
Abstract
Background:
Patella alta describes an abnormally high-riding patella in relationship to the femur and has been shown to correlate with patellofemoral pain, instability, chondromalacia, and arthrosis. Conventional measurements of patella alta involve multiple measurements and are often not defined on cross-sectional imaging as related to radiographs.
Hypothesis:
Patellar articular overlap on sagittal magnetic resonance imaging (MRI) will correlate well with conventional measurements of patella alta as measured by a standardized technique defined by our group.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
MRIs of 239 knees were reviewed by 3 attending surgeons with practices focusing on patellofemoral disease, as well as 2 sports medicine fellows and 1 musculoskeletal radiologist. Measurements included articular overlap, percentage of articular coverage, Caton-Deschamps index, Blackburne-Peel index, and modified Insall-Salvati index.
Results:
Interrater reliability was high for Caton-Deschamps, Blackburne-Peel, and modified Insall-Salvati indices (intraclass correlation coefficient [ICC], 0.877, 0.828, and 0.787, respectively). Articular overlap and percentage articular coverage correlated well with each other (ICC, 0.961; P < .001) and with the Caton-Deschamps (overlap r = –0.271, P < .001; coverage r = –0.131, P = .037) and Blackburne-Peel (overlap r = 0.343, P < .001; coverage r = –0.238, P < .001) indices. Articular overlap and percentage coverage failed to correlate with the modified Insall-Salvati index (overlap r = –0.117, P = .091; coverage r = 0.007, P = .918).
Conclusion:
Patellar articular overlap and percentage of patellar articular coverage show promise as a simpler alternative to conventional, ratio-based measurements of patellar height. Future studies are needed to evaluate the range of normal and the relationship to our traditionally used measurements.
Keywords
Patella alta describes an abnormally high-riding patella in relationship to the femur and has been shown to be correlated with patellofemoral pain, instability, chondromalacia, and arthrosis. 1,3,11,12,14,17,19 –24 An abnormally high patella may not engage the trochlear groove as early in knee flexion, allowing patellar instability. Multiple methods of assessing patellar height on plain radiographs have been described in the literature, including the Caton-Deschamps index, 9 the Insall-Salvati ratio 18 and its modified version, 15 the Blackburne-Peel index, 7 Blumensaat line, 8 the Bernageau index, 5 and the Biedert-Albrecht index. 6 All of the aforementioned measurement techniques, with the exception of the Blumensaat line, require a calculation to be performed rather than a simple measurement. Thus, the Blumensaat method of describing patellar location is the simplest of these techniques but requires specific positioning of the knee in 30° of flexion. It has thus been discounted by many authors because of its variability. 26 Biedert and Albrecht 6 described quantifying patellar height relative to the femoral trochlea on magnetic resonance imaging (MRI) in full extension but did not find that their measurement correlated well with other measurements of patellar height.
The lack of consensus regarding direct measurement of factors thought to be important in clinical decision making for patients with recurrent patellofemoral instability prompted our study of these factors in 2 groups of patients: 1 group with anterior cruciate ligament (ACL) tears and 1 group with recurrent patellofemoral instability. We hypothesized that the articular overlap of the patellar undersurface and femoral trochlear cartilage on sagittal MRI would correlate well with, and provide a simple and accurate alternative to, conventional measurements of patellar height.
Methods
In this institutional review board–approved retrospective cohort study, the MRIs of 239 patients were reviewed. MRIs were not obtained in full extension or with quadriceps activation; patients were positioned at rest in standard knee coils. From this group, 130 patients who underwent surgery for recurrent patellofemoral instability and who had preoperative MRIs available for review (PF group) were identified from the surgical records of the senior authors (D.W.G., B.E.S.S., S.S.). To compare this cohort with a control group of representative patients without patellofemoral instability, 109 patients within the same age range were randomly selected from our institution’s ACL registry database (ACL group). The ACL and the PF groups were combined and placed in random order to eliminate potential bias. Six reviewers reviewed the MRI studies for the patients in each group: 3 fellowship-trained orthopaedic surgeons with a practice focus on patellofemoral pathology, plus 2 orthopaedic sports medicine fellows and 1 fellowship-trained musculoskeletal radiologist.
