
Abstract
Background:
Ulnar collateral ligament reconstruction (UCLR) has become a common procedure performed in overhead-throwing athletes of many athletic levels.
Purpose/Hypothesis:
The purpose of this study was to determine whether clinical outcomes and return-to-sport (RTS) rates differ among patients undergoing UCLR based on graft choice, surgical technique, athletic competition level, handedness, and treatment of the ulnar nerve. We hypothesized that no differences would exist in clinical outcomes or RTS rates between technique, graft choice, or other variables.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients who underwent UCLR from January 1, 2004 through December 31, 2014 at a single institution were identified. Charts were reviewed to determine patient age, sex, date of surgery, sport played, handedness, athletic level, surgical technique, graft type, and complications. Patients were contacted via telephone to obtain the RTS rate, Conway-Jobe score, Timmerman-Andrews score, and Kerlan-Jobe Orthopaedic Clinic (KJOC) Shoulder and Elbow score.
Results:
Eighty-five patients (mean age at surgery, 19.3 ± 4.7 years; 92% male; 78% right hand–dominant) underwent UCLR between 2004 and 2014 and were available for follow-up. Overall, 87% were baseball pitchers, 49.4% were college athletes, and 41.2% were high school athletes. No significant difference existed between the docking and double-docking techniques, graft choice, handedness, sex, activity level, and treatment of the ulnar nerve with regard to clinical outcomes, RTS, or subsequent surgeries (all P > .05). More complications were seen in the docking technique compared with the double-docking technique (P = .036). Hamstring autograft was used more commonly with the docking technique (P = .023) while allograft was used more commonly with the double-docking technique (P = .0006).
Conclusion:
Both the docking and double-docking techniques produce excellent clinical outcomes in patients undergoing UCLR. No difference in outcome scores was seen between surgical technique or graft type. The double-docking technique had fewer complications than the docking technique.
Keywords
Ulnar collateral ligament reconstruction (UCLR), first performed by Dr Frank Jobe in the 1970s and described in the literature in the 1980s, has become a successful procedure for athletes suffering from a symptomatic, deficient ulnar collateral ligament (UCL) who wish to return to overhead activities. 3,4,9,12 Since its original description there have been many modifications to the UCLR technique, including varying graft choices, alternate methods to secure the graft on the ulna and medial epicondyle, and management of the ulnar nerve. 3,6,11,12,15,18 Although many different techniques currently exist, no study to date has compared 2 surgical techniques performed at a single institution, and no study has been able to elucidate how the ulnar nerve should be managed (always transposed vs only transposed if the patient has preoperative symptoms).
Furthermore, the number of graft choices for UCLR has increased and now includes both ipsilateral and contralateral palmaris autograft as well as hamstring autograft, plantaris autograft, a multitude of allografts, and others. 3,17 Studies have shown encouraging results with all of these graft choices, including recent evidence supporting the use of allograft, with return-to-sport (RTS) rates of 88% and patient satisfaction rates of 98%. 3,6,17 However, no study to date has been able to show superiority of 1 graft choice over another with regard to clinical outcome scores or RTS rates. Similarly, there is no current evidence to suggest a player’s handedness has an impact on their outcome or RTS rate. 14 Left-handed pitchers have been considered more valuable as they are in shorter supply than right-handed pitchers; therefore, it is important to understand whether they are able to RTS at the same rate as right-handed pitchers. Similarly, male and female athletes stress their elbow in different ways, so determining whether sex affects RTS rate is important.
Therefore, the purpose of this study was to determine whether clinical outcomes and RTS rates differ based on graft choice or surgical technique (either the docking or double-docking technique). A secondary aim of this study was to determine whether clinical outcomes and RTS rates differed by player handedness, whether the ulnar nerve was transposed, and athletic level of competition.
