
Abstract
Background:
Treatment of patellofemoral instability has evolved as our understanding of the relevant pathoanatomy has improved. In light of these developments, current practice patterns and management trends have likely changed to reflect these advancements; however, this has not been evaluated in a formal study.
Purpose:
To determine nationwide patient demographics, surgical trends, and postoperative complications associated with the operative management of patellar instability surgery.
Study Design:
Descriptive epidemiological study.
Methods:
A large private-payer database (PearlDiver) comprising patients covered by Humana and United Healthcare insurance policies was retrospectively reviewed using Current Procedural Terminology (CPT) codes to identify patients who underwent surgery for patellar instability. The study cohort was established by querying for patients billed under CPT codes 27420, 27422, or 27427 while satisfying the diagnostic requirement of patellar instability (International Classification of Diseases–9th Revision codes 718.36, 718.86, or 836.3). Patient demographics, surgical trends, concomitant procedures, and postoperative complications were determined.
Results:
A total of 6190 patients underwent surgical management for patellar instability. Adolescents (age range, 10-19 years) represented 51.5% of cases, and 59.6% were female. The number of patellar instability procedures increased annually over the study period in both the Humana (P = .004, R 2 = 0.76) and United Healthcare (P = .097, R 2 = 0.54) cohorts. The most common concomitant procedures were lateral retinacular release (43.7%), chondroplasty (31.1%), tibial tubercle osteotomy (13.1%), removal of loose bodies (10.5%), osteochondral grafting (9.5%), and microfracture surgery (9.5%). Manipulation under anesthesia was required in 4.6% of patients within 1 year. Patellar fracture within 1 year and infection within 30 days occurred in 2.1% and 1.2% of patients, respectively.
Conclusion:
Patellar instability surgery has increased over the past decade. This finding may be attributed to growing clinical evidence to support these procedures as well as increased surgeon familiarity and comfort with these specific techniques. We observed an unexpectedly high rate of concomitant lateral retinacular release. Overall, the rates of commonly recognized complications (stiffness, patellar fracture, and postoperative infection) were similar to those observed in smaller case series.
Recurrent patellofemoral instability is a condition that predominantly affects young adults, particularly females, in the second and third decades of life. 12 It is now understood that the associated pathophysiology involves disruption of the medial patellofemoral ligament (MPFL), the primary soft tissue stabilizer that provides 50% to 60% of the medial restraining force to lateral dislocation. 10,20 While the rate of recurrence after first-time dislocation is highly variable across studies (13%-40%), patients who have had at least 2 dislocations demonstrate a 50% recurrence rate. 18 These observed rates of redislocation are even higher among patients with confirmed MPFL injury on magnetic resonance imaging (MRI). 6,36 Risk factors for this condition include high-energy trauma at the time of primary injury, insufficient vastus medialis oblique (VMO) strength, positive family history, and preexisting anatomical variation such as ligament laxity, increased quadriceps (Q)-angle, trochlear dysplasia, and patella alta. 1
As a result of recurrent dislocation, patients frequently present with significant comorbid soft tissue and joint damage, particularly involving the articular cartilage of the patella, lateral femoral condyle, and trochlea. 31,45 The prevalence of traumatic cartilage damage after patellar dislocation has been shown to be as high as 40% to 96%. 10,46 Clinically, this may manifest as debilitating anterior knee pain, limitation of activities of daily living, and restricted participation in athletics. In the majority of cases, a course of nonoperative management (activity modification and physical therapy) is initiated. However, due to the prevalence of recurrent, symptomatic dislocation among this relatively young and active patient population, surgical treatment may be necessary to restore joint stability and improve function in cases of recurrent instability. Among these techniques, MPFL reconstruction has evolved over the past few decades, with numerous technical improvements in graft choice, surgical fixation, and graft tensioning, thereby resulting in improved functional outcomes in recent clinical studies. 11,15,23 Given the heightened awareness of comorbid soft tissue/articular cartilage pathology and an improved understanding of anatomic variations and their contributions to instability, additional surgical treatment may include concomitant articular cartilage procedures (eg, chondroplasty, autologous chondrocyte implantation, osteochondral allograft) or bony/soft tissue realignment (eg, lateral retinacular release, tibial tubercle transfer, trochleoplasty). 7,8,13,39,40
Despite the reported clinical success of patellar instability surgery, there are limited data on the current nationwide surgical trends, utilization, and associated complications of these procedures. 38 The purpose of this study was to determine patient demographics, surgical trends including concomitant procedures, and postoperative complications associated with patellar instability surgery using a large national database. We hypothesized that nationwide trends would reveal a steady annual increase in patellar instability surgery performed over the study period. Accordingly, we hypothesized a higher rate of postoperative complications than previously reported in smaller case series with wider adoption of the procedure.
