
Abstract
Background:
Rupture of the anterior cruciate ligament (ACL) is a common sports injury and is known to be associated with an increased risk of knee osteoarthritis. Several studies have indicated that the risk of additional injuries to the menisci and articular cartilage increases with delays in the treatment of ACL tears. However, no consensus has been reached regarding the ideal timing for ACL reconstruction in terms of preventing secondary lesions.
Purpose:
To determine how the time elapsed between an ACL lesion and its reconstruction affects the incidence of meniscal and chondral lesions.
Study Design:
Case series; Level of evidence, 4.
Methods:
Medical records of 764 patients who underwent primary ACL reconstruction were reviewed. Data from arthroscopic findings that included information about meniscal lesions and full-thickness articular cartilage lesions at the time of surgery were collected. The association between time elapsed between ACL lesion and reconstruction surgery and incidence of articular cartilage and meniscal lesions was analyzed by chi-square or Fisher exact test. The risk of secondary lesion was calculated by odds ratios (ORs) obtained from simple logistic regression analysis.
Results:
A positive correlation was observed between time after injury and the presence of any articular lesions (P = .003), cartilage lesions (P = .01), and medial meniscus lesions (P < .001). When analyzing the risk of secondary lesion relative to the reference period (<2 months), it was observed that the odds of finding any articular injury at the time of ACL reconstruction increased when the time from ACL injury to surgery was between 12 and 24 months (OR = 2.62) and >24 months (OR = 5.88). Furthermore, the odds of lesions on the medial meniscus increased when the timing between injury and surgery was 6 to 12 months (OR = 2.71) and continued to increase when the timing was 12 to 24 months (OR = 3.78) and >24 months (OR = 9.07).
Conclusion:
Associated articular lesions are more common if ACL reconstruction is delayed by ≥6 months (medial meniscus lesion) and ≥1 year (chondral or any meniscal lesion).
Rupture of the anterior cruciate ligament (ACL) of the knee is a common sports injury. Incidence rate varies from 0.03% in the general population 16 to 7.32% in female athletes. 26 This is a serious knee injury characterized by unsatisfactory function and loss of quality of life in the short term 7 and has shown to be associated with an increased risk of knee osteoarthritis. 14
The optimal management of a torn ACL is yet to be identified. When considering the potential development of knee osteoarthritis (OA), recent data show no clinical differences regarding the development of knee OA between knees surgically reconstructed early or late and those treated with rehabilitation alone. 10 However, when considering potential development of associated injuries, several studies indicate that the risk of additional injuries to the menisci and articular cartilage increases with delay in treatment of the ACL-injured knee. 2,4,5,11,21,25 This is important, since it is well established that the status of the meniscus and articular cartilage is critically important in the development of OA after injury to the ACL. 9,11,19,23 Delayed ACL reconstruction increases the likelihood of a meniscal tear or chondral lesions, suggesting that early ACL reconstruction could reduce or prevent additional chondral and meniscal injury. However, no consensus has been reached with regard to the ideal timing of ACL reconstruction in terms of reducing secondary lesions in ACL-deficient knees. 5,6,11,20
This study aimed to determine how the timing of surgical ACL reconstruction affected the incidence of meniscal and chondral damage. Our hypothesis was that delayed surgical reconstruction is associated with a greater presence of meniscal and articular cartilage lesions in the ACL-deficient knee.
Methods
This was a retrospective case series study. Medical records of patients who underwent primary reconstruction of the ACL between 1984 and 2013 by the same surgeon (W.M.A.) were reviewed. The study procedures took place in the surgeon’s private practice. This retrospective investigation was cleared by our ethics committee.
All records of patients who underwent ACL reconstruction surgery between 1984 and 2013 were included in this review. Patient records were excluded if they indicated any of the following: previous significant ipsilateral knee injuries, such as intra-articular fractures, articular infection, or patellar dislocation; previous knee surgery on the index knee; concomitant posterior cruciate ligament (PCL) and/or posterolateral corner (PLC) injury; multiligamentous lesions; concomitant major fracture; and absence of information required for the study (arthroscopic findings description or time elapsed between lesion and surgery).
