
Abstract
Background:
No consensus exists regarding the anatomic characteristics of the knee anterolateral ligament (ALL). A critical analysis of the dissections described in previous studies allows the division of the ALL into 2 groups with similar characteristics. The presence of considerable variability suggests that the authors may not be referring to the same structure.
Purpose/Hypothesis:
To perform a lateral anatomic dissection, by layers, seeking to characterize the 2 variants described for the ALL on the same knee. We hypothesized that we would identify the 2 variants described for the ALL and that these variants would have distinct characteristics.
Study Design:
Descriptive laboratory study.
Methods:
Thirteen unpaired cadaveric knees were used in this study. The dissection protocol followed the parameters described in previous studies. Immediately below the iliotibial tract, we isolated a structure designated as the superficial ALL, whereas between this structure and the articular capsule, we isolated a structure designated as the deep ALL. The 2 structures were measured for length at full extension and at 90° of flexion and for distance from the tibial insertion relative to the Gerdy tubercle. Potential contact with the lateral meniscus was also evaluated. After measurements were obtained, the 2 dissected structures underwent histologic analysis.
Results:
The superficial ALL presented a posterior and proximal origin to the center of the lateral epicondyle, its length increased on knee extension, and it exhibited no contact with the lateral meniscus. The deep ALL was located in the center of the lateral epicondyle, its length increased on knee flexion, and it presented a meniscal insertion. Both structures had a similar tibial insertion site; however, the insertion site of the deep ALL was located more posteriorly. The analysis of the histological sections for both structures indicated the presence of dense and well-organized collagen fibers.
Conclusion:
This anatomic study clearly identified 2 structures, described as the superficial and deep ALL, which were consistent with previous but conflicting descriptions of the ALL.
Clinical Relevance:
This study clarifies numerous controversies encountered in anatomic studies of the ALL. Knowledge regarding the existence of 2 distinct structures in the anterolateral knee will allow more accurate evaluation of their functions and characteristics.
Although described in 1879 by Segond, 26 the knee anterolateral ligament (ALL) has only recently been recognized as being important. 2,10 Its potential clinical importance is exemplified by patients with possible combined anterior cruciate ligament (ACL) and ALL rupture who continue to have a positive pivot shift after isolated ACL reconstruction. 13,29 Recent biomechanical studies have shown that the function of the ALL involves the restriction of the tibial anterolateral rotation relative to the femur, justifying its importance in pivot-shift control. 20,21,23 Nevertheless, there are a few studies that do not support this importance. 16,25
Although the ALL has been described previously in various anatomic studies, no consensus exists regarding its anatomic parameters. 2,5,10,23 The most prevalent difference among these studies is its femoral origin, with descriptions anterior and distal, 30 in the center, 2,10 and posterior and proximal to the lateral epicondyle. 5,23 Additionally, no consensus has been reached regarding other ALL characteristics, including its length, the presence of a meniscal insertion, and its change in length on flexion and extension, among others. 5,8,11,15,31
The presence of considerable variability among these studies suggests that the authors may not have described the same structure, although these authors have always referenced it as the ALL. An example of this discrepancy is the study by Dodds et al, 5 which described a posterior and proximal origin of the ALL in relation to the lateral epicondyle, the absence of a meniscal insertion, and increased length on knee extension, whereas the study by Helito et al 10 described the ligament as originating from the center of the lateral epicondyle, presenting a meniscal insertion, and its length increasing on knee flexion.
A critical analysis of the dissections reported in published studies allows these studies to be divided into 2 groups: one in which the femoral origin is posterior and proximal to the lateral epicondyle and tends to increase in length on knee extension 4,13 and the other in which the femoral origin is distal to or in the epicondyle center and tends to increase in length on knee flexion. 2,6,7 Many studies described mixed ALL characteristics and included parameters that could accommodate the 2 types of descriptions.
Therefore, the present study aimed to perform a lateral anatomic dissection by layers on the same knee with the intent of characterizing the 2 variants previously described for the ALL and of performing a histological analysis of the structures encountered. We hypothesized that we would identify the 2 variants described for this ligament: the superficial layer located immediately under the iliotibial tract (ITT) and the deep layer located within the anterolateral capsule.
Methods
For this study, 13 unpaired cadaveric knees were used. The dissection was initiated according to the parameters described by Daggett et al. 4 Initially, a circumferential incision was made in the thigh at a distance 15 cm above the joint line and another incision was made in the leg at a distance 15 cm below the joint line. The 2 incisions were connected to remove all skin and subcutaneous tissue. An incision 10-cm proximal to the epicondyle was performed at the ITT, and the ITT was reflected up to its distal insertion into the Gerdy tubercle. After dissection of the ITT, the tendon of the biceps femoris muscle was located at its insertion into the fibular head. This parameter was used to locate the insertion of the fibular collateral ligament (FCL) at the head of the fibula.
