
Abstract
Background:
Arthroscopic procedures may be technically challenging because of impaired vision, limited space, and the 2-dimensional vision of a 3-dimensional structure. Spatial orientation may get more complicated when the camera is pointing toward the surgeon.
Hypothesis:
Spatial orientation and arthroscopic performance may be improved by simply mirroring the image on the monitor in different configurations regarding the position and orientation of camera and instrument.
Study Design:
Descriptive laboratory study.
Methods:
Thirty volunteers from an orthopaedic department were divided into 3 equal groups according to their arthroscopic experience (beginners, intermediates, seniors). All subjects were asked to perform a standardized task in a closed box mimicking an endoscopic space. The same task had to be performed in 4 different configurations regarding camera and instrument position and orientation (pointing toward or away from the subject) with either the original or mirrored image on the monitor. Efficiency (time per stick; TPS), precision (successful completion of the task), and difficulty rating using a visual analog scale (VAS) were analyzed.
Results:
Mirroring the image demonstrated no advantage over the original images in any configuration regarding TPS. Successful completion of the task was significantly better when the image was mirrored in the configuration with the camera pointing toward and the instrument away from the surgeon. There was a positive correlation between TPS and subjective VAS difficulty rating (r = 0.762, P = .000) and a negative correlation between the successful completion of the task and VAS (r = −0.515, P = .000).
Conclusion:
Mirroring the image may have a positive effect on arthroscopic performance of surgeons in certain configurations. A significantly improved performance was seen when the arthroscope was pointing toward and the grasping instrument pointing away from the subject. Mirroring the image may facilitate surgery in such clinical situations.
Clinical Relevance:
Mirroring the image may facilitate arthroscopic procedures in certain clinical situations.
Arthroscopic techniques have revolutionized joint surgery in many aspects. The advantages of a minimized and soft tissue preserving surgical approach combined with an excellent overview of the articular anatomy are generally accepted. 3 The development of modern arthroscopes with different angles of view, a broad spectrum of arthroscopic instruments, and sophisticated surgical techniques has widened the field of current arthroscopic procedures. However, arthroscopic procedures may be technically challenging due to impaired vision, limited space to maneuver inside the joint, and the 2-dimensional vision of a 3-dimensional structure. 1,4 A particular challenge is the indirect visualization of the operative field via the camera onto a screen instead of direct view on the manual task. The most “natural” view is obtained if the surgeon is behind both the camera and instrument, both pointing away from the surgeon and toward the monitor. With this configuration, spatial orientation and movements correspond with the image on the monitor. However, in practical surgery, this configuration is not always achieved, for example, in a situation with the arthroscope pointing toward the surgeon. This unfavorable camera position in relation to the surgeon reverses both the anterior-posterior axis and the right-left orientation. The spatial orientation may get more complicated, accompanied with a decreased level of precision and an increase of time-consuming maneuvers. With repeated exposure to such situations and increasing surgical skills, the surgeon may learn to master these challenges. However, spatial orientation may be facilitated by simply mirroring the image on the monitor. By applying a vertical axis to mirror the image, the reversal of the anteroposterior axis remains unchanged, but the right-left orientation may be reversed according to the surgeon’s original orientation. It was the objective of this study to investigate the effect of a mirror image on arthroscopic manipulations in an experimental model. We hypothesized that mirroring the image may increase the spatial orientation and surgical precision in different configurations regarding the position and orientation of camera and instrument.
Methods
Test Subjects
Thirty volunteers, all employed by the Department of Orthopaedic Surgery of a university hospital, served as test subjects. Only subjects with right-hand dominance (n = 29) or ambidexterity (n = 1) entered the study to exclude any bias arising from mixed-hand dominance within the 3 groups. These subjects were divided into 3 groups of similar size (n = 10) according to their arthroscopic experience. In the “beginners” group, only medical students in their final year of medical school who had no prior exposure to arthroscopic or any other endoscopic surgery were accepted. In the “intermediate” group, residents with some arthroscopic experience (10-100 arthroscopic procedures) were tested. Subjects with an experience of more than 100 arthroscopic procedures were grouped as “seniors.”
