
Abstract
Background:
Osteoconductive additives are used in resorbable interference screws for anterior cruciate ligament (ACL) reconstruction to improve graft incorporation and mitigate adverse effects. There are no published studies that compare biological performances of bioresorbable and biocomposite screws without artifacts due to different follow-up times and intrinsic patient characteristics.
Purpose/Hypothesis:
The purpose of this study was to evaluate the efficacy of osteoconductive agents in bioresorbable screws for ACL reconstruction at minimum follow-up of 2 years by intrapatient comparison. The hypothesis was that osteoconductive ceramics would result in slower resorption, improved ossification, and less tunnel widening.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 28 ACL reconstructions at 2 centers were randomly assigned into 2 comparable groups: (1) the graft was fixed in the tibia using standard bioresorbable screws and in the femur using biocomposite screws with osteoconductive agents (biphasic calcium phosphate), and (2) the graft was fixed in the femur using a standard bioresorbable screw and in the tibia using a biocomposite screw with osteoconductive agents.
Results:
Twenty-seven patients completed evaluations at 29.9 ± 4.0 months. Resorption was complete for more bioresorbable (81%) than biocomposite (37%) screws (P = .0029), whereas satisfactory ossification was observed in more biocomposite (52%) than bioresorbable (15%) screws (P = .0216). The tunnel shape was normal in more biocomposite (81%) than bioresorbable (48%) screws (P = .0126), and marked cortical formation was twice more frequent for biocomposite (78%) than bioresorbable (37%) screws (P = .0012). Bioresorbable screws exhibited faster resorption in the femur (P = .0202) but not in the tibia (not significant). Conversely, biocomposite screws demonstrated better ossification, less tunnel widening, and more cortical formation in the tibia (P < .0001, P = .0227, and P < .0001, respectively) but not in the femur (not significant for all).
Conclusion:
Osteoconductive additives can reduce the extent of resorption while improving ossification, reducing tunnel widening, and increasing cortical formation.
Clinical Relevance:
The benefits of osteoconductive agents justify their associated costs for ACL reconstruction, particularly in the tibia.
Keywords
Bioresorbable interference screws for ligament reconstruction surgery were introduced to overcome disadvantages of metallic screws, including potential damage to grafts, need for surgical removal at a later stage, and distortion of postoperative scans. 15,27,37 Despite their widespread use, concerns persist regarding bioresorbable screws made of pure polymer due to undesirable biological responses, including screw migration, 27 tunnel widening, 12,17,24,25,33 and cyst formation, 40 in addition to risks of screw fracture during insertion 35 and unclear mechanical properties. 19,20,27
Bioresorbable polymers have been studied since the 1960s
21,22
and were first used in anterior cruciate ligament (ACL) reconstruction in the 1990s.
7
Initially, the main constituent was poly-
To improve bone ingrowth during screw resorption, osteoconductive ceramics such as β-tricalcium phosphate (β-TCP) or hydroxyapatite (HA) were added in different proportions to buffer the acidic degradation of bioresorbable polymers, 1,6,8,18 forming a new type of biocomposite screws. 1,2,4,18,26 Barber and Dockery 5 reported that at 7 years of follow-up, despite lengthy periods needed for complete degradation, PLLA screws were not completely replaced by bone. In another study at 4 years of follow-up, 4 the same authors evaluated in vivo degradation of β-TCP-PLLA screws, which proved osteoconductivity in most sites (75%) but yielded complete substitution by bone in only 10% of cases. In a later study at 3 years of follow-up, 6 the authors evaluated performance of PLLA/PGA/β-TCP composite screws with consistent findings: complete degradation and osteoconductivity confirmed in 81% of sites but complete substitution by bone in only 21% of cases. There are few published studies that directly compare biological performances of bioresorbable and biocomposite screws in ACL reconstruction; therefore, there is little evidence to justify the benefits or costs of osteoconductive agents.