Each reviewer received an identical instruction list with example images for each measurement. To control for potential confounding variables, the MRIs were examined for the knee flexion angle in the scanner as well as the presence or absence of effusion. Knee flexion was measured by drawing each limb of an angular measurement in the center of the medullary canal of the tibia and the femur on the sagittal view at the image showing the Blumensaat line. Knee effusion was noted in case additional joint fluid led to increased knee flexion or allowed for more lateral subluxation of the patella. In an effort to quantify lateral subluxation of the patella, a modified bisect offset was measured, modeled from the measurement described by Pal et al 25 : The widest dimension of the bony patella was noted on its axial MRI image. A line perpendicular to the posterior femoral condylar line on the MRI demonstrating the deepest portion of the femoral trochlea (Figure 1A) was projected to the axial image with the widest patellar dimension (Figure 1B). The width of the bony patella lateral to the bisect line was noted and utilized in comparison with the entire patellar width to calculate the modified bisect offset (Figure 1C).

(A) Posterior condylar line at most caudal portion of trochlea. (B) Axial magnetic resonance image with widest patellar dimension. (C) Bisect offset = a/(a + b).
The total patellar articular length was measured on the sagittal MRI that showed the greatest patellar length and articular cartilage thickness. The same image was then used to measure articular overlap, or the length of patellar cartilage overlying the trochlear cartilage, as measured parallel to the subchondral surface of the patella. The remaining “uncovered” length of patellar cartilage was also recorded so that articular overlap could be reported as an independent variable or as a percentage of overall articular length. Figure 2 demonstrates the measurement technique for articular overlap and percentage overlap (articular overlap divided by the overall patellar articular length). The same sagittal MRI images were utilized to measure the Caton-Deschamps (Figure 3A), Blackburne-Peel (Figure 3B), and modified Insall-Salvati (Figure 3C) indices of patellar height. If the selected sagittal image was deemed inadequate for measurement of the numerator portion of each index, the reviewer was permitted to adjust by a maximum of 1 MRI slice in either direction from the selected sagittal image for the patellar length.
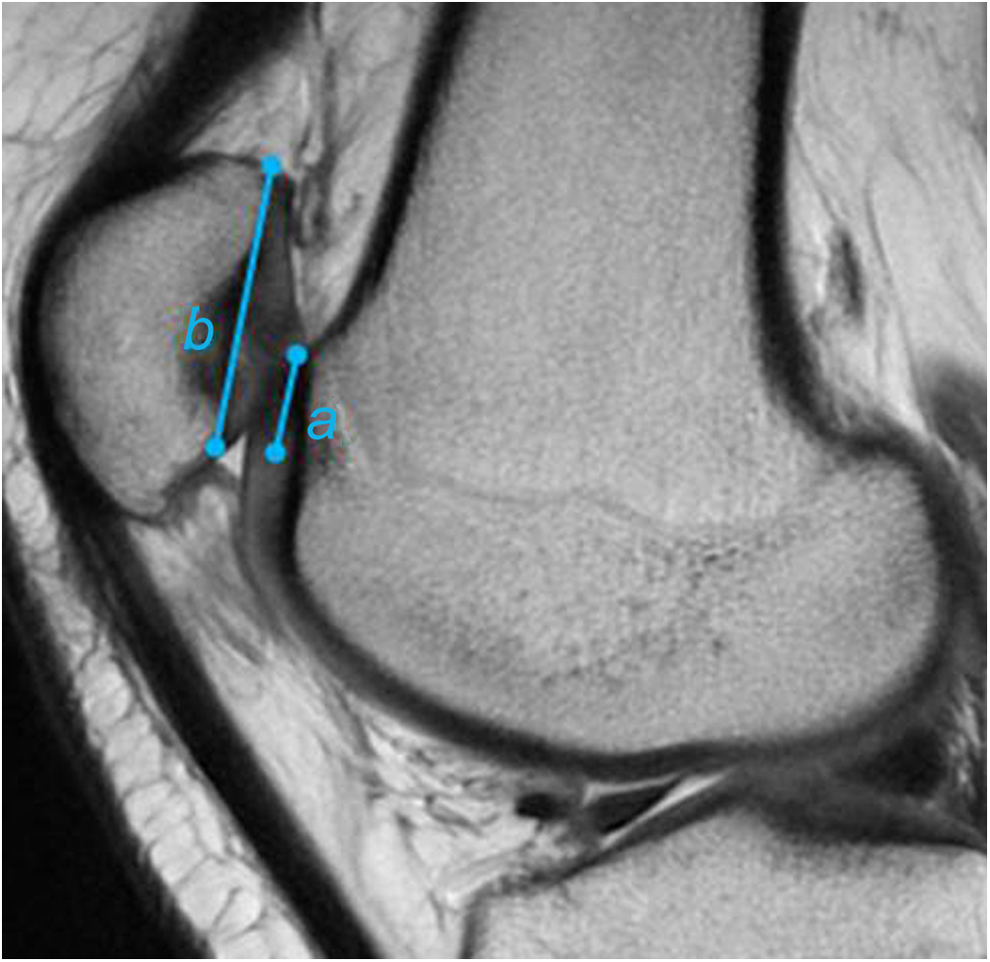
Articular overlap = a. Percentage coverage = (a/b) × 100.

