
Abstract
Background:
Tunnel enlargement is frequently seen in short-term follow-up after anterior cruciate ligament reconstruction (ACLR). According to new evidence, tunnel enlargement may be followed by tunnel narrowing, but the long-term evolution of the tunnels is currently unknown.
Hypothesis/Purpose:
The hypothesis was that tunnel enlargement is followed by tunnel narrowing caused by ossification as seen in follow-up using magnetic resonance imaging (MRI). The purpose of this study was to evaluate the ossification pattern of the tunnels, the communication of the 2 femoral and 2 tibial tunnels, and screw absorption findings in MRI.
Study Design:
Case series; Level of evidence, 4.
Methods:
Thirty-one patients underwent anatomic double-bundle ACLR with hamstring grafts and bioabsorbable interference screw fixation and were followed with MRI and clinical evaluation at 2 and 5 years postoperatively.
Results:
The mean tunnel enlargement at 2 years was 58% and reduced to 46% at 5 years. Tunnel ossification resulted in evenly narrowed tunnels in 44%, in conical tunnels in 48%, and fully ossified tunnels in 8%. Tunnel communication increased from 13% to 23% in the femur and from 19% to 23% in the tibia between 2 and 5 years and was not associated with knee laxity. At 5 years, 54% of the screws were not visible, with 35% of the screws replaced by a cyst and 19% fully ossified. Tunnel cysts were not associated with worse patient-reported outcomes or knee laxity. Patients with a tibial anteromedial tunnel cyst had higher Lysholm scores than patients without a cyst (93 and 84, P = .03).
Conclusion:
Tunnel enlargement was followed by tunnel narrowing in 5-year follow-up after double-bundle ACLR. Tunnel communication and tunnel cysts were frequent MRI findings and not associated with adverse clinical evaluation results.
In double-bundle (DB) anterior cruciate ligament reconstruction (ACLR), 2 femoral and 2 tibial bone tunnels are drilled at the anatomic ligament insertions. 10,15,18 The aperture fixation of the anteromedial (AM) and posterolateral (PL) hamstring grafts is done with either metal or biodegradable interference screws. Tunnel enlargement after ACLR is a common but poorly understood postoperative phenomenon. 28,36 In a recent study with serial magnetic resonance imaging (MRI), the bone tunnels of single-bundle (SB) ACLR rapidly enlarged for the first 6 months after surgery and thereafter slowly narrowed until 2 years of follow-up. 35 In other studies, the tunnels have remained constant after the rapid enlargement period in 1- to 2-year follow-up. 5,14,30 Tunnel enlargement may lead to tunnel communication after DB ACLR. 19 Nonsymptomatic tunnel communication seen on MRI has been reported in 10% to 19% of patients in the femur and in 24% to 29% of patients in the tibia in 1- to 2-year follow-up. 19,20,30 The long-term consequences of tunnel communication are unknown, but knee instability has been hypothesized to occur. 6,12,26
Bioabsorbable screws that are used for graft fixation have been manufactured using at least 7 different polymer combinations.
22
The absorption and ossification of the bioabsorbable screws have been evaluated using computed tomography (CT) and MRI.
2,3,8
In addition to screw absorption and ossification, small nonsymptomatic cysts inside and near the partially resorbed screws have been reported.
2,4,7,27,31,33
It was claimed that the widely used poly-
The purpose of this study was to examine the bone tunnel diameters and biodegradable
Methods
Patients
Written consent was required from all patients. The inclusion criteria were an ACL injury requiring reconstruction and closed growth plates. The exclusion criteria were previous ACLR, multiligament injury to the index knee, or injury to the contralateral knee.
Surgical Technique
All patients underwent DB ACLR by the same surgeon using the same anatomic technique with hamstring autografts as described previously in detail.