The purpose of this study was to evaluate the efficacy of osteoconductive ceramics in bioresorbable screws for ACL reconstruction, at a minimum follow-up of 2 years, through a prospective intrapatient comparative study. The hypothesis was that osteoconductive ceramics would result in slower resorption, improved ossification, and less tunnel widening. To our knowledge, there are no published studies that compare intrapatient biological performances of the 2 materials without artifacts due to different follow-up times and intrinsic patient characteristics (age, sex, metabolic level, daily activities, etc). Such comparisons would enable clinicians to select the appropriate material for patients and to justify the associated costs.
Methods
Study Design
We designed this prospective bicentric investigation in December 2010, and the institutional review board (IRB) approved the study protocol for both centers in February 2011 (IRB approval number 2011-001). In the period from May to December 2011, 60 patients who underwent primary ACL reconstruction by the 2 senior surgeons (J.B., N.G.) were requested to enroll in the study, of whom 28 provided written consent to participate and were eligible for inclusion.
The inclusion criteria were: adult patients with complete ACL tears confirmed (1) radiographically using magnetic resonance imaging (MRI) and (2) clinically by 2 or more indicators of instability (positive pivot shift, soft endpoint at the Lachman test, physical sensation of instability, and/or laximetry test >3 mm). The exclusion criteria were: adolescents, bilateral procedures, history of fracture or surgery on the operated knee, as well as metabolic diseases that could alter bone growth.
Two different interference screws, supplied by the same distributor (Amplitude SAS), were used for graft fixation in each patient: (1) Eclipse standard bioresorbable screw (THT Bioscience SAS), made entirely of PLDLLA (70%
The patients were randomly assigned into 2 comparable groups by alternating the location of the 2 interference screws in the tibia or in the femur in the consecutive order of operations (Table 1). In group A, the graft was fixed in the tibia using a bioresorbable screw and in the femur using a biocomposite screw. In group B, the graft was fixed in the tibia using a biocomposite screw and in the femur using a bioresorbable screw.
Patient Demographics a
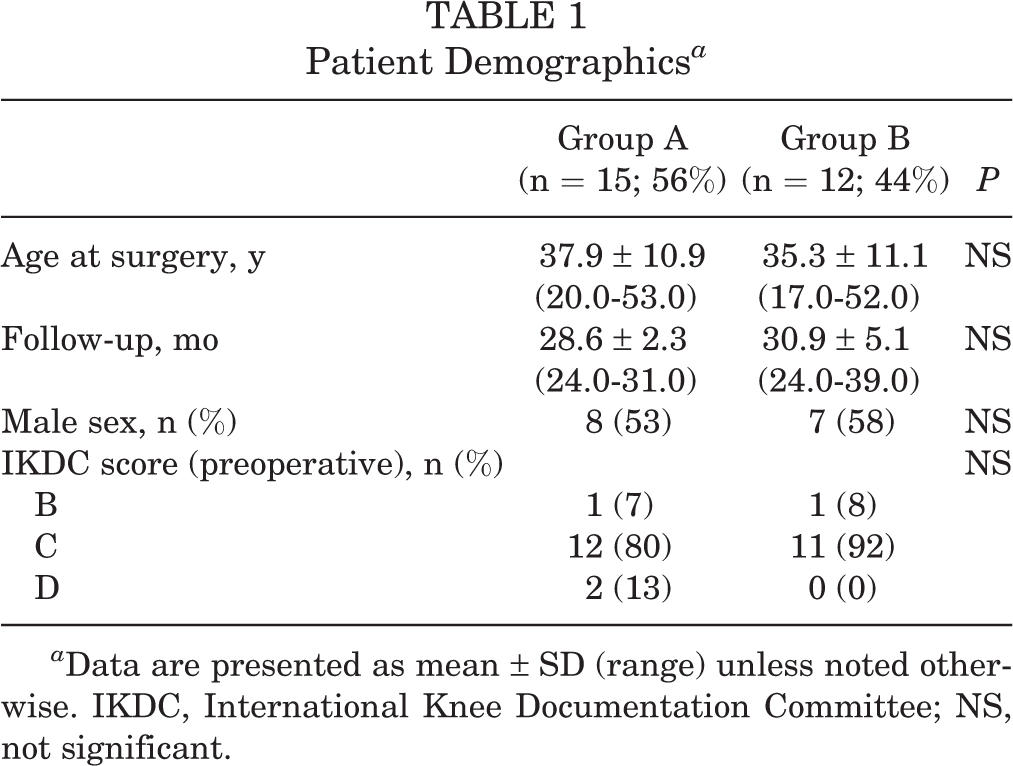
a Data are presented as mean ± SD (range) unless noted otherwise. IKDC, International Knee Documentation Committee; NS, not significant.
