
Abstract
Background:
Additional high-quality prospective studies are needed to better define the objective criteria used in relation to return-to-sport decisions after anterior cruciate ligament (ACL) reconstruction in active populations.
Purpose:
To investigate prospectively the relationship between functional performance test results at 24 weeks postoperative and return-to-sport activity (Tegner activity score) at 12 and 24 months, respectively, after synthetic (ligament advanced reinforcement system [LARS]) and autograft (doubled semitendinosus/gracilis [2ST/2GR]) ACL reconstructions.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 64 patients who underwent ACL reconstruction (32 LARS, 32 2ST/2GR autograft; mean age, 27.9 years; body mass index [BMI], 24.9 kg/m2) were assessed preoperatively and at staged intervals postoperatively up to 24 weeks for isokinetic testing of quadriceps and hamstring average power per repetition at 60 deg/s and 180 deg/s, a battery of hop tests, peak vertical ground-reaction force (vGRF), and time to peak vGRF (in seconds) during a step- and jump-down task onto a force platform and peak speed (m/s) using a global positioning system (GPS unit) during a running task. A cohort of 32 healthy matched participants (mean age, 26.31 years; BMI, 25.7 kg/m2) were also tested to act as reference. Pearson correlation was calculated to assess correlation of each performance measure at 24 weeks postoperative with activity outcomes (Tegner score) at 12 and 24 months.
Results:
The strongest correlation between physical performance tests and return-to-sport outcomes was observed with peak speed during running. Large correlations were also observed for hamstring isokinetic power and hop test for distance. Moderate correlations were observed for timed hop, peak vGRF during a jump-down task, and quadriceps isokinetic power. No statistical correlations were observed for time to peak vGRF during a step-down and jump-down task as well as peak vGRF during a step-down task. When the performance tests were pooled together, mean postoperative improvements of 24% were observed from preoperative to 24 weeks within the surgical cohort. For each performance test, preoperative level of function strongly correlated with performance levels on the same test at 24 weeks.
Discussion:
The results of this study indicate that clinicians might seek to prioritize these tests and the rehabilitation themes they imply when seeking to maximize postoperative ACL activity outcomes. The observed strength between pre- and postoperative performance tests and return-to-sport outcomes within this study highlights the potential value of preoperative conditioning before undergoing ACL reconstruction. Future research should examine absolute predictive criterion thresholds for functional performance-based tests and reinjury risk reduction after ACL reconstruction.
The aim of rehabilitation after anterior cruciate ligament (ACL) reconstruction is to return an individual to his or her chosen level of activity in a timely and safe manner. Successful return to sport (RTS) is broadly and variably defined, based on the preinjury competitive level played, the goals of the patient postinjury, and the sport level achieved after ACL reconstruction. 1,25 After surgery, RTS is often permitted as soon as 3 to 12 months, depending on the graft used. 66 Previous literature has strongly correlated patient-reported quality of life after ACL reconstruction with the ability to RTS. 22 Clinicians are often asked to make judgements when an athlete has functionally “recovered” sufficiently to allow a safe and durable return to activity. Although the practice is increasing, it is still relatively rare for clinicians to use objective physical performance measures to determine safe RTS, and rarely are the specific criteria used reported in practice. 25 Consensus is similarly lacking on which measures most strongly correlate with final RTS outcomes. 7 This lack of criteria may contribute to indecision on the optimal components of rehabilitation, 36 caution or reluctance to return to preinjury competitive sport after surgery, 3 and an elevated risk of further injury for those that do. 1,49,64 The most commonly used methods of objective criteria for RTS reflect the various components of rehabilitation after surgery. Functional performance tests generally include combinations of strength, 26,28,32,43,47,52,56,60 unilateral hopping, 5,8,10,20,27,28,45 jump landing, and/or running-based tests. ¶ Although optimized performance in so-called functional tests has been associated with reduced risk of further injury after RTS, 35 few prospective or longitudinal studies have evaluated which functional tests should be prioritized over others to maximize RTS potential. 19,30,31,37,39,55 A benchmark of >90% symmetry of the injured limb relative to the uninjured limb is most commonly used to determine satisfactory recovery of function postoperatively, 61,62 though literature has reported this benchmark as low as 80% 20,28 or as high as 95%. 62 A recent meta-analysis 41 identified that average symmetry varied from 94.6% to 99.6% for the physical performance tests commonly used in measurement of recovery after ACL reconstruction across a healthy active population. Although scores may be high on functional performance measures in practice, their ability to influence RTS success may not match patient expectations, thus making the surgery unsuccessful in the patient’s opinion.
