
Abstract
Background:
Rotator cuff tearing has been found to be clinically associated with other tendinopathies and compression neuropathies; a significant excess of these phenotypes has been seen in patients with rotator cuff tears. It is unclear if the association is secondary to environmental or genetic influences.
Purpose:
To examine population-based data for comorbid association of rotator cuff tearing and tendinopathies and compression neuropathies and to determine whether the association extends to relatives of patients with rotator cuff tears, which could suggest a genetic contribution.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The Utah Population Database (UPDB) contains health and genealogical data on over 2 million Utah residents. Current Procedural Terminology, Fourth Revision, codes (CPT 4) and International Classification of Diseases, Ninth Revision, codes (ICD-9) entered in patient records were used to identify patients with rotator cuff tearing and with comorbid tendinopathies and compression neuropathies. We tested the hypothesis of excess familial clustering of these other phenotypes with rotator cuff tearing using a well-established method (estimation of relative risks) in the overall study group of rotator cuff patients (N = 1889).
Results:
Significantly elevated risk for elbow, hand/wrist, foot/ankle, knee, and hip tendinopathies, as well as for all tendinopathies and compression neuropathies, was observed in rotator cuff tear cases themselves (P < 2.8e–13), in their spouses (P < .02), and in their first-degree relatives (P < 5.5e–4). A significant excess of elbow (P = .01), foot/ankle (P = .04), and all tendinopathies (P = 3.1e–3) was also observed in second-degree relatives, and a significant excess of compression neuropathies (P = .03) was observed in third-degree relatives.
Conclusion:
The current study shows strong evidence of familial clustering of rotator cuff tearing with other tendinopathies and with compression neuropathy. Observed increased risks in spouses and first-degree relatives supports shared environmental risk factors for rotator cuff tearing, most tendinopathies, and compression neuropathies. Increased risks to third-degree relatives for compression neuropathy suggest an association of these phenotypes that may have a shared genetic etiology.
The etiology of rotator cuff tearing is unclear, although likely multifactorial. Decreased vascularity, mechanical impingement, intrinsic degeneration, trauma, and a genetic predisposition have all been postulated as causative factors associated with the development of rotator cuff tearing. 3,7,14,15,17,20 Rotator cuff disease has been observed in excess in patients with other tendinopathies and compression neuropathies, including lateral epicondylitis, Achilles tendonitis, carpal tunnel syndrome, and de Quervain tenosynovitis. 22,23 Kraushaar and Nirschl 11 described a syndrome in patients with rotator cuff tendonitis with a predisposition to developing tendonitis at several sites, including the lateral epicondylitis, and carpal tunnel syndrome as a result of flexor tendon tenosynovitis. Several epidemiologic studies have reported an association of various tendinopathies and compression neuropathies in occupational work injuries. 16,18 No prior studies have evaluated a potential genetic predisposition for the concomitant development of tendinopathies or compression neuropathies in patients with rotator cuff tearing.
Several authors have investigated the clinical association of rotator cuff tendonitis and other tendinopathies or compression neuropathies. Titchener et al, 23 utilizing a large national health care database, determined a significant association between individuals with rotator cuff disease and Achilles tendonitis, lateral epicondylitis, and carpal tunnel syndrome. The same authors reported an association between lateral epicondylitis and rotator cuff pathology, de Quervain disease, and carpal tunnel syndrome. 22 Limitations of their analysis include a heterogeneous rotator cuff phenotype based on hospital coding. Histologic studies comparing tendon biopsies from patients with rotator cuff tendonitis, lateral epicondylitis, and Achilles tendonitis show remarkable similarities. 6,9 A genetic etiology of global tendon dysfunction could potentially explain these histologic and clinical associations.
The purpose of this study was to examine evidence for association of rotator cuff tearing and other tendinopathies and compression neuropathies in rotator cuff tear cases and their close and more distant relatives to identify evidence for a genetic contribution to the disease association. Identification of a genetic predisposition for global tendon dysfunction and compression neuropathies would support the use of preventative measures, including work modification and rehabilitation in individuals at risk for the development of these diseases. We tested the hypothesis of excess risk for global tendinopathies or compression neuropathies in patients with rotator cuff tearing and their relatives using a well-established method: estimation of relative risks (RRs). Our hypothesis is that patients with rotator cuff tears are at greater risk to have associated tendinopathies and compression neuropathies as well as their family members compared with a control population without a diagnosis of rotator cuff tearing.