Operative Technique
All operations were performed under general or spinal anesthesia with the patients in the supine position and a tourniquet placed high on the thigh. The operative technique and surgical instrumentation (Amplitude SAS) were identical for all patients and for both types of interference screws. A lateral post at the tourniquet level maintained leg position in the frontal plane, and a distal support positioned the knee at 90° of flexion, allowing full range of motion if needed.
All patients received single-bundle autografts harvested from the hamstrings. The cartilage and meniscus status were assessed through 2 standard portals: optical and instrumental. 36 Meniscal repair procedures were performed in 10 knees.
Graft Preparation
The graft was harvested from the hamstrings to form a 4-strand configuration using the gracilis and semitendinosus, which were left attached on their tibial insertions then doubled and sutured together to achieve appropriate length and thickness for the size of the patient. The femoral tunnel was prepared using an outside-in guide for femoral tunnel placement. The tibial tunnel was prepared with a standard 60° angulation guide using the landmarks described by Purnell et al. 28 The diameters and depths of interference screws were selected depending on the calibrated length and thickness of the graft obtained. A modified Lemaire extra-articular procedure 14 was performed in 4 knees with a strip of the iliotibial band 8 cm long and 10 mm wide, with the insertion on the Gerdy tubercle preserved in case of explosive pivot shifts. In those 4 cases, the lateral tenodesis fixation was always distant from the ACL graft fixation sites and unlikely to influence the interference screws on either tibial or femoral sides. The isometric point for lateral tenodesis was determined in a similar way to the Lemaire procedure, just posterior to the lateral epicondyle, and the graft traction sutures were used for fixation without passage under the lateral collateral ligament, introduced through a 6-mm femoral bone tunnel in the isometric position, and fixed with an interference screw. The strip was tightened with the knee in 70º of flexion and neutral rotation. There were no intraoperative complications encountered.
Postoperative Rehabilitation
Progressive rehabilitation was followed immediately after surgery, with passive and active motion exercises as tolerated by the patient. Range of motion exercises aimed at obtaining full extension but avoiding hyperextension, and there was no limitation in flexion. Weightbearing was allowed with crutches during the first 3 weeks, and progressive return to sports activities was authorized after 6 to 9 months. For knees in which lateral tenodesis and/or meniscal repairs were performed, the range of motion exercises and return to weightbearing were moderated according to the ability of each patient.
Clinical and Radiographic Evaluation
Clinical and radiographic evaluations were conducted 24 months after surgery. The clinical assessment was based on the International Knee Documentation Committee (IKDC) objective form. The radiographic assessment was based on computed tomography (CT) scans obtained following the same protocol using an Aquilion RXL 16-detector row low-dose scanner (Toshiba) with the following settings: 120 kV, 100 mAċs, 0.5-mm slice thickness, reconstruction filters “bone” (FC90) and “soft” (FC08). The native images were imported into an image-processing software (OsiriX; Pixmeo SARL) dedicated to DICOM images. 31,32 The imaging software enabled simultaneous visualization of CT cross-sections in 3 planes (frontal, sagittal, and transverse) to address quantitative and qualitative measurements. Specimens of the 2 interference screws were scanned in vitro with the same machine and setting to calibrate their radiodensity in Hounsfield units (HU). The average recorded values for the 2 types of screws immersed in water were 153 HU for the standard bioresorbable screw and 1144 HU for the BCP biocomposite screw.
