
Abstract
Background:
Various tenodesis methods are being used for long head of the biceps tendon lesions. However, there is no consensus on the most appropriate surgical method.
Hypothesis:
There are significant differences in incidence of cosmetic deformity and persistent bicipital pain between open subpectoral and arthroscopic intracuff tenodesis groups.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included 72 patients who underwent biceps tenodesis and rotator cuff repair between January 2009 and May 2014 and who were followed for at least 1 year. Open subpectoral tenodesis was performed in 39 patients (group A), and arthroscopic intracuff tenodesis was performed in 33 patients (group B).
Results:
In group A, the mean visual analog scale (VAS) score for pain during motion and mean University of California, Los Angeles (UCLA) and Constant scores significantly improved from 4.6, 18.6, and 64.5 preoperatively to 1.9, 30.5, and 86.5 at last follow-up, respectively (P < .001 for all). In group B, these scores significantly improved from 5.1, 17.6, and 62.9 preoperatively to 1.8, 31.5, and 85.9 at last follow-up, respectively (P < .001 for all). Popeye deformity was noted in 2 (5.2%) patients from group A and 5 (15.6%) patients from group B (P = .231). Additionally, persistent bicipital tenderness was noted in 1 (2.6%) patient from group A and 8 (24.2%) patients from group B (P = .012).
Conclusion:
Both open subpectoral tenodesis and arthroscopic intracuff tenodesis show good clinical outcomes for long head of the biceps tendon lesions. However, open subpectoral tenodesis may be more appropriate, considering the low incidence of Popeye deformity and tenderness.
Lesions of the long head of the biceps tendon (LHBT) are commonly associated with rotator cuff tears and are known to cause shoulder pain and functional impairment. 1,2,10 An operative procedure to treat LHBT pathology is often performed along with rotator cuff repair. 2,16
Various surgical procedures have been proposed to address pathological conditions associated with the LHBT, and these are generally classified into tenotomy and tenodesis. The potential advantage of tenodesis over simple tenotomy is the avoidance of complications, including muscle atrophy and cramping, weakness in elbow flexion and supination strength, and cosmetic deformity. 15,22,24 Therefore, tenodesis has increased in popularity. Numerous fixation approaches for tenodesis have been suggested, which are generally classified into arthroscopic and open approaches. 27,28 The different tenodesis techniques can be divided into soft tissue fixation and bony fixation, 24 and bony fixation is further divided into suprapectoral tenodesis and subpectoral tenodesis based on its position, using the pectoralis major muscle as a reference. 11
Soft tissue tenodesis was first introduced by Rodosky et al, 21 and it has been shown to be more cost-effective than bony fixation. 7,13 Additionally, it has been shown to be simpler and faster to perform than bony fixation and is therefore more effective for concomitant lesions, which require procedures such as rotator cuff repair. 18 Additionally, a soft tissue tenodesis allows the biceps tendon to augment the rotator cuff repair. 2,4 Among the bony fixation techniques, suprapectoral biceps tenodesis has emerged as a popular technique because it can be performed arthroscopically and is easier to perform than subpectoral biceps tenodesis. 11,28 However, because of concerns that postoperative bicipital pain can persist after proximal tenodesis, some authors have suggested subpectoral tenodesis as optimal. 1,16,17,20 Subpectoral tenodesis has been shown to have a superior biomechanical biceps length-to-tension relationship compared with arthroscopic suprapectoral tenodesis. 15,16,30 Additionally, it has a low probability for neurological injury owing to the large distance between the tenodesis site and nerves 12,26 and has the ability to eliminate potential lesions from the bicipital groove. 1,12,16,20 However, its disadvantage is that it requires an additional open procedure. 17,30 A number of different tenodesis techniques are being used for the treatment of LHBT lesions. However, the ideal tenodesis technique and tenodesis site remain controversial.