Methods
After institutional review board approval (IRB approval number: 14051905-IRB01), the surgical database of a single practice was reviewed from January 1, 2004 through December 31, 2014 to locate all patients who underwent UCLR by 1 of 8 sports, shoulder/elbow, or hand fellowship–trained surgeons. The authors have previously reported the aggregate outcomes for this group of patients, but that this study sought to further break out the effect of graft choice, surgical technique, handedness, and other variables. 8 The methods of patient identification and contact were similar between the current study and the previous study. 8
Of the 156 patients (157 elbows) who were identified in the search, 120 patients were more than 18 months out from surgery and met the inclusion criteria for the current study. These patients were then contacted via telephone calls. Patients were asked about their ability or inability to return to sport and their function on return to sport (the same, better, or worse than prior to surgery). The following scores were obtained through questioning: Conway-Jobe score, Timmerman-Andrews score, and Kerlan-Jobe Orthopaedic Clinic (KJOC) Shoulder and Elbow score. We modified the KJOC score for telephone use as previously described. 1,8 We then compared the clinical outcome scores and RTS rates between the 2 surgical techniques, all graft choices, player handedness, preoperative level of competition, and treatment of the ulnar nerve.
The 2 surgical techniques performed on patients in this study were the standard docking and double-docking techniques, both of which have been previously described. 8,16 There were 6 fellowship-trained sports medicine and shoulder and elbow surgeons (4 authors: B.R.B., C.A.B-J., B.J.C., A.A.R.) who performed the standard docking technique in the same manner, and 2 hand fellowship–trained attending physicians who performed the double-docking technique (1 author: M.S.C.). All surgeons are team physicians for a professional baseball team and have experience with UCLR. Briefly, the techniques differ in the method of fixation of the graft on the ulna and medial epicondyle. In the standard docking technique, a tunnel is drilled on the ulna with the assistance of a guide at the level of the sublime tubercle, through which the graft is passed. The graft is then docked into a blind-ended socket in the medial epicondyle and tied over a bone bridge of at least 1 cm. The holes to allow the sutures to exit the medial epicondyle can be created free hand or with the use of a guide. In the double-docking technique a single, isometric blind-ended socket is drilled both on the ulna as well as the medial epicondyle. The tunnel on the ulna is drilled in the center of the sublime tubercle with a 4.5-mm drill bit, and a 0.0625–inch Kirschner wire is placed into the blind-ended socket and used to create 2 divergent holes that leave at least a 1-cm bone bridge on the ulna posterolaterally. Sutures from the prepared graft are passed out these holes using a suture-passing device, and the sutures are tied down under maximal tension. Similarly, a blind-ended socket is created at the UCL footprint of the medial epicondyle, but instead of tying sutures over a bone bridge, a 10-mm cortical button is used to secure the graft. With the forearm supinated and a varus stress placed on the elbow, the sutures are tied down over the button. 8 Furthermore, all surgeons included in this study treated the ulnar nerve in an identical manner. Neither the docking nor the double-docking technique requires the ulnar nerve to be transposed. As such, the nerve was only transposed if the patient had preoperative ulnar nerve symptoms such as shooting pain down the ulnar forearm when pitching, numbness and tingling in the pinky or ulnar half of the ring finger, wasting of the first dorsal interosseous muscle, or a positive tinel/ulnar nerve compression test at the elbow. The ulnar nerve was also transposed if it subluxated on intraoperative examination. Electromyography was not routinely performed as ulnar neuropathy in athletes is largely a dynamic phenomenon. If the nerve needed to be transposed based on these variables, every surgeon performed the transposition in an identical manner: a concomitant anterior, subcutaneous ulnar nerve transposition. If no preoperative ulnar nerve symptoms existed and the nerve was stable on intraoperative examination, the patient did not have a formal transposition. A period of immobilization and rest was followed by gradual range of motion, strengthening, and a graduated return to throwing program in all patients.
The rehabilitation protocol for each surgeon followed the same basic principles and was routinely divided into 4 phases. 20 The time spent in each stage varied and was tailored to the individual athlete. Phase 1 involved rest, with the elbow typically placed in hinged elbow brace or splint and limit full extension for 2 to 4 weeks. Return to throwing activities typically began at approximately 4 months, although some surgeons waited until 5 or 6 months to allow throwing. Throwing from a mound was reserved until a minimum of 6 months since the mean time to return to the same level of sport is greater than 1 year. 9
Statistical Analysis
Descriptive statistics were calculated and reported as mean ± standard deviation for continuous data and frequencies with percentages for categorical data. Association between independent and dependent (outcome) variables was determined using the Student t test, Fisher exact test, linear regression, and analysis of variance (ANOVA) as appropriate for each comparison. P < .05 was used for statistical significance. Multivariate logistical regression analysis was performed for RTS, complications, and subsequent surgery to control for possible confounding factors.
