 1). Prior to treatment, all patients were counseled regarding the procedure(s), possible risks, and postinjection recovery before consenting to ATI and completing study documentation. Ethical approval was obtained, and all study procedures were undertaken according to the Declaration of Helsinki 1975.
Patient Demographics and the Oxford Hip Score (OHS) at Baseline (Preinjection) and 12 Months Postinjection a

a L, left; N/A, not applicable; R, right.
Patella Tendon Biopsy
Under sterile conditions, the patella tendon was marked, and a suitable area was infiltrated with local anesthetic. Under ultrasound, a 14-gauge Tru-Cut needle was placed in the patella tendon, and 2 biopsy specimens were taken. Tendon tissue was placed in transport medium (DMEM F12 with 20% fetal bovine serum). As part of the Code of Good Manufacturing Practice (GMP) for human blood and tissues (2000) protocol, a 60-mL sample of venous blood was taken for infection and viral screening, including: human immunodeficiency virus, hepatitis B and C, human T-lymphotropic virus, and syphilis. Patients were allowed immediate full weightbearing after the patella tendon biopsy but were advised to limit strenuous activities for 48 hours. The same consultant radiologist performed all procedures.
Cultivation of Autologous Tenocytes
Tenocyte cultivation was performed at Orthocell Ltd. The tendon tissue was digested enzymatically to extract the tenocytes. These cells were expanded by in vitro culture in a certified Therapeutic Goods Administration (TGA)–licensed facility. Tenocytes used for implantation were characterized by quantitative real-time polymerase chain reaction (PCR). It has previously been reported that this technique maintains the tenocyte phenotype. 4,5
Quantitative Real-Time PCR
Previously, we have analyzed the profile of tendon-derived cells and identified that they contain progenitor cells that differ from bone marrow mesenchymal stem cells and fibroblasts. 26 To further examine whether these tendon progenitor cells have the capacity of producing anabolic growth factors that may induce matrix synthesis and cell proliferation after injection, we have examined the growth factor profiles of these cells, including platelet-derived growth factor α (PDGFα), fibroblast growth factor β (FGFβ), transforming growth factor β (TGFβ), bone morphogenetic protein 2 (BMP-2), BMP-7, insulin-like growth factor 1 (IGF-1), and PDGFβ. A portion of the cells from each patient was harvested at the time of implant for cellular characterization analysis using real-time PCR.
The total RNA was extracted from the cultured tendon-derived cells from patients using the PureLink RNA Mini Kit (Invitrogen; Life Technologies) according to the manufacturer’s instructions. The RNA from dermal fibroblast and synovial fibroblasts was used as a control. Single-stranded cDNA was synthesized from 1 μg of RNA using 200 U of M-MLV reverse transcriptase, 20 U of RNasin ribonuclease inhibitor, 0.5 mM of deoxynucleotide triphosphate, and 0.5 μg of oligo-dT 15 primer (a short sequence of deoxythymine nucleotides) in a total volume of 20 μL for each sample (Promega). To determine the gene expression profile of the tendon-derived cells from patients, relative quantitative real-time PCR was performed on a Bio-Rad MyiQ real-time PCR system (Bio-Rad Laboratories Pty Ltd). The total volume of each PCR reaction was 25 μL, containing 12.5 μL SensiMix (Bioline), 0.25 μL of probe (100 nM) (Roche Diagnostics), 6.25 μL of double-distilled water, 5 μL of cDNA, and 0.5 μL of each primer (400 nM). These are listed in Table 2. Real-time PCR was carried out at 95°C for 15 minutes, 40 cycles at 95°C for 15 seconds, 60°C for 60 seconds, and 72°C for 15 seconds. Housekeeping GAPDH (glyceraldehyde 3-phosphate dehydrogenase) was included as an internal control. A cycle threshold value was obtained for each sample, and the comparative 2-delta-delta-CT method was used to calculate the relative expression level of each target gene, as previously described.
