
Abstract
Background:
We previously developed a novel technique using an alternate soaking process that improves tendon-bone healing by hybridizing the tendon graft with calcium phosphate (CaP). However, the effects of the CaP-hybridized tendon graft on anatomic single-bundle anterior cruciate ligament (ACL) reconstruction remain unclear.
Purpose:
To determine the effects of CaP-hybridized tendon grafts compared with untreated tendon grafts 6 months after anatomic single-bundle ACL reconstruction using a goat model.
Study Design:
Controlled laboratory study.
Methods:
Animals were divided into a CaP group (n = 5 goats) and a control group (n = 5 goats), and we analyzed (1) knee kinematics and in situ forces under applied anterior tibial loads of 50 N and internal tibial torque of 2.0 N·m in the grafts at full extension and at 60° and 90° of knee flexion, (2) the mean percentage of bone tunnel enlargement using computed tomography (CT), and (3) the histology of the tendon-bone interface.
Results:
The in situ forces under applied anterior tibial loads of 50 N at 60° and 90° of knee flexion in the CaP group were greater than those in the control group (P < .05). The red safranin-O–stained area, indicating glycosaminoglycans in the cartilage layers at the joint aperture sites of the anterior femoral and posterior tibial bone tunnel, was greater in the CaP group than that in the control group (P < .05). The lengths of the nonbonding gap area between the anterior femoral and posterior tibial bone tunnels in the control group were greater than those in the CaP group (P < .05). No significant difference could be detected in the mean percentage of bone tunnel enlargement between the 2 groups.
Conclusion:
The CaP-hybridized tendon graft enhanced tendon-bone healing at the joint aperture site in both anterior femoral and posterior tibial tunnels 6 months after anatomic single-bundle ACL reconstruction in goats. The in situ forces under applied anterior tibial loads at greater flexion angles in the CaP group increased compared with controls.
Clinical Relevance:
Anatomic single-bundle ACL reconstruction using CaP-hybridized tendon grafts may lead to better postoperative knee function.
Keywords
Tendon-bone healing is one of the most important factors for a successful anterior cruciate ligament (ACL) reconstruction using a soft tissue graft. 11,24 In a previous study, we developed a novel technique that improves tendon-bone healing by hybridizing calcium phosphate (CaP) to the tendon grafts using an alternate soaking process. 29 With this technique, areas of scarless direct bonding between the CaP-hybridized tendon graft and the bone were observed 2 to 3 weeks after implantation of the tendon into bone in rabbits, likely because the bonelike microstructure contains low-crystalline apatite and type I collagen. 20,21 After nonanatomic single-bundle ACL reconstruction in a goat model, better anterior stability and greater in situ forces were observed in the CaP-hybridized tendon graft when an anterior tibial load of 50 N was applied using a robotic universal force/moment sensor (UFS) system 1 year after surgery. 19 Moreover, in the CaP group, the percentage of bone tunnel enlargement was smaller than that in the control group, and a more direct insertion-like formation with the cartilaginous layer at the interface at the joint aperture site was found when compared with that in the control group 2 years after surgery. 18 Furthermore, in a clinical trial, the CaP-hybridized tendon grafts improved anterior knee stability and Lysholm scores at 2-year follow-up, and a reduced percentage of bone tunnel enlargement in both tunnels was noted at 1-year follow-up compared with the untreated tendon grafts when applied during nonanatomic single-bundle ACL reconstructions using a transtibial tunnel approach. 16 However, anatomic single-bundle ACL reconstructions show better biomechanical function and clinical results than nonanatomic single-bundle ACL reconstructions. 13,23,28 The effects of CaP-hybridized tendon grafts on the biomechanical function and tendon-bone interface after anatomic single-bundle ACL knee reconstructions has not yet been reported.
We hypothesized that the biomechanical function after anatomic single-bundle ACL reconstruction using the CaP-hybridized tendon graft will be better than those achieved using untreated tendon grafts 6 months after surgery because of enhanced tendon-bone healing. The objectives of this study were to determine the effects of the CaP-hybridized tendon grafts on the repair site by analyzing (1) the knee kinematics and in situ forces on the grafted tendon, (2) bone tunnel enlargement using computed tomography (CT), and (3) the histology of the interface between the tendon graft and bone compared with the results of untreated tendon grafts 6 months after anatomic single-bundle ACL reconstruction in a goat model.