Results
A total of 120 patients with prospectively collected surgical data underwent UCLR between January 1, 2004 and December 31, 2013, were more than 18 months out from surgery, and therefore were eligible for inclusion. Eighty-five (71%) were available via telephone interview at a mean follow-up of 60 ± 30.8 months. The mean age at surgery was 19.3 ± 4.7 years, and mean age at the time of follow-up was 24 ± 5.4 years. Of these patients, 92% were male, 78% were right hand–dominant, and 87% were baseball pitchers. There were 42 collegiate (49.4%), 35 high school (41.1%), 5 recreational (5.9%), and 3 middle school (3.5%) athlete.
Eighty athletes (94.1%) were able to return to the same or higher level of competition. Of baseball pitchers, 92.1% returned to the same or higher level of function. There were no significant differences between RTS rate, subsequent surgeries, Timmerman-Andrews score, or KJOC score between graft type, surgical technique, whether or not the ulnar nerve was transposed, player handedness, or athletic level (Tables 1 -5). There was no association between graft type and preoperative level of athletic competition (Table 6). However, significantly more allografts were used in the double-docking technique (P = .0006) while significantly more hamstring autografts were used in the docking technique (P = .023) (Table 7). More complications were seen after the docking technique than the double-docking technique (P = .036) (Table 2). Five patients in the standard docking group required subsequent ulnar nerve transposition (1 of whom had an ulnar nerve transposition at the index procedure), while no patients in the double-docking group underwent subsequent ulnar nerve transposition. One patient in the double-docking group underwent a subsequent elbow arthroscopy for loss of motion. One patient in the standard docking group had a subsequent ulnar stress fracture that was managed conservatively, and 1 patient in the standard docking group retore his UCL 5 years after a successful RTS but opted not to have it revised. Multivariate logistical regression analysis did not show any different results when controlling for confounding factors. The complication rate in the double-docking technique remained significantly lower than in the standard docking technique (P 2= .0162). Table 8 shows the surgical technique and graft choice by surgeon.
Outcomes Based on Graft Type a

a There were no significant differences between groups. KJOC, Kerlan-Jobe Orthopaedic Clinic; RTS, return to sport.
Outcomes Based on Surgical Technique a

a KJOC, Kerlan-Jobe Orthopaedic Clinic; RTS, return to sport.
b There were significantly more complications with the docking technique than with the double-docking technique (P = .0364). No other significant differences were found between groups.
Outcomes Based on Hand Dominance (Side of UCLR) a

a There were no significant differences between groups. KJOC, Kerlan-Jobe Orthopaedic Clinic; RTS, return to sport; UCLR, ulnar collateral ligament reconstruction.
Outcomes Based on Concomitant Ulnar Nerve Transposition a

a There were no significant differences between groups. KJOC, Kerlan-Jobe Orthopaedic Clinic; RTS, return to sport.