15
In brief, the tibial tunnels were created to the anatomic footprint with a guide. The tibial AM tunnel was located in the anterior part of the footprint and the tibial PL tunnel in the posterior part of the footprint. The femoral tunnels were created via an anteromedial portal with freehand technique to the anatomic insertions of the AM and PL bundles of the ACL. The bony wall between the femoral tunnel apertures was at least 1 to 2 mm. The grafts were fixed with bioabsorbable interference screws (
Rehabilitation
Full weightbearing was allowed immediately in the postoperative rehabilitation program. No brace was used. Crutches were used for 3 to 4 weeks, and closed kinetic chain exercises were started immediately after surgery. Cycling was permitted on an ergometer at 4 weeks. If full functional stability was achieved, running was permitted at 3 months and pivoting sports at 6 months.
MRI Evaluation
Patients underwent MRI scans at 2 and 5 years after surgery. The results of the 2-year MRI evaluation of 66 patients have been published previously. 19,20 In the 2-year evaluation, a 1.5-T MRI (Signa Excite HD imager; GE Healthcare) was used. The 1.5-T imaging protocol included sagittal T1-weighted images with a repetition time/echo time of 2800/19 ms and a slice thickness/gap of 4.0/1.0 mm, sagittal proton density (PD)–weighted images (2320/24 ms and 4.0/1.0 mm), sagittal T2-weighted images (3740/78 ms and 4.0/1.0 mm), coronal T1-weighted images (500/16 ms and 4.0/1.0 mm), coronal fat-suppressed (FS) images (3300/74 ms and 4.0/1.0 mm), axial FS PD-weighted images (1940/40 ms and 4.0/1.0 mm), and oblique sagittal and coronal T1-weighted images along the AM graft plane (660/16 ms and 3.0/0.3 mm).
The 5-year evaluations were done using 3 T MRI (MAGNETOM Trio 3T; Siemens Healthcare Sector) and 8-channel knee coil. The 3-T imaging protocol included sagittal PD-weighted images (2800/19 ms and 3.0/0.3 mm), sagittal FS T2-weighted images (5100/80 ms and 3.0/0.3 mm), coronal T1-weighted images (1150/18 ms and 3.0/0.3 mm), coronal FS T2-weighted images (4600/85 ms and 3.0/0.3 mm), axial FS PD images (3650/36 ms and 3.0/0.3 mm), and oblique sagittal and coronal PD-weighted images along the AM graft plane (2800/19 ms and 2.5/0.25 mm).
The images were evaluated by 2 musculoskeletal radiologists using a PACS (picture archiving and communication system) workstation (Carestream VuePacs v11.14). Tunnel width was measured independently, and the pattern of bone tunnel ossification and the findings of tunnel communication and screw absorption were evaluated in consensus. The width of the femoral and tibial tunnels was measured in anteroposterior (AP) and mediolateral (ML) directions at the largest part of the tunnels, and the means of the measurements were used as the maximum tunnel width (Figure 1). 20 In cases of tunnel communication, the common aperture was measured and used for both tunnels (Figures 2 and 3). Tunnel width was compared with the diameter of the drill used. 20 The ossification pattern of the tunnels was divided into 3 groups: evenly narrowed (remaining tunnel of approximately constant diameter) (Figure 4), conical (remaining tunnel conical with pronounced narrowing of the distal tunnel) (Figure 4), and fully ossified (Figure 1). Tunnel communication was evaluated at the tunnel aperture and up to 1 cm distal from the joint line. 30 The biodegradable screws were evaluated and graded as completely visible (Figure 5), partially visible (Figures 3 and 4), and not visible (Figures 1 and 6). 24 In addition, the replacement of screws by bone or a fluid-filled cyst was also evaluated (Figures 1 and 6).

Measurement of the femoral anteromedial tunnel diameter using a coronal T1-weighted magnetic resonance image. The arrow indicates the fully ossified posterolateral femoral tunnel and screw.

Measurement of the common aperture of the communicating femoral tunnels using a sagittal proton density–weighted magnetic resonance image.