Methods
A retrospective review of the PearlDiver Patient Record Database (www.pearldiverinc.com) was conducted for patients undergoing patellar instability surgery. This commercially available database consists of approximately 20 million patients with orthopaedic diagnoses compiled from 2 large private insurance providers based in the United States: United Healthcare and Humana. Clinical diagnoses can be queried by using patient billing codes, including those classified by International Classification of Diseases–9th Revision (ICD-9) and Current Procedural Terminology (CPT). 3,48,50
To ensure appropriate study inclusion, a cohort of patients undergoing patellar instability surgery was determined by searching for relevant billing codes (CPT codes 27420, 27422, and 27427) while satisfying the diagnostic requirement for patellar instability (ICD-9 718.36, 718.86, or 836.3). Data were available from 2007 to 2011 for the United Healthcare database and from 2007 to 2014 for the Humana database. The demographic data for each record included the patient’s age, sex, and year of procedure. For age distributions, patients were categorized into groups aged 10 to 19 years (adolescents), 20 to 34 years (young adults), and ≥35 years (adults) based on the known demographics of patellar instability. A linear regression model was used to determine the R 2 coefficient and associated P value to ascertain the trends for the annual number of procedures across the study period. Statistical significance was set at the P < .05 threshold.
To determine the incidence of concomitant procedures, the aforementioned cohort was queried to identify patients who underwent a secondary procedure on the same day and billing record as the primary patellar instability procedure. The incidence of commonly recognized postoperative complications was also determined by querying the database for secondary procedures performed for the following: (1) infection requiring surgical treatment within 30 days of the index procedure, (2) loss of motion requiring manipulation under anesthesia within 1 year of the index procedure, and (3) patellar fracture within 1 year of the primary procedure (Table 1).
CPT Codes for Primary Patellar Instability Surgery, Associated Concomitant Procedures, and Postoperative Complications a

a CPT, Current Procedural Terminology.
Results
A total of 6190 patients who underwent patellar instability surgery were identified during the aforementioned time period (Table 2). Of these, 1067 patients were identified in the Humana database from 2007 to 2014 and 5123 were identified in the United Healthcare database from 2007 to 2011. Females comprised 59.6% of the total cohort. Overall, 51.5% of cases were adolescents (age range, 10-19 years) and 33.0% were young adults (age range, 20-34 years). The sex and age distributions were comparable between Humana and United Healthcare cohorts. In the Humana cohort, we observed an annual increase in the number of patellar instability procedures performed over the study period from 2007 to 2014 (P = .004, R 2 = 0.76). We also observed an overall increase in annual case volume over the study period in the United Healthcare cohort; however, this trend was not statistically significant (P = .097, R 2 = 0.54).