Experimental Setup
A small closed black plastic box was designed (110 × 80 × 60 mm) to mimic an endoscopic space. The interior of the box was not visible from the outside from any angle. On the 2 narrower opposing side walls (80 mm), 2 holes were drilled 30 mm above the sole plate at a distance of 40 mm to each other. These holes served as endoscopic ports. The floor of the box was covered with a 10-mm-thick foam layer to facilitate endoscopic manipulation of objects fallen on the floor. Two identical double lines with 2 × 3 tubes (20 × 15 × 12 mm) were placed in the box in a symmetrical configuration. A wooden stick of 20 × 2 mm was placed in each of the 6 tubes on the right side.
The same standard 30° arthroscope (Fa Karl Storz Endoscopes) and arthroscopic grasping forceps were used for all experiments. To complete the setup, the box was placed on a table. The arthroscope was connected to a light source and to a monitor. For the test configurations with the original (unmirrored) image, the monitor was placed in line with the box and the operator. The ports of the box were facing either the operator or the monitor in the different configurations of the experiment. For the mirrored configurations, the monitor was replaced by a mirror at the same distance and angle. The monitor itself was placed at the left side of the operator facing the mirror to produce an exact mirrored image of the original of equal size and without any distortion. The placement of the monitor in this configuration did not allow any visualization of the original image on the monitor by the test subjects to exclude any bias of the experiments (Figure 1).

Schematic setting in mirroring the arthroscopic image with a conventional mirror. In this setting, the test subject had no direct view of the original image. Distance with and without the mirror was kept constant.
Test Configurations
Four different configurations (Figure 2) for the placement of the arthroscope and grasping instrument were investigated. The task configurations were determined as follows: configuration A, arthroscope and grasping instruments were introduced through the left and right ports of the side of the box facing the operator, both pointing away from the operator. In configuration B, the arthroscope was introduced through the left port of the side of the box facing the operator and pointing away from the operator. The grasping instrument was introduced into the box from the right port of the opposite side of the box pointing toward the operator. In configuration C, the arthroscope was placed through the left port on the opposite side of the box, pointing toward the operator. The grasping instrument was placed on the right side of the wall facing the operator and pointing away from the operator. In configuration D, both the arthroscope and the grasping instrument were introduced through the ports from the opposite side of the box pointing toward the operator.

Task configurations A to D after completion when all sticks were placed in the tubes on the left side. (A) Task A is performed with the camera and instrument pointing away from the subject. (B) The camera is pointing away and the instrument toward the subject in task B. (C) Task C is performed with the camera pointing toward and the instrument away from the subject. (D) Both camera and instrument are pointing toward the subject in task D. The box cover is not shown; it inhibits direct vision of the setup. The camera is always held in the left hand and inserted through the left portal.
Each of the above-described configurations was also tested by using a mirrored image of the original view. The configuration with the mirrored image of configuration A was designated A–. The mirrored configurations B, C, and D were designated accordingly B–, C–, and D–.
Tasks, Rules, and Outcome Measurements
The same rules were applied for all tasks: The arthroscope was to be guided by the left hand and the grasping instrument with the right. It was the objective of the tasks to transfer the 6 sticks from the right double-line of cylinders into the cylinders located on the left side of the box, 1 stick in each cylinder. If a stick fell to the floor during the task, the operator was allowed to retrieve it. A maximum time of 20 seconds was allowed to pick up the stick again. If the stick could not be retrieved within these 20 seconds, the operator had to move on to the remaining sticks. However, the task was considered incomplete. For a successful completion of the task, all sticks had to be transferred into the designated cylinders. Time per stick (TPS) was calculated by dividing the total time to finish the task by the number of sticks that were successfully placed in the designated cylinders.
Each operator had 1 attempt to complete the task for every of the 4 configurations, adding up to a total of 8 tests (4 original views and 4 corresponding mirrored images). One half of each group started with the original views, the other with the mirrored images in order to avoid a uniform training bias. No pretest practicing was allowed to exclude a potential learning effect.