Growth Factor Primer Sequences a
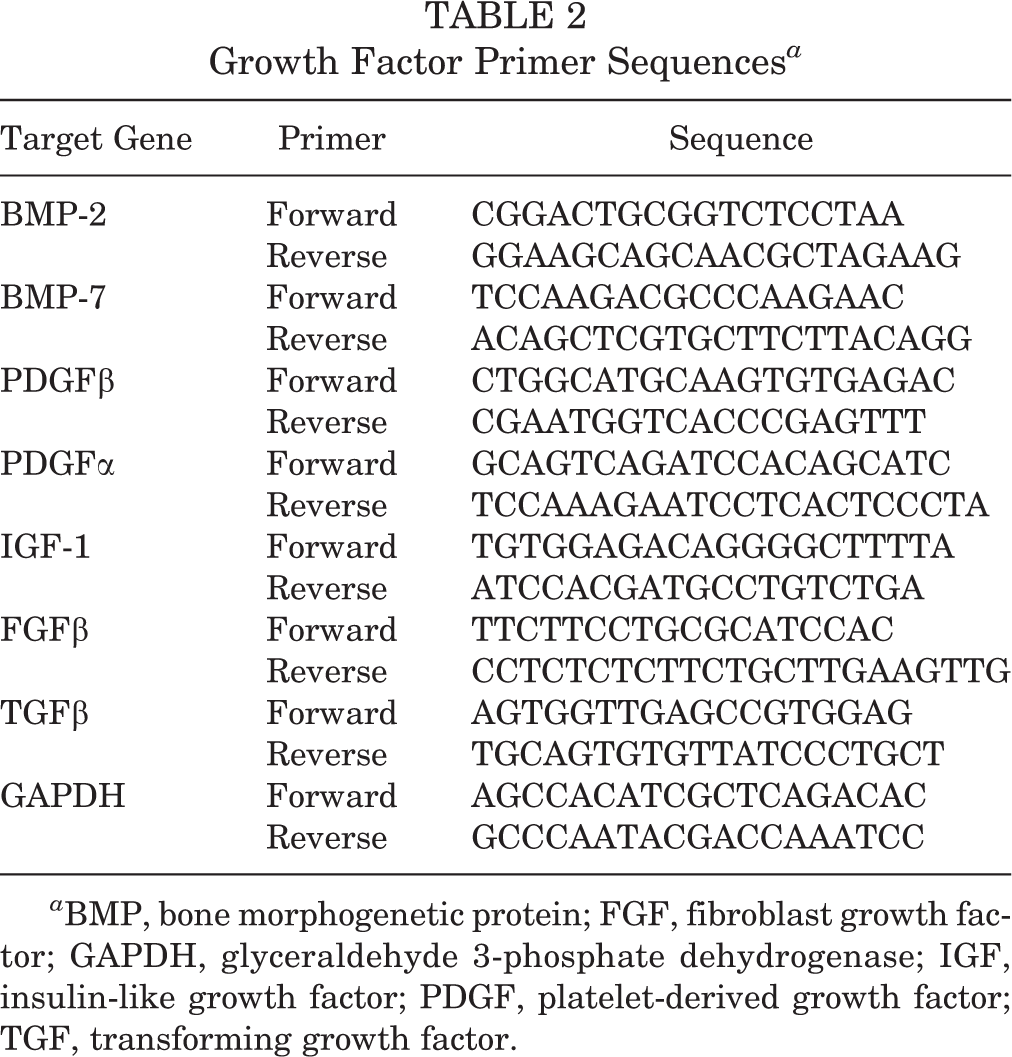
a BMP, bone morphogenetic protein; FGF, fibroblast growth factor; GAPDH, glyceraldehyde 3-phosphate dehydrogenase; IGF, insulin-like growth factor; PDGF, platelet-derived growth factor; TGF, transforming growth factor.
Autologous Tenocyte Injection (ATI)
In a second-stage procedure, approximately 4 weeks after the initial tendon biopsy, patients underwent a single tenocyte injection. The patient was placed in the lateral decubitus position, and the skin was prepared with a suitable antiseptic solution. Under ultrasound, 2 mL of autologous tenocytes (2-5 × 106 cells/mL) suspended with 10% autologous human serum were injected into the tendinopathic area using a 22-gauge needle. The same consultant radiologist again performed all procedures. The patient was advised to rest for 48 hours postinjection but could mobilize as tolerated.