Measurement of the common aperture of the communicating tibial tunnels using a sagittal proton density–weighted magnetic resonance image. The arrow indicates a partially visible anteromedial tunnel screw.

A conical femoral anteromedial (AM) tunnel and an evenly narrowed tibial AM tunnel in an oblique coronal proton density–weighted magnetic resonance image. The arrow indicates a partially visible screw.

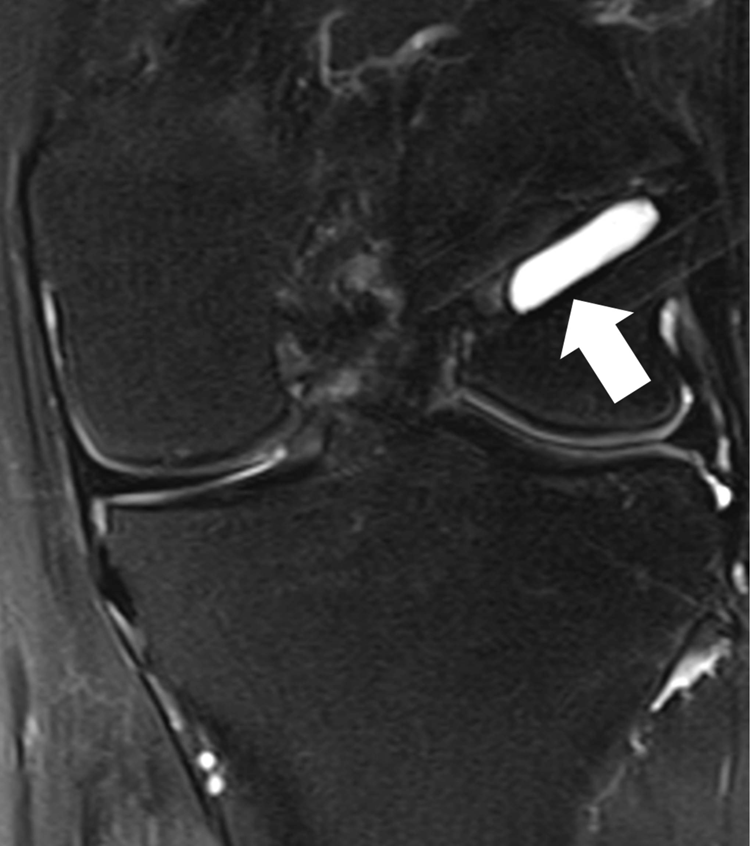
The arrow indicates the completely visible screw in the posterolateral femoral tunnel in a coronal T2-weighted fat-suppressed magnetic resonance image at 2-year evaluation.
The same patient as in Figure 5 at 5-year magnetic resonance imaging. The posterolateral femoral tunnel screw is not visible. The arrow indicates a fluid-filled cyst in the location of the resorbed screw in a coronal T2-weighted fat-suppressed magnetic resonance image.
Clinical Evaluation
The 2- and 5-year postoperative clinical evaluations were done by 2 senior orthopaedic residents. The evaluations included International Knee Documentation Committee (IKDC) and Lysholm knee scores. In the IKDC evaluation, the anterior stability and side-to-side difference of both knees was tested using a KT-1000 arthrometer (MEDmetric Corp).
Statistical Methods
The data were analyzed using IBM SPSS Statistics, version 19.0 software (IBM Corp). The statistical significance of the results was calculated using a 2-tailed t test with the significance level set to <.05. Bland-Altman interobserver agreements between the tunnel measurements were calculated using Stata 8.2 software (StataCorp LP).
Results
Between the years 2004 and 2008, 75 patients were prospectively enrolled into the study. During the first 2 years of follow-up, 8 patients were lost due to long travel distances, and 1 patient suffered a new injury and needed revision surgery. In total, 66 patients were available for MRI and 61 patients for clinical evaluation at 2-year evaluation. The mean follow-up time from surgery to 2-year MRI was 23 months (range, 17-30 months). The mean time interval from 2-year MRI to 2-year clinical evaluation was 151 days (range, 10-424 days).