On each patient scan, the following parameters were qualitatively assessed in a single iteration on both tibial and femoral segments on multiple transverse slices to ensure tunnels were evaluated along their full length. This was performed by an experienced radiologist (R.B.) who was blinded to the types of screws implanted: Resorption (Figure 1), based on the visibility of the screw within the bone tunnel, with reference to established radiodensities for cortical bone (350-500 HU), cancellous bone (150-160 HU), and resorbable interference screws (200-300 HU)
5
: Intact, distinct, continuous, and homogeneous solid Visible, nonhomogeneous solid with some dissolution Ghost, diminished solid with considerable dissolution Resorbed, invisible, replaced by bone or scar tissue Ossification as described by Barber and Dockery
4
: Grade 1: Little or no ossification Grade 2: Some ossification, discontinuous or with a wide lucent rim Grade 3: Ossification with thin lucent rim Grade 4: Good ossification, border of tract vague Tunnel widening (Figure 2) compared with the screw tract: None, unchanged Figure-of-eight
3
Enlarged, widening at some levels Wide, considerable widening at all levels Cortical formation, denoting the presence of a thin or marked cortical rim around the tunnel wall. Cyst formation, noting size and location.

Screw resorption based on the visibility of the screw within the bone tunnel. (A) Intact, distinct, continuous, and homogenous solid; (B) visible, nonhomogenous solid with some dissolution; (C) ghost, diminished solid with considerable dissolution; and (D) resorbed, invisible, replaced by bone or scar tissue.

Tunnel widening compared with the screw tract. (A) None, unchanged; (B) figure-of-8; (C) enlarged, widening at some levels; and (D) wide, considerable widening at all levels.
All patients provided informed consent for the use of their data for research, and the ethical board of both centers approved the study in advance (IRB approval number 2011-001).
Statistical Analysis
Statistical analyses were performed using R version 3.1.3.1 (R Foundation for Statistical Computing). Multivariable analyses were performed to determine whether radiographic outcomes were influenced by screw material, screw location, or patient sex. Descriptive statistics were used to summarize the data. As data were not normally distributed, the statistical analyses were nonparametric. Between-group differences were tested using Wilcoxon rank sum tests (Mann-Whitney U test). Categorical data were analyzed using Fisher exact tests. P values <.05 were considered statistically significant.
Results
Of the original 28 patients enrolled, a total of 27 patients (14 men, 13 women) completed clinical and radiographic evaluation at mean follow-up (±SD) of 29.9 ± 4.0 months (median, 30 months; range, 24-39 months). There were no intraoperative complications or postoperative complications. There were no revisions or reoperations.
The preoperative objective IKDC score was B in 2 knees, C in 22 knees, and D in 1 knee and the postoperative objective IKDC score was A in 10 knees, B in 14 knees, and C in 1 knee (a 30-year-old female who had a marked pivot shift). The postoperative subjective IKDC score, available for 25 of 27 patients, was a mean ± SD of 83.3 ± 12.9 (median, 89.7; range, 54-100), which was weakly but significantly correlated to time interval between operation and imaging (Pearson r = 0.41; 95% CI, 0.022-0.695; P = .04).
The radiographic evaluation revealed complete resorption of 32 screws (59%) and satisfactory ossification (Barber grades 3 and 4) in 18 screws (33%). Tunnel widening was observed to different extents around 19 screws (35%) and marked cortical formation was seen around 31 screws (57%). There were no cysts nor screw migration observed.