Methods
Surgical Procedure
Fifteen skeletally mature female Saanen breed goats (weight, 40-60 kg) were used in the present study (CaP group, n = 5; control group, n = 5; intact ACL, n = 5). We used the intact ACL data as the reference values for biomechanical analysis. All animal experiments and breeding were performed according to the conditions approved by the ethics committees of the University of Tsukuba. All activities were implemented in accordance with the National Institutes of Health Guidelines for the Care and Use of Laboratory Animals and the ARRIVE (Animal Research: Reporting of In Vivo Experiments) guidelines.
The surgical technique used was the same as that described in our previous studies except for the placement of both bone tunnels. 19,22 The right knee joint was opened and the ACL completely resected. Gross anterior subluxation of the tibia was confirmed by manual examination. In our previous study, we drilled from the anteromedial surface of the proximal tibia to the tibial insertion of the ACL and through the lateral femoral cortex consecutively using a transtibial tunnel approach. 18,19,22 Therefore, the femoral tunnel placement was at the high noon position and shallow. In this study, we used independent drilling techniques to perform anatomic single-bundle ACL reconstruction more precisely. We drilled using a 2.4-mm-diameter Kirschner wire from the center of the femoral insertion of the ACL to the lateral cortex of the distal femur, and the femoral bone tunnel was reamed using a 7.0-mm-diameter cannulated drill. Next, we drilled using a 2.4-mm-diameter Kirschner wire from the center of the tibial insertion of the ACL to the medial cortex of the proximal tibia using the patellar groove as a guide to ensure a similar tibial tunnel angle. This tibial bone tunnel was then reamed using a 7.0-mm-diameter cannulated drill. The length of the tibial tunnel was at least 15 mm.
The flexor digitorum longus (FDL) tendon (total length, 16 cm) was harvested for use as the graft tendon in the right knee. The tendon was cut into 2 sections and folded to quadruple. A 4-stranded tendon length of 40 mm with a diameter of 7.0 mm was prepared. An Endobutton (10 mm) was attached to the proximal end of the grafts, and No. 2 nonabsorbable sutures were placed using the Krackow technique 10 in the distal ends of the graft.
For the CaP hybridization method, the intra-articular portion of each graft was covered with the sleeve of a rubber glove and tied on each side using No. 2 nonabsorbable sutures to prevent soaking during CaP hybridization.
16,18,19,22
Next, the grafts were soaked in 100 mL of a Ca solution (100 mmol/L CaCl2; 30 mmol/L
After hybridization or saline soaking, the grafts were passed through the femoral and tibial tunnels (Figure 1). The graft was secured on the femoral side with the Endobutton. The graft was then tensioned with a manually applied maximal force and fixed on the tibial side by tying the sutures around a 4.5-mm cortical screw. We irrigated the wound with 500 mL of a saline solution and sutured the capsule and skin. After surgery, all animals underwent intravenous prophylactic antibiotic therapy consisting of 1 g cefazolin every 12 hours for 3 days.
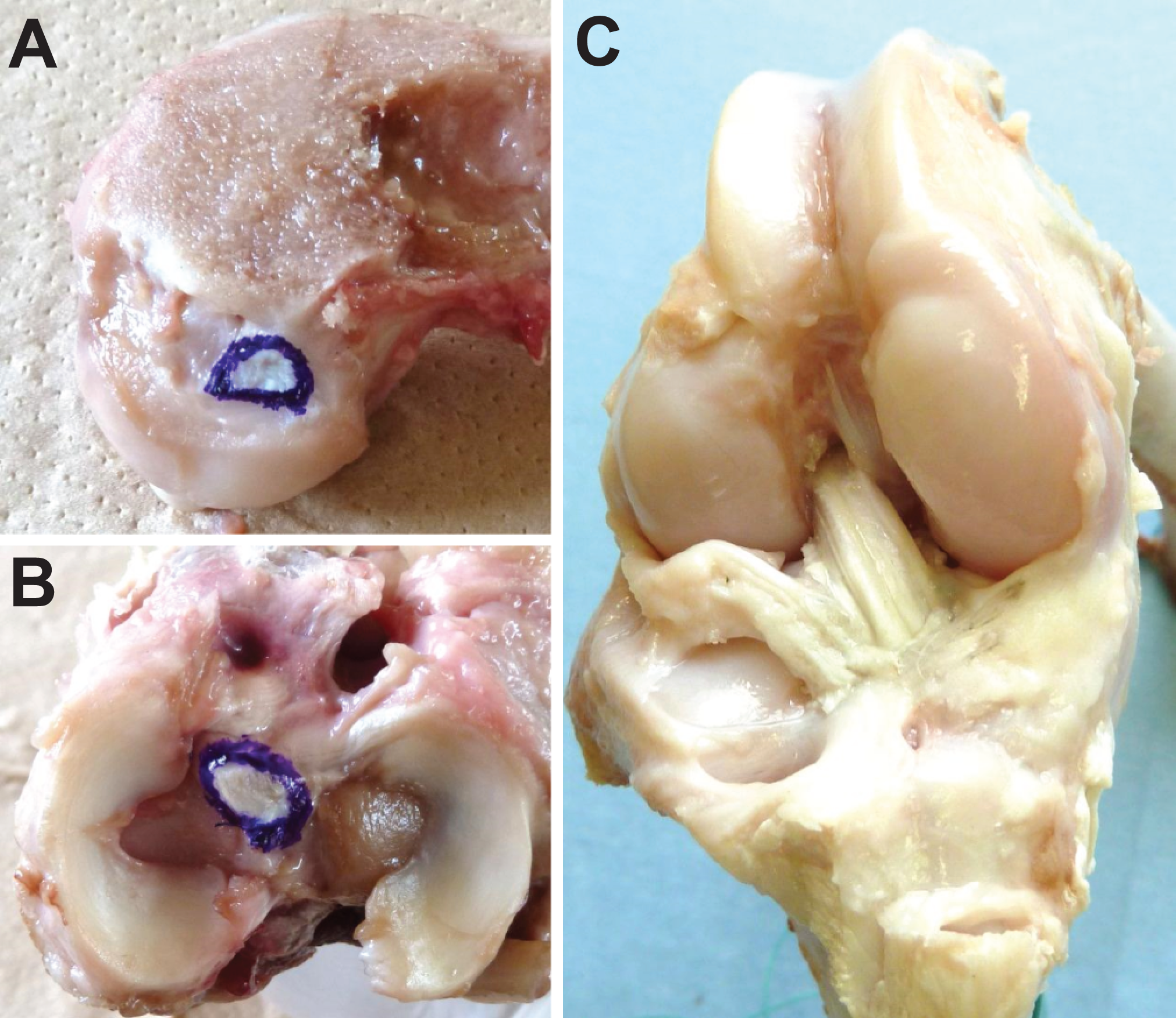
Anterior cruciate ligament (ACL) reconstruction in a goat model. (A) The blue circle indicates the femoral attachment of the ACL. (B) The blue circle indicates the tibial attachment of ACL. (C) ACL graft replacement.