The purpose of the present study was to present the clinical outcomes and compare the incidences of cosmetic deformity and persistent bicipital pain between open subpectoral tenodesis and arthroscopic intracuff tenodesis (a type of soft tissue tenodesis) performed along with rotator cuff repair in patients with concomitant LHBT lesions and rotator cuff tears. We hypothesized that there would be significant differences in the incidence of cosmetic deformity and persistent bicipital tenderness between open subpectoral and arthroscopic intracuff tenodesis.
Methods
This was a retrospective study, and final approval of exemption by the institutional review board at our institution was obtained (KMC IRB 1530-04).
Demographic Data
A total of 89 patients underwent biceps tenodesis at our institution between January 2009 and May 2014. Of these 89 patients, 72 who underwent simultaneous rotator cuff repair and who were followed up with for at least 1 year were included in the present study. Seventeen patients were excluded because they had an intact rotator cuff tear, an isolated subscapularis tear, or a rotator cuff tear that was not repaired. Open subpectoral tenodesis was performed in 39 patients (group A), and arthroscopic intracuff tenodesis was performed in 33 patients (group B). In group A, the mean patient age was 59.6 years (range, 39-79 years) and the mean follow-up was 22.9 months (range, 16-37 months). In group B, the mean patient age was 63.6 years (range, 52-75 years) and the mean follow-up was 24.2 months (range, 12-64 months).
The rotator cuff tear size was measured intraoperatively using a calibrated probe under direct arthroscopic visualization after debridement of the degenerated tendon edges. The tears were classified based on the size of the greatest diameter of the tear, according to the system proposed by DeOrio and Cofield. 6 In group A, there were 15 small-sized tears, 17 medium-sized tears, 5 large-sized tear, and 2 massive tears, and in group B, there were 4 small-sized tears, 8 medium-sized tears, 15 large-sized tears, and 6 massive tears (Table 1).
Patient Demographics

Surgical Indications
Tenodesis was performed when bicipital groove tenderness was clearly noted in a preoperative physical examination along with anterior shoulder pain and a partial or almost complete tear of the biceps tendon was confirmed arthroscopically. The surgical technique was chosen based on patient factors, such as age, activity, and concern about cosmetic deformity, and lesion factors, such as rotator cuff tear type. Open subpectoral biceps tenodesis was performed in patients who were young and active and in patients who were very concerned about cosmetic deformity, regardless of rotator cuff size. Arthroscopic intracuff biceps tenodesis was performed in older patients who were not very active and who had large to massive rotator cuff tears as well as in patients who were not very concerned about cosmetic deformity, even when the tear was small to medium in size.
Operative Techniques
All procedures were performed in a beach chair position with the back flexed to 70°. Standard arthroscopic portals for rotator cuff repair were established. Glenohumeral joint evaluation was performed using the standard posterior viewing portals. Details of the intra-articular injuries, such as the degree of rotator cuff tear and lesions of the biceps tendon, were evaluated. Before rotator cuff repair, the biceps was tenotomized from the superior labrum at its origin on the supraglenoid tubercle using an electrocautery device (Arthrocare).
Open Subpectoral Biceps Tenodesis
After arthroscopic rotator cuff repair, an approximately 3-cm longitudinal incision was made at the superior border of the axilla, and the inferior border of the pectoralis major muscle was identified through the incision. A blunt dissection was performed under the pectoralis major muscle and it was retracted laterally. The biceps tendon was identified in the anterior aspect of the humerus and retracted medially, exposing the bicipital groove. A tenodesis site was identified as far proximal on the humerus as possible remaining in line with the normal biceps position. We visually confirmed adequate tension and length during flexion and extension of the elbow. Once the fixation site was exposed, a hole was bored using a 4.0-mm pinecone burr up to the intramedullary canal, followed by insertion of a 5.0-mm Super Revo suture anchor (Linvatec). After positioning the medially retracted biceps tendon at the original site, it was fixed with 3 strands of Hi-Fi suture (Linvatec) using the Mason-Allen stitch technique while maintaining the original length and tension of the biceps. After fixation, the tenotomized tendon from the superior labrum was pulled downward and was cut just above the fixation site (Figure 1).