Clinical Assessment
All patients were independently assessed preinjection and at 3, 6, 12, and 24 months postinjection. The primary outcome measure was the Oxford Hip Score (OHS), and a minimally important clinical change for this measure has been estimated as 11 points in patients undergoing hip arthroplasty. 1 A visual analog pain scale (VAS) was employed to assess hip pain at rest, on a whole number rating scale from 0 (no pain) to 10 (worst pain). Finally, the 36-item Short Form Health Survey (SF-36) was employed to evaluate general health producing a mental component score (MCS) and a physical component score (PCS). All patients were asked how satisfied they were with the results of their outcome using a 7-point satisfaction rating scale (highly satisfied, quite satisfied, satisfied, not sure, unsatisfied, quite dissatisfied, highly dissatisfied).
MRI Assessment
All patients underwent postinjection MRI at a mean of 8.7 months (range, 6-12 months). All scans were performed on a Phillips Achieva 3T system (Phillips Healthcare). The sequences utilized to evaluate the gluteal tendons were a coronal proton density (repetition time [TR], 3500 ms; echo time [TE], 30 ms; slice thickness, 3.5 mm), a coronal T2 fat-suppressed (TR, 4500 ms; TE, 60 ms; slice thickness, 3.5 mm), and an axial proton density fat-suppressed (TR, 3500 ms; TE, 20 ms; slice thickness, 4 mm), all obtained with a field of view (FOV) of 18 cm.
In the absence of a recognized objective radiological scoring system for gluteal tendinopathy, we adapted a scoring tool employed by Pfirrmann et al. 21 In brief, the gluteus minimus tendon and the lateral and posterior components of the gluteus medius tendon were analyzed separately. Hyperintense signals extending to both surfaces of the tendon defined tendon tears or detachments (absent or present), and osseous detachment of the tendon was recorded. Tendon diameter was qualitatively rated (normal, thinned, or thickened) based on the radiologist’s knowledge of normal tendon anatomy. Tendon signal intensity was graded as normal (hypointense) or abnormal (increased signal intensity) compared with normal tendon signal intensity. Abductor tendon ossification was also documented (absent or present). Bursal fluid collections were rated as absent or present, as was a “fan sign,” described by Pfirrmann et al 21 ; the fan shape made by the muscle tissue of the gluteus medius muscle reached the bone outline of the greater trochanter, with a positive response documenting the presence of a defect in the muscle tissue.
Data and Statistical Analysis
Mixed-effects regression models with random intercept and time as a factor variable were used to estimate changes in clinical outcomes over time. In addition to the estimate of degree of improvement at 12 and 24 months, change from baseline to postinjection time points for the OHS was dichotomized as a minimal clinically important change of 11 points. 1 Ninety-five percent confidence intervals and P values are provided for all contrasts of interest. Due to the small sample size, the nonparametric Friedman (repeated-measures analysis of variance [ANOVA]) and Wilcoxon signed rank test (paired t test) were also performed to assess rank differences and confirm conclusions from regression models. Spearman rho was used to assess whether change in OHS at 12 months was associated with age or duration of symptoms.
Changes in MRI measures pre- to postinjection were assessed using the McNemar test. All pre- (n = 12) and postinjection (n = 12) MRI scans were independently reviewed and scored by 2 experienced musculoskeletal radiologists, blinded to the clinical details of the cases, to evaluate interrater reliability. One radiologist rescored a random sample of 20 pre-/postoperative scans to evaluate intrarater reliability. Inter- and intrarater reliability was assessed using the Cohen kappa and prevalence and bias-adjusted kappa (PABAK). 2 Statistical analysis was performed using SPSS software (version 17.0; IBM Corp).
Results
Two patients missed their 3- and 6-month clinical evaluations. No patient received additional treatment during the study period. Figure 1 shows the study flowchart.