The purpose of this prospective study was to examine the strength of relationships between specific objective functional tests (isokinetic strength testing of the hamstring and quadriceps muscle groups at 60 deg/s and 180 deg/s; a battery of single-leg hop tests; peak vertical ground-reaction force [vGRF] and the time taken to achieve this peak during a step-down and jump-down task; and peak speed during a running test) with RTS outcomes (as measured by the Tegner activity scale [TAS]) at 12 and 24 months postoperative to assess utility of these tests in clinical practice. Two different ACL procedures were used: autologous doubled semitendinosus/gracilis (2ST/2GR) and synthetic ligament advanced reinforcement system (LARS) grafts. Given the implications of different rehabilitation protocols between surgical procedures, the intention in this study was not to directly compare surgical procedures but rather to look at participants who had selected 2 different ACL procedures in parallel to each other, with reference to the outcome measures associated with recovery of function and their influence on postoperative activity levels. We hypothesized that more dynamic performance tests (peak speed, jump-down test, and hop testing) would have stronger correlations with RTS outcomes than less dynamic ones (isokinetic testing and step-down test) given their logical synergy with higher level function.
Methods
Patients who satisfied the inclusion criteria (Table 1) were considered eligible to be enrolled into the study from February 2012 until June 2014. Participants were recruited who met the inclusion criteria for 2 different surgical groups: either a LARS or a 2ST/2GR autograft ACL reconstruction procedure. An additional group was recruited consisting of healthy matched participants from the general population based on age, body mass index (BMI), and activity level (as measured by TAS) to act as a performance reference for the surgical groups.
Inclusion and Exclusion Criteria a
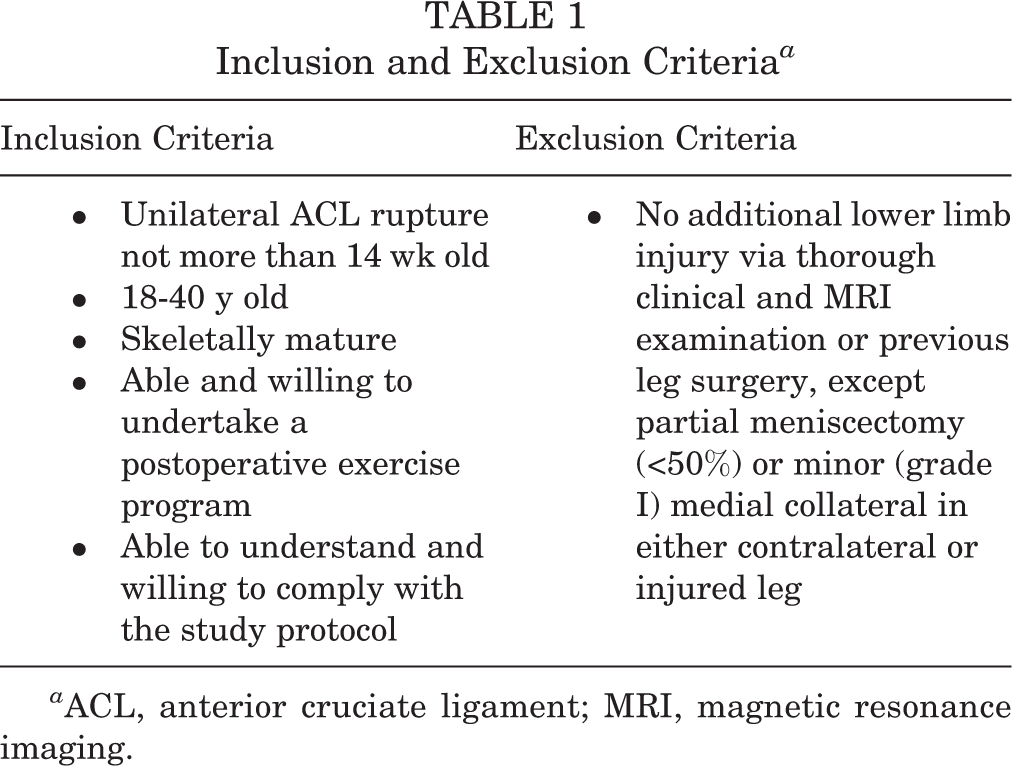
a ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
Surgical Considerations, Postoperative Care, and Rehabilitation Protocol
Surgery was performed by 3 senior orthopaedic consultants, each with over 10 years of experience. Two types of grafts were used: autologous doubled semitendinosus/gracilis (2ST/2GR) and double-bundle ACL LARS graft using a DB40 or DB50 graft, depending on patient size. All 3 surgeons performed 2ST/2GR procedures, whereas only 1 surgeon performed the LARS procedures. Table 2 summarizes the rehabilitation protocol for both surgical groups.
Rehabilitation Protocols for Patients with Hamstring (2ST/2GR) and LARS Grafts a

a GR, gracilis; LARS, ligament advanced reinforcement system; ST, semitendinosus.
Testing Protocol
Two blinded assessors who were not authors of the study and who were both qualified physical therapists performed all tests at the indicated time points. For the purposes of this investigation, the dominant leg was considered the leg the participant preferred to use when kicking a ball. Participants were assessed pre- and postoperatively by 4 performance batteries, as indicated in Table 3. Isokinetic testing, hop testing, and both step-down and jump-down testing were all tested in the same order each time on the same day, with running testing conducted on a different day although still in the same week.