Open subpectoral tenodesis technique at the superior border of the axilla. The pectoralis major muscle was retracted laterally. A tenodesis site was identified as far proximal on the humerus as possible while remaining in line with the normal biceps position.
Arthroscopic Intracuff Biceps Tenodesis
An 18-gauge spinal needle was passed just lateral to the anterolateral border of the acromion, with assurance that the needle pierced the rotator cuff first and then subsequently passed through the tenotomized biceps tendon. After the needle was placed in a satisfactory position on the tenotomized biceps, No. 1 PDS suture (Ethicon) was passed through the spinal needle and the needle was withdrawn. Then 2-0 Ethibond (Ethicon) was shuttle-relayed on the PDS. With the first loop of Ethibond in place, the 18-gauge spinal needle was passed through the rotator cuff and the tenotomized biceps in such a way that it passed the biceps tendon at a distance of 1 cm from the previously passed Ethibond. The No. 1 PDS suture was passed through the spinal needle, and the needle was pulled out, with the PDS suture kept in place outside the biceps tendon. From the anterior working portal, the PDS and Ethibond were pulled out and shuttle-relayed again so that the free end of the Ethibond suture passed through the biceps tendon and was pulled out from the anterolateral corner of the acromion, which ensured that the Ethibond suture passed twice through the biceps. With the first Ethibond suture loop under the biceps, a second Ethibond suture loop was similarly prepared. The 2 Ethibond suture loops under the biceps were then tied over the rotator cuff, thereby bringing the LHBT into contact with the undersurface of the articular portion of the rotator cuff and ensuring that intracuff tenodesis was achieved. Following this procedure, the rotator cuff tear was repaired (Figures 2 and 3).
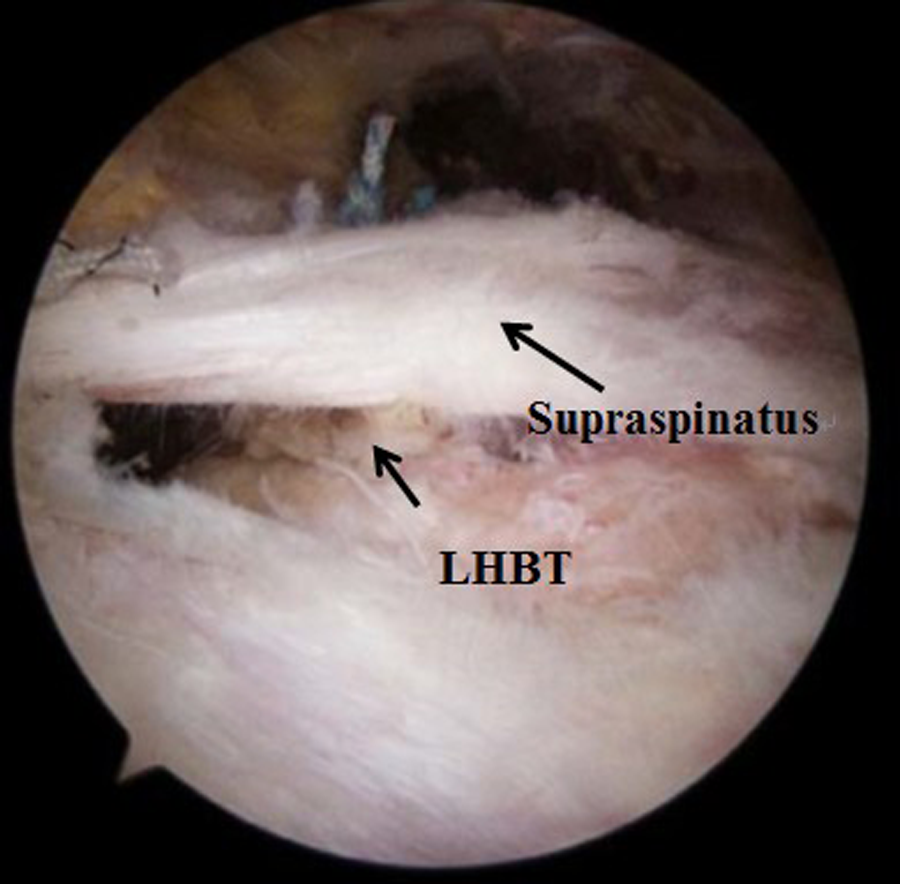
Arthroscopic subacromial view of intracuff tenodesis after tying over the rotator cuff. Two Ethibond loops were placed under the biceps and tied over the rotator cuff. LHBT, long head of biceps tendon.