Patient Characteristics a
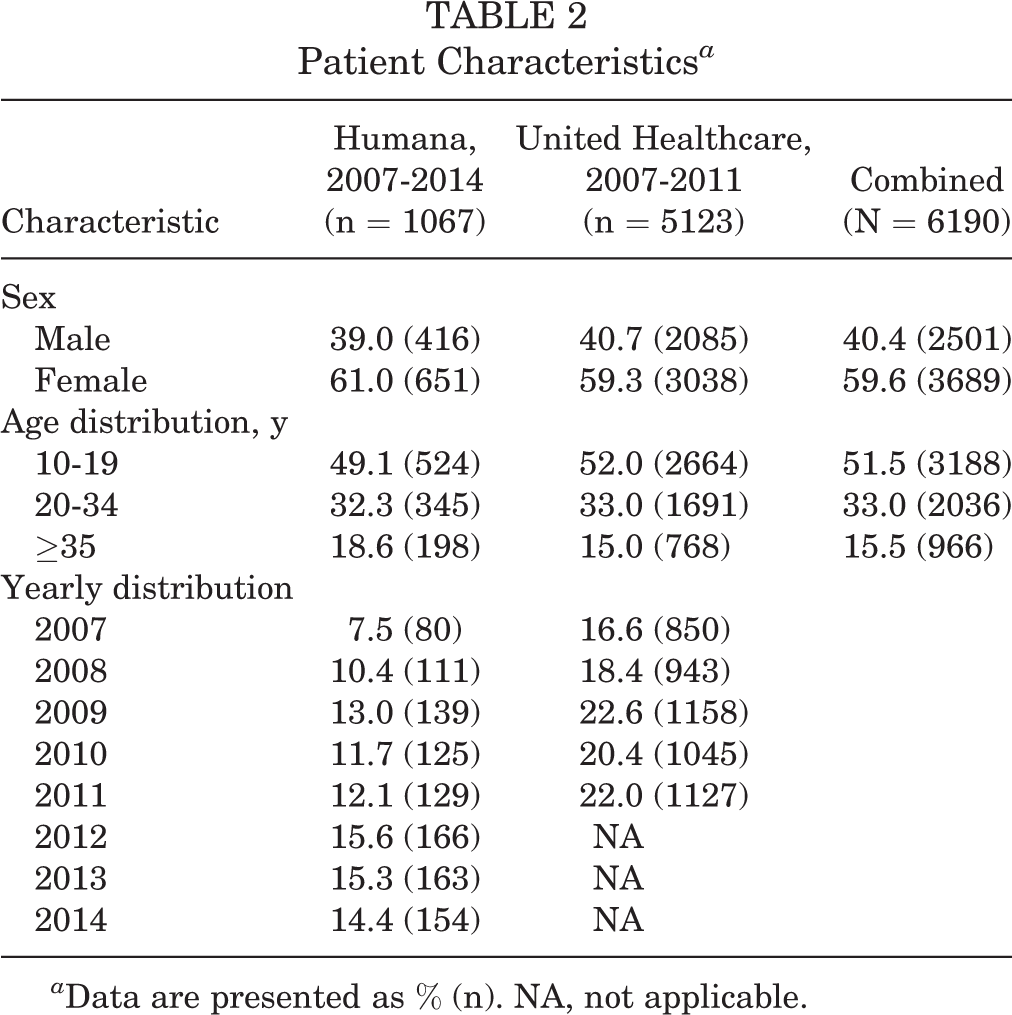
a Data are presented as % (n). NA, not applicable.
The database was queried for a series of CPT codes corresponding to concomitant procedures and postoperative complications requiring surgical management. The most common concomitant procedures were lateral retinacular release (43.7%), chondroplasty (31.1%), tibial tubercle osteotomy (13.1%), removal of chondral fragments/loose bodies (10.5%), chondroplasty (9.5%), and microfracture surgery (9.5%) (Table 3). With regard to complications, loss of knee motion requiring manipulation under anesthesia (MUA) occurred in 4.6% of patients within 1 year of the primary patellar stabilization procedure. Patellar fracture occurred in 2.1% of the cohort within 1 year of the index procedure, and infection requiring reoperation occurred in 1.2% of the cohort (Table 4). The incidence of concomitant procedures and complications was comparable between the Humana and United Healthcare cohorts.
Concomitant Procedures Associated With Patellar Instability Surgery a

a Data are presented as % (n).
Postoperative Complications Associated With Patellar Instability Surgery a

a Data are presented as % (n).
Discussion
As our understanding of the pathoanatomy associated with patellofemoral instability has improved and surgical techniques have evolved, patellar stabilization surgery, and MPFL reconstruction in particular, has emerged as a popular treatment option for patients with recurrent instability. Several clinical studies have demonstrated reliable success with reduced rates of patellar instability and objective improvements in knee function. 11,23,32 Current data on management trends and complications have been limited to small case series. 33,34,43 There is a paucity of data regarding the nationwide practice patterns and surgical trends associated with these procedures in the United States. Utilizing a national population-based analysis, we observed a statistically significant increase (P = .004, R 2 = 0.76) in the number of patients who underwent surgical management of patellar instability in the Humana registry from 2007 to 2014. This observation may reflect increased surgeon comfort and familiarity with relevant techniques as well as broader acceptance and adoption of commonly accepted procedures as more scientific evidence has become available to support the reliable success of patellar stabilization, specifically MPFL reconstruction.