Calculation (a/b) of the (A) Caton-Deschamps index, (B) Blackburne-Peel index, and (C) modified Insall-Salvati index.
Data Collection
Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at the Hospital for Special Surgery. REDCap is a secure, web-based application designed to support data capture for research studies 16 and is supported by a Clinical and Translational Science Center grant (CTSC GRANT UL1TR000457).
Statistical Analysis
Interrater reliability of all measurements between all raters was measured using intraclass correlation coefficients (ICCs) with 95% CIs to estimate the precision of the ICC. Pearson correlation coefficients were calculated to evaluate the bivariate correlation between articular overlap and percentage articular coverage against Caton-Deschamps, Blackburne-Peel, and modified Insall-Salvati indices. Differences in radiographic measurements between patellofemoral pain/instability and ACL patients were compared using independent-samples t tests. All analyses were conducted using SPSS version 22.0 (IBM Corp), with statistical significance set to P ≤ .05.
Results
Interrater reliability was high for articular overlap (ICC, 0.928) and percentage articular coverage (ICC, 0.938) (Table 1). Likewise, interrater reliability was high for Caton-Deschamps, Blackburne-Peel, and modified Insall-Salvati indices (ICC, 0.877, 0.828, and 0.787, respectively). Articular overlap and percentage articular coverage correlated well with each other (r = 0.961, P < .001) and with the Caton-Deschamps (overlap r = –0.271, P < .001; coverage r = –0.141, P = .037) and Blackburne-Peel indices (overlap r = –0.343, P < .001; coverage r = –0.238, P < .001). However, articular overlap and percentage articular coverage failed to correlate significantly with the modified Insall-Salvati index (overlap r = –0.117, P = .91; coverage r = 0.007, P = .918) (Table 2).
Interrater Reliability for Variables in All Patients a
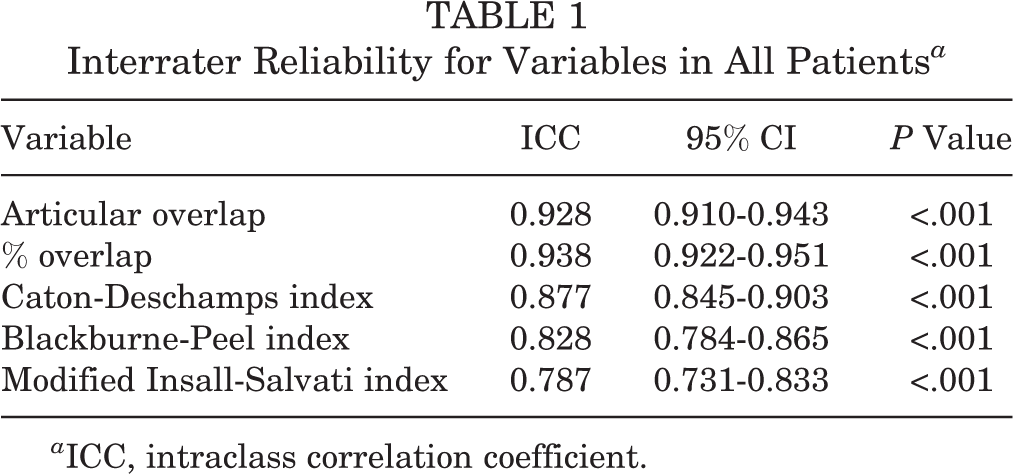
a ICC, intraclass correlation coefficient.