Tenotomized biceps tendon was sutured under the rotator cuff, thereby making the long head of the biceps tendon come into contact with the undersurface of the articular portion of the rotator cuff. Reproduced with permission from Cho et al. 3
Postoperative Rehabilitation
All patients followed a standard postoperative rehabilitation program. On the first postoperative day, the patients started passive range of motion (ROM) exercises, including pendulum exercises, passive forward flexion, and external rotation in a tolerable range, and were instructed to perform 10 repetitions 3 times a day. Active exercises were not allowed until 6 weeks postoperatively or until full passive ROM was regained. Active biceps exercise was allowed at 6 weeks postoperatively, and muscle-strengthening exercises were introduced thereafter gradually.
Preoperative and Postoperative Evaluation
All patients underwent physical examination 1 day before operation. Postoperative evaluations were performed at 3, 6, 9, and 12 months and then yearly on an outpatient basis, and the results of the last follow-up were analyzed. Preoperative and postoperative subjective pain at rest and during active shoulder motion were assessed using a visual analog scale (VAS). Quantitative muscle strength of the rotator cuff was assessed using the portable handheld Nottingham Mecmesin Myometer (Mecmesin). Elevation strength was tested with the patient in the seated position with the arm flexed to 90° in the scapular plane. Elbow flexion and supination strength were not routinely measured. External and internal rotation were tested with the shoulder in a neutral position and the elbow in 90° of flexion. For shoulder ROM, active forward flexion, external rotation at the side, internal rotation to the posterior, and abduction were assessed before and after surgery.
Internal rotation to the posterior was measured by vertebral level of the hand. The Constant score 5 and the Shoulder Rating Scale of the University of California at Los Angeles (UCLA) 8 were used for clinical assessment. Additionally, the presence of a grossly evident Popeye sign was recorded as a cosmetic deformity, and persistent tenderness at the bicipital groove after biceps tenodesis was noted.
Statistical Analysis
A paired t test was performed to evaluate the differences between preoperative and postoperative pain, ROM, muscle strength, and clinical scores in groups A and B. The Pearson chi-square test and Fisher exact test were performed to compare cosmetic deformity and persistent bicipital pain between the 2 groups. All statistical analyses were performed using SPSS version 21.0 (IBM). Significance was set at an α level of .05 with 95% confidence intervals.
Results
Pain
In the open subpectoral biceps tenodesis group, the mean VAS score both at rest and during motion improved significantly from 2.35 ± 1.64 (range, 0-7) preoperatively to 0.35 ± 0.62 (range, 0-2) at follow-up (P < .001) and from 4.66 ± 1.88 (range, 2-8) preoperatively to 1.94 ± 1.57 (range, 0-4) at final follow-up (P < .001), respectively. In the intracuff biceps tenodesis group, the mean VAS score both at rest and during motion also decreased significantly from 1.93 ± 2.01 (range, 0-7) preoperatively to 0.21 ± 0.48 (range, 0-3) at follow-up (P < .001) and from 5.12 ± 2.28 (range, 2-8) preoperatively to 1.78 ± 1.65 (range, 0-6) at follow-up (P < .001), respectively (Tables 2 and 3).
Clinical Outcome of the Open Subpectoral Tenodesis Group a

α Boldfaced P values indicate statistical significance. Abd, abduction; ER, external rotation; ERs, external rotation at the side; FF, forward flexion; IR, internal rotation; IRp, internal rotation to the posterior; N/A, not applicable; T, thoracic vertebra; UCLA, University of California at Los Angeles; VAS, visual analog scale.