Univariate Analysis
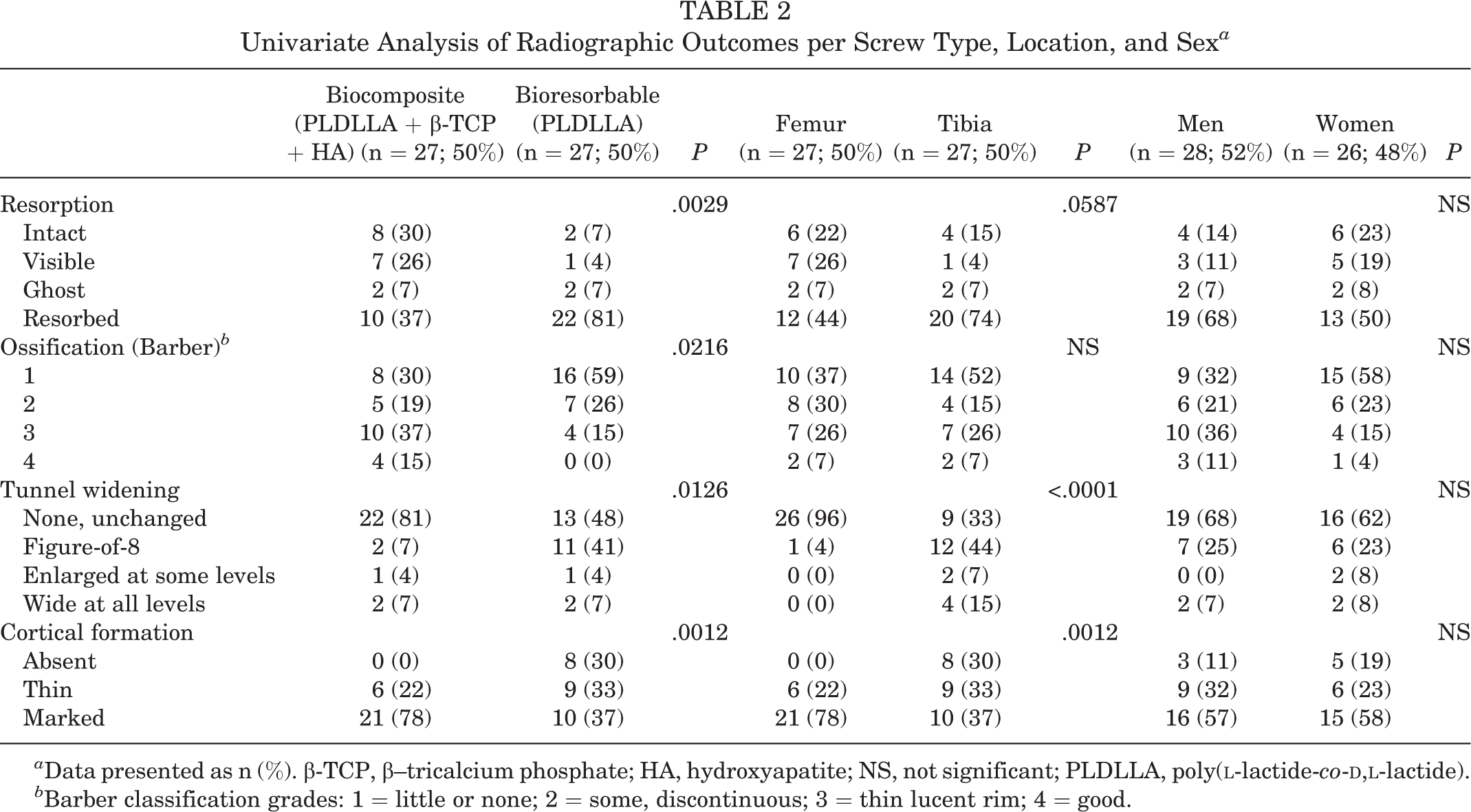
Comparing radiographic findings for the 2 types of interference screws, resorption was complete for more of the bioresorbable (81%) than the biocomposite (37%) screws (P = .0029), whereas satisfactory ossification (Barber grades 3 and 4) was observed in more of the biocomposite (52%) than the bioresorbable (15%) screws (P = .0216) (Table 2). Furthermore, the shape of the tunnel was unchanged or “normal” in more of the biocomposite (81%) than the bioresorbable (48%) screws (P = .0126), and likewise marked cortical formation was twice more frequent for the biocomposite (78%) than the bioresorbable (37%) screws (P = .0012).