Pre- and Postoperative Physical Performance Measure Assessment Schedule a

a GPS, global positioning system.
Isokinetic Testing
Before isokinetic testing, the participant was allowed a 5-minute warm-up on an exercise bicycle. After the purpose of the test was explained, the isokinetic machine was set up as per manufacturer’s recommendations (Humac Norm; CSMI Solutions) with the subject sitting; the nonoperative leg was tested first and the injured limb second. The results of concentric/eccentric testing for both quadriceps and hamstrings were pooled into a single result and reported as average power (in watts) per repetition.
Hop Tests
The hop tests were performed as described by Reid et al. 53 The single hop for distance was performed as outlined by Daniel et al. 17 The timed 6-m hop was performed as outlined by Barber et al. 5 The triple hop for distance and crossover hop were performed as outlined by Noyes et al, 45 with the latter test performed over a 15-cm strip on the floor. For each hop test, the participants performed 1 practice trial for each limb, followed by 2 measured and recorded trials. For each set of tests, participants were instructed to begin with the nonoperative limb. To minimize fatigue, a rest period was offered between types of hop tests (up to 2 minutes) and between individual hop test trials if needed (typically less than 30 seconds was sufficient). The series of hop tests took approximately 10 minutes to administer. The hop for distance tests were represented as the combined sum (distance measured in meters) of each test battery, with the 6-m timed hop analyzed separately (measured in seconds).
vGRF and Time to Peak vGRF During Step-Down and Jump-Down Tests
The step-down and jump-down tests were performed as described by Colby et al 16 and VanMeter, 63 respectively. Two forms of data were collected using Bioware data acquisition software for each trial (Kistler): peak vGRF normalized to bodyweight and the time taken (seconds) from initial foot contact to vGRF. The step-down and jump-down tests consisted of a single drop step from a height of 15 cm onto the force plate. In each case, the nonoperated leg was tested first, followed by the operated leg. Participants were instructed to stabilize as quickly as possible and to remain as still as possible for 10 seconds. For the jump-down test, to standardize the jump-down movement, a predetermined “target” was utilized to control the height of the jump that the participant had to touch before landing once the jump had commenced. The target was defined as 50% of their maximal double-leg countermovement jump as measured using a Vertec jump tester (Sports imports). For both tests, the participant performed at least 3 practice trials on each leg to minimize possible learning effects. During each test, 3 trials were recorded for each leg.