Study flowchart. ATI, autologous tenocyte injection; MRI, magnetic resonance imaging; OHS, Oxford Hip Score; SF-36, Short Form–36; VAS, visual analog scale.
Growth Factor Profiles of Tendon Progenitor Cells
As previously described, cultured autologous tendon-derived cells were characterized using flow cytometry and real-time PCR for type I collagen, scleraxis, aggrecan, MAGP2, and Mohawk (Table 2) to ensure the purity and potency of tendon cell phenotype. To further investigate whether autologous tenocytes express growth factors, real-time PCR was used to examine numbers of growth factors that have been shown to have an anabolic effect for tendon, cartilage, and bone. Figure 2 shows that autologous tendon-derived cells expressed growth factors mRNA at different levels. The majority of these cases express high levels of mRNA for PDGFα, FGFβ, and TGFβ, which have been shown to induce tendon development. 10

Gene expression of growth factors in autologous tenocytes. BMP, bone morphogenetic protein; FBF, fibroblast growth factor; GAPDH, glyceraldehyde 3-phosphate dehydrogenase; IGF, insulin-like growth factor; PDGF, platelet-derived growth factor; TGF, transforming growth factor.
Clinical Outcomes
Figure 3 demonstrates the incremental pattern of improvement in the OHS from preinjection to 24 months. There was statistically significant evidence for improvements from baseline (preinjection) to 6 months postinjection (change, 8.3 points; 95% CI, 3.9-12.8; P = .009), with mean improvement estimated to be 14.9 points by 12 months (95% CI, 10.6-19.2; P < .001). Seven of 12 patients demonstrated a clinically important change of 11 or more points (Table 1). The degree of improvement in the OHS was not estimated to be associated with age (Spearman rho, –0.306; P = .334) or the duration of symptoms (Spearman rho, –0.182; P = .572).
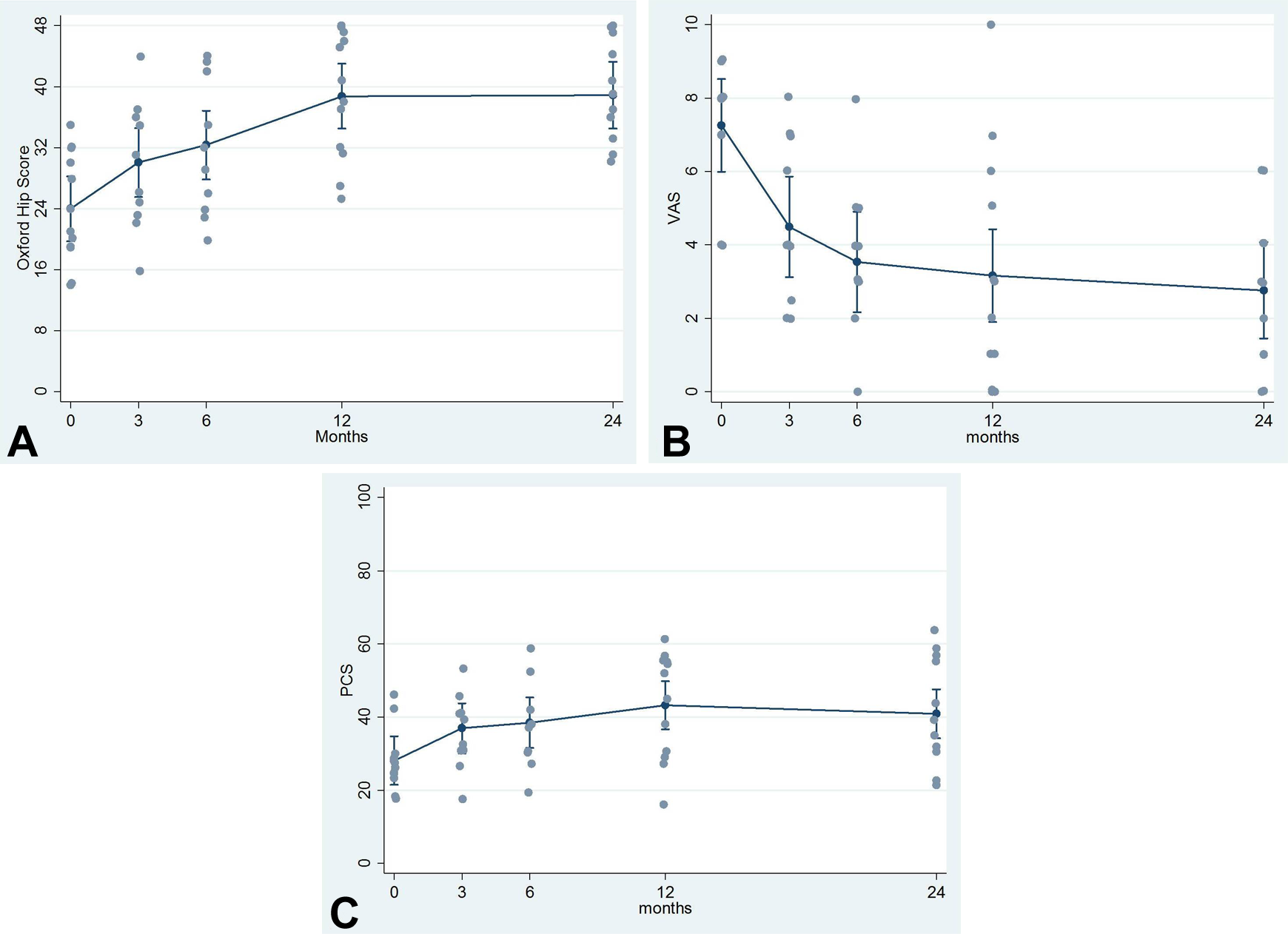
Mean (95% CI) pre- and postinjection patient-reported clinical outcomes including the (A) Oxford Hip Score, (B) visual analog pain scale (VAS), and (C) the physical component subscale (PCS) of the 36-item Short Form Health Survey.