Univariate Analysis of Radiographic Outcomes per Screw Type, Location, and Sex a
a
Data presented as n (%). β-TCP, β–tricalcium phosphate; HA, hydroxyapatite; NS, not significant; PLDLLA, poly(
b Barber classification grades: 1 = little or none; 2 = some, discontinuous; 3 = thin lucent rim; 4 = good.
Comparing radiographic findings in the femur and the tibia, complete resorption was more frequent in the tibia (74%) than in the femur (44%) (P = .0587) whereas satisfactory ossification (Barber grades 3 and 4) was identical in both bones (33% each) (P = .54). Moreover, the shape of the tunnel was “normal” in almost all femurs (96%) but only in one-third of tibiae (33%) (P < .0001), and marked cortical formation was twice more frequent in femurs (78%) than tibiae (37%) (P = .0012).
Radiographic findings were not correlated with patient age or sex. The clinical scores were not correlated with any radiographic outcomes, except for ossification in the femur, where satisfactory ossification (Barber grades 3 and 4) was associated with higher subjective IKDC scores (P = .006).
Bivariate Analysis
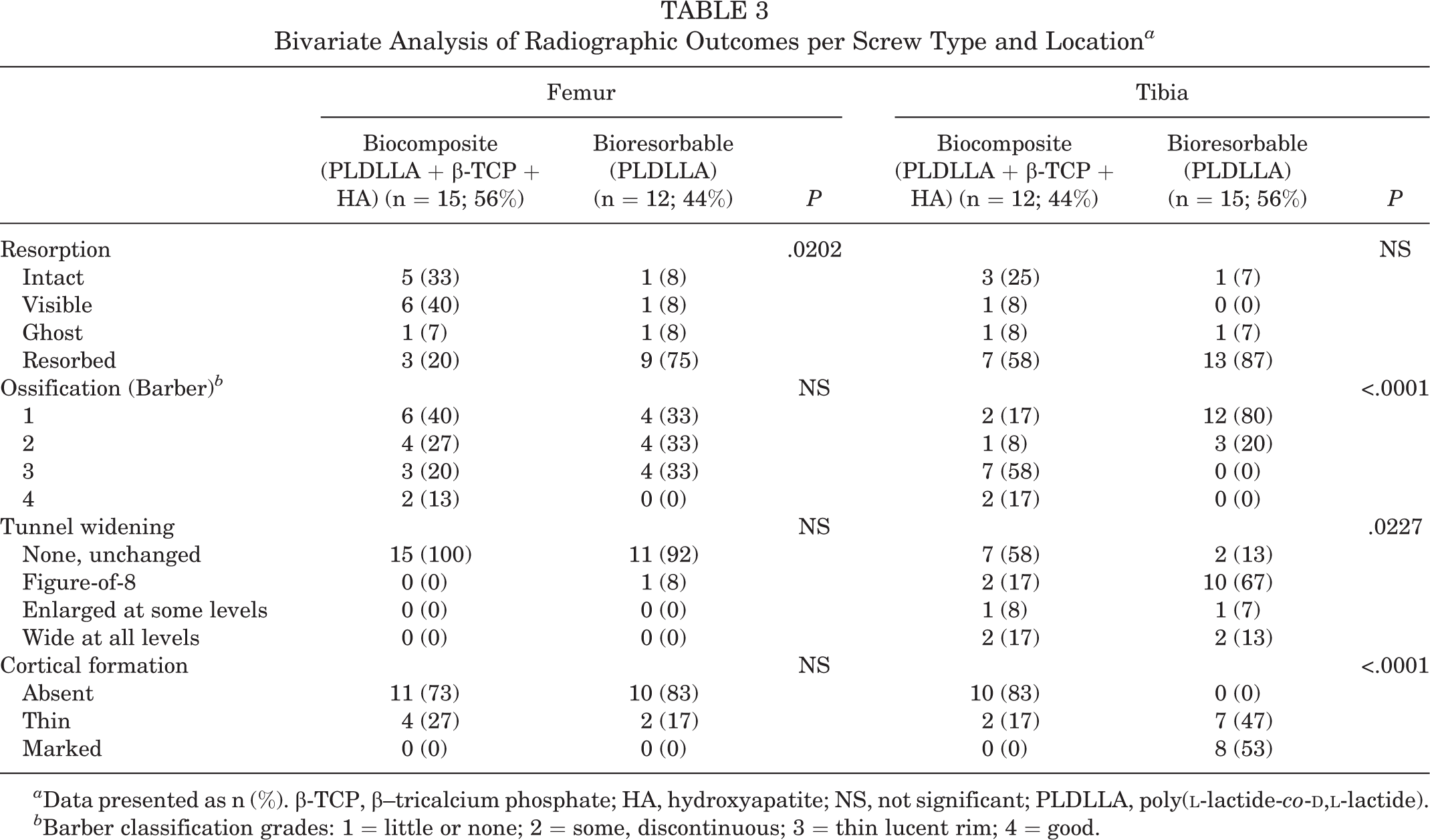
When considering the femur and tibia separately, the 2 types of screws exhibited different outcomes. Bioresorbable screws exhibited significantly greater resorption in the femur (P = .0202) but not in the tibia (not significant) (Table 3). Conversely, biocomposite screws demonstrated significantly better ossification, less tunnel widening, and more cortical formation in the tibia (P < .0001, P = .0227, and P < .0001, respectively) but not in the femur (not significant for all).
Bivariate Analysis of Radiographic Outcomes per Screw Type and Location a
a
Data presented as n (%). β-TCP, β–tricalcium phosphate; HA, hydroxyapatite; NS, not significant; PLDLLA, poly(
b Barber classification grades: 1 = little or none; 2 = some, discontinuous; 3 = thin lucent rim; 4 = good.
Discussion
The most important finding of this intrapatient study was that, at a mean follow-up of 2.5 years, the addition of osteoconductive agents to bioresorbable interference screws significantly decreased the extent of resorption while improving ossification, reducing tunnel widening, and increasing cortical formation. Moreover, the benefits of osteoconductive additives were more discernible in the tibia than in the femur. The secondary finding was that, compared with tibial screws, femoral screws generally exhibited slower resorption, less tunnel widening, and more cortical formation.