Postoperatively, all goats were allowed free activity in a 50-m2 cage. The goats were sacrificed 26 weeks after surgery. Clinically, 6 months after ACL reconstruction is a generally important time for returning to light sporting activities including cutting and jumping before returning to sports. 12 A total of 5 specimens were analyzed from each of the CaP and control groups. The other 5 specimens were nonoperated intact knees (intact ACL group). The 15 knee specimens were harvested, sealed in double plastic bags, and immediately stored at −20°C until use for biomechanical analysis. 19
Biomechanical Analysis
We performed the biomechanical analysis using the same testing methods in our previous study. 19 The robotic testing system (FRS2010; Technology Service) consisted of a 6–degrees of freedom (DOF) manipulator, servomotor controllers, and a control computer. The femoral clamp was fixed to the lower mechanism and the tibial clamp was fixed to the upper mechanism via a UFS (SI-660-60; ATI). The hardware and software performances are described in our previous work. 6 The robotic system was capable of controlling the displacement and force/moment applied to the knee in all 6 DOF based on a mathematical description of knee kinematics and kinetics. 3,5 Thus, this testing system permits the measurement of multiple degrees of freedom knee kinematics and the in situ forces in the ACL replacement graft while the knee is subjected to externally applied loads. 13,14,26
Before the biomechanical analysis, each specimen was thawed for 24 hours at room temperature. The tibia and femur were cut 20 cm from the joint line, and the surrounding skin and muscles were removed. First, 1 specimen was secured to the testing system using the locations of the femoral insertion sites of the medial and lateral collateral ligaments as positioning points. To identify the neutral position of the knee, the path of passive flexion-extension of the joint from full extension to 90° of knee flexion was first determined by the robotic UFS testing system in force-control mode. The starting points for the application of external loads were determined throughout the range of flexion at the position where all of the external forces and moments in the joint were minimized. After determining the path of passive flexion-extension of the knee, the robotic UFS testing system was used in force-control mode to determine the 5-DOF knee kinematics in response to a 50-N anterior-posterior (A-P) tibial load and a 2.0-N·m internal-external tibial torque at full extension and fixed knee flexion angles of 60° and 90°. 19 However, we could not analyze the internal tibial rotation at 90° of knee flexion for all specimens because the rotation angle at 90° was so large that the arms of the robot interfered with each other. The 3-dimensional path of knee motion was recorded for 5 cycles, and the 6-DOF forces/moments on the knee recorded during the fifth cycle were considered to represent the original knee motion. The ACL or ACL graft was then transected via an arthrotomy, and the testing system reproduced the identical 3-dimensional path of knee motion as before transection while again measuring the 6-DOF forces/moments on the knee during the fifth cycle. The in situ forces in the ACL or ACL graft during the flexion-extension, A-P drawer tests, and internal tibial rotation tests were calculated using the difference in force/moment during the fifth cycle data between the intact and transected knee states using the principle of superposition. 4 A single engineer who was blinded to the identifications of the specimens performed the evaluations.