The 5-year evaluation was first restricted to a random sample of 40 patients due to MRI availability, but finally, only 31 patients were available for MRI and 29 patients for clinical evaluation due to long travel distances. The mean follow-up time from surgery to 5-year MRI was 67 months (range, 46-89 months). The mean time interval from 5-year MRI to 5-year clinical evaluation was 40 days (range, 5-123 days). The mean time interval from 2-year MRI to 5-year MRI was 44 months (range, 25-63 months).
Tunnel Enlargement and Narrowing
The mean narrowing of the 4 tunnels was in total 12% between 2 and 5 years (Table 1). In Bland-Altman comparisons, the mean difference between the 2 radiologists ranged from 0.9 to 1.8 mm in the 2-dimensional measurements of the 4 tunnels.
Tunnel Diameters a

a AM, anteromedial; PL, posterolateral.
b Two-tailed t test.
Pattern of Tunnel Ossification
At the 2-year MRI, all tunnels were enlarged, with no signs of ossification. At the 5-year MRI, 44% of the tunnels were evenly narrowed, 48% were conical, and 8% were fully ossified (Table 2). The patients with evenly narrowed femoral PL tunnels had a better range of motion in knee flexion than the patients with conical PL tunnels (149° and 140°, respectively, P = .02). The other differences in clinical evaluations were small and not statistically significant.
Different Patterns of Tunnel Ossification at 5-Year Magnetic Resonance Imaging a

a AM, anteromedial; PL, posterolateral.
Tunnel Communication
Femoral tunnel communication increased from 13% to 23% of patients between 2- and 5-year MRIs. Tibial tunnel communication increased from 19% to 23% of patients during the same period. In 5-year evaluation, the patients with tunnel communication in MRI had less laxity in instrumented anterior stability measurement (side-to-side difference 1.9 mm with and 2.8 mm without femoral tunnel communication [P = .35] and 1.5 and 2.8 mm with and without tibial tunnel communication [P = .20]) and higher Lysholm scores (91 and 88 on the femoral side [P = .59] and 93 and 88 on the tibial side [P = .38]). But the differences were not statistically significant. Similarly, the differences in other clinical evaluations were small and statistically not significant.
Screw Findings
The MRI findings of the screws are shown in Table 3. In cases where screws were not visible, a fluid-filled cyst in the previous screw position was seen in 60% of patients in the femoral AM tunnels, in 47% of patients in the femoral PL tunnels, in 88% of patients in the tibial AM tunnels, and in 63% of the patients in the tibial PL tunnels. The remaining 40%, 53%, 12%, and 37% of nonvisible screws were replaced by bony ingrowth. Patients with a tibial AM tunnel cyst had higher Lysholm scores than patients without a cyst (93 and 84, respectively; P = .03). There were no other statistically significant associations with tunnel cysts found with other tunnels or clinical tests.
Biodegradable Screws in Magnetic Resonance Imaging

Discussion
This study showed that the maximum diameters of the 4 bone tunnels of DB ACLR narrowed between 2- and 5-year postoperative MRIs. Thus, our hypothesis was confirmed. The tunnel ossification pattern was described as evenly narrowed, conical, or fully ossified. Despite tunnel narrowing, tunnel communication increased during follow-up. Nearly half of the bioabsorbable
The enlargement of the bone tunnels has been seen in many studies 1 to 2 years after ACLR.
¶
The causes of tunnel enlargement are unknown and probably multifactorial, with proposed mechanical and biochemical causes.
11,36
The development of tunnel changes has been followed in 2 previous studies using serial cross-sectional imaging.
9,35
In the study with serial CT follow-up, the SB ACLRs were completed using the transtibial technique, and the bone–patellar tendon–bone (BPTB) graft was fixed with titanium interference screws.