Methods
The Utah Population Database (UPDB) includes genealogical data for over 2 million Utah founders and their descendants; some family records extend back 15 generations. 19 The original Utah genealogy data came from 3 generation family group sheets with a couple, parents of each member of the couple, and all of their children. Since the early 1970s, genealogy data have been added in the form of trios from state vital statistics data (eg, mother, father, and child from a birth certificate). This has resulted in individual genealogy data of varying quality and quantity. We identified all individuals with genealogy data whose genealogy data included both parents, all 4 grandparents, and at least 6 of their 8 great-grandparents (12 of their 14 immediate ancestors) who also had linked medical data for this analysis.
The University of Utah Health Sciences Center (UUHSC) data warehouse is an electronic database including all patient-related information from inpatient hospital and outpatient clinic visits since 1994. The UUHSC data has been linked to the UPDB genealogical data to allow identification of patients with a phenotype of interest and study of the genetic relationships between affected individuals. The majority of recognized genetic relationships occur in the same generation (eg, siblings, cousins) due to the small window of view to phenotype data.
Methods for the analysis of the UPDB genealogical and linked hospital data have been well reported and represent examination of a number of different phenotypes. 2,21,25 We estimated relative risks for tendinopathies and for compression neuropathies in rotator cuff tear cases, their spouses, and in their first-, second-, and third-degree relatives in the UPDB who also had UUHSC data to test for an association between these phenotypes.
Disease Rates
To estimate RRs for these disease associations, it is necessary to calculate the rates of rotator cuff tearing and other tendinopathies and compression neuropathies. We estimate these disease rates from all hospital patients who have linked genealogical data (approximately 400,000 patients). An attempt is made to record-link all patients at the University of Utah Hospital and Clinics to the genealogical data in the UPDB each year. All individuals in the UPDB with UUHSC data and at least 12 of their 14 immediate ancestors also in the UPDB were assigned to 1 of 205 cohorts. These cohorts are based on sex, 5-year birth year range, birth state (Utah or not Utah), and birth county (urban or rural). Cohort-specific rates for each phenotype were calculated using the total number of UUHSC patients in each cohort as the denominator and the number of patients with the phenotype of interest in each cohort as the numerator.
Relative Risks in Relatives
The RR for a phenotype of interest among the relatives of patients with rotator cuff tear is estimated as the ratio of the number of cases observed among the relatives to the number of cases expected among the relatives. For example, to estimate the RR of compression neuropathy among the first-degree relatives of individuals with rotator cuff tearing, we compared the number of first-degree relatives of rotator cuff tear patients who were diagnosed with compression neuropathy to the expected number of relatives diagnosed with compression neuropathy. The number of expected cases can be obtained by multiplying the population rate of compression neuropathy times the number of first-degree relatives. Because disease rates can vary by sex and birth year, we perform this calculation stratified by cohort to get a more accurate count of expected number of cases. The number of expected cases of compression neuropathy among first-degree relatives of the patients with rotator cuff tearing was therefore calculated by counting all of the first-degree relatives of the rotator cuff tear patients by cohort (without duplication), multiplying the cohort-specific number of relatives by the cohort-specific rate of compression neuropathy, and then summing over all cohorts. The RR of compression neuropathy among first-degree relatives of patients with rotator cuff tear was then estimated as the ratio of observed cases to expected cases. The significance of the test of the null hypothesis (RR = 1.0) was determined by a Fisher exact test for the 2 × 2 table. Confidence intervals for the RR were estimated as given by Agresti. 1
No patient identifiers were used in this study; all analysis of genetic relationships between affected individuals was nonidentifiable. The study was approved by both the University of Utah Institutional Review Board as well as the oversight body for the UPDB.
Results
Identification of Cases
We required that all patients have a minimum genealogy data set that included at least 12 of their 14 immediate ancestors. The number of such patients with rotator cuff tear identified with various diagnoses and procedure coding is shown in Table 1. Patients are only counted once regardless of how many diagnostic codes for a phenotype of interest were present in their record; all patient counts in Table 1 show the count for the first code encountered in the medical record.