A pattern of incremental improvement was also observed for the VAS and the PCS subscale of the SF-36, the majority of which occurred in the first 3 months (Figure 3). Evidence of improvement from baseline to 3 months postinjection was observed for the VAS (change, –2.8 points; 95% CI, –4.4 to –1.2; P = .001) and PCS (change, 8.8 points; 95% CI: 3.2-14.5; P = .002). An estimated mean change in the VAS from baseline to 12 months was –4.1 (95% CI, –2.6 to –5.6; P < .001). The mean (SD) for the PCS subscale of the SF-36 preintervention was 28.1 (8.5) and ranged from 17.4 to 46.1. An estimated mean change in the PCS from baseline to 12 months was 15.2 (95% CI, 9.8-20.5; P < .001). The improvement for the VAS and PCS was maintained to 24 months, with the estimated change from baseline to 24 months being –4.5 points (95% CI, –6.1 to –2.9; P < .001) for the VAS and 12.8 points (95% CI, 7.3-18.3; P < .001) for PCS.
All 12 patients completed the patient satisfaction questionnaire at 12 months postsurgery; 5 were highly satisfied, 3 were satisfied or quite satisfied, 2 were unsure, and 2 were dissatisfied with the outcomes of their procedure. Satisfaction at 12 months showed good concordance with improvements at 12 months, with those patients with the most improvement being highly satisfied and those with the lowest being dissatisfied or unsure (see Table 1).
MRI Outcomes
We sought to examine whether the pathological features of tendinopathy seen on MRI were correlated with the clinical outcome after ATI. We observed no significant improvement from pre- to postinjection in any tendon features measured by MRI (Table 3). Intrarater agreement was absolute or high for all MRI measures (PABAK range from 0.727 to 1.00). Interrater agreement was absolute or high for all MRI measures, with the exception of tendon signal intensity for the lateral portion of the gluteus medius (Table 4). Figure 4 shows the pre- and postinjection MRI for 1 patient, demonstrating improved appearances.