After the 8 attempts, every operator was asked to rate the level of difficulty for every task by applying a visual analog scale (VAS) ranging from 0 (very easy) to 100 (extremely difficult), which is a commonly used rating tool. 6,7
Statistical Evaluation
Statistical analysis was performed using SPSS 21.0 (version 21.0; IBM Corp). As data did not show normal distribution, the Mann-Whitney U test was used to assess differences of the outcome parameters (TPS, VAS difficulty rating, and rate of completion of tasks) between the different groups. P < .05 was considered statistically significant.
Results
Time per Stick
Overall, median TPS was significantly longer when the image was mirrored in configurations A and B (camera pointing away from operator) compared with the original image (A, 14.3 vs A–, 62.8 seconds [P < .01]; B, 30.0 vs B–, 52.5 seconds [P < .05]. In contrast, mirroring the image had no significant influence in configurations C and D (camera pointing toward operator) (C, 51.6 vs C–, 39.1 seconds [P > .05]; D, 59.5 vs D–, 63.3 seconds [P > .05]).
Subgroup analysis showed that TPS in configuration A was significantly longer when the image was mirrored for all different level of experience (P < .01) (Figure 3). In configuration B, TPS was longer for beginners when the image was mirrored (P < .05), whereas no influence of mirroring was observed for intermediates and seniors. However, the seniors completed the tasks faster than beginners when the image was mirrored in configuration B (P < .05). The level of experience had no significant influence on all the other tasks.

Time per stick (TPS) for tasks A to D (original images) and tasks A– to D– (mirrored images). (A) In the overall results, mirroring of tasks A and B led to significantly longer TPS. (B) Subgroup analysis for TPS showed a pronounced disadvantage in mirrored tasks A and B when performed by the less-experienced subjects. Error bars indicate 95% CIs. Statistically significant between-group difference: *P < .05 and **P < .01, mirrored versus not mirrored; # P < .05, beginners versus seniors.
Successful Completion of Tasks
Completion rate was very high (97%) in configuration A (Figure 4). It was significantly lower in all other configurations compared with A (P < .01: A vs A–, B, B–, C, D, and D–; P < .05: A vs C–). The lowest completion rate was achieved in configuration D (42%). Mirroring significantly reduced the completion rate of task A (62% vs 96%; P < .01). In contrast, mirroring was associated with a better completion rate in task C– when compared with task C (73% vs 46%; P < .05).

