
Abstract
Background:
Muscle strength of the involved limb is known to be decreased after injury. Comparison with the uninvolved limb has become standard of practice to measure progress and for calculation of limb symmetry indices (LSIs) to determine readiness to return to sport. However, some literature suggests strength changes in the uninvolved limb also are present after lower extremity injury.
Purpose:
To examine the uninvolved limb strength in a population of adolescent athletes after an anterior cruciate ligament (ACL) injury and compare strength values with those of the dominant limb in a healthy control group.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 64 athletes were enrolled in this study, including 31with injured ACLs (mean age, 15.6 ± 1.4 years) and 33 healthy controls (mean age, 14.9 ± 1.9 years). The median time from injury to testing was 23 days for the ACL-injured group. Participants underwent Biodex isokinetic strength testing at 60 deg/s to assess quadriceps and hamstring strength. Isometric hip strength (abduction, extension, external rotation) was measured using a handheld dynamometer. The muscle strength of the uninvolved limb of the ACL-injured group was compared with that of the dominant limb of the healthy control group.
Results:
The results showed a significant difference in quadriceps muscle strength between the 2 study groups (P < .001). Isokinetic quadriceps strength of the uninvolved limb in the ACL group was significantly decreased by 25.5% (P < .001) when compared with the dominant limb of the control group.
Conclusion:
The results of this study demonstrate a decreased isokinetic strength of the quadriceps muscle in the uninvolved limb after ACL injury as compared with healthy controls. Consideration should be taken when using the uninvolved limb for comparison when assessing quadriceps strength in a population with an ACL injury.
Anterior cruciate ligament (ACL) disruption is a common cause of knee instability and dysfunction, with a reported incidence between 36.9 and 60.9 per 100,000 persons per year. 6,16 It is reported that up to 250,000 ACL reconstructions (ACLRs) are performed each year in the United States, with over 50% of cases involving those between the ages of 15 to 25 years who practice sports. 14 Given the high rate of injury and subsequent surgery, ACL injury, reconstruction, and rehabilitation have been a topic of interest among clinicians and researchers for years.
One area of recent interest has been in the return-to-sport phase of rehabilitation. Typically, athletes are put through a battery of tests that measure range of motion, strength, and power. Historically, measurements are taken on both the involved and uninvolved limb and limb symmetry indices (LSIs) are recorded, with a goal for the injured limb to be within 80% to 90% of the uninvolved limb. 9,18,23 Subjects are subsequently released or not released based on the results of the testing; however, more recently, concerns have been raised regarding the efficacy of this practice. Specifically, whether comparing the involved limb to the uninvolved limb at the time of release is an appropriate comparison. 26 Detraining of the uninvolved limb due to inactivity and possible neuromuscular changes after contralateral injury and the high rate of contralateral ACL tears have raised concerns regarding this practice. 26
Quadriceps muscle strength has been examined extensively, and despite a plethora of research, findings consistently demonstrate muscle strength asymmetries of up to 80% at time of release and up to 2 years after surgery. 2,7,13,15,17,19 To support this concern regarding LSI, research has shown that after ACLR, quadriceps muscle cross-sectional area is decreased compared with the uninvolved side, and this has been shown to be directly correlated with decreased strength in this population. 21 One way of measuring this is through the use the central activation ratio (CAR), which is the ratio between a person’s maximal voluntary contraction divided by their maximal voluntary contraction with the addition of superimposed stimulation. This has also been found to be decreased bilaterally after ACLR, resulting in what is defined as bilateral quadriceps activation failures (QAFs). 7 These findings support the notion that bilateral comparisons after ACLR are problematic as the uninvolved limb may also be decreased. A solution that has been proposed to help resolve this issue is to compare the rehabilitated limb at time of return to sport with the uninvolved limb immediately after or after injury to generate a comparison known as estimated preinjury capacity (EPIC). 29 This scenario would allow a snapshot assessment of the healthy limb when the subject is still active and before deconditioning could occur. Whereas this seems like a reasonable suggestion, currently, little literature is available to support this method.