Clinical Outcome of the Arthroscopic Intracuff Tenodesis Group a

α Boldfaced P values indicate statistical significance. Abd, abduction; ER, external rotation; ERs, external rotation at the side; FF, forward flexion; IR, internal rotation; IRp, internal rotation to the posterior; N/A, not applicable; T, thoracic vertebra; UCLA, University of California at Los Angeles; VAS, visual analog scale.
Range of Motion
In groups A and B, there were no significant differences in forward flexion (FF), external rotation at the side (Ers), internal rotation to the posterior (IRp), and abduction (Abd) between preoperative evaluation and last follow-up (Tables 2 and 3).
Muscle Strength
The mean muscle strength of the open subpectoral biceps tenodesis group for forward flexion, external rotation, and internal rotation was 5.5, 5.0, and 5.4 kg preoperatively and 5.7, 5.1, and 5.5 kg at the last follow-up (P = .014, P = .350, and P = .166), respectively. The mean preoperative muscle strength of the intracuff biceps tenodesis group was 5.1 kg for forward flexion, 3.8 kg for external rotation, and 4.4 kg for internal rotation; at final follow-up, the muscle strength changed to 5.5, 3.7, and 4.4 kg, respectively (P = .007, P = .627, and P = .605) (Tables 2 and 3).
Clinical Assessment
In the open subpectoral biceps tenodesis group, the mean UCLA score significantly improved from 18.6 ± 2.5 (range, 15-26) preoperatively to 30.5 ± 3.6 (range, 22-35) at the last follow-up (P < .001). Similarly, it improved from 17.5 ± 2.1 (range, 13-24) preoperatively to 31.5 ± 3.1 (range, 21-35) at final follow-up in the arthroscopic intracuff biceps tenodesis group (P < .001). Furthermore, the mean Constant score significantly improved from 64.5 ± 6.8 (range, 43-80) preoperatively to 86.5 ± 5.3 (range, 77-94) at final follow-up in the open subpectoral biceps tenodesis group (P < .001) and from 62.9 ± 8.5 (range, 36-74) preoperatively to 85.9 ± 6.1 (range, 67-98) at final follow-up in the intracuff biceps tenodesis group (P < .001) (Tables 2 and 3).
Cosmetic Deformity
Popeye deformity occurred in 2 patients (5.2%) from the open subpectoral biceps tenodesis group and 5 patients (15.6%) from the arthroscopic intracuff biceps tenodesis group. There was no significant difference in the incidence of cosmetic deformity between the 2 groups (P = .231) (Tables 2 and 3). The 2 patients with Popeye deformity from the open subpectoral biceps tenodesis group did not complain of persistent bicipital pain or functional impairment at final follow-up. However, in 2 of 5 patients with Popeye deformity from the arthroscopic intracuff tenodesis group, the patients complained of persistent tenderness at the bicipital groove (Table 4).
Clinical Outcome of Patients With Persistent Bicipital Tenderness After Tenodesis at Final Follow-up a

a F, female; M, male; N/A, not applicable; UCLA, University of California at Los Angeles; VAS, visual analog scale.
Persistent Bicipital Tenderness
One patient (2.6%) in the open subpectoral biceps tenodesis group and 8 patients (24.2%) in the intracuff biceps tenodesis group had persistent tenderness at the bicipital groove (Tables 2 and 3). There was a significant difference between the 2 groups (P = .009). One patient with persistent bicipital tenderness from the open subpectoral biceps tenodesis group had a normal ROM; however, bicipital tenderness as well as diffuse pain was reported at rest and during motion, and it was accompanied with cervical foraminal stenosis at multiple levels. Among the 9 patients with persistent bicipital tenderness, the mean VAS score at rest and during motion and the mean UCLA and Constant scores at final follow-up were 1.7 ± 1.0, 3.9 ± 1.2, 27.1 ± 3.8, and 79.2 ± 7.3, respectively, which differed from average scores in this study. Therefore, persistent bicipital tenderness was found to have a negative effect on clinical outcome (Table 4).