UUHSC Patients With a Diagnosis of Rotator Cuff Surgery or Tear a

a Patients were only counted once regardless of how many rotator diagnosis codes were present in their record. All patient counts show the count for the first ICD-9 or CPT-4 code encountered in the medical record. CPT-4, Current Procedural Terminology, Fourth Revision; ICD-9, International Classification of Diseases, Ninth Revision; UUHSC, University of Utah Health Sciences Center.
We used the International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes and the Current Procedural Terminology, Fourth Revision (CPT-4) procedure codes to identify all patients at the UUHSC with a diagnosis of rotator cuff tearing or rotator cuff repair surgery (Table 1). We identified 1889 patients with rotator cuff repair surgery or tear by the presence of CPT-4 codes (29827, 23410, 23412, or 23420) or ICD-9 codes (727.61 or 840.4). The tendinopathy diagnoses and compression neuropathies analyzed were identified using ICD-9 and CPT-4 codes as shown in Table 2.
Codes Included for Tendon Dysfunction and Compression Neuropathy and Phenotypes. a
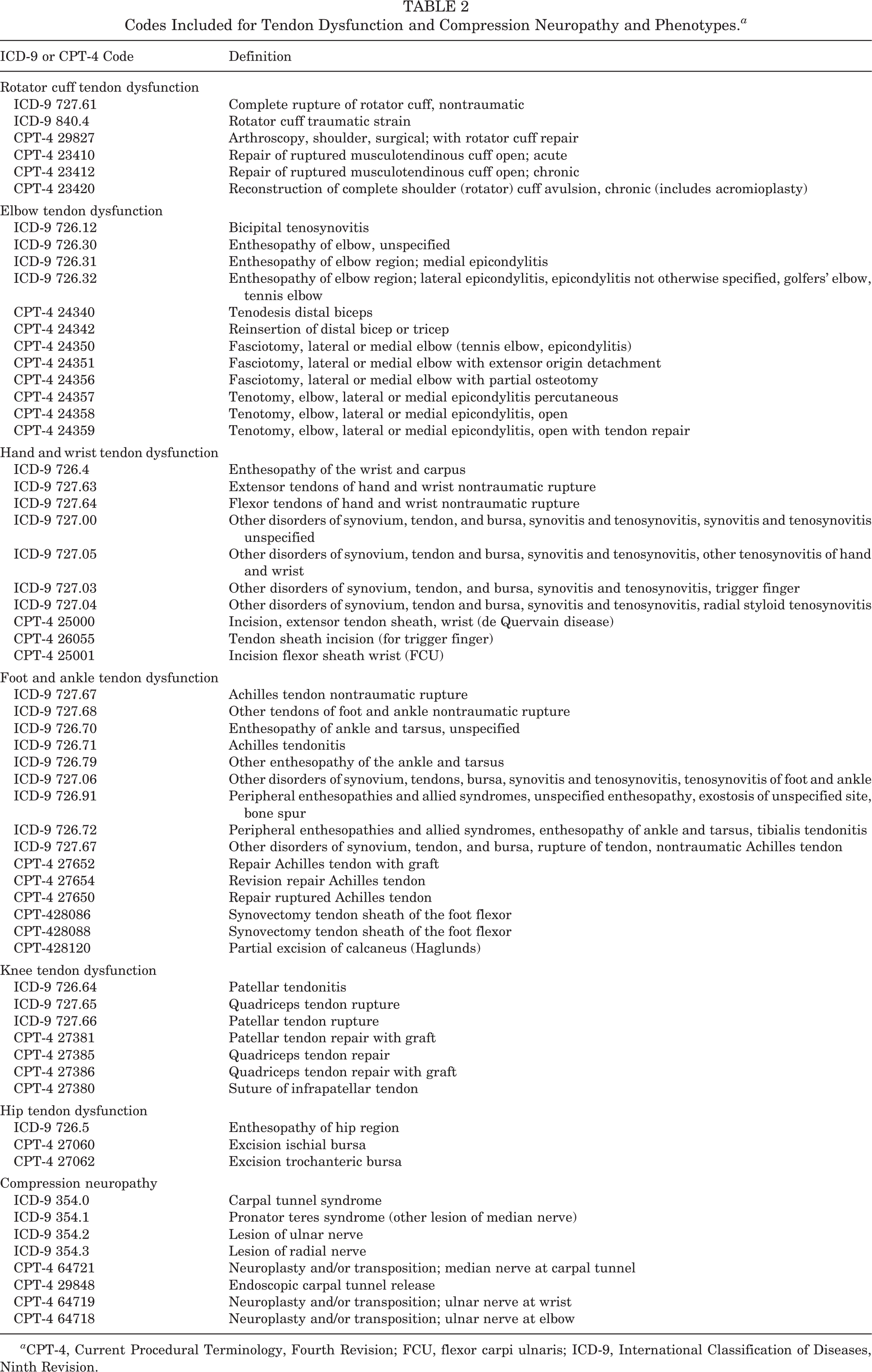
a CPT-4, Current Procedural Terminology, Fourth Revision; FCU, flexor carpi ulnaris; ICD-9, International Classification of Diseases, Ninth Revision.