The diagnosis of ACL lesion was achieved through standard physical examination and confirmed via arthroscopy. Magnetic resonance imaging (MRI) was also used in more recent cases. All patients were operated on by a single surgeon using the same technique. The arthroscopic findings were recorded on a standardized form (apart from the surgical description record) that included information about the presence or absence (regardless the size) of any full-thickness meniscal lesion (medial or lateral), full-thickness cartilage lesion (lateral femoral condyle, medial femoral condyle, lateral tibial plateau, medial tibial plateau, trochlea, or patella), ACL lesion, and PCL lesion. Lesions occurring in different sites were counted as multiple lesions (eg, if a given patient had a lesion in the medial meniscus, lateral femoral condyle, and medial tibial plateau, 1 meniscal lesion and 2 chondral lesions were reported). Only 1 lesion per site was considered, which means that if there were 2 separated lesions at the medial meniscus it was reported as 1 medial meniscus lesion. Chondral or meniscal lesions were addressed if necessary. ACL reconstruction was performed through a single-incision arthroscopic technique (using a transtibial approach), with a bone-tendon-bone graft harvested from the middle third of the patellar tendon and fixed with interference screws at the tibia and femur. Chart reviews were performed by a single knee surgery fellow who selected all the charts of subjects who fit the inclusion and exclusion criteria. Patient age, sex, date of injury, date of surgery, trauma mechanism, and arthroscopic findings were retrieved from patients’ records. The same person manually entered the data into an electronic spreadsheet. Once the data set was completed, the data were exported to statistical software (PASW Statistics for Windows, version 18.0; IBM Corp). A second independent statistician conducted the statistical analysis.
For the analysis of the sample descriptive variables, multivariate analysis of variance (MANOVA) with 2 factors (time since injury [<2 months, >2-6 months, >6-12 months, >12-24 months, and >24 months] and sex [male/female]) and 2 dependent variables (patient age and number of associated injuries) was used. Data distribution was checked using the Shapiro-Wilk test and homogeneity of variance-covariance matrices using the Box M test. Univariate analyses and post hoc Tukey tests were used as necessary, with P values adjusted for multiple testing to determine significant differences. Descriptive data regarding the association between the time after injury and the appearance of new lesions were presented as frequencies of occurrence (absolute and relative). The association between the time after injury and the occurrence of knee injuries (any related knee injury, medial meniscus, lateral meniscus, chondral injury) was analyzed using the chi-square test or Fisher exact test when appropriate. The chance (risk) of lesion occurrence was determined by odds ratio (OR), calculated by simple logistic regression. The reference period used was of 0 to 2 months after injury. SPSS 18.0 statistical software (IBM Corp) was used for all analyses, adopting a significance level (α) of 5% (P < .05).
Results
Sample characteristics are presented in Table 1. There were 764 records of ACL reconstruction between 1984 and 2013. Of these, there were 40 (5.23%) with previous surgery (2 cases of arthroscopic meniscectomy, 1 tibial osteotomy, and 37 previous ACL reconstructions), 1 (0.13%) with a tibial plateau fracture, 10 (1.30%) with concomitant PCL and/or PLC lesion, 2 (0.26%) with multiligamentous lesions, and 41 (5.36%) records with missing data. After exclusion criteria, 672 records remained for analysis. Of these, 651 (96.87%) patients were male, with a mean age of 28 years. The mean duration of time between injury and surgery was 812 days.
Sample Characteristics a

a P values were obtained with multivariate analysis of variance.
bP < .05 compared with periods <2 months and between 2 and 6 months after injury.
cP = .077 compared with period of >6 to 12 months.
dP < .001 compared with all time periods after injury.
The patient age did not differ regarding time after injury (F = 1.76, P = .136) (Table 1). Thus, the association analysis between the time after injury and the presence of knee injuries was conducted regardless of patient sex and age.
A positive correlation was observed between time after injury and number of related knee injuries (Wilks λ = 0.97, F = 2.95, P = .003), with an increase in secondary lesions in patients undergoing surgery after 24 months compared with those undergoing surgery within 12 months of ACL rupture (F = 4.4, P = .002). Patients who had surgery between 12 and 24 months after rupture also had more lesions when compared with those who had surgery within the first 6 months (P < .05).
In addition, a positive association was observed between injury-to-surgery time and: (1) number of related knee injuries (χ2 = 67.5, P < .001), (2) presence of any knee-related injuries (χ2 = 47.3, P < .001), (3) specific lesions on the medial meniscus (χ2 = 106.9, P < .001), and (4) specific lesions in articular cartilage (χ2 = 13.6, P = .01) (Table 2). There was no significant association with lesions in the lateral meniscus (χ2 = 5.6, P = .230) (Table 2).
Association Between Time After Injury and Knee-Related Injuries to the Medial Meniscus, Lateral Meniscus, and Articular Cartilage a

a Values are expressed as n (%). LM, lateral meniscus; MM, medial meniscus.
b Significant association (chi-square test).
When analyzing the risk of injury relative to the reference period (>2 months), it was observed that the odds of occurrence of any related knee injury increased between 12 and 24 months (OR = 2.62) and >24 months (OR = 5.88) after the initial ACL injury. Furthermore, the odds of having a larger number of related knee injuries increased after 12 and 24 months (Table 3 and Figure 1).