The purpose of this study was to evaluate the efficacy of osteoconductive ceramics in bioresorbable screws for ACL reconstruction at a minimum follow-up of 2 years. The hypothesis was that osteoconductive ceramics would result in slower resorption, improved ossification, and less tunnel widening. The results confirm the hypothesis that osteoconductive additives effectively improve performance of tibial PLDLLA screws, though their benefits are less pronounced for femoral PLDLLA screws.
The ossification rate inevitably depends on the resorption rate. On one hand, if resorption outpaces ossification, the screw tract could become filled with fibrous tissue and there would be insufficient matrix scaffold to support bone ingrowth. On the other hand, if resorption is much slower than ossification, the screw could represent a physical barrier to osteocyte proliferation. Our findings affirm these observations as they demonstrate that at 2 years, fully resorbed screws had lower grades of ossification. Remodeling of the tunnel to fill with cancellous bone is favorable for graft healing and in case of revision surgery. 18,26 The addition of TCP or HA is known to buffer the acidic degradation of bioresorbable polymers 1,6,8,18 and thereby maintain a longer lasting scaffold for bony ingrowth and prevent sharp declines in local pH levels. 1 Johnston et al 18 found that HA promotes ossification of PLLA screws and noted complete resorption in their entire series at 5 years. Tecklenburg et al 38 evaluated resorption and ossification of HA-PLLA and TCP-PLLA screws and found no signs of degradation nor ossification at 2 years. It seems that 2 years is insufficient time for complete resorption and ossification of some bioresorbable polymers (semicrystalline) such as PLLA and for biocomposite materials whose polymer matrix is also made of PLLA, as outlined in the review article of Kontakis et al. 20 While Barber and Dockery 5 estimated resorption times to be over 24 months for PLLA screws, 39 Kontakis et al 20 found different resorption times, ranging from 4 to 7 weeks for PGA screws, 2 to 3 years for PDLLA screws, and over 5 years for PLLA screws.