Therefore, the purpose of this study was to examine the uninvolved limb strength in adolescent athletes after an ACL injury and in comparison with the dominant limb strength in a healthy control group. We hypothesized that uninvolved limb strength in adolescent athletes who had suffered an ACL injury would be similar to dominant limb strength in a group of healthy adolescent controls.
Methods
A total of 64 participants who met inclusion criteria were enrolled in this study, 31 with ACL injuries and 33 healthy controls. Table 1 displays the characteristics of the participants for both groups. All participants were screened before enrollment by the study staff to assess inclusion eligibility. For both groups, participants were considered for the study if they were between the ages of 13 and 25 years and if they were involved in a level 1 sport (eg, basketball, football, or soccer). For the ACL-injured group, eligible participants were enrolled if they injured their ACL for the first time and did not have any full-thickness chondral injuries or grade 2 or 3 medical collateral ligament (MCL), lateral collateral ligament (LCL), or posterior collateral ligament (PCL) injuries. For the control group, eligible participants were enrolled if they were not experiencing an active lower extremity orthopaedic injury and had not been injured within the past 3 months. After the screening process, if the participants were eligible, they were invited to participate in the study. All participants gave informed consent to participate, and the rights of each person were protected. If the participant was a minor, parental consent and child assent were attained. After enrollment in the study, each participant’s anthropometric data (height, weight) were measured using a Weigh Beam eye-level scale (Detecto), and each participant completed a demographic information sheet that included injury history and sports participation. For the ACL-injured group, the median time from injury to testing was 23 days (interquartile ratio [IQR], 13.5-42.5 days). We did not control for activity level from time of injury to time of testing; however, all participants were ambulating without assistive devices and were part of a prehabilitation program with their athletic trainer and/or physical therapist, and all subjects went on to have surgery.
Characteristics of Participants for Each Group a

a ACL, anterior cruciate ligament; NA, not applicable.
b Statistically significant difference between groups (P < .05).
c There were 14 repairs and 7 debridements.
Biodex Testing
The Biodex Multi-Joint Testing and Rehabilitation System (Biodex Medical Systems) was used for testing isokinetic quadriceps muscle strength. Participants were seated on the Biodex system and secured with padded straps around the thigh, pelvis, and torso to minimize accessory and compensatory movements during testing. 4,11 The femoral condyle of the tested limb was aligned with the Biodex axis of rotation following the manufacturer’s instructions. Participants performed 5 repetitions of submaximal knee extension/flexion to familiarize themselves with the testing motion. To determine knee strength for both the quadriceps and hamstring muscles, participants performed 5 consecutive concentric contractions at 60 deg/s. 3 The uninvolved side of participants in the ACL-injured group and the dominant side of healthy participants were tested. The dominant limb was defined as the limb the subject reported as the limb they would choose to kick a ball with. Finally, the average of the 5 trials was normalized to body weight and used for data analysis. 11
Hip Strength Testing
Isometric hip strength was measured in 3 distinct directions of abduction, extension, and external rotation. These directions were chosen as weaknesses in these movements have been studied as possible contributing factors to ACL injuries. 5,28 All measurements were taken using the “break test” method with a handheld dynamometer (MicroFET 2; Hoggan Scientific LLC). 22 A handheld dynamometer, rather than the Biodex system, was selected for assessing hip muscle strength because of time constraints involved with the clinical nature of the study. In addition, the use of a handheld dynamometer to determine hip muscle strength was the standard clinical testing protocol at the affiliated institution. For hip muscle strength testing, the clinician stabilized the proximal segment of the participants at the hip and then instructed the subject to push maximally into the dynamometer for a duration of 3 to 5 seconds. Measurements were taken by the same physical therapist to ensure consistency. In addition, a pilot reliability study was performed on 10 healthy participants who were included in the control group. The intrarater reliability was found to be good for hip abduction (intraclass correlation coefficient [ICC], 0.96; 95% CI, 0.85-0.98), hip extension (ICC, 0.98; 95% CI, 0.93-0.99), and hip external rotation (ICC, 0.87; 95% CI, 0.59-0.97]).