Discussion
Over the past decade, interest in biceps injury and treatment has increased. LHBT lesions have been reported to be a major source of anterior shoulder pain 9,11,19 and often associated with other shoulder diseases, most commonly rotator cuff lesions. 2,16 Thus, various surgical operative techniques, such as tenotomy and tenodesis, have been attempted for LHBT lesions, along with rotator cuff repair. Many surgeons prefer biceps tenodesis for LHBT lesions as tenotomy has been reported to be associated with postoperative cosmetic deformity and cramping. 2,16,22,24 Vellios et al 27 presented demographic trends in biceps tenodesis across the United States. According to the report, the number of biceps tenodesis procedures increased from 2047 in 2007 to 5832 in 2011. Additionally, Werner et al 28 reported a significant increase in the overall number of biceps tenodesis procedures being performed. Tenodesis can be performed at a suprapectoral site in the bicipital groove, a subpectoral site below the bicipital groove at the pectoralis major tendon, or other positions, such as soft tissue sites. 11,13,29 Historically, many studies have attempted to determine the superior technique among these various tenodesis techniques. 7,11 –15,18,24,26,29,30 However, the optimal surgical technique and appropriate tenodesis site remain controversial.
In 1994, Rodosky et al 21 introduced a simple all-arthroscopic soft tissue technique for LHBT lesions, and Sekiya et al 25 called this technique the percutaneous intra-articular transtendon (PITT) technique. Lopez-Vidriero et al 13 reported that the PITT technique has the benefits of avoiding hardware complications and reducing cost. In their study on 15 fresh-frozen cadavers, the suture anchor and PITT techniques exhibited satisfactory strength, with no statistical difference between the techniques. Some authors have reported that the soft tissue tenodesis technique has the advantages of simplicity and cost effectiveness with minimal technical challenge, and that this technique is particularly useful when combined with other procedures, such as rotator cuff repair. 3,7,18 Moreover, it has been shown to allow for biceps augmentation in rotator cuff repair. 2,4
In our study, both techniques showed significant improvements in the VAS pain, UCLA, and Constant scores at final follow-up compared with preoperatively. Furthermore, although arthroscopic intracuff tenodesis was often performed with large to massive rotator cuff tear repair, the results with arthroscopic intracuff tenodesis were similar to results with open subpectoral biceps tenodesis. However, the incidence of persistent anterior shoulder tenderness was significantly higher with arthroscopic intracuff tenodesis than with open subpectoral biceps tenodesis, and the incidence of Popeye deformity tended to be greater with arthroscopic intracuff tenodesis than with open subpectoral tenodesis. In particular, the mean clinical assessment scores in patients with persistent anterior shoulder tenderness differed from those in the other patients. Therefore, the surgeon must weigh the advantages of intracuff tenodesis with the increased risk of persistent anterior shoulder tenderness.
Recently, arthroscopic suprapectoral tenodesis has become popular as it can be performed more easily than open subpectoral tenodesis. 22,27,28 Studies conducted by groups that support arthroscopic suprapectoral tenodesis have reported that the clinical outcomes did not significantly differ between arthroscopic suprapectoral tenodesis and open subpectoral tenodesis. 11,14,29 Lutton et al 14 presented a series of 17 patients who underwent arthroscopic suprapectoral biceps tenodesis and reported that there were no cosmetic deformities or other complications. Werner et al 29 performed a comparative study between arthroscopic suprapectoral tenodesis (32 procedures) and open subpectoral tenodesis (50 procedures), with a follow-up period of ≥2 years, and reported that there were no significant differences in postoperative clinical assessment scores, ROM, and muscle strength between the 2 treatment methods. Recently, Gombera et al 11 performed a prospective comparative study between all-arthroscopic suprapectoral biceps tenodesis (23 procedures) and open subpectoral biceps tenodesis (23 procedures) and reported that there was no occurrence of Popeye deformity or arm cramping in both groups of patients. Additionally, there were no significant differences in the mean American Shoulder and Elbow Surgeons (ASES) and satisfaction scores as well as incidence of persistent pain between the 2 treatment methods. Furthermore, no complications were noted in patients who underwent all-arthroscopic tenodesis; however, superficial infection and brachial plexopathy were noted in 1 patient each who underwent open subpectoral tenodesis. Nevertheless, concerns about persistent bicipital groove pain after arthroscopic suprapectoral tenodesis remain, owing to the presence of a tendon within the bicipital groove. 