Outcomes Based on Athletic Level a
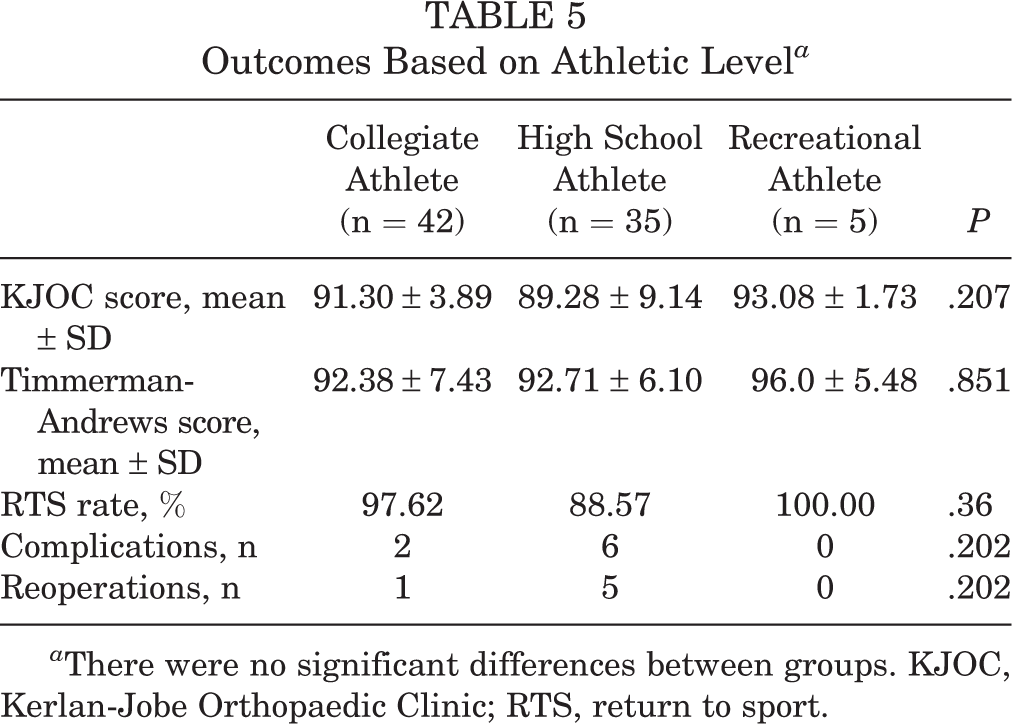
a There were no significant differences between groups. KJOC, Kerlan-Jobe Orthopaedic Clinic; RTS, return to sport.
Graft Choice and Level of Activity a

a Association between level of play and graft the patient received, P = .765.
Graft Choice and Surgical Technique a

a KJOC, Kerlan-Jobe Orthopaedic Clinic; RTS, return to sport.
b Hamstring autograft was more common in the docking technique (32.7% vs 11.1%). c Allograft was more common in the double-docking technique.
Number of UCLRs Performed by Surgeon, With Graft Choice and Technique a
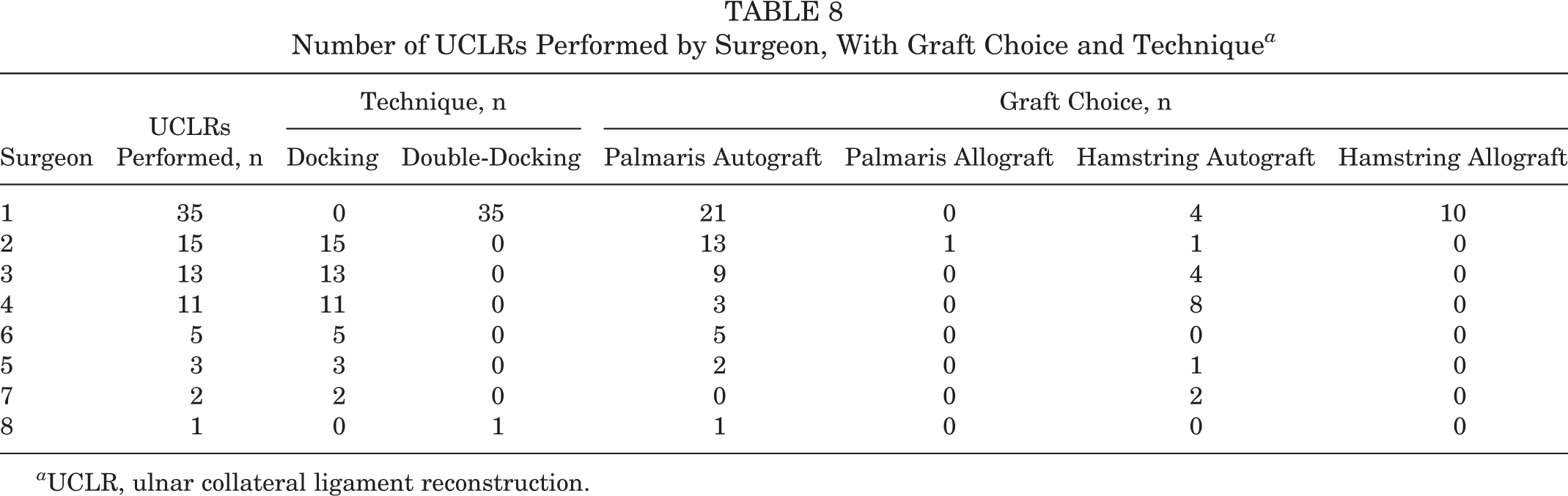
a UCLR, ulnar collateral ligament reconstruction.