Peak Speed
This test was conducted in the same week as the other forms of testing although on a separate day. Participants were instructed to arrive in a fully rested and hydrated state, having consumed no food within 40 minutes before testing or having performed any strenuous exercise in the previous 48 hours. The participant was fitted with a global positioning system (GPS) harness and unit between the scapulae as per the manufacturer’s instructions (SPi ProX 15Hz; GPSports). A standardized dynamic warm-up included movement drills and progressive runs over a 60-m space. During testing, no active encouragement was given. Participants performed 12 maximal accelerations from 0 to 40 m. The peak speed (m/s) achieved during these efforts was recorded.
Statistical Analysis
Statistical analysis was performed using SPSS version 23 (IBM Corp). A power analysis was derived from Cohen, 15 and sample size was determined so that the study had 80% power to detect an effect size as large as 0.7 standard deviation on the dependent variables of interest in the study, with an alpha value of 0.05, 2-tailed. This analysis determined that 32 participants were required from each surgical procedure for sufficient statistical power to be achieved. In Cohen’s terms, the effect size that the study was set up to detect is medium-large. For each test, the mean and standard deviation were obtained for each group. For each performance test, a repeated-measures analysis of variance (ANOVA) was utilized to assess the pattern of recovery over time in relation to surgical type and sex. No sex-specific or between-graft statistical differences were observed in the gradient of recovery for all of the tests in question (P > .069). Pearson correlation was calculated to assess correlation of each performance measure as it related to RTS activity outcomes (TAS) at 12 and 24 months as reported in part 1 of this study (see the Appendix). 41 As recommended by Cohen, 15 a “small” correlation was deemed as r = 0.1 to 0.3, a “medium” correlation as r = 0.3 to 0.5, and a “large” correlation as r > 0.5.
Inter- and intrarater reliability of the outcome measures was analyzed in a test sample of healthy recruited participants separate to the main study (n = 9). Using the criteria established by Shrout and Fleiss, 58 all tests demonstrated excellent reliability (intraclass correlation [ICC], >0.75), with the exception of the step-down/jump-down test (Table 4), which was assessed as “good” (ICC, 0.40-0.75). The reliability of isokinetic dynamometry 18 and wearable GPS technology 6,12 has been previously established as “excellent” for the variables of interest. Although the TAS weights itself toward certain sports, the scale has been shown to have acceptable test-retest reliability as well as acceptable content, criterion, and construct validity for ACL injuries with a minimum detectible change score of 1. 9
Intraclass Coefficients for Inter- and Intrarater Reliability

A total of 64 surgical participants were recruited into the study. There were also 32 participants in the healthy reference group. The age range of participants varied from 18 to 33 years. Independent-samples t tests, with concomitant Levene tests for equality of variance, were performed for age, height, and weight and found to be equivalent between groups (Table 5).The activity-based pre- and postoperative (TAS) demographics of the participants are previously described in part 1 of this study (see the Appendix). 41 As a reference, 81% of participants within the surgical cohort had returned to their preoperative level of activity by 12 months, and 83% by 24 months, indicating the surgical cohort to be a suitable sample for the current investigation. Given that previous literature 42 has not found an effect of limb dominance on the physical performance tests used in this study, limb dominance was not considered a covariant.
Participant Demographics a

a BMI, body mass index; GR, gracilis; LARS, ligament advanced reinforcement system; N/A, not applicable; ST, semitendinosus.