For hip abduction (Figure 1A), participants were placed in a side-lying position. A belt was used to help stabilize the subject’s pelvis to the table. The limb that was closest to the table was placed in approximately 30° of hip flexion with 90° of knee flexion. 8,20 The participant’s test limb was taken into a neutral position (relative to abduction/adduction) and slight hip extension. The dynamometer was placed just proximal to the subject’s tibiofemoral joint line. The clinician helped to stabilize the pelvis while the subject was instructed to push maximally into the dynamometer.
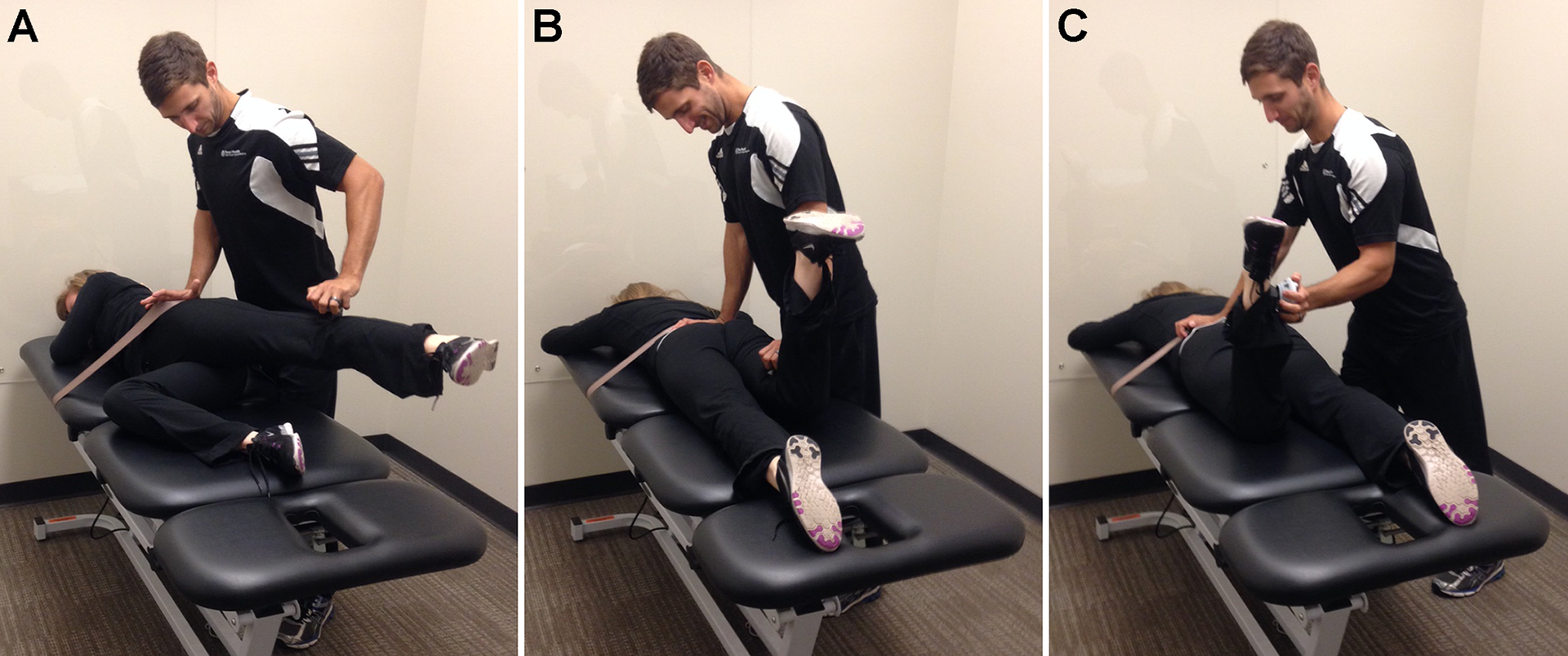
Hip muscle strength testing: (A) abduction, (B) extension, and (C) external rotation.
Hip extension (Figure 1B) was tested in the prone position, and a belt was utilized to assist in stabilizing the participant’s pelvis. 8,20 The testing limb knee was flexed to 90°, and the dynamometer was placed at the most distal aspect of the posterior thigh. The clinician helped to stabilize the proximal segment at the hip while the subject was instructed to push maximally into the dynamometer.