Computed Tomographic Analysis
After biomechanical analysis, the 10 frozen goat specimens from the CaP group and the control group were scanned using CT (Brilliance CT 64; Philips) to assess the femoral and tibial bone tunnels. A CT (voltage, 120 kV; current, 230 mA) scan with the knee in full extension was taken, and the images were analyzed by a single radiologist. A single standard protocol was used consistently throughout the study. The initial volume acquisition was with 0.9-mm slices from 30 mm above the femoral tunnel to 30 mm below the tibial tunnel. Three-dimensional images were reconstructed using the Virtual Place Lexus workstation (AZE Ltd). Axial images of the femoral and tibial bone tunnels were obtained from the reconstructed 3-dimensional images. We measured the tunnel cross-sectional areas (CSAs) of the femur and tibia at the joint aperture site using the axial images. The increase in tunnel CSA was calculated as: CSA increase (%) = (CSA at 6 months − initial CSA) × 100/initial CSA. 18,22 The initial CSA was defined as the diameter of the reamer. A single radiologist who was blinded to the identifications of the specimens performed the evaluations.
Histological Analysis
After CT imaging, the specimens in the CaP and control groups were prepared for histology. First, the femur–ACL graft and ACL graft–tibia complex were harvested. The specimens were then fixed in 10% neutral-buffered formalin for 1 week, decalcified using 10% ethylenediaminetetraacetic acid (EDTA) for 8 weeks, and embedded in paraffin. The specimens were cut along the center of the bone tunnel in the sagittal plane and sliced to 5 µm thick. Hematoxylin and eosin (H-E) and safranin-O staining were performed to identify the cartilage layer in the tendon-bone interface using light microscopy. The histology of the tendon-bone interface (fibrous tissue such as Sharpey fiber–like tissue, the cartilaginous interface, and the nonbonding gap area at the joint aperture site) and of the intra-articular portion of the grafted tendon was compared between the CaP and control groups. At the joint aperture site in the anterior and posterior interfaces in both the femur and tibia, the area of red safranin-O–stained glycosaminoglycans (GAG) in the cartilage layer and the length of the nonbonding gap area from the joint were measured using Mac Scope software (Mitani). 18,19 The ligament tissue maturation index (LTMI) described by Murray et al 15 was used to evaluate the maturation of the tendon grafts according to the following 3 criteria: (1) cellular aspects including cell density, nuclear shape, and orientation; (2) extracellular matrix characteristics, including crimp; and (3) vascular features including blood vessel density and maturity (total score, 28 points). A single veterinarian who was blinded to the identifications of the specimens performed the evaluations.
Statistical Analysis
The obtained biomechanical data, CT analysis, and histological analyses were compared using Student t tests. P < .05 was considered statistically significant.
Results
Biomechanical Analysis
All of the ACL grafted tendons were intact at 26 weeks. The mean full extension angles of the knees were 16.0° ± 4.2° (CaP), 20.8° ± 7.7° (control), and 21.0° ± 6.0° (intact ACL). The biomechanical data for the groups (CaP, n = 5; control, n = 5; intact ACL, n = 5) in response to a 50-N applied anterior tibial load and a 2.0-N·m applied internal tibial torque are shown in Tables 1 and 2.