Correlation of Articular Overlap and Percentage Overlap With Standard Measurements of Patellar Height a

a Articular overlap and percentage overlap correlated well with each other and with the Caton-Deschamps and Blackburne-Peel indices, but not with the modified Insall-Salvati index.
When the values for patellar height were classified as categorical variables and compared between the PF and ACL groups (Table 3), significant differences emerged for articular overlap <6 mm (P = .012), Caton-Deschamps >1.2 (P < .001), and Blackburne-Peel >1.0 (P < .001). However, while the PF group exhibited lower mean values for articular overlap and percentage articular coverage than the ACL group, these did not reach statistical significance as continuous variables (P = .218 and .446, respectively). The PF group had significantly higher values for Caton-Deschamps (P < .001), Blackburne-Peel (P < .001), and modified Insall-Salvati (P = .001) indices than the ACL group (Table 4). The PF group also exhibited a significantly higher bisect offset than the ACL group (P < .001).
Comparison of Categorical Variables Between the ACL and PF Groups a

a ACL, anterior cruciate ligament; PF, patellofemoral instability.
Comparison of Continuous Variables Between the ACL and PF Groups a
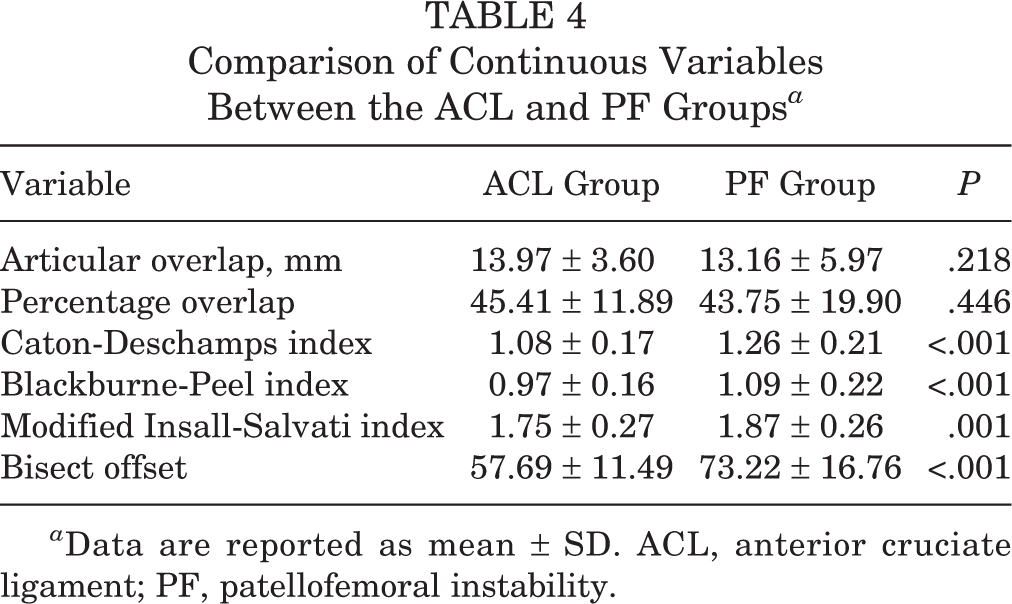
a Data are reported as mean ± SD. ACL, anterior cruciate ligament; PF, patellofemoral instability.
The ACL group was found to have a 6.5% rate of patella alta as defined by Caton-Deschamps >1.2, and the PF group was found to have a 39.7% rate of patella alta (P < .001). When measured by Blackburne-Peel >1.0, the ACL group exhibited an 8.3% rate of patella alta, and the PF group 30.2% (P < .001). When separated by these definitions of patella alta, the groups were found to have significant differences in articular overlap in both instances (P < .001 for both Caton-Deschamps and Blackburne-Peel) (Table 5). However, no receiver operating characteristic (ROC) curve could be generated with a false-positive rate less than 25%, so no formal cutoff has been suggested.
Correlation of Articular Overlap With Conventional Measurements of Patella Altaa

a Data are reported as mean ± SD.