Successful completion of tasks A to D (original images) and tasks A– to D– (mirrored images). (A) In the overall results, a significant advantage was observed when task C was mirrored. (B) The subgroup analysis showed similar results for the 3 experience subgroups, with a pronounced positive effect of mirroring task C for intermediates and less success for seniors. The seniors had less difficulty completing mirrored task A compared with the beginners and intermediates. Statistically significant between-group difference: *P < .05 and **P < .01, mirrored versus not mirrored; § P < .05, intermediates versus seniors.
VAS Difficulty Rating
Mirroring configuration A significantly increased the subjective VAS difficulty rating in all groups, unrelated to their experience (Figure 5). Mirroring had no significant effect on the difficulty rating in all other configurations.
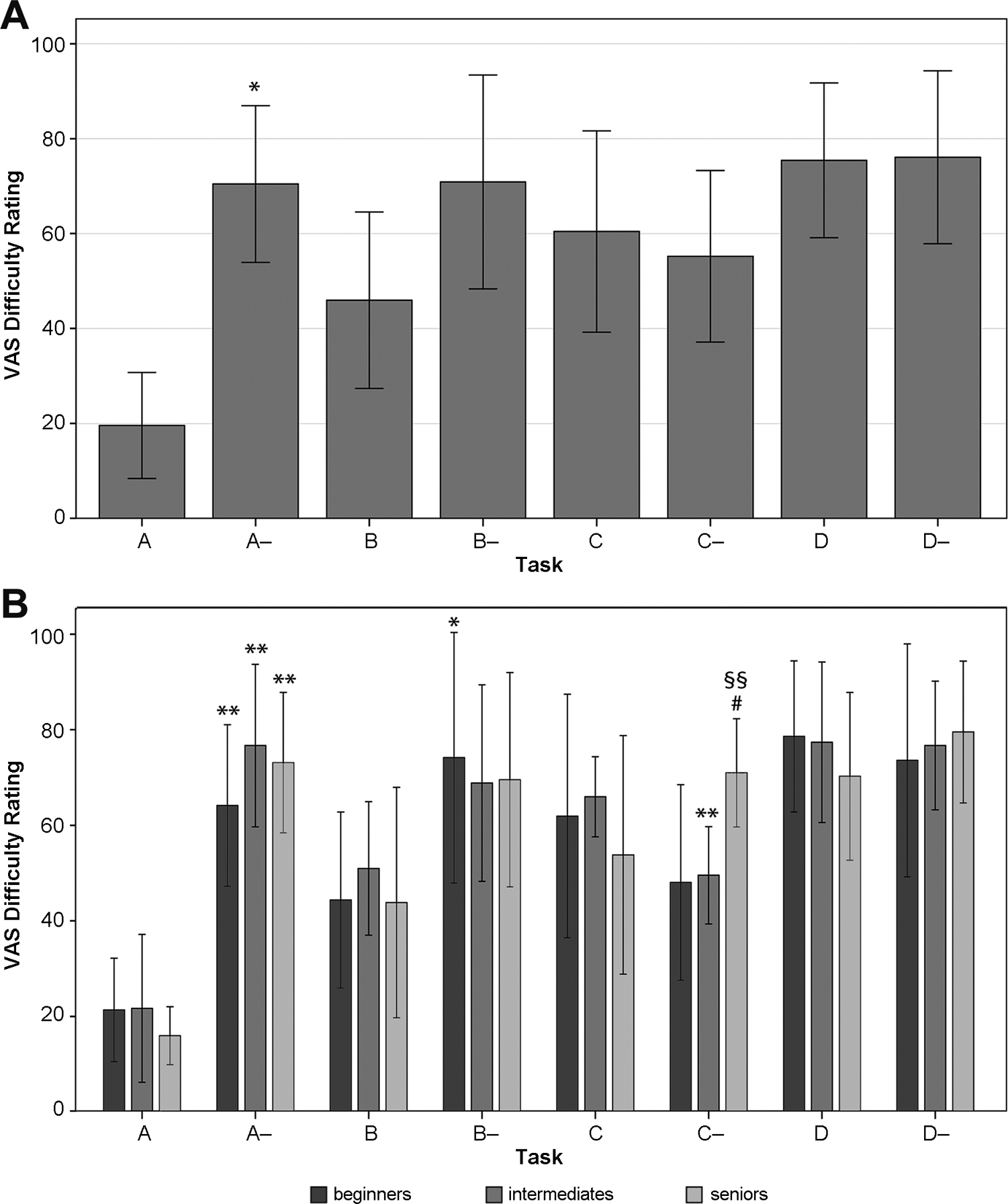
Visual analog scale (VAS) difficulty rating for tasks A to D (original images) and tasks A– to D– (mirrored images). (A) In the overall results, the VAS difficulty rating was significantly different only when task A was mirrored. This unfavorable effect was expected, as task A was also rated easier than the other tasks. Task D was rated as difficult, independent of mirroring. Error bars indicate ±1 SD. (B) Subgroup analysis showed a beneficial effect for intermediates when performing C as a mirrored task, whereas seniors rated mirrored task C as significantly more difficult compared with beginners and intermediates. Error bars indicate 95% CIs. Statistically significant between-group difference: *P < .05 and **P < .01, mirrored versus not mirrored; # P < .05, beginners versus seniors; §§ P < .01, intermediates versus seniors.
Subgroup analysis revealed a heterogeneous pattern. The mirrored configuration C was rated significantly more difficult by seniors compared with intermediates (P < .01) and beginners (P < .05). Intermediates rated the task in the mirrored configuration C easier than in the original setting C (P < .01). For beginners and seniors, mirroring had no influence on the difficulty level in C.
Correlation Between Objective and Subjective Outcome Parameters
There is a positive correlation between TPS and the subjective VAS difficulty rating (r = 0.762, P = .000). A negative correlation was seen between the successful completion of tasks and the subjective VAS difficulty rating (r = −0.515, P = .000).