Pre- and Postinjection MRI-Based Changes
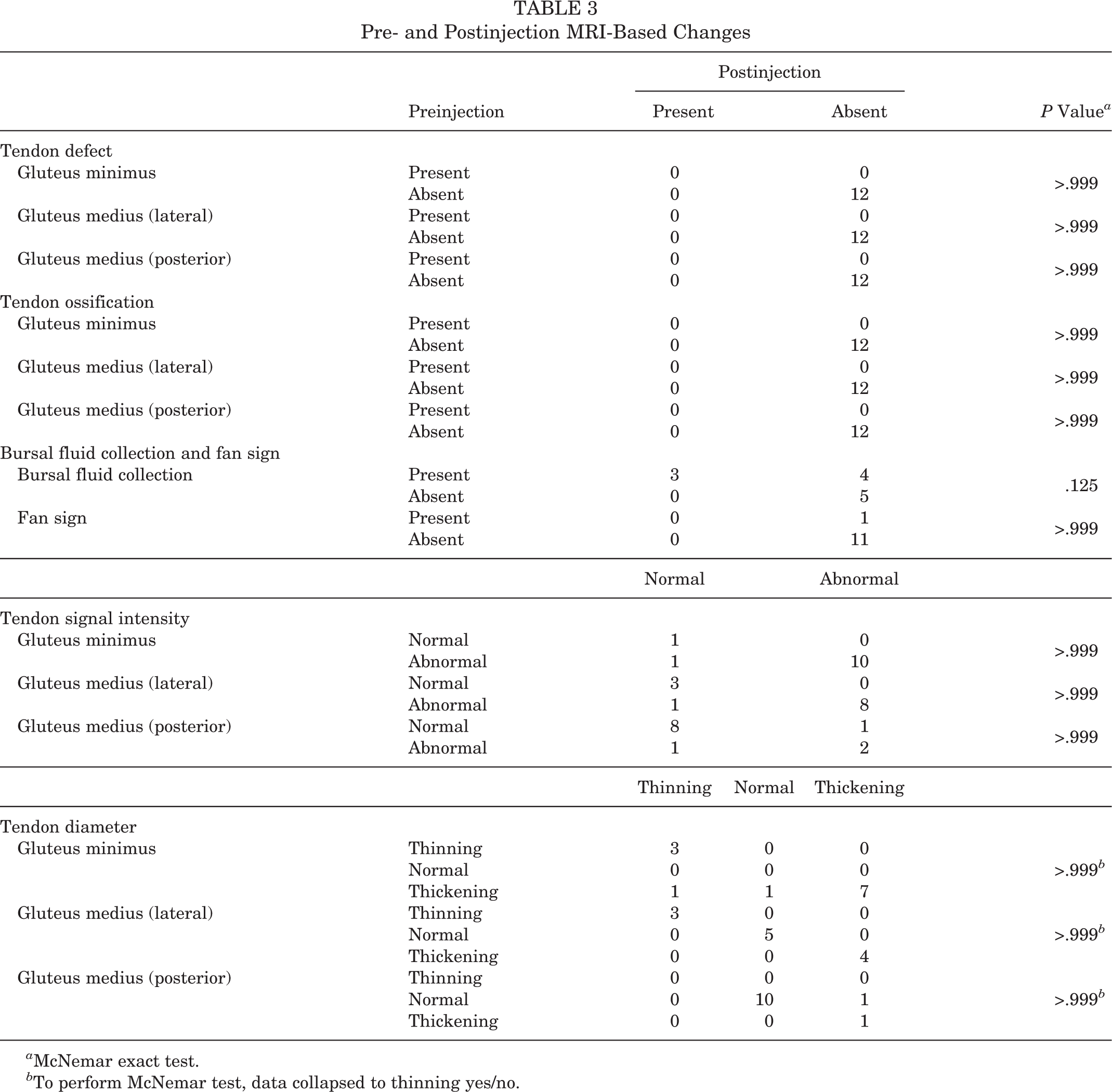
a McNemar exact test.
b To perform McNemar test, data collapsed to thinning yes/no.
Evaluation of inter-rater reliability of the MRI-based scoring variables using Cohen’s kappa and Prevalence and Bias Adjusted Kappa (PABAK).