We estimated RRs for all of the tendinopathy or neuropathy diagnoses shown in Table 2 for the rotator cuff tear cases; their first-, second-, and third-degree relatives; and all of their spouses. The estimated RRs are shown in Table 3, which includes the number of cases (or relatives or spouses, respectively), the observed number of relatives with the diagnosis, the expected number of relatives, the significance of the hypothesis test for RR = 1.0 (P), the estimated relative risk (RR), and the 2-tailed 95% confidence interval for the RR.
Estimated Relative Risks for Associated Disorders in Rotator Cuff Tear Patients; Their First-, Second-, and Third-Degree Relatives; and Their Spouses a
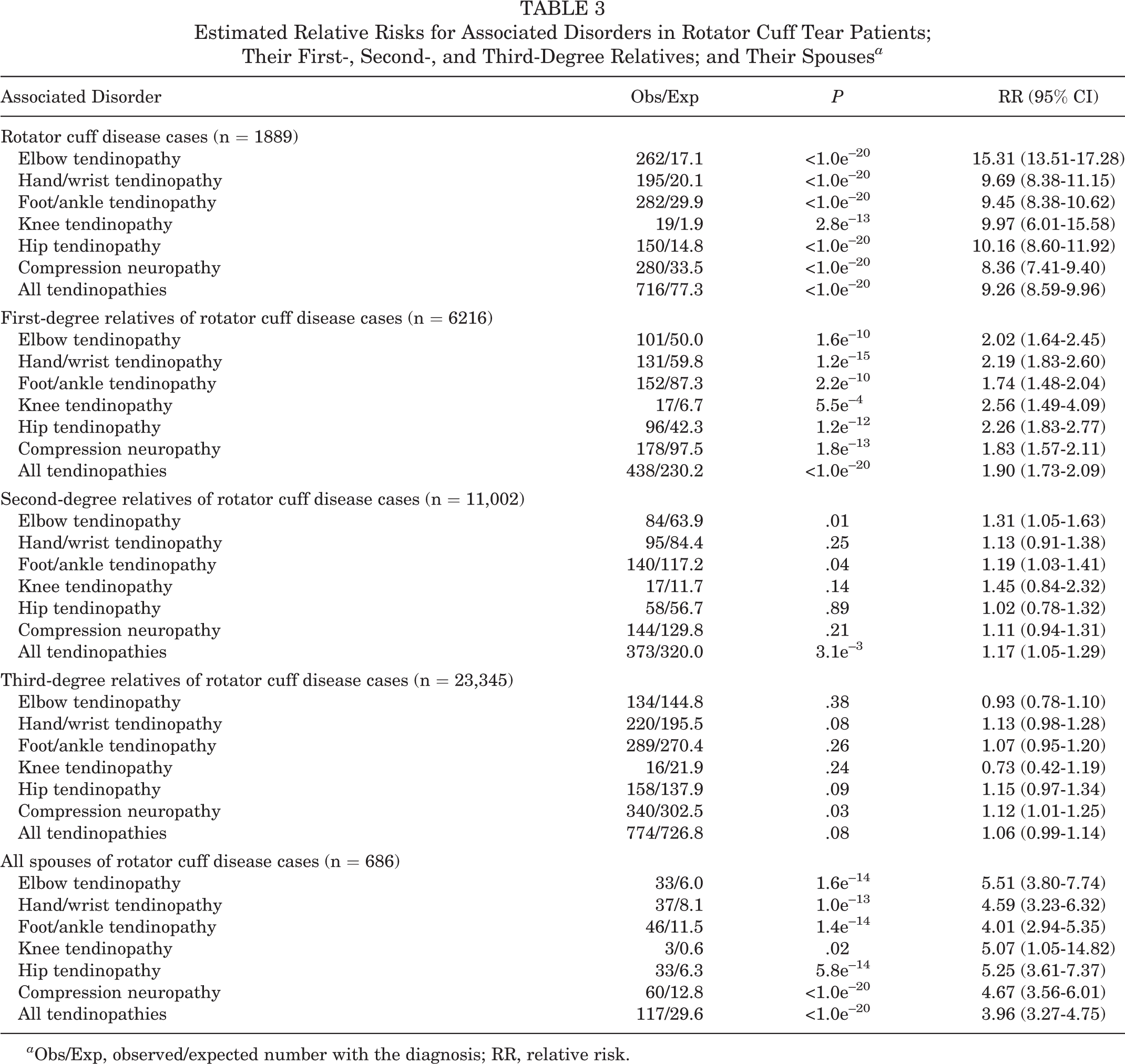
a Obs/Exp, observed/expected number with the diagnosis; RR, relative risk.