The soft tissue around the FCL was removed at its distal aspect for isolation at a distance 20 mm proximal to the head of the fibula, so as not to reach the tissues located above the FCL. After the isolation of the FCL, anterior and posterior capsulotomies were performed to isolate and expose the ALL. Easier dissection was obtained through internal rotation of the tibia in relation to the femur, and this procedure facilitated the identification of a strip-shaped structure with an oblique path over the lateral epicondyle and the FCL toward the region posterior to the Gerdy tubercle. This structure was designated as the superficial ALL (Figure 1). Markers were placed on the anterior and posterior regions of this strip at its femoral origin and tibial insertion. After marker placement, the following measurements were obtained using a digital caliper with an accuracy of 0.01 mm: the length of the anterior and posterior regions of the ligament in full extension and at 90° of flexion, and the distance of the anterior and posterior regions of the tibial insertion of the ligament in relation to the Gerdy tubercle. Contact with the lateral meniscus was also evaluated. Tibial rotation during flexion and extension of the knee was manually controlled.
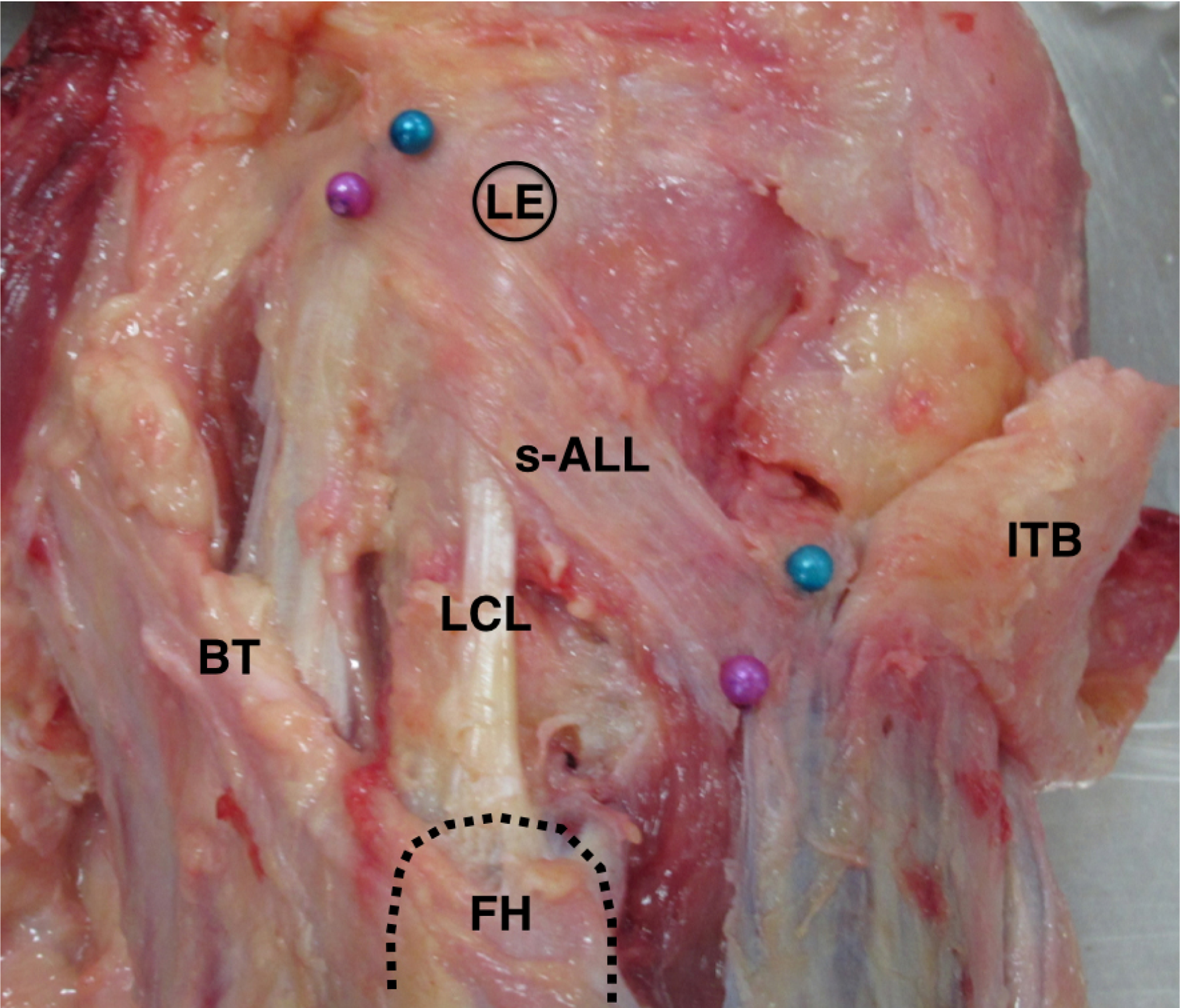
Anatomic dissection of a right knee showing the superficial anterolateral ligament (s-ALL) running from a femoral point posterior and proximal to the lateral epicondyle (LE) toward the anterolateral tibia, passing over the lateral collateral ligament (LCL) origin. BT, biceps tendon; FH, fibular head; ITB, iliotibial band.