a Prevalence and bias adjusted kappa.

Coronal magnetic resonance image of the same patient (A) preinjection and (B) at 6 months after autologous tenocyte injection demonstrating a reduction in both gluteus medius tendon thickness (arrow) and the extent of intratendon T2 high signal intensity.
Complications
There were no injection or biopsy site infections, though 3 patients reported some immediate discomfort at the patella tendon biopsy site, all of which responded to topical nonsteroidal anti-inflammatory gel. There have been no long-term complications related to the biopsy site. There were no complications after the ATI injection. One patient (patient 1, Table 1) did not respond to ATI treatment and has since undergone surgery to repair her gluteal tendon, after her 12-month review. This patient reported a change in the OHS from 19 to 25 (pre- to 12 months postinjection), though also reported a prior duration of symptoms of 12 years.
Discussion
Gluteus medius and/or minimus tendinopathy is now accepted as the most prevalent pathology in those with pain and tenderness over the greater trochanter, 11 though conservative treatment modalities demonstrate high symptom recurrence rates. 18,19 In an attempt to explore advanced therapeutic options, we have conducted the first prospective case study of ATI specifically in patients with chronic gluteal tendinopathy. In this study, we have demonstrated that ATI significantly improved early clinical patient-reported outcomes, with further improvement and sustained benefit to 24 months. All patients in this study reported improvement in the OHS, with 7 of 12 patients demonstrating a clinically important change of 11 or more points by 12 months. A similar pattern of incremental improvement was observed for the VAS and the PCS subscale of the SF-36.
Currently, steroid injections are the mainstay of treatment for gluteal tendinopathy, 22 and while they have demonstrated good short-term efficacy, 15 recurrence of pain is common. 8 This was reflected in this study, with patients undergoing an average of 3.2 prior injections (range, 2-5), with no benefit from their most recent injection. It has been shown that apoptosis and autophagic cell death are common in other tendinopathic conditions. 3 This, coupled with the lack of inflammation seen with tendinopathic conditions, may explain why steroid injections do not give long-lasting relief of symptoms and provides rationale for investigating the potential benefit of ATI. In comparison with a study by Labrosse et al, 15 who showed only short-term benefits after steroid injections, patients in this pilot trial displayed early improvement in pain scores that were sustained up to 24 months after ATI. Our data demonstrate promise in the use of ATI in the treatment of gluteal tendinopathy.
Recently, other injection therapies such as PRP or autologous blood have become increasingly popular for their potential application in the treatment of tendinopathy. Although the product of ATI contains 10% patient serum without platelets and white blood cells, it is very unlikely that 10% autologous human serum will have any effect on the clinical outcome. This is supported by a recent meta-analysis on the effect of PRP in tendinopathy, which demonstrated that only leukocyte-rich PRP has a therapeutic effect on tendinopathy. 9 According to manufacture requirements, the presence of 10% patient serum within ATI is used for cell stability as it contains a high concentration of human albumin. The fact that 4 of these patients had previously received intratendon PRP injections without benefit also reiterates the minimum therapeutic impact of 10% serum in the injection media.
Animal studies have demonstrated that autologous tenocytes are effective in treating chronic tendon degeneration. 4,5 Others have injected tenocyte-like cells cultured from skin fibroblasts into tendinopathic tendons. 6,7 The presented ATI technique differs from previously published methods in that tenocytes are prepared from the same cell line rather than collagen-producing tenocyte cells used from skin fibroblasts. ATI has already demonstrated improved clinical (and radiological) outcomes in patients with chronic lateral epicondylitis. 24,25 A similar benefit has also been shown for ATI in the rotator cuff. 26 Given the apoptosis and autophagic cell death seen in chronic tendinopathy, 3 one of the potential mechanisms of action of ATI contributing to the clinical improvement observed may be the incorporation of Feridex-labeled injected tenocytes into the tendon matrix, seen previously in an animal study. 4 In addition, this study also showed that injected autologous tenocytes may produce growth factors, including FGFβ, TGFβ, and PDGFα, that can act in the autocrine and paracrine actions for the induction of tendon cell proliferation and matrix production.