Odds Ratios for the Association Between Number of Lesions and Time After Knee Injury a

a OR, odds ratio.
b Significant association (P < .0125, Fisher exact test), adjusted value for multiple tests.

Odds ratios (±95% CI) for the association of the number of lesions and the time after knee injury. *Significant association (P < .0125, Fisher exact test), adjusted value for multiple tests.
The risk of lesions on the medial meniscus increased at 6 to 12 months (OR = 2.71) and continued to increase at periods between 12 and 24 months (OR = 3.78) and >24 months (OR = 9.07) after ACL injury (Table 4 and Figure 2A). On the other hand, a tendency toward increased odds was observed for articular cartilage injury after 24 months (P = .056) (Table 4 and Figure 2B), and there was no change in the odds for injuries to the lateral meniscus after the first 2 months (P > .05) (Table 4 and Figure 2C).
Odds Ratios for the Association Between Number of Lesions (Meniscal and Chondral) and Time After Injury a

a LM, lateral meniscus; MM, medial meniscus; OR, odds ratio.
b Significant association (P < .0125, Fisher exact test), adjusted value for multiple tests.
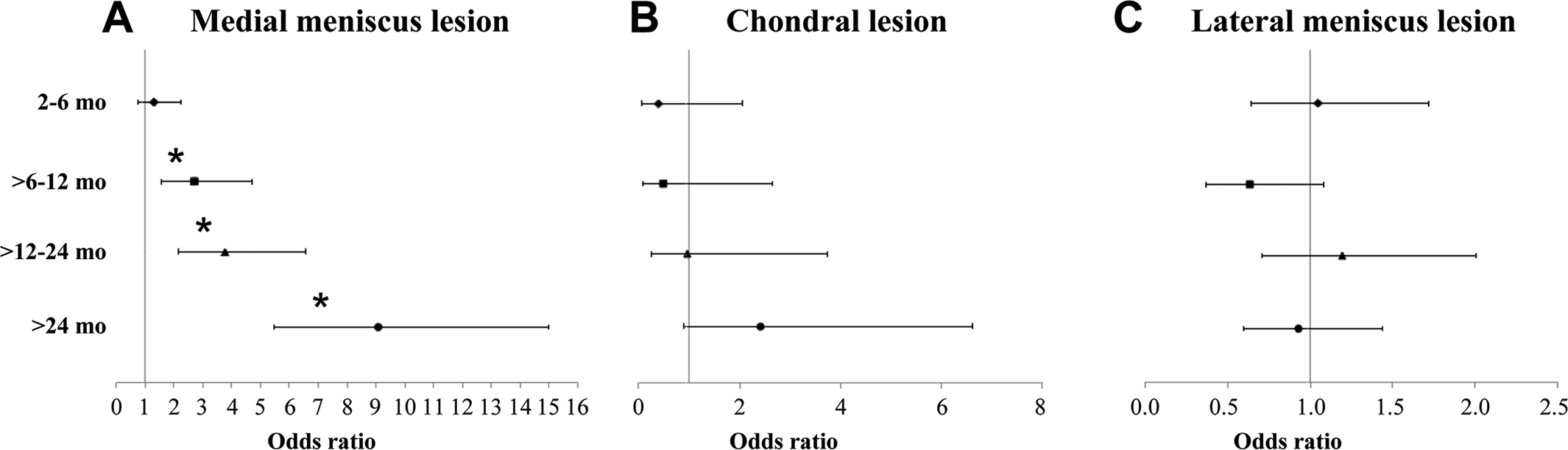
Odds ratios (±95% CI) for the association of meniscus and chondral lesions with time after knee injury. (A) Medial meniscus lesion, (B) chondral lesion, and (C) lateral meniscus lesion. *Significant association (P < .0125, Fisher exact test), adjusted value for multiple tests.
Discussion
Increased time between injury and ACL reconstruction increased the odds of occurrence of other intra-articular lesions of the knee, with greater odds for injury to the medial meniscus after 6 months and to the cartilage after 24 months when compared with the reference period (up to 2 months). To our knowledge, this is the largest case series correlating arthroscopic findings with ACL reconstruction timing. Surgery bias was controlled as all procedures were performed by the same surgeon. Through statistical analysis it was possible to suggest a time point when the occurrence of meniscal and chondral lesions starts to increase.