Discussion
This study aimed to determine whether clinical outcomes and RTS rates differed between surgical technique, graft choice, and other variables after UCLR. The authors’ hypotheses were partly confirmed in that no significant differences in clinical outcomes or RTS rates were found between the 2 surgical techniques, graft choices, player handedness, management of the ulnar nerve, or preoperative level of competition. However, the complication rate was higher in the standard docking group compared with the double-docking group.
The initial published description of UCLR in 1986 described the use of a “tendon graft” when performing the surgery as well as routine submuscular transposition of the ulnar nerve. 12 As commonly occurs with the first description of any new technique, there were several complications, including a 12.5% rate of postoperative ulnar neurapraxia requiring reoperation and 19% of transient ulnar neurapraxia. 12 Also, the RTS rate to the same or higher level of competition was 62.5%. Modifications to this initial technique have produced RTS rates greater than 85% using the docking and modified docking techniques. 2,8,16,19 However, there are little data comparing various graft choices for UCLR and RTS rates/clinical outcomes. The current study showed that RTS rates and clinical outcomes were not significantly different between graft choices, including allograft, with an overall RTS rate of 94.1%.
With the multitude of graft choices available, the surgeon is at liberty to use many different tendons when performing a UCLR. A recent biomechanical study evaluated the angular valgus deformation at the elbow using grafts of varying thickness (palmaris longus, triceps brachii, extensor carpi radialis longus, and semitendinosus) and found no difference in resistance to valgus moments at the elbow between the various grafts. 5,7,13 Similarly, Cain et al, 3 in a review of 942 patients who underwent UCLR by a single surgeon, found no difference in RTS rates between patients who received a palmaris longus autograft, gracilis autograft, or plantaris autograft. These results were similar to the results of the current study as there was no difference between graft choice and RTS rates/clinical outcomes. This shows that while surgeons and/or patients may have a preference for palmaris autograft, hamstring autograft, or allograft, the clinical results do not differ. Hence, the conversation with patients regarding graft choice should include the pros and cons of each, with the bottom line that the type of graft the patient picks will likely not affect their RTS rate and clinical outcome. Harvest site morbidity is a potential complication of using an autograft, although this was not seen in the current study. This is significant as use of allograft alleviates donor site morbidity, decreases operating room time, and eliminates the variability in autograft quality and size. However, the use of an allograft carries an added monetary cost and a very low risk of disease transmission. 10 The cost-benefit analysis of autograft versus allograft in UCLR has yet to be studied.
Similarly, management of the ulnar nerve has become a topic of question in recent years as some of the accepted techniques routinely transpose the nerve while others only transpose the nerve if the patient is having preoperative ulnar nerve symptoms such as numbness and tingling in the ring and small fingers or if the nerve is unstable intraoperatively. 3,6 A systematic review by Vitale and Ahmad 19 in 2008 found that patients who had their ulnar nerve routinely transposed had a 9% rate of postoperative ulnar neuropathy, with only 75% of good/excellent results compared with those who did not have it routinely transposed, and had a 4% rate of postoperative ulnar neuropathy and 89% good/excellent results. However, this review came out prior to the largest series of UCLR patients by Cain et al 3 and included patients who underwent submuscular ulnar nerve transposition, so the numbers from this review may have changed had this large patient population been included and the submuscular cases been excluded. None of the authors in this study routinely transpose the ulnar nerve but rather perform an anterior subcutaneous transposition only when preoperative ulnar nerve symptoms are present or if the nerve is unstable intraoperatively. Our study found that patients who had their ulnar nerve transposed had no significant difference in clinical outcomes or RTS compared with those who did. Five of 85 patients (6%) in this study required a reoperation for ulnar nerve transposition; all of these patients complained of preoperative numbness and tingling in the pinky and ulnar half of the ring finger, but 1 had additional intrinsic dysfunction of the hand that improved after transposition. Only 1 of these 5 patients underwent an ulnar nerve transposition at the time of their index UCLR. All of these patients who required a subsequent ulnar nerve transposition after their UCLR underwent UCLR with the standard docking approach. It is unclear whether the issues with the ulnar nerve were technique- or indication-related. Furthermore, had all patients undergone obligatory ulnar nerve transposition regardless of preoperative symptoms, it seems there may have been fewer reoperations for subsequent ulnar nerve transposition. However, it is unknown if other complications would have arisen from this.