Results
Isokinetic Strength Testing
Quadriceps
From preoperative to 24 weeks postoperative, the surgical leg improved isokinetic power in a steady linear fashion an average of 19% across the surgical cohort (Figure 1). At 24 weeks postoperative, the operated leg had a mean symmetry index of 89%, compared with 98.7% for the healthy reference group. Quadriceps power at 24 weeks (Table 6) was moderately correlated with activity levels (TAS) at 12 (r = 0.445, P = .001) and 24 months (r = 0.438, P = .001). Furthermore, preoperative quadriceps power on the injured leg was strongly correlated with quadriceps function postoperatively at 24 weeks (r = 0.734, P < .001).

Pre- and postoperative physical performance limb symmetry index for hop tests and isokinetic dynamometry. Pre-Op, preoperative.
Pearson Correlations of Physical Performance Measures With RTS Levels at 12 and 24 Months Postoperative a

a GPS, global positioning system; RTS, return to sport; vGRF, vertical ground reaction force.
bP < .001.
Hamstring
Hamstring strength in the operated leg was reduced relative to baseline in the early postoperative period, before improving in the remaining period (Figure 1). The overall net isokinetic power change from pre- to postoperative averaged 0% across the surgical cohort. In relative terms, the surgical group averaged 87% relative symmetry for the operated leg at 24 weeks postoperative compared with 81.5% for the healthy reference group. Mean hamstring power at 24 weeks (Table 6) had a strong correlation with activity levels (TAS) at 12 (r = 0.616, P < .001) and 24 months postoperative (r = 0.571, P < .001). Preoperative hamstring power on the injured leg also had a large correlation with hamstring function at 24 weeks postoperative (r = 0.615, P < .001), indicating that preoperative power was a strong determinant of postoperative hamstring power.
Combined Hop Test for Distance and 6-m Timed Hop
The combined hop test for distance on the operated leg improved an average of 16% (Figure 1) from preoperative baseline, with mean limb symmetry index of 88% within the surgical cohort at 24 weeks compared with 99.8% for the healthy reference group. Total hop for distance at 24 weeks (Table 6) had a large correlation with activity levels (TAS) at 12 (r = 0.553, P < .001) and 24 months (r = 0.527, P < .001). Preoperative total hop for distance on the injured leg had a strong correlation with total hop for distance at 24 weeks postoperative (r = 0.600, P < .001).
For the 6-m timed hop, the operated leg improved an average of 39% from baseline within the surgical cohort. At the 24-week testing period, the surgical group demonstrated 90% relative symmetry compared with the 99.8% observed in the healthy reference group. The 6-m timed hop function at 24 weeks (Table 6) had a moderate correlation with activity levels (TAS) at 12 (r = 0.445, P < .001) and 24 months postoperative (r = 0.428, P = .001). Preoperative 6-m timed hop function on the injured leg had a strong correlation with 6-m timed hop performance on the injured leg at 24 weeks postoperative (r = –0.510, P < .001).
Peak Speed During Running Using GPS
Within the healthy reference group, a mean ± SD peak speed of 6.81 ± 1.60 m/s was observed as a relative benchmark for the surgical groups. Mean peak speed for the surgical cohort at 24 weeks postoperative was 6.45 ± 1.8 m/s, with an overall change from 12 to 24 weeks of 15%. Peak speed at 24 weeks postoperative had a statistically strong correlation (Table 6) with activity level (TAS) at 12 months (r = 0.896, P < .001) and 24 months (r = 0.511, P = .008). Preoperative combined total hop for distance function on the injured leg had a large correlation with peak speed function at 24 weeks postoperative (r = 0.638, P = .001), which may imply that optimal neuromuscular function before surgery may indicate postoperative peak speed ability.
vGRF During Step-Down and Jump-Down Tasks
Peak vGRF of the injured leg during a step-down task at 12 weeks postoperative was not related to activity level (TAS) at 12 (r = –0.011, P = .940) or 24 months (r = –0.125, P = .377), indicating that the test was not correlated with RTS outcomes. Increased peak vGRF during the jump-down task at 24 weeks was moderately correlated with activity level (TAS) at 12 months (r = 0.443, P = .013) and 24 months (r = 0.434, P = .015). Within this latter test, at 24 weeks postoperative, the surgical cohort demonstrated relative symmetry of 94%; however, the operated leg on average generated 63% of the vGRF observed in the healthy reference group (the latter group averaging 2.95 times bodyweight peak vGRF).