Biomechanical Data in Response to a 50-N Anterior Tibial Load for the Intact ACL, CaP, and Control Groups at 6 Months a
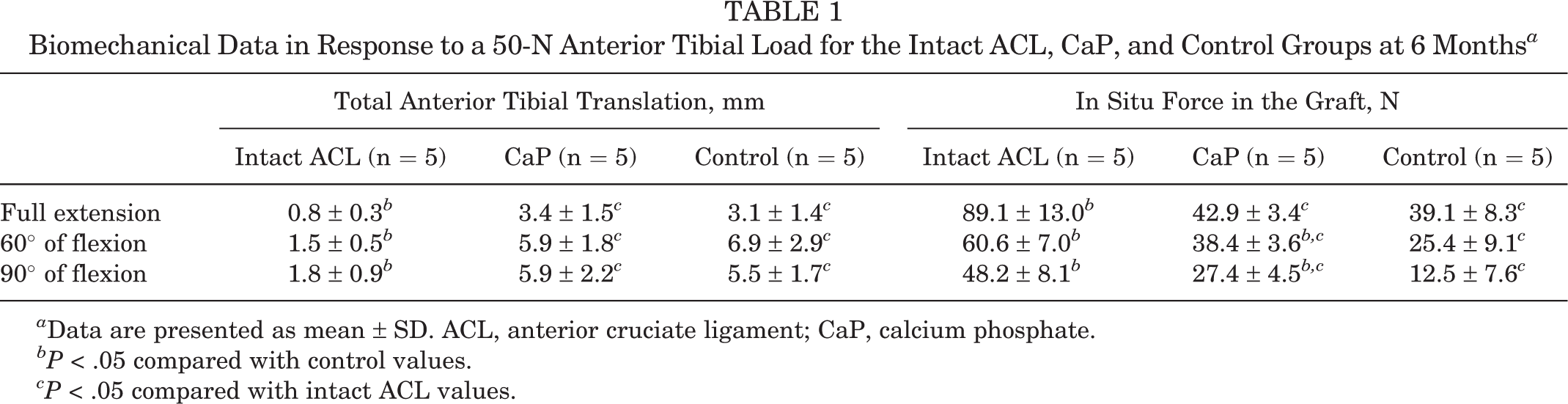
a Data are presented as mean ± SD. ACL, anterior cruciate ligament; CaP, calcium phosphate.
bP < .05 compared with control values.
cP < .05 compared with intact ACL values.
Biomechanical Data in Response to a 2.0-N·m Internal Tibial Torque for the Intact ACL, CaP, and Control Groups at 6 Months a
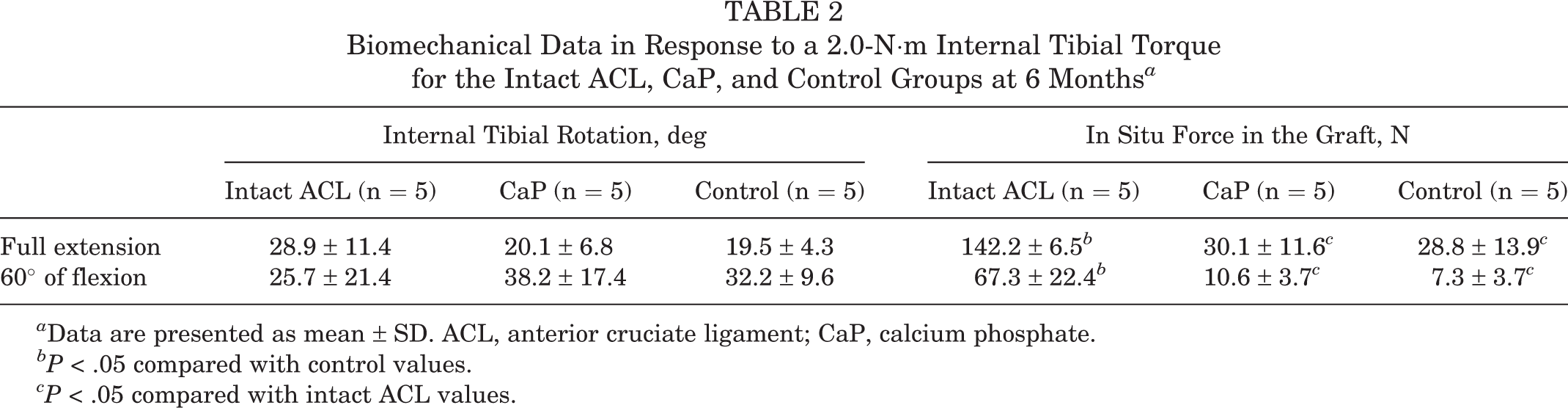
a Data are presented as mean ± SD. ACL, anterior cruciate ligament; CaP, calcium phosphate.
bP < .05 compared with control values.
cP < .05 compared with intact ACL values.