After performing these measurements for the superficial layer, the superficial ALL was reflected to expose the structures located in the underlying deep layer. In this layer, we attempted to identify a thickening of the capsule or a ligament-like structure that originated around the center of the lateral epicondyle. Ease of dissection in this layer was obtained through knee flexion and internal rotation of the tibia in contrast to the outer region, which was facilitated by knee extension. We clearly observed another structure immediately adjacent to the outer structure. Its path toward the tibia was very similar to the superficial ALL close to the joint line; however, its origin was located more distal relative to the superficial structure origin, very close to the center of the lateral epicondyle and it presented a vertical orientation on knee flexion. This structure was designated as the deep ALL (Figure 2). The same markings and measurements performed on the outer structure were conducted for the inner structure.
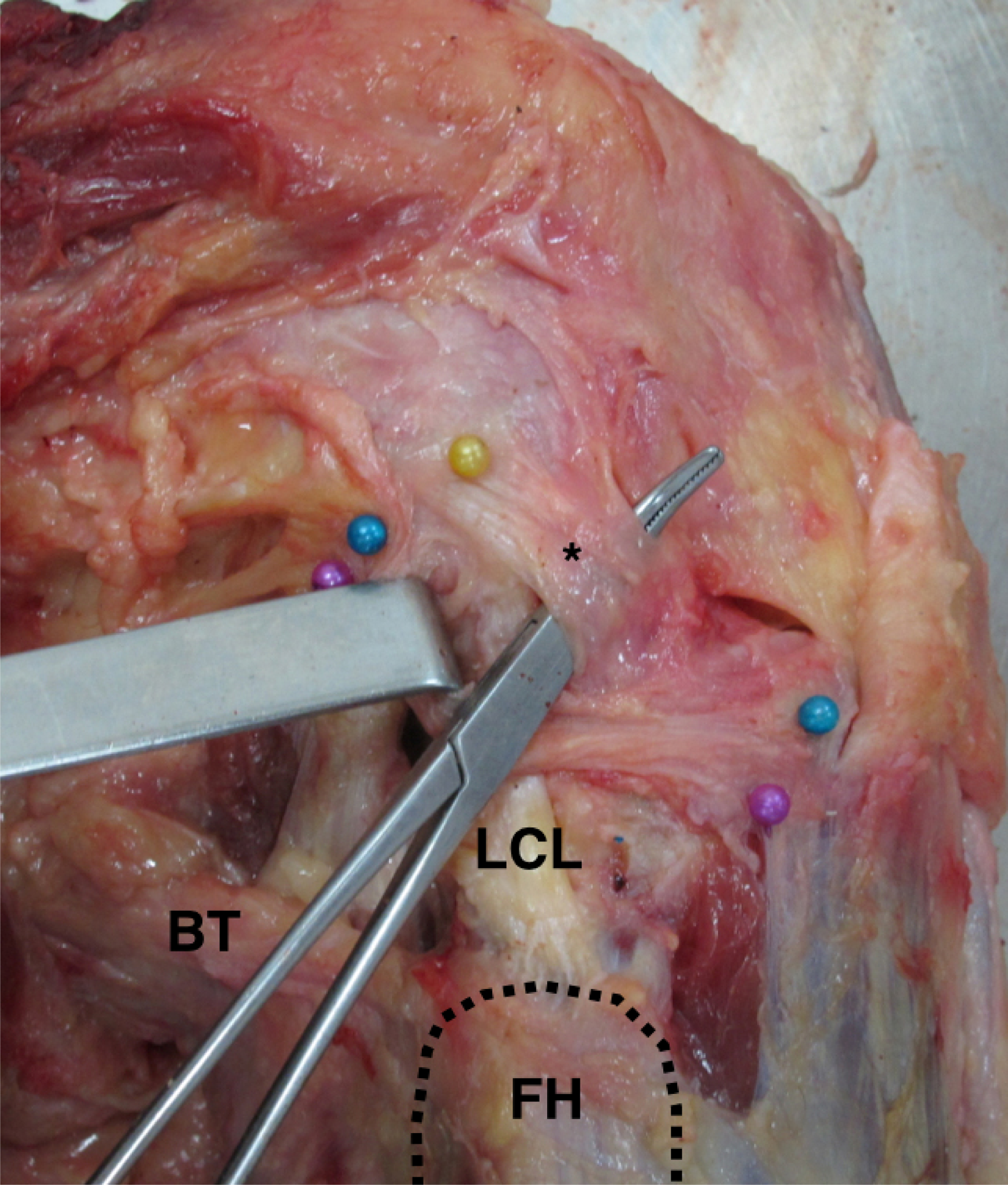
Anatomic dissection of a right knee showing the deep anterolateral ligament (asterisk) below the superficial anterolateral ligament. The yellow marker points the center of the lateral epicondyle. BT, biceps tendon; FH, fibular head; LCL, lateral collateral ligament.