Time to Peak vGRF During Step-Down and Jump-Down Tasks
Time to peak vGRF of the injured leg during the step-down task at 12 weeks had no statistical correlation with activity level (TAS) at 12 months (r = 0.073, P = .650) or 24 months (r = 0.077, P = .634). Time to peak vGRF function of the injured leg during a jump-down task at 24 weeks similarly had no correlation with activity levels (TAS) at both 12 months (r = –0.294, P = .102) and 24 months (r = –0.237, P = .192), indicating that timed peak vGRF was not correlated with later RTS level.
Discussion
This prospective study identified 2 important clinically relevant findings. First, large statistical correlations were observed after ACL reconstruction for peak speed during running, hop test performance, and hamstring isokinetic power at 24 weeks postoperative compared with RTS outcomes at 12 and 24 months. Moderate statistical relationships were also observed between TAS outcomes and quadriceps isokinetic strength and 6-m timed hop test results, respectively. Imperfect return to preinjury activity outcomes are widely reported after ACL reconstruction, in the region of 63%, 1,3 although the rehabilitation components that maximize these postoperative activity goals are less understood. Results within this cohort of seemingly above average (>80% preinjury) RTS participants suggest that running speed, hamstring strength, and hop tests (and the rehabilitation themes they represent) might be prioritized during the rehabilitation process to optimize RTS outcomes. The study only partially confirmed an initial hypothesis that more dynamic performance tests would have the strongest correlations with postoperative RTS level. A second important output of this study was that large statistical correlations were observed between preoperative results and performance within the same test at 24 weeks postoperative, indicating there may be value in preoperative conditioning to optimize postoperative recovery potential. Pooled pre- to postoperative improvements across the performance tests of interest measured 24%. To our knowledge, this is the first study to describe speed-based GPS running parameters specifically in relation to postoperative ACL reconstruction participants.
The strongest statistical correlation with RTS level within the present study was observed for peak running speed results. GPS technology and running speed is an increasingly utilized performance measure in elite sport, though its use as an outcome measure in ACL rehabilitation has not been previously described and may be very useful in the clinical setting. Reid et al 54 reported that within elite men’s rugby union, players needed to perform speed zone entries from 5.1 to 6.7 m/s 48 to 97 times during a game, and 6 of 8 positions on the field required 4 to 17 entries >6.8 m/s per game. Furthermore, 13% to 15% of match performance in elite women’s rugby sevens is conducted at running speeds greater than 5 m/s, 14 and 1.5% of game time in elite female field hockey athletes was spent at speeds >5.2 m/s. 40 Although we did not look at speed/endurance or repeat sprint ability as part of this study, the results of the surgical cohort indicate the ability to achieve peak speeds has strong statistical correlation with RTS level. Future research might examine the effects of peak speed and speed-endurance capability on postoperative ACL reinjury risk.
Hop tests for distance had strong statistical correlations, while 6-m timed hop had moderate correlations with RTS level. Previous literature has found a positive relationship between hop test performance and self-reported knee function 21,24,37 –39 as well as postoperative quadriceps torque. 65 However, the hop test may not correlate to kinematic risk factors for ACL injury such as peak flexion angles and moment asymmetry, 65 and so it is probably indicative of gross horizontal motor power rather than movement quality per se. The association between hop tests and RTS level is less understood. 59 The results of this study reaffirm the potential value of this tool in maximizing RTS ability. Future research could investigate the strength of any predictive relationship of hop test performance and reinjury risk compared with other dynamic tests.