The in situ forces under applied anterior tibial loads in the CaP group were greater than those in the control group at 60° (P = .009) and 90° (P = .003) of knee flexion but not significantly different than that at full extension (P = .189). The in situ forces in the intact ACL group were significantly greater than those in the other groups at full extension (P < .001 vs CaP; P < .001 vs control) and at 60° (P < .001 vs CaP; P < .001 vs control) and 90° (P < .001 vs CaP; P = .003 vs control) of knee flexion. There were no significant differences in the anterior translations at full extension (P = .396) or at 60° (P = .268) or 90° (P = .391) of knee flexion between the CaP and control groups. The anterior translations in the intact ACL group were significantly smaller than those in the other groups at full extension (P = .003 vs CaP; P = .003 vs control) and at 60° (P < .001 vs CaP; P = .002 vs control) and 90° (P = .003 vs CaP; P < .001 vs control) of knee flexion.
The in situ forces under applied internal tibial torque were not significantly different at full extension (P = .438) or at 60° of knee flexion (P = .096) between the CaP and control groups. The in situ forces in the intact ACL group were significantly greater than those in the other groups at full extension (P < .001 vs CaP; P < .001 vs control) and at 60° of knee flexion (P < .001 vs CaP; P < .001 vs control). There were no significant differences in the internal tibial rotation angles at full extension or at 60° of knee flexion between any of the groups (CaP vs control, P = .427 and P = .260; CaP vs intact ACL, P = .089 and P = .170; intact ACL vs control, P = .062 and P = .275).
Computed Tomographic Analysis
The mean percentage of bone tunnel enlargement in the femoral bone tunnel CSA was 51.3% ± 20.9% in the control and 27.9% ± 34.5% in the CaP groups (P = .115). The tunnel enlargement of the tibial bone tunnel CSA was −2.8% ± 22.7% in the control and 2.9% ± 20.4% in the CaP groups (P = .343). No significant difference could be detected in the mean percentage of bone tunnel enlargement between the groups.
Histological Analysis
The results of histological analysis for the CaP (n = 5) and control (n = 5) groups are shown in Tables 3 and 4. The areas of GAG stained red by safranin-O in the cartilage layers were greater in the CaP group at the anterior surface of the femoral bone tunnel at the joint aperture site (P = .009) and at the posterior surface of the tibial bone tunnel at the joint aperture site (P = .031) than those of the control group. In the CaP group, areas of GAG stained red by safranin-O in the cartilage layers between the grafted tendon and bone at the aperture sites were observed in all 5 specimens on the anterior surface of the femoral bone tunnel, in 3 of 5 specimens on the posterior surface of the femoral bone tunnel, in 4 of 5 specimens on the anterior surface of the tibial bone tunnel, and in all 5 specimens on the posterior surface of the tibial bone tunnel. In the control group, however, areas of GAG staining at the aperture sites were observed in 2 of 5 specimens on the anterior surface of the femoral bone tunnel, in 3 of 5 specimens on the posterior surface of the femoral bone tunnel, in 4 of 5 specimens on the anterior surface of the tibial bone tunnel, and in 4 of 5 specimens on the posterior surface of the tibial bone tunnel (Figure 2). In the other specimens, Sharpey fiber–like tissue, which is fibrous tissue between the grafted tendon and bone, was observed. Long Sharpey fibers were observed at the anterior bone tunnel; short and dense fibers were observed at the posterior bone tunnel.
GAG Area by Safranin-O Staining in Cartilage Layers at Interface a

a Data are presented as mean ± SD. CaP, calcium phosphate; GAG, glycosaminoglycan.
bP < .05 compared with control values.
Length of the Nonbonding Gap Area From the Joint a

a Data are presented as mean ± SD. CaP, calcium phosphate.
bP < .05 compared with control values.