The demographics in this large nationwide cohort were generally consistent with those reported in smaller case series. The observed age distribution confirms that patellofemoral instability commonly affects patients in their adolescent and young adult years, defined as ages 10 to 19 and 20 to 34 years, respectively, in this study. 17,47 In general, the female predominance of this condition is explained by established anatomic variations, particularly an increased Q-angle and femoral anteversion relative to males. 25,28 However, some authors have noted that sex is not a significant risk factor for patellar dislocation, and that in the case of acute, traumatic patellar dislocation, males actually have a greater incidence of injury. 21,47
Recurrent patellar dislocation is associated with an increased prevalence of patella alta, increased tibial tubercle to trochlear groove (TT-TG) distance, rotational deformity, and trochlear dysplasia. 42 Certainly, multiple factors contribute to the overall risk of patellar dislocation, and the presence of various anatomic factors must be addressed at the time of surgery to ensure a successful outcome. Using the PearlDiver database, we were able to determine the most common concomitant procedures that were performed at the time of patellar stabilization. We observed an unexpectedly high rate of lateral retinacular release (43.7%) in our patient cohort. While this technique has largely fallen out of favor as an isolated procedure for the treatment of recurrent dislocation due to unacceptably high failure rates, many studies have reported its concomitant use with stabilization procedures such as MPFL reconstruction. 4,19,37 Though the lateral retinaculum is an important secondary stabilizer of the patellofemoral joint, 16,26 the efficacy of combined MPFL reconstruction and lateral release is controversial, with some studies showing no significant difference in success rates and others showing reduced lateral stability with in vivo and biomechanical models. 9,27,44 Despite the aforementioned data, our analysis demonstrates that lateral release is frequently performed as an adjunct procedure in patients who undergo patellar stabilization. Tibial tubercle osteotomy, which can be performed to optimize patellar alignment and correct patellar height, was performed in 13.1% of patients. While the precise incidence of this procedure has not been studied to our knowledge, it is a reliable treatment option in skeletally mature patients with patella alta or an increased TT-TG distance. 2,18 Though no epidemiological studies have investigated the precise incidence of increased TT-TG distance in patients with patellofemoral instability, some authors have reported that a TT-TG distance >20 mm can be observed in 20% to 50% of patients undergoing patellofemoral stabilization procedures. In context, the findings of our study suggest that tibial tubercle osteotomy may be underperformed by practicing surgeons. 23,30 However, some recent studies have suggested that an elevated TT-TG distance (>20 mm) may not be an absolute indication for tibial tubercle medialization with MPFL reconstruction. 24 Certainly, additional procedures to correct osseous abnormalities such as trochleoplasty and rotational osteotomies are effectively performed outside the United States; however, further studies are necessary to determine their precise role and clinical efficacy. 22,29 Finally, the overall rate of procedures related to cartilage pathology was high in our patient cohort. The incidence of concomitant chondroplasty (31.1%) and chondral fragment/loose body removal (10.2%) confirms the relatively high frequency of cartilage damage observed at the time of surgical intervention in other case series. 10,13 However, we acknowledge that this number may be an underestimate, as chondroplasty may not be billed as a separate CPT code in all cases due to procedure bundling. Osteochondral grafting (9.5%) and microfracture surgery (9.5%) were performed in a large number of patients, thereby demonstrating the emergence of cartilage repair/restoration techniques as a well-accepted treatment option in patients with moderate to high-grade traumatic cartilage lesions resulting from dislocation. 13,14,39
Recent studies suggest that a high complication rate is associated with patellar stabilization surgery. A meta-analysis by Shah et al 38 demonstrated that there is an overall complication rate of 26.1% in patients undergoing MPFL reconstruction. Another review by Parikh et al 33 found an overall postoperative complication rate of 16.2% among young adults. In these analyses and other case reports/series, a large proportion of complications involve recurrent instability, which can be attributed to a combination of several factors, including failure of graft fixation or poor tunnel placement, poor graft integration, and unrecognized anatomic risk factors for recurrent instability. The overall rate of failure due to recurrent instability has been studied and is estimated to occur in 5% to 28% of patients. 