Hip external rotation (Figure 1C) was measured in prone using a belt to assist in stabilizing the subject’s pelvis. The knee of the testing limb was flexed to 90°. 8,20 The tester stood on the opposite side of the testing limb to apply appropriately directed pressure. The dynamometer was placed at the medial malleolus of the testing limb.
Three trials were completed on each limb, with a 30-second rest between each consecutive contraction. The average of the 3 trials was used for data analysis and all measurements were normalized to body weight.
Statistical Analysis
All data analyses were performed using SPSS version 23 (IBM Corp). To compare the characteristics of the participants between the 2 groups, independent t tests were used to examine age, height, and weight, and chi-square tests were used to examine sex, limb dominance, and side of injured limb for the ACL-injured group. Before statistical analyses, all hip and knee strength data were assessed for normality and for outliers. Two separate 1-way multivariate analyses of variance (MANOVAs) were used to assess between-group differences in muscle strength, one for knee and the other for hip, because the units of measurement for hip and knee muscle strength were not the same. If significance was found, univariate analyses of variance (ANOVAs) were followed. The alpha level was set at P < .05 for all statistical analyses.
Results
Chi-square statistics showed a significant difference (P = .000003) in the distribution of men/women between the 2 groups, with only 2 men out of 33 healthy compared with 17 men out of 31 participants with an ACL injury.
Table 2 lists the normalized hip and knee muscle strength for both groups. Follow-up univariate ANOVAs revealed a significant difference in the normalized quadriceps muscle strength between the 2 groups (P < .001) but not for normalized hamstrings muscle strength (P = .414). In addition, the MANOVA used to assess hip strength variables (external rotation, extension, and abduction) showed no significant differences (P = .472).
Strength Measures for Each Group a

a Strength measures were normalized to body weight (BW). ACL, anterior cruciate ligament; ICC, intraclass correlation coefficient.
b Statistically significant difference between groups (P < .05).
Discussion
The results of this study indicate that there was quadriceps muscle weakness of the uninvolved limb after an ACL injury compared with the dominant limb in healthy controls. Historically, limb symmetry indices are calculated between the involved and uninvolved limb for strength testing to determine readiness to return to sport. More recently, it has been suggested that using the preoperative strength of the uninvolved limb may be a more accurate comparison. However, this finding suggests that using the muscle strength of the preoperative uninjured limb for comparison may not be ideal at time of injury. Interestingly, the results indicate that there were no group differences in the hip muscles between the uninvolved limb of those injured and those of healthy controls. There also were no differences in knee flexion muscle strength between the uninjured limb of injured athletes and the dominant limb of the healthy control group. Had muscle weakness throughout the uninvolved limb been found, an argument for general deconditioning could be made. However, the only difference seen was in the strength of the quadriceps muscles.
This selected quadriceps muscle weakness on the uninvolved side is consistent with previous literature that examined voluntary quadriceps muscle activation using twitch interpolation, which is a measure of muscle activation through superimposed stimulation. In 2 separate studies, Urbach and Awiszus 23 found a bilateral decrease in volitional quadriceps activation in an ACL-injured population as compared with healthy controls. The decrease in the uninjured limb was explained by a decrease in voluntary activation. In a follow-up study, Urbach et al 24 reported a more significant decrease in quadriceps activation when subjects sustained an ACL injury with accompanying joint damage as compared with those with an ACL injury only and as compared with healthy controls. A limitation to these studies is that the median time from injury to testing was 119 days, with the longest gap in time from injury to time of testing being 54 months. In the current study, the median time from injury to testing was only 23 days, which suggests that bilateral quadriceps activation failure occurs relatively quickly. These results have strong implications on the focus of preoperative strengthening and the need to immediately begin addressing not only the involved limb but also the uninvolved limb with directed rehabilitation. Chmielewski et al 1 examined 100 consecutive subjects who sustained an ACL injury and underwent 4 weeks of preoperative therapy with a mean time from injury to testing of 6 weeks. They reported that at time of testing, 21% of their subjects had bilateral quadriceps activation failure (QAF). 1 Although the current study did not measure QAF, the quadriceps muscle strength deficit in the uninvolved side could be an indication of QAF 7,27 and is a more clinically measurable variable. As such, our results are in line with those of previously published work that demonstrated deficits in quadriceps muscle strength of the uninvolved limb after unilateral injury.