9
In the study with serial MRI follow-up, the SB ACLRs were also completed using the transtibial technique, and both BPTB grafts and hamstring tendon grafts were used with bioabsorbable
In studies on tunnel enlargement after DB ACLR, the follow-up times have ranged from 8 to 26 months, and enlargement of the 4 tunnels increased up to 50%. 1,16,20,23,29,30 We are not aware of previous studies that have compared 2- and 5-year postoperative MRI tunnel measurements after DB ACLR. Our result of tunnel narrowing between 2- and 5-year MRIs is similar to the only previously published finding of tunnel narrowing after SB ACLR with shorter follow-up. 35 In cases with conical tunnels in our study, the maximum diameter was measured at the large tunnel aperture, although most of the ossification was seen in the narrowed distal part of the tunnel. The method of maximum diameter measurement was chosen instead of tunnel volume calculation for better reproducibility and usefulness in clinical work. In addition, in cases with tunnel communication, the diameter of the common aperture was used for both tunnels. Thus, our result of tunnel narrowing underestimates the total amount of ossification. Based on previous studies and our results, after ACLR, the bone tunnels first enlarge until 6 months and thereafter slowly narrow between 6 months and 2 years, and the narrowing continues for at least 5 years after surgery. 35
Interestingly, in another study with 5-year postoperative MRI, not all tunnels were enlarged, which might, in our opinion, reflect early tunnel enlargement and subsequent narrowing, resulting in a nearly original drill diameter at 5 years. 21 In a previous DB ACLR study, some tunnels were fully ossified as early as 2 years after surgery, but in our findings, the tunnels were enlarged 2 years postoperatively, and only a few were fully ossified at 5 years. 23
Our conical tunnel ossification pattern finding is similar to a recent SB ACLR study that used the same bioabsorbable
The absorption rate of different biodegradable screws is variable and depends, among other factors, on the material construct and the degree of crystallization.
22,33
In long-term follow-up, PLLA screws have taken 10 to 16 years to fully absorb and ossify, and cyst formation has been frequent but not associated with adverse outcome.
31,33,34
In 5-year follow-up, PLLA-hydroxyapatite (PLLA-HA) screws were partially absorbed and incompletely ossified.
2
In studies of β-tricalsium phosphate PLLA (β-TCP-PLLA) screws, almost complete ossification was seen 3 to 4 years postoperatively.
3,25
In 2- to 4-year follow-up, β-TCP polylactic-co-glycolic acid (β-TCP-PLGA) screws were partially absorbed and not ossified.
4,7
In a previous study of the same
The limitations of our study include the mean time of 44 months between the MRI studies that prevented a more detailed analysis of the changes in the tunnels and the screws between 2 and 5 years postoperatively. The total follow-up time also varied from 46 to 89 months, which increased the possibility that different tunnel shapes and screw absorption findings may reflect different stages of these slow processes. The third and most important limitation is the possible patient selection bias, as we were able to evaluate only 31 of 66 patients in 5-year follow-up. The remaining patients were lost due to noncompliance and geographical restraints. The strengths of the study are long follow-up time, prospective study setting, and the good image quality of the 3-T MRI used in the 5-year evaluations.
Conclusion
Our study is the first to use MRI to evaluate tunnel changes 5 years after DB ACLR. Tunnel narrowing caused by bony ingrowth progressed slowly between 2 and 5 years after surgery and resulted in both evenly narrowed and conical tunnels. The biodegradable interference screws, once absorbed, were replaced by fluid-filled cysts and bone. The MRI findings of tunnel communication and tunnel cysts were frequent but not associated with a worse clinical outcome.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Ethical Committee of Tampere University Hospital.
Acknowledgment
The valuable help of Anna-Stina Moisala, MD, PhD, in the 2-year clinical evaluations is sincerely acknowledged.