5,7,8,18,33,41 Unfortunately, because of the inability to specifically identify laterality using the PearlDiver database (ie, discern ipsilateral revision surgery from contralateral primary failure), this study was unable to reliably determine the rate of graft failure after reconstruction. Despite this limitation, we were able to determine the rate of other common complications on a large nationwide scale. The observed rate of MUA for knee arthrofibrosis ranges from 3.5% to 4.5% after surgical stabilization. 33,38 We found that loss of motion requiring MUA occurred at a comparable rate of 4.6% within 1 year of surgery. Shah et al 38 noted that postoperative patellar fracture is a rare but severe complication that occurred in 0.6% of their combined cohort. Parikh et al 33 found a slightly higher fracture rate of 3.3% among 179 patients. Our study found that patellar fracture occurred in 2.1% of the 6190 cases that were performed across the United States. While some studies have observed increased rates of postoperative patellar fracture after the use of bone tunnels for graft fixation, there has been a trend toward techniques that avoid utilization of tunnels. 15,35 Finally, our analysis also found that postoperative infections requiring surgical intervention are a rare (1.2%) complication after patellar instability surgery, which is consistent with previous studies. 33,38,49
The primary advantage of a large database study is that it allows for analysis of nationwide trends across multiple centers and providers rather than providers at a single institution or region. It also avoids sampling bias by exclusively evaluating cases performed at academic or high-volume sports medicine centers. This is critical in studying a topic with as much variability as patellar instability. Furthermore, by analyzing such a large cohort, this study confers a population size and level of statistical power not otherwise achievable through conventional chart review. Despite these strengths, this study has several limitations that should be noted. First, the patient data obtained from the database are less comprehensive than those available through formal chart review. Accordingly, we were unable to determine the precise cause of postoperative complications. Given the inability to precisely determine laterality or indications for billed procedures, we were unable to determine rates of recurrent instability and removal of hardware. Next, because the database is analyzed by a formal query of CPT and ICD-9 codes, there is the possibility of error from inaccurate coding. Furthermore, the CPT codes used in this study reference historical procedures that are seldom performed today (Hauser, Campbell, Roux-Goldthwait, Maquet) because there are no specific codes for modern patellar stabilization procedures (eg, MPFL reconstruction). In the present study, we utilized the 3 most commonly accepted CPT codes within the Humana and United Healthcare databases and attempted to eliminate any errors in patient inclusion by cross-referencing the soft tissue procedures with the ICD-9 codes that are specific for patellar instability/dislocation. Because of this, we advocate that CPT codes be reevaluated and potentially updated to reflect the procedural terminology used in modern practice. We similarly acknowledge that procedural bundling/unbundling can significantly affect the incidence of secondary procedures, which may or may not be separately coded by individual practitioners in a way that is difficult to discern (eg, CPT-27422 potentially includes lateral retinacular release, CPT-27420 potentially includes tibial tubercle transfer). Overall, it is most likely that bundling would generally lead to underestimation of concomitant procedure rates. Finally, there is no access to clinical outcome data by which to analyze treatment decisions reflected in the PearlDiver database.
Conclusion
Patellar instability surgery has evolved over the past few decades. Using a national insurance database, we found an annual rise in the rate of surgical procedures performed across the United States. We observed an unexpectedly high rate of lateral release and noted a large percentage of patients underwent cartilage repair/restoration surgery. The most commonly recognized complications (knee stiffness, patellar fracture, and infection) occur at a relatively low frequency, which is consistent with data from smaller case series. Overall, these data may prove useful for counseling patients on the risks of complications after patellar instability surgery, as these procedures have become more widely adopted and utilized within the United States.
Footnotes
Presented as a poster at the American Academy of Orthopaedic Surgeons 2015 Annual Meeting, Las Vegas, Nevada, March 2015, and as part of the International Guided Poster Tour in Sports Medicine on March 26, 2015.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C.W. has stock/stock options in PearlDriver Inc.
Acknowledgment
The authors thank Mr Anthony D’Oro and Dr Zorica Buser for their assistance in developing the PearlDiver database query.