In the context of unilateral deficits after joint injury, arthrogenic muscle inhibition (AMI) has been suggested as the underlying cause. 7 AMI after joint injury results in the body altering neural drive to surrounding musculature in an effort to protect the joint. It has been suggested that the mechanism behind AMI is the altered afferent input from mechanoreceptors in the joint resulting in reduced efferent output from the quadriceps alpha motor neurons, resulting in decreased muscle activation. 7 Although this explanation is widely accepted for decreased strength of the injured limb, it also helps explain deficits in the uninjured limb. Urbach et al 23 –25 suggested that a central mechanism is responsible for “adjusting the bilateral fusimotor-muscle-spindle system in cases of joint pathology” resulting in the bilateral deficits. Similarly, Konishi et al 10 demonstrated gamma loop dysfunction in the uninjured quadriceps femoris muscle of patients with unilateral ACL injury. These authors reported these subjects had an abnormal response to prolonged vibration stimulation compared with a control group. These findings suggest an abnormal gamma loop function in the uninjured limb, and normal gamma loop function is necessary to exert maximal voluntary contraction. As an explanation, Konishi et al 10 suggested 2 possible mechanisms to explain the bilateral quadriceps deficit. The first is that the afferent feedback from the ACL-ruptured side could send inhibitory signals to the quadriceps femoris muscle of the intact contralateral leg via interneurons in the spinal cord. The second is that inhibitory signals in the supraspinal system, such as the brain and motor cortex, could result in bilateral quadriceps weakness in patients with ACL injury. 10 This previous research provides a working theory and explanation for bilateral activation deficits after ACL injury. This may also help explain why no differences in the current study were found in either the knee flexors or the more proximal hip muscles on the uninjured limb.
The findings from the current study and from previous work may have many clinical implications. First, it is clear that bilateral QAF resulting in decreased muscle strength is present subsequent to and occurs quickly after ACL injury and may be present for an extended period of time after injury. 1 This implies that there is a strong need for immediate preoperative therapy aimed at restoring quadriceps strength of the uninvolved limb. In addition, it also suggests that preoperative quadriceps strength of the uninvolved limb may not be an adequate comparison for LSI values for release from physical therapy or return to sport. Further research is warranted to compile a database of age- and sex-matched healthy controls for comparisons of quadriceps muscle strength for release from physical therapy and for the return-to-sport decision. This would provide a more accurate value for comparison to help determine whether a patient has restored full muscle strength. Based on the results of the current study, other strength values (knee flexion, hip abduction, hip extension, and hip external rotation) used for comparison to the preoperative uninvolved limb are acceptable, as no differences were found between the uninvolved limb and the dominant limb of healthy controls in these tests.
There are limitations to this study. First, the current study did not control for activity from time of injury to time of testing; however, all individuals remained active as they were attempting to return to sport after surgery. Additionally, this study did not control for lower limb length in calculation of hip strength; however, the data were normalized to body weight and this is consistent with other published data. In addition, the use of handheld dynamometry in measuring the subjects’ hip strength may have underestimated their true strength. However, we were consistent across groups with our measurement technique and demonstrated good intrarater reliability in our measurements. Finally, while we did attempt to have equal groups for comparison, there were more women subjects in the healthy control group. This was due to a larger number of healthy women in our data pool. Although men usually have greater hip and knee strength than women, we did not include sex in the statistical analyses because the strength data were normalized to body weight. 12
Conclusion
The results of this study indicate decreased quadriceps muscle strength of the uninvolved limb after an ACL injury compared with healthy controls. The exact mechanism of this finding is not completely understood at this time, and future research is warranted to better understand the underlying cause and how quickly this mechanism begins after injury.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Texas Health (approval number CR00001778).