Tunnel widening is a matter of concern as it precludes revascularization and ossification of the screw tract and jeopardizes long-term graft integrity. 10 It is unclear whether tunnel widening can be prevented or limited by cortical formation. Tunnel widening generally occurs within the first 3 to 6 months and stabilizes thereafter. 8,10,33 It can be caused by a multitude biologic and mechanical factors. 10,12,17,23,25,33 Biologic factors include synovial fluid infiltration, which would induce osteolytic cytokines, heat necrosis from tract drilling, and nonspecific inflammatory responses; mechanical factors include micromotion, bungee-cord effect redirecting forces at the tunnel entrance, and accelerated rehabilitation. In agreement with our findings, Robinson et al 30 demonstrated that tunnel widening can be reduced by the addition of HA to interference screws, though few others investigated the effects of material compositions particularly, though numerous studies were conducted to compare widening using Endobuttons versus screws. 10,12,17,23,25,33 The majority of studies that focused on tunnel widening followed quantitative approaches to compare diameters or cross-sectional areas of tunnels at different time intervals. 8,10,12,17,23,25,33 In our experience, measuring tunnel diameter or area is challenging and subjective as it is difficult to establish the level of measurement and radiographic incidence angle.
The present data reveal considerable differences in radiographic outcomes between the femur and the tibia, which imply that optimal composition may be different depending on screw location. While biocomposite screws are associated with higher costs than standard bioresorbable screws, their superior performance is only observed in the tibia, not in the femur. Numerous authors have demonstrated differences between bone densities 9,13 and remodeling rates 18 of the distal femur compared with the proximal tibia. Because of its lower density and because the line of applied force is parallel to the axis of the tibial tunnel, tibial fixation is weaker, less stiff, and more likely to slip under cyclic loading than fixation using the femoral fixation site. 11
Bioresorbable interference screws were introduced to overcome disadvantages of metallic screws, including potential damage to grafts, need for surgical removal, and distortion of postoperative images. 15,27,37 Despite their widespread use, concerns of adverse responses persist, including migration, 27 tunnel widening, and cyst formation. 40 The function of a bioresorbable screw in ACL reconstruction is to grant sufficient fixation until the graft incorporates and to resorb sufficiently while promoting osteoconductivity until completely replaced by bone. 4,8,42 Osteoconductive ceramics such as β-TCP or HA were introduced in bioresorbable screws to enhance the rate of bone replacement in the tunnel as the screw resorbs. 1,2,4,18,26 The costs of biocomposite screws are considerably greater than those of standard bioresorbable interference screws, 18,19,27,29 though the selling prices and government reimbursements differ between countries and manufacturers. There are few published studies that directly compare biological performances of bioresorbable and biocomposite screws in ACL reconstruction, providing little evidence to justify the benefits or costs of osteoconductive agents.
The present study has several limitations, including the small cohort sizes, short follow-up times, and the qualitative nature of radiographic outcomes analyzed. Furthermore, the clinical assessment overlooked pain and inflammation as separate outcomes, although they were accounted for within the IKDC score. It would certainly be beneficial to reevaluate our series at a follow-up of 5 years or longer and to expand the number of patients. The study has some strengths, however, notably its prospective and comparative design, the inclusion of patients operated on by 2 independent surgeons at 2 different centers, and the ability to perform intrapatient analyses of biological performance and thereby reduce artifacts due to different follow-up times and intrinsic patient characteristics.
Conclusion
The addition of biphasic calcium phosphate to PLDLLA interference screws used in ACL reconstruction reduces the speed of resorption while improving ossification, reducing tunnel widening, and increasing cortical formation. The benefits of osteoconductive additives are more discernible in the tibia than in the femur. To our knowledge, there are no published studies that compare intrapatient biological performances of the 2 materials without artifacts due to different follow-up times and intrinsic patient characteristics. Such comparisons would enable clinicians to select the appropriate material for patients and to justify the associated costs.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Financial support was received from Amplitude SAS for manuscript preparation.