After measurements, the 2 structures dissected were removed en bloc and analyzed by histology. The ligament samples were placed in a 4% formalin solution. After tissue processing, tissue slides with a thickness of up to 4 μm were prepared and stained with hematoxylin and eosin (H&E). The areas of the ligaments were identified and photographed. The number of fibroblasts per mm2 was calculated to compare the 2 structures between each other and with the adult ACL cell count average. 27
The Student t test was used to compare the measurements of the anterior and posterior regions of the superficial and deep ALL on 90° of flexion and full extension to detect changes in the lengths of the ligaments with knee range of motion.
Results
At least 1 band of the ALL was identified in all the dissected knees (Figure 3). The superficial ALL was identified in 12 knees, and the deep ALL was identified in 13 knees. In 1 of the dissected samples in which the superficial ALL was not identified, the deep ALL was identified immediately superficial to the capsule.
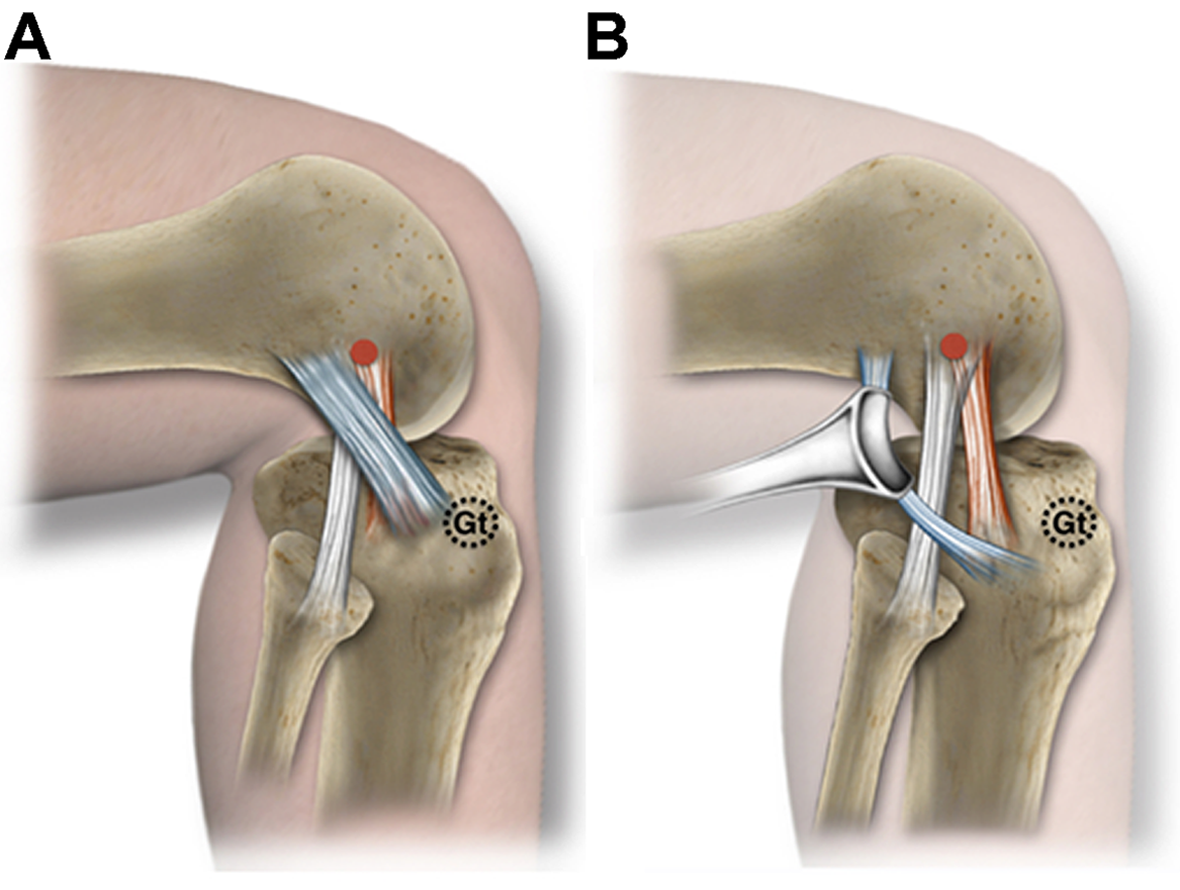
Lateral region of a right knee. (A) The superficial anterolateral ligament (s-ALL) (blue) origin is located posterior and proximal to the lateral epicondyle (LE) (red ball) and it runs superficial to the fibular collateral ligament (FCL) (white) origin toward the tibia. (B) After the removal of the s-ALL, it is possible to visualize the deep ALL (red) origin fibers close to the center of the LE and to the FCL origin. Gt, Gerdy tubercle.