Significantly elevated risk for elbow, hand/wrist, foot/ankle, knee, and hip tendinopathies; all tendinopathies; and for compression neuropathies was observed in rotator cuff tear cases themselves (P < 2.8e–13), in their spouses (P < .02), and in their first-degree relatives (P < 5.5e–4) (Table 3). These results suggest shared environmental and behavioral risk factors. However, significantly elevated risks for elbow dysfunction (RR = 1.31), foot and ankle dysfunction (RR = 1.19), all tendinopathies in second-degree relatives (RR = 1.17), and significantly elevated risk for compression neuropathy in third-degree relatives (RR = 1.12) suggest the presence of a genetic contribution to these disorders.
Discussion
Prior data support a significant genetic predisposition for individuals with rotator cuff tearing to have family members with rotator cuff tearing. 20 Rotator cuff tearing has been associated with other tendinopathies including lateral epicondylitis, Achilles tendonitis, and compression neuropathies. 22,23 It is unclear whether this association is due to environmental or genetic effects. 22,23 The current data strongly support an environmental component as well as a genetic component to the development of global tendinopathies and compression neuropathies in patients with rotator cuff tearing. Specifically, spouses of patients with rotator cuff tearing were at a greater risk for developing all tendinopathies and compression neuropathies, suggesting environmental influences. First- and second-degree (for the all tendinopathy group) and first-, second-, and third-degree relatives (for compression neuropathies) of patients with rotator cuff tearing were at significantly increased risk for the development of these diseases, suggesting a genetic contribution to their etiology.
Overall there are limited data supporting an association between various tendinopathies. Walker-Bone et al 24 attempted to determine the prevalence and interrelation of musculoskeletal disorders of the upper extremity. The authors surveyed 9696 adults of working age in the United Kingdom for the presence of musculoskeletal disorders and found significant overlap of patients with shoulder disorders, lateral and medial epicondylitis, de Quervain disease, and carpal tunnel syndrome. 24 Roquelaure et al 16 identified similar associations between rotator cuff syndrome, lateral epicondylitis, and carpal tunnel syndrome in 2685 French workers. Finally, Titchener et al 23 performed a large case-control study using a large national health care database in the United Kingdom looking for associations of tendinopathies and carpal tunnel syndrome with rotator cuff disease. The authors reported an increased risk for the development of Achilles tendonitis (odds ratio [OR] = 1.78), trigger finger (OR = 1.99), lateral epicondylitis (OR = 1.71), and carpal tunnel syndrome (OR = 1.55) in patients with rotator cuff disease compared with controls. 8 All these studies support an association between tendon dysfunction and compression neuropathies and rotator cuff tearing, although it is unclear whether these are environmental or genetic. Our data support that likely both environmental and genetic effects contribute to the associations.
The methodology utilized in the current study is similar to that previously performed to identify a genetic predisposition for other chronic diseases and cancers. The UPDB combines a computerized genealogy of the Utah pioneers and their descendants with various data, including the Utah Cancer Registry, Utah death certificates, and the University of Utah Hospital and Clinics. 4,19 This resource has been used to define the genetic contribution to many other phenotypes and was the basis of the identification in Utah pedigrees of BRCA1, BRCA2, and p16. 5,10,13 Using this resource and similar methodology, we explored the hypothesis of a genetic contribution to global tendinopathies and compression neuropathies in patients with rotator cuff tearing and have shown a strong genetic predisposition for tear development.