Histological sections stained with safranin-O from the calcium phosphate (CaP) group at the anterior bone tunnel of the joint aperture site in the femur. The right side of the images is distal and the left side is proximal. (A) Low-magnification image (40×); (B) higher magnification image (100×) of the square area in (A); and (C) higher magnification image (400×) of the square area in (B). A cartilage layer stained red indicating glycosaminoglycans was observed between the grafted tendon and bone. b, bone; c, cartilage tissue; t, tendon graft.
The lengths of the nonbonding gap area from the joint in the control group were greater than those in the CaP group at the anterior surface of the femoral bone tunnel (P = .011) and the posterior surface of the tibial bone tunnel (P = .047). In the CaP group, nonbonding gap areas at the aperture sites of the femoral bone tunnel were observed on the anterior surface in 4 of 5 specimens and on the posterior surface in 1 of 5 specimens and of the tibial bone tunnel on the anterior surfaces in 0 of 5 specimens and on the posterior surface in 1 of 5 specimens. In the control group, however, nonbonding areas at the aperture sites of the femoral bone tunnel were observed on the anterior surface in all 5 specimens and on the posterior surface in 3 of 5 specimens and of the tibial bone tunnel on the anterior surface in 0 of 5 specimens and on the posterior surface in 4 of 5 specimens (Figure 3).

Histological sections stained with safranin-O from the control group at the anterior bone tunnel of the joint aperture site in the femur. The right side of the images is distal and the left side is proximal. (A) Low-magnification image (40×) and higher magnification (400×) images of the (B) right and (C) left square areas in (A). Fibrous connective tissue (Sharpey fiber–like tissue) was observed at the tendon-bone interface, as well as a gap area at the joint aperture site. No cartilage layer indicated by red glycosaminoglycan staining was observed at the tendon-bone interface. b, bone; f, fibrous tissue; t, tendon graft.
The maturation of the tendon grafts was similar in the CaP and control groups 6 months after surgery. The LTMI scores were 22.8 ± 3.1 for the CaP group and 20.8 ± 2.0 for the control group, with no significant difference between groups (P = .265).
Discussion
The CaP-hybridized tendon graft enhanced tendon-bone healing at the joint aperture site 6 months after anatomic single-bundle ACL reconstruction in goats. The areas of GAG stained red by safranin-O in the cartilage layers of the CaP group on the anterior surface of the femoral bone tunnel at the joint aperture site and the posterior surface of the tibial bone tunnel at the joint aperture site were greater than those of the controls. The cartilage layer in the CaP group was more distinct than that in the control group. Tensile stress and/or compressive stress at the interface could have promoted the formation of cartilage tissue after being directly bonded with the bone tunnel in the CaP group. 17,19,31 On the other hand, fibrous tissue (Sharpey-like fibers) and nonbonding gap areas at the interface in the control group could have been formed by shear stress between the grafted tendon and the bone associated with the bungee 7 and windshield wiper effects. The anterior femoral and posterior tibial sides may experience more graft tunnel motion than other areas. The CaP-hybridized tendon graft directly bonded with the bone likely because the bonelike microstructure contains low-crystalline apatite and type I collagen of tendon graft, 20,21 suggesting that the interface can better resist the shear stress. The ACL insertion consists of 4 distinguishable transition tissue layers: the ligaments, fibrocartilage, mineralized fibrocartilage, and bone. 1,2 The cartilage layers function as shock absorbers by reducing the gradient of stiffness between the ligament and bone. 9,27 We believe that the structure of the cartilaginous insertion is necessary for a functional ACL reconstruction because the cartilaginous insertion layers can compensate for the varied elastic moduli of the grafted tendon and bone. 1,2 However, the improvement of the tendon-bone healing in the CaP group was observed at only 1 time point (6 months) in this study. Therefore, longer follow-up is needed to clarify the long-term effects of CaP-hybridized tendon graft after anatomic single-bundle ACL reconstruction. Although the improved tendon-bone healing in the CaP group did not result in the maturation of the tendon graft, the firm fixation of the grafts prepared using the CaP-hybridization method may promote the maturation and recovery of the mechanical strength of the midsubstance of the graft by more effectively transferring the forces to the ligament. To show this, however, immunohistochemical and microstructural analyses at longer follow-up are needed.