In 1983, Noyes et al 18 stated that the “dilemma concerning the proper treatment of a knee with a deficient anterior cruciate ligament is largely because of a lack of knowledge of the extent of the functional disability caused by such an injury.” Thirty years later, we still have no answer to what is the optimal treatment of a torn ACL. Apparently the fate of the ACL-deficient knee is sealed at the moment of its injury, regardless of the chosen treatment. 7,14,19 However, it is known that the long-term results of a successful ACL reconstruction, in terms of clinical outcomes and OA development, are affected by the status of the menisci and articular surface. 9,12,15,19,24 In a recent systematic review 19 that included 31 different studies, the highest-rated studies reported low prevalence of knee OA for individuals with isolated ACL injury (0%-13%) and a prevalence of knee OA between 21% and 48% for subjects with combined injuries. Shelbourne and Gray 24 analyzed the long-term follow-up of an impressive number of 1231 patients who underwent ACL reconstruction and found that patients who had more meniscus and articular cartilage damage at the time of surgery had more arthritic changes and subjective symptoms at follow-up. It was stated that “if an ACL reconstruction can be performed successfully before meniscus and articular cartilage damage occurs, the reconstruction may protect the knee from developing symptomatic meniscus tears.” 24 Therefore, one of the goals of treatment for the ACL-deficient knee is to prevent the occurrence of meniscal and chondral lesions.
The ideal timing for an ACL reconstruction remains debatable. The definition of acute varies from days to weeks after injury, and subacute may include the first several months after injury. The classification of chronic or late reconstruction varies from 3 months to more than 1 year. 8 This inconsistency makes it very difficult to compare results of acute and delayed ACL reconstructions reported in the literature. 3 Some studies found a higher prevalence of meniscal tears in patients undergoing reconstruction after 6 months 2,5 or 12 months 4,6 compared with those undergoing early reconstruction. One study 20 concluded that ACL reconstruction within the first 3 months postinjury is an effective way of reducing the risk of secondary meniscal tears.
The present study found a direct relationship between time from injury to ACL reconstruction and prevalence of associated injuries. This is in accordance with Ralles et al, 21 who reviewed 1434 patients who underwent primary ACL reconstruction and found an association between increasing time from injury to ACL reconstruction and increased incidence of secondary lesions. Granan et al 11 evaluated all patients registered in the Norwegian National Knee Ligament Registry and found that the odds of cartilage lesion increased by 1% for each month elapsed from injury date to surgery. According to Brambilla et al, 4 attention must be paid to patients with an elevated body mass index (BMI), as these authors found a close association between BMI and associated lesions. Chhadia et al 5 found a strong association with increasing time to surgery and increased risk of medial meniscus injury. Our analysis found that, when considering each of the menisci separately, only the OR of a medial meniscus lesion increased over time. This is probably due to its function as a restraint to anterior tibial translation in the absence of the ACL, since it has been long demonstrated that the medial meniscus is a restrictor against anterior displacement of the tibia in knees lacking a functioning ACL. 1,13 The recommendation of some authors to only perform ACL reconstruction in young and active patients does not take into account the increasing incidence over time of chondral and medial meniscal tears, which can lead to osteoarthritis. 14
Our study has limitations. First, it is a retrospective study. Second, the size or type of the meniscal tears or the thickness of articular cartilage lesions were not characterized. Third, the sample comprised only 3% women. This could be explained as a cultural issue since Brazilian women are not involved in sports such as soccer or basketball, highly associated with ACL injuries in Brazil. Even if it did not influence the results, the limited data on females prevent us from making any statements regarding sex. Fourth and most important, it was impossible to know whether the observed concomitant lesions occurred previous to the ACL tear, at the time of trauma that led to the ACL tear, or sometime between ACL injury and reconstruction since there was no time-zero MRI. We do not know how many times the knee may have pivoted before and/or after injury. We also do not know the reason for the delay in treatment for each patient or even their activity level during the delay period. However, statistical analysis found a direct relationship between time from injury to ACL reconstruction and prevalence of associated injuries. Thus, one could assume that most concomitant lesions happened after the initial trauma, since subjects who retained an unstable knee for longer periods presented with more meniscal or chondral lesions at the time of surgery. The difference found in the results regarding medial or lateral meniscus lesions is in accordance with this, since medial meniscus overload in the ACL-deficient knee is well established.
Other factors such as proper rehabilitation and level of activity are involved in the natural history of an ACL-deficient knee. 17 Regaining and maintaining full range of motion is also of crucial importance after an ACL injury. 22 Apparently the treatment of an ACL tear must focus on stabilizing the knee as soon as possible, either through surgery or through a rehabilitation program. Although delayed ACL reconstruction increased the likelihood of meniscal and chondral lesions, suggesting that early ACL reconstruction should reduce or prevent additional injuries, high-quality evidence-based data such as randomized controlled trials are needed.
Conclusion
Associated articular lesions are more common if ACL reconstruction is delayed by 6 or more months (medial meniscus lesion) and 1 or more year (chondral or any meniscal lesion).
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.