Superficial ALL Findings
The superficial ALL presented its origin posterior and proximal relative to the center of the lateral epicondyle in all cases, passing superficial to the epicondyle and the origin of the FCL toward the tibia. It inserted onto the tibia between the Gerdy tubercle and the head of the fibula with its anterior and posterior regions a mean 10.96 and 16.82 mm from the center of the Gerdy tubercle, respectively (Table 1). The mean length of the superficial ALL was 53.3 mm for its anterior portion and 53.0 mm for its posterior portion on extension. The length of the anterior region was similar to that observed after 90° of flexion of the knee (P = .19), whereas the length of the posterior region decreased by approximately 3 mm on average (P < .001). Visually, this structure appeared tense on knee extension and loose on knee flexion. No direct attachment between this structure and the lateral meniscus was found. It was possible to clearly characterize a distinction between the superficial and deep layers of the ALL. Connecting fibers were observed between these 2 structures, being more frequent near the joint line and their distal insertion.
Anatomic Characteristics of the Superficial and Deep Layers of the ALL a
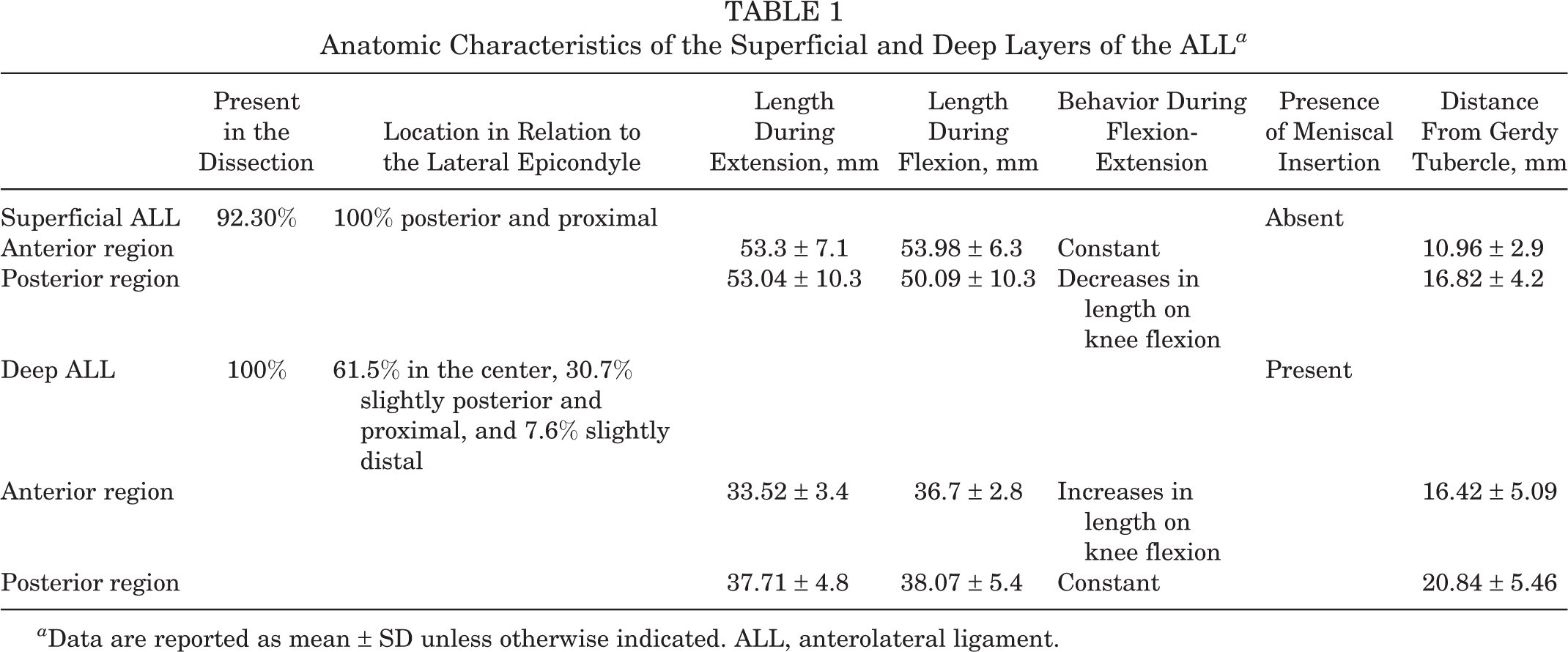
a Data are reported as mean ± SD unless otherwise indicated. ALL, anterolateral ligament.