Almost all tendinopathies individually showed an environmental influence, as suggested by significantly elevated relative risks for all diagnoses in spouses. Only all tendinopathies, foot and ankle, and elbow showed an increased relative risk in second-degree relatives, and compression neuropathies showed increased relative risks in third-degree relatives, suggesting a genetic predisposition. A possible reason for the lack of each individual tendinopathy group to show a genetic predisposition includes smaller numbers of patients in each tendon dysfunction group, thereby limiting the analysis. The data still strongly support both environmental and genetic influences on the development of tendon dysfunction and compression neuropathies.
A limitation of this study is the use of diagnostic codes for phenotype assignment. Because diagnosis codes are dependent on the clinician, a diagnosis of rotator cuff tearing, other tendinopathy, or compression neuropathy may be less accurate from a nonorthopaedist compared with that from an orthopaedic specialist. We attempted to limit this bias by limiting identification of patients to diagnoses of specific tendinopathies and compression neuropathies, excluding all codes associated with global joint-related pain, strains, or dysfunction. The use of CPT-4 codes for rotator cuff repair surgery as well as neuroplasty or transposition improves the accuracy of the diagnoses but does not completely eliminate inaccuracy due to incorrect surgical indications. We also recognize there may be inaccurate coding using the specific codes for each tendinopathy or neuropathy, especially by a nonorthopaedist, due to misdiagnosis. We elected to include both the ICD-9 and CPT-4 codes to increase the overall number of patients analyzed, improving the ability to perform a population-based analysis. We recognize that the majority of patients were included based on a clinical diagnosis as opposed to undergoing surgery.
Other limitations include censoring that may have occurred in the data resource. In this analysis, we were able to identify only patients at the University of Utah Hospital and Clinics who were coded with a diagnosis or procedure indicating the presence of rotator cuff disease, other tendon dysfunctions, or compression neuropathy and who also had at least 3 generations of genealogical data. The UUHSC serves 20% of Utah state. Additionally, individuals who were not seen at the UUHSC, who were seen before 1994, or whose data did not appropriately link were also censored. This censoring of data occurs uniformly across the data resource, to relatives of both patients and controls, and has been shown to have no bias on the overall results. Finally, there is a high concentration of patients of the Church of Jesus Christ of the Latter-Day Saints (LDS or Mormon) faith in the region of the country from which the study population is derived. Consequently, there may be cultural or behavioral factors that may influence the prevalence of rotator cuff disease in these patients. Regardless, the Utah population has been shown to be representative of the Northern European regions from which its founders came and to have low to normal inbreeding levels when compared with those in the United States overall. 8,12 Despite these potential limitations, our results still suggest that there is a genetic component to the development of global tendon dysfunction and compression neuropathy in patients with rotator cuff tearing, taking into consideration these potential environmental effects.
Tendinopathies and compression neuropathies likely have multifactorial etiologies including mechanical and environmental influences and have been associated with rotator cuff tearing in many large population-based studies. We have shown a strong environmental influence to the development of these diseases in patients with rotator cuff tears. Identification of causal environmental factors resulting in the development of global tendinopathies and compression neuropathies in these patients will aid in the prevention of these disorders. We have additionally shown a strong genetic predisposition specifically for the development of global tendinopathies and compression neuropathies in patients with rotator cuff tears and their relatives. Future applications of these data include high-risk pedigree studies to identify the predisposition gene(s) responsible for these observations and the analysis of potential candidate genes associated with global tendon dysfunction and compression neuropathies. A better understanding of abnormal genetics for tendinopathies and compression neuropathies may allow for early identification of at-risk individuals as well as the development of potential alternative biologically directed treatment methods.
Conclusion
The current study shows strong evidence of familial clustering of rotator cuff tearing with other tendinopathies and with compression neuropathy. Observed increased risks in spouses and first-degree relatives supports shared environmental risk factors for rotator cuff tearing, most tendinopathies, and compression neuropathies. Increased risks to third-degree relatives for compression neuropathy suggest an association of these phenotypes that may have a shared genetic etiology.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Partial support (greater than $10,000) for all datasets within the Utah Population Database was provided by the University of Utah Huntsman Cancer Institute.