Despite the statistically significant improvement in clinical scores, we failed to demonstrate obvious MRI-based improvement in the majority of cases. A recent review by McMahon et al 20 suggested that while a paucity of data exist for the management and imaging of these conditions, MRI should be the imaging modality of choice in the investigation of GTPS. However, studies tend to concentrate on the effectiveness of MRI for predicting the presence of a tear rather than tendinopathy. Furthermore, while MRI has demonstrated benefit in the pretreatment diagnosis and planning for a patient with clinical signs of GTPS, to our knowledge, there are no studies evaluating the appearance of gluteal tendons after treatments such as injections, nor is there a preexisting validated tool to evaluate improvement from an intervention. MRI performed after surgical repair of gluteal tendons often demonstrates ongoing tendon abnormality and thickening, 16 while a recent systematic review found that false positives were common when assessing the accuracy of MRI for gluteal tendon tears. 27 Westacott et al 27 concluded that better designed studies demonstrate poor accuracy and that ultrasound in skilled hands may be the investigation of choice. This becomes relevant when considering our inability to demonstrate obvious radiological improvement in the majority of cases, despite the reported clinical improvement.
Our study does have several limitations. Firstly, small case numbers were investigated given the primary outcome was safety specifically in the use of ATI for gluteal tendinopathy. While a safety study has been previously undertaken for lateral epicondylitis, 24,25 the gluteal tendon is a different and weightbearing tendon and may behave in a different way to the upper limb. Second, we acknowledge the lack of a comparative group and the potential for clinical changes that could occur purely as a result of placebo or the natural recovery time line (particularly in those with a shorter duration of symptoms). However, it should also be noted that statistically significant evidence for improvements was noted by 6 months postinjection, and the shortest symptom duration reported was 6 months. Furthermore, all 12 patients had failed to obtain benefit from other conservative treatments such as structured exercise, had received no benefit (or were worse) from their most recent cortisone injections (with patients undergoing an average of 3.2 prior injections), and had a duration of symptoms of on average 33.2 months (minimum, 6 months; 9 patients at least 12 months; 6 patients at least 24 months). Furthermore, the improvements obtained were sustained for 24 months, which, combined with the history of failed prior treatment in these patients, may well show benefit beyond a placebo response in the absence of a control group. Third, we employed the OHS, a clinical measure specific for hip osteoarthritis, as our primary outcome clinical tool. While it would appear that the OHS has good face validity for GTPS, there is currently no validated patient-reported outcome measure for gluteal tendinopathy or GTPS. Finally, we sought to investigate MRI-based changes in addition to clinical improvement. We acknowledge that obvious radiological improvement in the majority of cases could not be demonstrated despite the reported clinical improvement. This may be limited by our lack of a preexisting validated tool to evaluate MRI improvement from an intervention or that postinjection MRI was undertaken too early, given that 1- and 4.5-year MRI improvement has been reported using ATI for lateral epicondylitis. 24,25 These are areas for future research.
Conclusion
This study demonstrated safety in using ATI specifically in the treatment of recalcitrant gluteal tendinopathy. There were no persistent complications as a result of the tendon biopsy or tenocyte injection. Furthermore, this prospective case series revealed significant and sustained improvement in clinical scores to 24 months after ATI in patients who had previously undergone unsuccessful conservative treatments. Given that gluteal tendinopathy remains a challenging condition to treat, especially when conventional conservative measures fail, this pilot study has provided useful data and shown sufficient promise for the design of a randomized controlled study investigating ATI for gluteal tendinopathy.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Orthocell supplied the autologous tenocyte injection used in this trial. J.R.E. and M.H.Z. were reimbursed costs associated with attending a symposium from Orthocell. M.H.Z. and G.C.J. hold stock in Orthocell.
Ethical approval for this study was obtained from the Hollywood Private Hospital Ethics Committee (HPH374), and the study was registered with the Australia and New Zealand Clinical Trials Registry (ACTN12612000383864).