Deep ALL Findings
The findings regarding the deep ALL included the location of its origin in the center of the lateral epicondyle in most cases (n = 8). In only 1 case, the center of this structure was identified as slightly distal to the center of the lateral epicondyle, while in 4 cases, this structure was presented slightly posterior and proximal to the center of the epicondyle. Its distal insertion was posterior to the Gerdy tubercle, more posteriorly than the insertion of the superficial ALL, with mean values of 16.4 and 20.8 mm for the anterior and posterior regions, respectively. The mean length of the anterior and posterior regions of the deep ALL on extension was 33.5 and 37.7 mm, respectively. With knee flexion, the length of the anterior region increased by approximately 3 mm on average (P < .001), whereas the length of the posterior region remained constant (P = .72). Visually, this deep structure appeared slightly more tense with knee flexion, although these changes were subtle. Before its insertion onto the tibia, some fibers of the deep ALL inserted in the external surface of the lateral meniscus in all cases, between its body and its anterior horn (Figure 4). It was possible to see direct fibers inserting on the lateral meniscus periphery.

Anatomic dissection frontal view of a right knee showing the superficial anterolateral ligament (s-ALL) superficial to the deep anterolateral ligament (d-ALL). The d-ALL clearly inserts (asterisk) on the external surface of the lateral meniscus (LM). LFC, lateral femoral condyle.
Histological analysis of the central part of the superficial and deep layers of the ligament indicated the presence of dense and well-organized collagen fibers (Figure 5). The number of fibroblasts per mm2 was similar in both regions: 301 fibroblasts/mm2 in the outer region and 245 fibroblasts/mm2 in the inner region, slightly lower than the adult ACL. 27
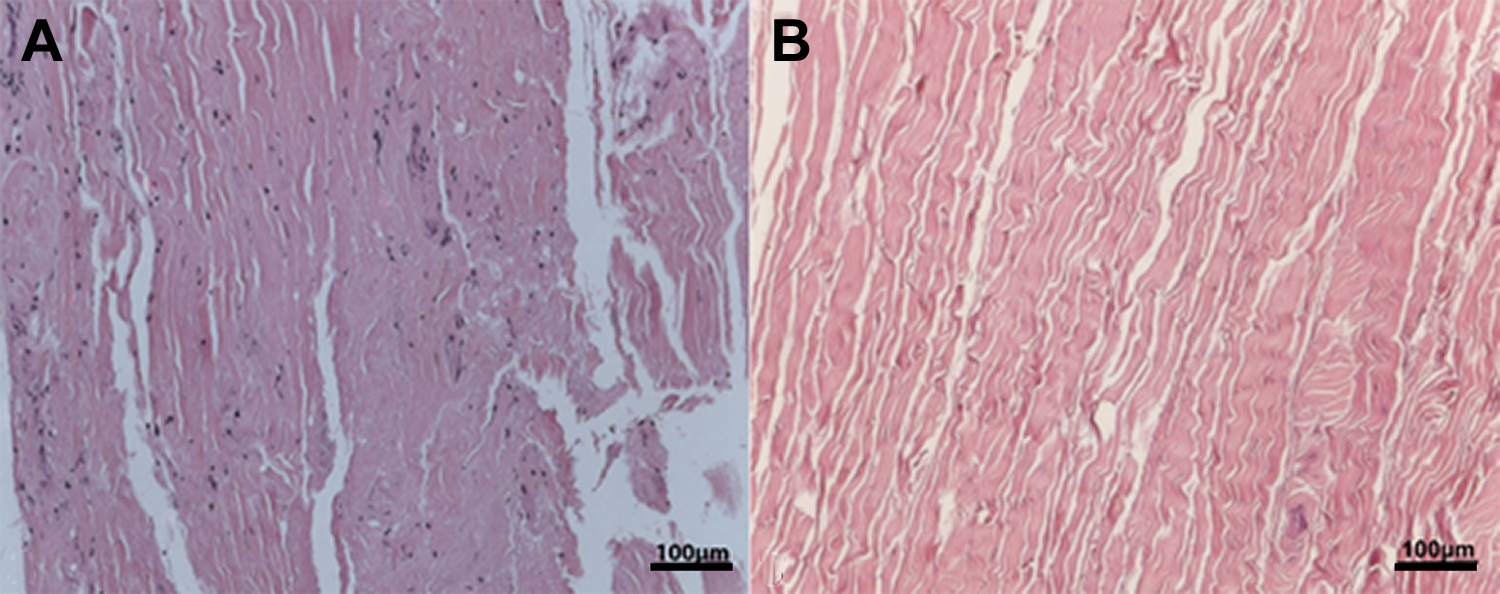
Histological sections of the (A) superficial and (B) deep anterolateral ligament showing well-organized and dense connective tissue. Scale bars = 100 μm.