The complication rates in this study were statistically significantly higher in the docking group compared with the double-docking group. A prior systematic review of varying UCLR surgical techniques found the complication rate to be lowest with the docking technique; however, this review did not include any patients who underwent UCLR with the double-docking technique. 19 Although the complication rate was higher in the docking group, the clinical outcomes and RTS rates did not differ between groups. The lower complication rate in the double-docking group could have been a direct effect of the technique itself compared with the standard docking and its management of the ulnar nerve or a higher surgical volume of the attending who performed the majority of the double-docking UCLRs.
Finally, level of competition, player handedness, and sex did not play a significant role in RTS rates or clinical outcomes. Hence, the true value of these data is that the treating surgeon can clearly articulate to their patient that these factors likely do not play a significant role in their clinical outcome. These data will hopefully allow surgeons to answer many questions patients have prior to undergoing UCLR, alleviating many of the uncertainties patients experience prior to surgery. Further prospective studies comparing all available surgical techniques are necessary to determine whether 1 technique produces superior outcomes.
Limitations
While this study is one of the largest outcome studies of UCLR in the literature, it is not without its limitations. First, there were 6 surgeons who use the docking technique and 1 who uses the double-docking technique. Although all 6 surgeons who utilize the docking technique perform surgery in the same manner, this could introduce bias as some surgeons may be more adept at the operation than others, although all are team physicians for a Major League Baseball team and have significant experience performing UCLR. Unfortunately, only a randomized study between docking and double-docking techniques or between various grafts can truly answer the question of what the ideal technique and graft choice for performing a UCLR is. Also, although the follow-up rate was good at 71%, we were unable to contact 29% of patients, which could introduce selection bias. There was no subset of patients who had their ulnar nerve transposed regardless of preoperative symptoms, so conclusions regarding treatment of the ulnar nerve in this cohort of patients could not be drawn. Patients did not have preoperative clinical scores to compare with postoperative scores, and the surgical data were extracted from the electronic medical record. There were patients who were lost to follow-up, which could have affected the results. Patients were not examined in person, so range of motion, elbow laxity, ulnar nerve examination, radiographs, strength, and other variables was unable to be assessed. The KJOC questionnaire was administered over the telephone, and it is possible that this introduced some recording or recall bias. Furthermore, this questionnaire has not been validated for over-the-telephone use, although the patients seemed comfortable when answering questions. Finally, the rehabilitation protocol for each individual patient was not examined so there could have been slight variability between these protocols, leading to differences in outcomes. A post hoc power analysis was performed that showed a power of 0.296 to detect a difference in RTS based on graft choice. Therefore, the possibility of a type 2 error is present in this study.
Conclusion
Both the docking and double-docking techniques produce excellent clinical outcomes in patients undergoing UCLR. No difference in outcome scores was seen between surgical technique or graft type. The double-docking technique had fewer complications than the docking technique.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.R.B. receives research support from ConMed Linvatec, DJ Orthopaedics, Ossur, Smith & Nephew, and Tornier and receives publishing royalties from SLACK Inc. M.S.C. is a paid consultant for Acumed and Integra and receives royalties from Integra. B.J.C. receives research support from Aesculap/B.Braun, Arthrex, Byroti, Medipost, National Institutes of Health (NIAMS and NICHD), and Zimmer; receives royalties from Arthrex, DJ Orthopaedics, Elsevier Publishing, Saunders/Mosby, and SLACK Inc; has stock/stock options in Carticept and Regentis; is a paid consultant for Regentis; and receives other financial or material support from Athletico, Ossur, Smith & Nephew, and Tornier. A.A.R. receives royalties from Arthrex, Saunders/Mosby, and SLACK Inc; is a paid consultant for Arthrex; receives research support from DJO Surgical, Ossur, and Smith & Nephew; and receives other financial or material support from Arthrex. B.R.B., C.A.B.J., B.J.C., and A.A.R. are team physicians for the Chicago White Sox.