Discussion
Our experiments demonstrate a potential positive effect on performance of endoscopic manipulations when the original endoscopic image is mirrored and the camera was pointed toward the operator with the instrument pointing away (configuration C). In this configuration, a movement of the instrument to the left and away as guided by the operator is visualized as a movement to the right and toward the camera on the screen. Mirroring this image results in a leftward movement but the instrument is still moving toward the operator as seen on the screen. In other words, mirroring corrects the visualization of a sideward movement when the arthroscope is pointed toward the operator whereas it has no effect regarding anterior to posterior movements.
Our analyses clearly show that mirroring this configuration increased the overall rate of completed tasks significantly, although no effect was seen regarding time to complete the task. Of interest is the observation that the improved rate of completed tasks was not uniform among the different groups of experience. Intermediates performed significantly better when this configuration was mirrored but there was no significant improvement seen for beginners and seniors. Furthermore, intermediates found that the difficulty of the task was significantly lower when the image was mirrored in this configuration. On the other hand, the VAS difficulty rating for the mirrored image was considered significantly higher by seniors than by the other groups. The reasons for these observations remain unclear. One could hypothesize that seniors have learned to cope with this configuration with increasing experience and mirroring this configuration is a new situation they have not learned to cope with yet, and thus, the potential benefit did not pay off immediately. Intermediates with limited experience might have more quickly adapted to the mirror effect, resulting in a significant benefit, both by objective and subjective measurements. However, beginners did not demonstrate any benefit from image mirroring.
We only investigated the immediate effect of image mirroring on subjects with different levels of experience. Because of this study design, we cannot comment on long-term results regarding the training effect with image mirroring. If introduced during an early stage of arthroscopic training, image mirroring may be beneficial to cope with configurations when the camera points toward the surgeon. It may also be beneficial for more experienced surgeons once they get used to it.
As expected, mirroring had a negative effect on performance, and it was rated more difficult by all subjects in the standard configuration with the camera and the instrument both pointing away from the operator. In contrast, mirroring the original image may improve the surgeon’s arthroscopic performance when the camera points toward the surgeon. In conclusion, an optional electronic on-demand activation and deactivation of a mirrored screen view may therefore be regarded as a relevant potential benefit and welcome additional feature of current arthroscopic equipment.
Limitations
Only 30 subjects, divided into 3 groups of different experience levels, were tested. Furthermore, we investigated only 1 endoscopic task with different configurations regarding the position of the camera and instrument. The tasks mainly required instrumental movements in the right-left axis and less forward or backward maneuvers. Thus, the tasks may not represent a realistic clinical situation. However, since the effect of mirroring the image on performance and subjective difficulty rating of the tasks were our main outcome parameters, this limitation may be of minor significance. A standard arthroscopic knee or shoulder trainer would have come with several potential biases. It was not our intention to test the anatomic knowledge of the subjects or specific arthroscopic skills. We focused on spatial orientation and the effect of image mirroring in a simple endoscopic setting.
The lack of significance between some groups and tasks may be related to the rather limited sample size. An a priori power analysis to determine the needed number of subjects was not possible due to the lack of any data regarding the effect of image mirroring in the current literature.
The subjects for this study were chosen according to their arthroscopic experience, which only correlates with performance in testing basic arthroscopic skills in simulators along with postgraduate years. 4,5 Despite the division into 3 groups with different arthroscopic experience, there was a considerable heterogeneity within the groups with regard to the individual performance. Other features and individual skills that may influence the subjects’ performance such as laterality, eye-hand coordination, or spatial sense were not evaluated. 2 Thus, the results from the subgroup analyses should be treated with caution.
Intermediates and even more seniors had certainly accumulated a considerable amount of experience in dealing with different configurations during their surgical career. In contrast, only the immediate effect of image mirroring was studied without previous training and time to adapt to this potential facilitation. Thus, the true value of the mirror image may be underestimated in this study.
Conclusion
Mirroring the image may have a positive effect on arthroscopic performance of surgeons in certain configurations. However, this observation is not uniform. A significantly increased performance was seen when the arthroscope was pointing toward and the grasping instrument pointing away from the operator. Mirroring the image may facilitate surgery on such occasions. To gain a potential value in the clinical situation, more experimental and clinical tests are required.
Footnotes
Acknowledgment
The authors thank Michel Schlaeppi, PhD, for his contribution to the statistical analysis and Mark Rudin, MD, for his work on the manuscript.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not sought for the present study.