Discussion
The Caton-Deschamps index, 9 Insall-Salvati ratio, 18 modified Insall-Salvati ratio, 15 Blackburne-Peel index, 7 Blumensaat line, 8 and Bernageau index 5 were designed based on plain radiographs. Utilization of a system that is based on a lateral plain radiograph expands its utility for the general orthopaedic population who may not have undergone advanced imaging. However, Biedert and Albrecht 6 considered their MRI-based method to be potentially superior because, as shown by van Huyssteen et al 28 and Staeubli et al, 27 bony anatomy is not necessarily predictive of the precise location of articular cartilage on the undersurface of the patella and in the femoral trochlea. While the Biedert-Albrecht patellotrochlear index was found to have good interobserver reliability, it did not correlate well with traditional radiographic measurements of patellar height. 2,4 This may be due in part to the fact that the Biedert-Albrecht index was measured in full extension, allowing slackening of the patellar tendon and potential understatement of any patella alta as measured on flexed knee lateral radiograph. In addition, systems that require several measurements to determine patellar location introduce increased opportunity for error.
Dejour et al 10 recently published a study of the Sagittal Patellofemoral Engagement (SPE) index, a measurement similar to percentage articular coverage. Patellar overlap of the trochlea was measured on 2 different sagittal MRI images: one with the greatest length of patellar cartilage and the other with the greatest length of femoral trochlear cartilage. This measurement failed to correlate with the Caton-Deschamps index.
In our methods, percentage articular coverage was included in the list of measurements in case the overall length of the patella affected the correlation of the new measurements with the conventional indices. This did not prove to be the case, as both the articular overlap and percentage articular coverage measurements correlated well with both Caton-Deschamps and Blackburne-Peel indices. As a continuous variable, while the PF group had significantly more patella alta than the ACL group as measured by the conventional indices of patellar height, the differences in articular overlap and percentage articular coverage between the 2 groups failed to reach statistical significance. This may be due in part to normal variance among PF group patients: Not all patients with patellofemoral instability exhibit patella alta. When articular overlap was defined by a cutoff of less than 6 mm as a definition of patella alta, however, the groups proved statistically significant. Thus, prospective studies are needed to determine cutoffs of normal versus pathologic measurements of articular overlap and percentage articular coverage.
Strengths and Limitations
The patients in the ACL registry do not truly constitute a “normal” control group given their proven pathology. We elected to utilize these MRIs rather than recruit normal subjects for new MRIs given the retrospective nature of the study and the cost associated with new MRI studies. Likewise, only those patients with patellofemoral pathology who had preoperative MRIs in our institution’s radiology system were selected, introducing potential selection bias. We did not specifically quantify patellar tilt or subluxation as part of our measurements, and instead utilized the modified bisect offset as an overall combination of the two. This decision was made consciously to avoid complicating the study and burdening the reviewers with measurements that are not primarily utilized in clinical decision making.
The conventional measurements of patellar height utilized in this study were originally described for use on plain radiographs, and our study focused on MRI. Unfortunately, because many of the patients presenting for care at our institution travel significant distances, their plain radiographs were obtained at outside facilities and either contained suboptimal lateral views or were unobtainable for our study. A “perfect” lateral radiograph can be difficult to obtain in the office and often requires more than 1 attempt, adding to the radiation exposure. In addition, knee flexion can vary between radiographs, potentially changing the values involved in the conventional ratios as the patellar tendon is on different tension. Up to 70% of patients with patellofemoral instability have been found to have chondral or osteochondral injury. 13 We therefore consider MRI to be a standard of care portion of the orthopaedic evaluation of a patient with patellofemoral instability. A final concern is that knee position in an MRI coil tends to be closer to full extension than in a standard lateral radiograph, potentially allowing slackening of the extensor mechanics. Our measurements may therefore tend to underestimate patella alta by conventional methods.
Conclusion
Patellar articular overlap correlates well with conventional measurements of patellar height in the sagittal plane and shows promise as a simpler alternative to the conventional indices. The strong correlation of our measurements of patellar height with patellar instability indicates their potential utility as standardized methods of translating conventional indices from plain radiographs to cross-sectional imaging. Articular overlap <6 mm on sagittal MRI is useful as a corollary of conventional definitions of patella alta by Caton-Deschamps and Blackburne-Peel measurement. Prospective clinical and biomechanical studies are needed to establish the normal and pathologic ranges of these values and determine their specific roles in the pathophysiology of patellofemoral instability.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: J.L.M. has received education grants for resident simulation training from Arthrex and Acumed; J.T.N. has received an outside grant from the Clinical and Translational Science Center for salary support; D.W.G. is a consultant for Arthrex; a close family member of B.E.S.S. is a consultant for Arthrex; S.S. owns stock/stock options in Zimmer.