The differences of the mean percentage of bone tunnel enlargement between both groups were not significant. Using a nonanatomic ACL reconstruction goat model, the percentage of bone tunnel enlargement in the CaP group was smaller than that in the control group. 18 A nonanatomic single-bundle ACL reconstruction showed greater tunnel enlargements than an anatomic single-bundle ACL reconstruction. 30 Graft-tunnel motion leads to bone tunnel enlargement at the joint aperture site for grafts fixed by suspensory fixation. 25 The graft-tunnel motion in the anatomic ACL reconstruction may be smaller than that in the nonanatomic ACL reconstruction in goats because of tunnel placement. A comparison with the bone tunnel at time 0 may be necessary to evaluate bone tunnel enlargement exactly. Moreover, a longer follow-up is needed to investigate the bone tunnel enlargement in the CaP group.
The in situ forces under an applied anterior tibial load at 60° and 90° of knee flexion in the CaP group were greater than those in the control group 6 months after anatomic single-bundle ACL reconstruction in goats. However, the in situ force at full extension under applied anterior tibial load and internal tibial torque in the CaP group was not significantly different than that in the control group. Clinical studies in humans have shown that anatomic graft placement improves knee laxity (anterior tibial translation with the Lachman examination, anterior load, and pivot shift) and is closer to the native ACL when compared with nonanatomic graft placement. 23 We believe that the improved graft mechanics with anatomic placement may lessen the effect of rapid bone-tendon healing on in situ forces near full extension.
Although the appearance of the grafted tendons in the CaP and control groups was similar, the CaP-hybridized tendon showed better tendon-bone healing in the cartilage layer and smaller nonbonding gap areas at the joint aperture sites of the anterior femoral and posterior tibial bone tunnels compared with that of the control group. Therefore, the attachment area with cartilage between the CaP-hybridized tendon graft and the bone may be larger than that in the control grafts near the joint. The CaP-hybridized tendon can enhance better fixation at the joint aperture sites than the untreated tendon. The length of the grafted tendon midsubstance portion from the femoral fixation point to the tibial fixation point in the CaP group may be shorter than that in the control group. Therefore, the in situ forces under applied anterior tibial load at higher flexion angles in the CaP group can be larger than those in the control group. 8 At higher flexion angles, the effect of the CaP method may exceed the effect of the surgical method.
The anterior translation and the internal tibial rotation in the CaP group were not significantly different than those in the control group. In our previous study, the CaP-hybridized tendon reduced anterior tibial translation in nonanatomic ACL reconstruction in goats when compared with untreated tendon. 19 Since anatomic ACL reconstruction resulted in superior stability compared with nonanatomic ACL reconstruction, 13,23 significant differences may not have been detected between the CaP and control groups. The CaP-hybridized tendon may not lead to improved stability in anatomic single-bundle ACL reconstruction. The biomechanical functions in the intact ACL group were better than those in the CaP and control groups. The kinematics of the knee are affected by joint geometry and differences in the surrounding tissues caused by osteoarthritis and contracture between the normal and reconstructed knees. Furthermore, ACL reconstruction in goats is not a perfect model of the human operation, requiring different appropriate initial tension, appropriate graft thickness, choice of arthroscopic technique, and rehabilitation protocol, among others.
Clinically, the earlier tendon-bone healing in the CaP group may allow quicker active rehabilitation and could lead to less graft elongation or rerupture. Anatomic single-bundle ACL reconstruction using CaP-hybridized tendon grafts may lead to better postoperative knee function.
There are several limitations to the present study. An animal model of ACL reconstruction was used for this study. The evaluations were performed at only a single time point in this study. A small number of specimens were used for this study. A longer follow-up and use of a larger number of animals are needed to clarify the effects of the CaP-hybridized tendon graft in anatomic single-bundle ACL reconstruction. In the evaluation of bone tunnel enlargement, a comparison with the bone tunnel at time 0 may be necessary. An investigation into the relationship between tendon-bone healing and tendon graft remodeling would also be beneficial.
Conclusion
The CaP-hybridized tendon graft showed improved histologic tendon-bone healing at the joint aperture site in both bone tunnels 6 months after anatomic single-bundle ACL reconstruction in goats. The in situ forces under applied anterior tibial loads at higher flexion angles in the CaP group were also increased. There were no significant differences in laxity or the in situ forces at full extension under applied anterior tibial load and internal tibial torque between both groups. Anatomic single-bundle ACL reconstruction in goats did not restore normal laxity or loads even with the addition of CaP to the graft.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by JSPS KAKENHI (grant No. 24500792).