1,9,12,16,17,20 Friedman et al 9 reported that synovitis in the LHBT remained if the tendon was fixed to the proximal area, and this caused persistent pain or failure over time. Therefore, some authors have suggested that subpectoral tenodesis was more appropriate than suprapectoral tenodesis. 16,17,20,23 Mazzocca et al 16 presented a series of 41 patients who underwent open subpectoral tenodesis with a mean follow-up of 29 months and reported that the mean ASES score after the procedure was 89. Additionally, no patient had pain in the intertubercular groove. Sanders et al 23 performed a retrospective comparative study between proximal and distal tenodesis sites in 188 patients and reported that the revision rate was higher for proximal arthroscopic tenodesis (45%) than for distal open tenodesis (8%). Nho et al 20 reported pain after subpectoral tenodesis in only 2 of 353 patients (0.57%) at 3 years, and they stated that the low rate of persistent pain might be due to removal of the tendon from within the bicipital groove. Our study also showed that the incidence of persistent bicipital pain was significantly lower with open subpectoral tenodesis than with arthroscopic intracuff tenodesis. Open subpectoral tenodesis has advantages over arthroscopic suprapectoral tenodesis in eliminating the source of persistent pain and providing biomechanical superiority for the reestablishment of the length-to-tension relationship. 15,16,20,30 Additionally, open subpectoral tenodesis has been reported to have a low likelihood of causing neurological injury as its site is far from nerves. 12,26 However, surgeons who prefer the arthroscopic approach state that an additional open procedure is inevitable with open subpectoral tenodesis, leading to a high complication rate. 11,17,30 However, Nho et al 20 reported that 7 of 353 patients (2%) experienced complications after subpectoral biceps tenodesis over a period of 3 years. Of these 7 patients, 2 (0.57%) experienced persistent bicipital pain, 2 (0.57%) experienced Popeye deformity, 1 (0.28%) experienced deep wound infection, 1 (0.28%) experienced musculocutaneous neuropathy, and 1 (0.28%) experienced reflex sympathetic dystrophy. In our study, only persistent bicipital pain and Popeye deformity were noted with subpectoral biceps tenodesis, and the complication rate was relatively low.
The present study had some major limitations. First, the patients were not randomized. Therefore, a direct comparison of the clinical scores was not possible as the surgical indications were not clear, and demographic data and rotator cuff tear size did not match between the 2 treatment groups. Our intracuff tenodesis group tended to be older patients with larger rotator cuff tears. It is possible that the higher incidence of bicipital tenderness in this group could be a result of recurrent cuff pathology that is commonly seen in this population. Second, we cannot definitively distinguish whether the improvement in outcome scores was because of the rotator cuff repair, biceps procedure, or a combination of the two, but our study’s main purpose was comparing outcomes of bicipital groove tenderness and Popeye deformity in 2 different tenodesis techniques. Third, this study had a relatively short mean follow-up period and a small sample size. Further longer term follow-up studies with a larger group of patients are needed. Fourth, this was a retrospective study, and therefore, it had similar limitations of other retrospective studies.
Conclusion
In our study, both open subpectoral tenodesis and arthroscopic intracuff tenodesis with concomitant rotator cuff repair showed improvement in outcome scores for LHBT lesions accompanied by rotator cuff tears. There was no significant difference in the rate of Popeye deformity between the 2 techniques, but the incidence of persistent bicipital tenderness was shown to be significantly lower in the open subpectoral tenodesis group as compared with the arthroscopic intracuff tenodesis group. This result provided clinical evidence for the concern that bicipital pain may persist due to potential lesions in the distal bicipital groove. Therefore, open subpectoral tenodesis may be more appropriate for LHBT lesions accompanied by rotator cuff tears, considering the lower incidence of persistent bicipital tenderness with this procedure.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.