Interestingly, isokinetic hamstring testing had the second strongest correlation with RTS outcome at 12 and 24 months postoperative. Optimized hamstring function has been proposed as an important resistor of anterior tibial shear at initial ground contact 11 and may have a protective effect after ACL reconstruction. Hamstring donor site morbidity is also a well-described occurrence after hamstring autograft procedures. 2 Previous work 13 nonetheless has established the link between peak hamstring force and the ability to generate running speed, and the results of this study suggest that participants who are able to improve hamstring power postoperatively may have a better chance of optimizing RTS outcomes. Isokinetic quadriceps strength testing had a moderate statistical correlation with RTS results. Although the influence of quadriceps strength testing on midterm sports participation has previously been advocated, the magnitude of relationship is less understood. 59 Previous work 4,23,28,56 has demonstrated that reduced postoperative quadriceps function and limb asymmetry may result in reduced external knee flexion moments and reduced peak vGRF compared with the uninvolved limb, which are identified kinematic risk factors for ACL injury. 33,57 The results of this study reinforce the relevance of quadriceps strength development in RTS potential.
The present study observed a moderate relationship between RTS level at 12 and 24 months postsurgery, with increased peak vGRF during a jump-down task at 24 weeks postoperative. A consistent strategy of surgical participants was observed to reduce vGRF forces and prolong the time taken to achieve such a peak, in direct contrast to the observations made within the healthy reference group. Previous studies have shown that reduced peak vGRF during single-leg countermovement jumping has been associated with suboptimal sports participation long after ACL reconstruction, 46 and there may also be an inherent compensation to increase peak vGRF on the uninvolved limb in postoperative knees 48 or utilize a “dampening” strategy with the involved limb. 57 Although a potential limitation of this test was lower inherent reliability compared with other tests in this study, the results suggest that postoperative participants who are able to increase vGRF with jump-down tasks may optimize postoperative activity potential.
Limitations to this study include the study design as an ecological study rather than a randomized controlled trial. While age, BMI, and preoperative activity levels were similar between surgical procedures, it is possible that a selection bias may have occurred. The study also utilized 3 surgeons, and although a power analysis was used to determine sufficient statistical power for the study, a larger participant cohort could add greater generalizability to the study. Although the study observed a 24-month postoperative follow-up to arguably reflect the period with the greatest activity level changes, ideally a follow-up of up to 5 years would add further strength to the results. We utilized both a synthetic graft and 2ST/2GR autograft in the study, and it is possible that the results are generalizable only to these 2 surgical populations. However, we did not observe statistical differences in the gradient of recovery between surgical groups, and previous literature 9 has reported that while graft selection may influence the actual timing of RTS, the differences afforded have not been shown to effect clinical or functional outcome measures. On this basis, the results of this study may hold applicability to a wider audience, with a focus toward 12- and 24-month activity results. Strengths of the study were the prospective regular follow-up of participants within the allocated time period and the blinding of assessors. Future research should further investigate the absolute thresholds for individual physical performance–based recovery and the relationships of these tests with kinematic risk factors of ACL injury previously identified in the literature.
Conclusion
Large-effect statistical relationships were observed for peak speed during running, hamstring isokinetic power, and hop tests for distance with RTS outcomes at 12 and 24 months. Moderate correlations were observed for timed hop, peak vGRF during a jump-down task, and quadriceps isokinetic power. In the context of these data being obtained with a cohort displaying relatively high return to preinjury sport levels (>80%), the results of this study indicate that clinicians might seek to prioritize these tests and the rehabilitation themes they imply when seeking to maximize postoperative ACL activity outcomes. Pooled postoperative improvements of 24% were observed across the surgical participants from preoperative to 24 weeks. Future research should examine absolute predictive thresholds for physical performance–based tests and reinjury risk reduction after ACL reconstruction.
Footnotes
Notes
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this project was received in the form of a PhD Scholarship to T.M.M. at the University of Canberra.
Ethical approval for this study was obtained from the University of Canberra Committee for Ethics in Human Research.
Appendix
Mean Tegner activity scores (TAS) for hamstring and LARS (ligament advanced reinforcement system) groups combined (surgical groups). Error bars represent interquartile range. Pre-Op, preoperative. Image reproduced from McGrath et al. 41