Discussion
The main finding of this study was the identification of 2 distinct layers of the ALL, superficial and deep, with histological confirmation of the presence of a true ligament in both. The analysis of the anatomic studies that focused on dissection of the ALL allowed the division of these studies into 2 major groups, each of which described 2 anatomically distinct structures, albeit with conflicting yet complementary characteristics: 1 group described ALL structures similar to those of this study and resembling the superficial portion, 4,5,15,18 whereas the other group presented descriptions resembling the deep portion. 2,10
Some anatomic studies described the ALL as having an anterior and distal origin to the lateral epicondyle, 30 with origin on the epicondyle 2,10 and a posterior and proximal origin to the epicondyle, 5,15,18 whereas some anatomic series have described variations in the same group of dissected knees. 1,4,19,24 One possible explanation for the anatomic difference is the difficulty of the dissection, which can be even more difficult if formalin cadavers are used. The probable cause of disagreement between the cited studies lies in the dissection technique, which sought to identify the ALL as only 1 main structure. The dissection protocol used by Daggett et al 3,4 serves as an example of this, which involved dissection in a distal to proximal direction to avoid damage to the ALL fibers located over the FCL, thereby always allowing visualization of the superficial structures. The performance of the dissection in a proximal to distal direction may damage some of the ALL fibers, as was observed in the study by Helito et al, 10 who aimed to expose the lateral epicondyle to identify the ALL, therefore visualizing only deeper structures. In a study focused on identifying radiographic landmarks for ALL reconstruction, Heckmann et al 6 discussed that the femoral point they found was more posterior than the point found by Helito et al 9 in a similar study. They explain these differences may be due to anatomic variability or methodological difference in the way the ALL the origin was identified. We add as a cause that those authors might be commenting on different structures.
The superficial ALL described herein has anatomic points of reference similar to those described in the studies that reported the ALL as having a posterior and proximal origin to the epicondyle. 4,5,15,18 Dodds et al 5 reported no relation with the lateral meniscus for that structure. Considering the major anatomic characteristics observed in these studies, we conclude that they refer to the structure we herein described as the superficial ALL. Although Kennedy et al 15 described a structure that increased in length on knee flexion, these results may have been obtained because of a mixed dissection of the 2 structures. In a biomechanical study, Imbert et al 14 showed that an ALL with a proximal and posterior origin in relation to the lateral epicondyle increases in length with knee extension.
The deep ALL described in this study has anatomic points of reference similar to those found in the anatomic descriptions of Helito et al, 9,10 Claes et al, 2 and Zens et al. 31 We also found a correlation between the deep ALL and the lateral meniscus, as previously detailed by Helito et al. 8 According to the biomechanical studies performed by Helito et al 11 and Zens et al, 31 the ALL increases in length on knee flexion, which suggests tension on flexion. Considering the main characteristics found in these studies, we conclude that these structures refer to the structure herein described as the deep ALL. Also, it is possible to infer that the deep ALL described in this study has an anatomic description similar to the “middle-third of the lateral capsular ligament” described by Hughston et al 12 in 1976 as it “attaches proximally to the lateral epicondyle of the femur and distally at the tibial joint margin.” Claes et al 2 have already stated that the description by Hughston et al 12 was the closest description of an ALL-like structure in the current literature. A summary of the previous anatomic ALL study findings is shown in Table 2.
Summary of Previous Anatomic ALL Study Findings a

a ALL, anterolateral ligament; FCL, fibular collateral ligament; LE, lateral epicondyle; MRI, magnetic resonance imaging.
Among the variants evaluated, we did not identify any variant similar to that described by Vincent et al, 30 who observed that the origin of the ALL was closely associated with the tendon of the popliteal muscle and whose analysis of 1 case indicated that the ALL originated from the popliteal tendon. Vincent et al 30 were the first to conduct a specific study on the anatomy of the ALL, enabling great progress in the study and discussion about this structure. Therefore, we believe that the improvements in the dissection techniques and the increased anatomic knowledge of the ALL have allowed a detailed description of the anatomic parameters over time. Additionally, part of the latter study was performed on patients during arthroplasty procedures, which undoubtedly limited the access to and appropriate exposure of this complex anatomic structure.
The tibial insertion was close between the superficial and deep ALL, although the insertion of the deep portion was located more posterior in relation to the Gerdy tubercle. Considering the limited changes in the characteristics of the ALL with the change in the point of tibial insertion, as reported in the study by Kittl et al, 17 we believe that little attention was directed to small differences in the description of the ALL insertion in the posterior region of the Gerdy tubercle. In contrast to what was observed in the tibial region, small changes in the femoral position relative to the lateral epicondyle may completely alter the characteristics of the ALL during flexion-extension and during knee rotation because of the noncircular shape of the condylar profile.
With regard to the biomechanical function of the anterolateral structures in the control of the rotational stability of the knee, particularly for pivot-shift control, the tensioning of the ALL in or near full extension appears more logical. Sonnery-Cottet et al 28 described a technique involving the fixation of an anatomic reconstruction of the ALL in full extension with excellent results in 2 years. Despite this theoretical improved performance during extension, Parsons et al 22 reported that the tension in the ALL increased starting at 35° of knee flexion, which also suggests a role in flexion. Rasmussen et al 23 also reported the biomechanical importance of the ALL in a cadaveric study and suggested that residual anterolateral instability of the knee may be attributed to the ALL injury. A double-bundle reconstruction procedure, as described in recent studies, may offer stability in extension and flexion, even though they were based in different tibial insertions with the same femoral attachment. 7,28 In this respect, our findings regarding the superficial and deep layers provide the first anatomic and biomechanical bases for discussion. Despite these findings, some studies 16,25 found no significant biomechanical importance for the ALL. However, the anatomic dissections undertaken by these authors were not described in detail.
Although it is possible to anatomically differentiate these structures, both structures showed similar histological characteristics related to the presence of a true ligament, a result that is similar to those of Helito et al 10 and Macchi et al. 19 Therefore, we believe that the ALL should be considered as a functional unit with a role both in extension and flexion, and this dual role should be considered in discussions about its injuries and reconstruction. Caterine et al 1 conducted an anatomic study that found the 2 variations of the ALL origin and suggested that this ligament could be composed of multiple thickenings of the lateral capsule, an inhomogeneous structure in comparison with ACL. Our findings confirmed and expanded this concept. Nowadays, considering the pivot shift control close to knee extension and the clinical results obtained with fixation in full extension, 27 we recommend that surgeons consider reconstruction of the superficial ALL to control the pivot shift.
The limitations of this study include the limited number of anatomic specimens, although other studies were conducted with similar or smaller sample sizes. The previous experience of the authors, with more than 100 dissections, and the consistency of the findings minimize this limitation. Another limitation involves the manual performance of the knee angle measurements, although aided by the use of a goniometer, and the observation of the characteristics of the ligament on flexion and extension in a simplified manner (ie, in neutral rotation, without biomechanical testing conducted with external rotation, internal rotation, and traction).
In summary, we believe that this study clarifies some controversies about the anatomic descriptions of the ALL. We did not discredit any studies but rather reconciled these controversies by describing the superficial and deep ALL, with histological confirmation. Therefore, we should consider these structures as an anterolateral ligament complex of the knee, consisting of the superficial and deep layer of the ALL, the anterolateral capsule, and fibers of the iliotibial tract. Despite representing a major step in the analysis of this well-described structure, the present study neither assigned any differential functional value to these regions nor does it suggest that they should be considered for reconstruction. Therefore, more studies should be conducted to further elucidate the roles of these structures.
Conclusion
This anatomic study clearly identified 2 structures designated as the superficial and deep ALL—findings consistent with previous but conflicting descriptions of the ALL. Additionally, these structures presented distinct characteristics during knee flexion and extension. Histological analysis of both structures indicated the presence of a true ligament.
Footnotes
The authors reported no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Departamento de Ortopedia e Traumatologia, Faculdade de Medicine da Universidade de São Paulo.