
Abstract
Background:
The frequency of osteochondritis dissecans (OCD), a disorder of the subchondral bone and articular cartilage, is not well described.
Purpose:
To assess the frequency of pediatric OCD lesions that progress to surgery based on sex, joint involvement, and age.
Study Design:
Descriptive epidemiology study.
Methods:
A retrospective chart review (2007-2011) was performed on OCD. Inclusion criteria included OCD of any joint and patients aged 2 to 19 years. Exclusion criteria included traumatic osteochondral fractures or coexistence of non-OCD intra-articular lesions. Differences in progression toward surgery were compared between age groups, sex, and joint location. Logistical regression analysis was performed by sex, age, and ethnicity.
Results:
Overall, 317 patients with a total of 334 OCD lesions were found. The majority of lesions (61.7%) were in the knee, with ankle, elbow, shoulder, and foot lesions representing 25.4%, 12.0%, 0.6%, and 0.3% of all lesions, respectively. The majority of joints needing surgery were in the knee (58.5%), with ankle and elbow lesions representing 22.9% and 18.6% of surgeries performed, respectively. The percentage of all OCD lesions progressing to surgery was 35.3%; surgical progression for knee, ankle, and elbow joints was 33.5%, 31.8%, and 55.0%, respectively. Logistic regression analysis found no statistically significant different risk of progressing to surgery for OCD of the knee, elbow, and ankle between sexes. Patients aged 12 to 19 years had a 7.4-times greater risk of progression to surgery for knee OCD lesions than 6- to 11-year-olds. Patients aged 12 to 19 years were 8.2 times more likely to progress to surgery for all OCD lesions than patients aged 6 to 11 years. Progression to surgery of ankle OCD did not significantly differ based on location. Three of 4 trochlear lesions progressed to surgery, along with 1 of 1 tibial, 1 of 3 patellar, 40.3% of lateral femoral condylar, and 28.2% of medial femoral condylar lesions.
Conclusion:
In this large cohort study of pediatric OCD patients, 35% progressed to surgery. Progression to surgery did not differ significantly between sexes with OCD of any joint. Progression to surgery for OCD of the knee, elbow, and ankle strongly correlated with patient age at the time of diagnosis.
Clinical Relevance:
The knowledge of likelihood of progression to surgery of OCD by location, sex, and age is useful in counseling patients and in planning treatment. This study confirms a worse prognosis in the nonoperative treatment of older patients with OCD.
Surgical intervention for osteochondritis dissecans (OCD) has long been recognized as an important aspect of the treatment algorithm. 17,38,40 While conservative (nonoperative) treatment is often utilized for early stage or stable lesions, lesions that fail to heal, appear unstable by magnetic resonance imaging (MRI), or coincide with the presence of loose bodies may require surgical intervention. Despite many years of interest regarding the diagnosis and treatment of OCD, the literature is sparse regarding the actual need for surgical intervention. Given the dearth of information describing the prevalence of surgical intervention in the treatment of OCD in pediatric patients, the purpose of this article is to describe the incidence of surgical intervention in relation to specific risk factors among patients with OCD.
Methods
After institutional review board approval was obtained, a retrospective chart review of all patients diagnosed with OCD was performed between 2007 and 2011. Inclusion criteria included OCD of any joint and patients aged 2 to 19 years at the time of diagnosis. Exclusion criteria included traumatic osteochondral fractures, less than 1 year of follow-up, and the coexistence of any intra-articular lesions other than OCD.
As described in prior studies on OCD of the ankle and knee, 25,26 age at diagnosis, sex, race and ethnicity, joint involvement, side involved, and specific location within the joint were included as variables. Specific locations in the knee included the medial femoral condyle (MFC), lateral femoral condyle, patella, trochlea, and the lateral or medial tibial plateau; in the ankle, we included medial talus, lateral talus, central talus, and distal tibia; last, the sites in the elbow included the trochlea and capitellum. Age for each patient was obtained from the electronic medical record and was categorized as 2 to 5, 6 to 11, or 12 to 19 years. Progression to surgery was noted and the surgical technique recorded for each patient. The decision to perform surgery as well as the selection of surgical technique was made on an individual basis by the surgeon who was treating the patient. Differences in progression to surgery were compared between different age groups, sexes, and joint locations.
Chi-square analysis was done to determine differences by both age group and sex. The associations between progression to surgery and race/ethnicity, age, and sex were assessed using multivariable logistic regression models to estimate odds ratios (ORs) and 95% CIs. The model was adjusted for race (non-Hispanic white, Hispanic, black, Asian or Pacific Islander, other/unknown), age, and sex. Possible interactions between age, sex, ethnicity, and progression to surgery were examined using this multivariate logistic regression analysis. An alpha level of 0.05 was used to determine statistical significance, and SAS Enterprise Guide version 4.2 (SAS Institute) was used for all analyses.
Results
Overall, 317 patients with a total of 334 OCD lesions were identified (Table 1). The breakdown of the 317 patients was as follows: 192 patients (60.6%) had knee lesions, 85 patients (26.8%) had ankle lesions, 37 patients (11.7%) had elbow lesions, 2 patients (0.6%) had shoulder lesions, and 1 patient (0.3%) had a lesion of the foot. Of the 334 OCD lesions, 206 lesions (61.7%) were in the knee, 85 lesions (25.4%) were in the ankle, 40 lesions (12.0%) were in the elbow, 2 lesions (0.6%) were in the shoulder, and 1 lesion (0.3%) was in the foot (Table 2). The analysis of surgical progression revealed that 118 OCD lesions went on to surgery (35.3%). This included 69 of 206 knee OCD lesions (33.8%), 27 of 85 ankle lesions (31.8%), 22 of 40 elbow lesions (55.0%), and no surgeries in the 2 shoulder and 1 foot lesions.
Demographics of Subjects Included in the OCD Surgery Model a
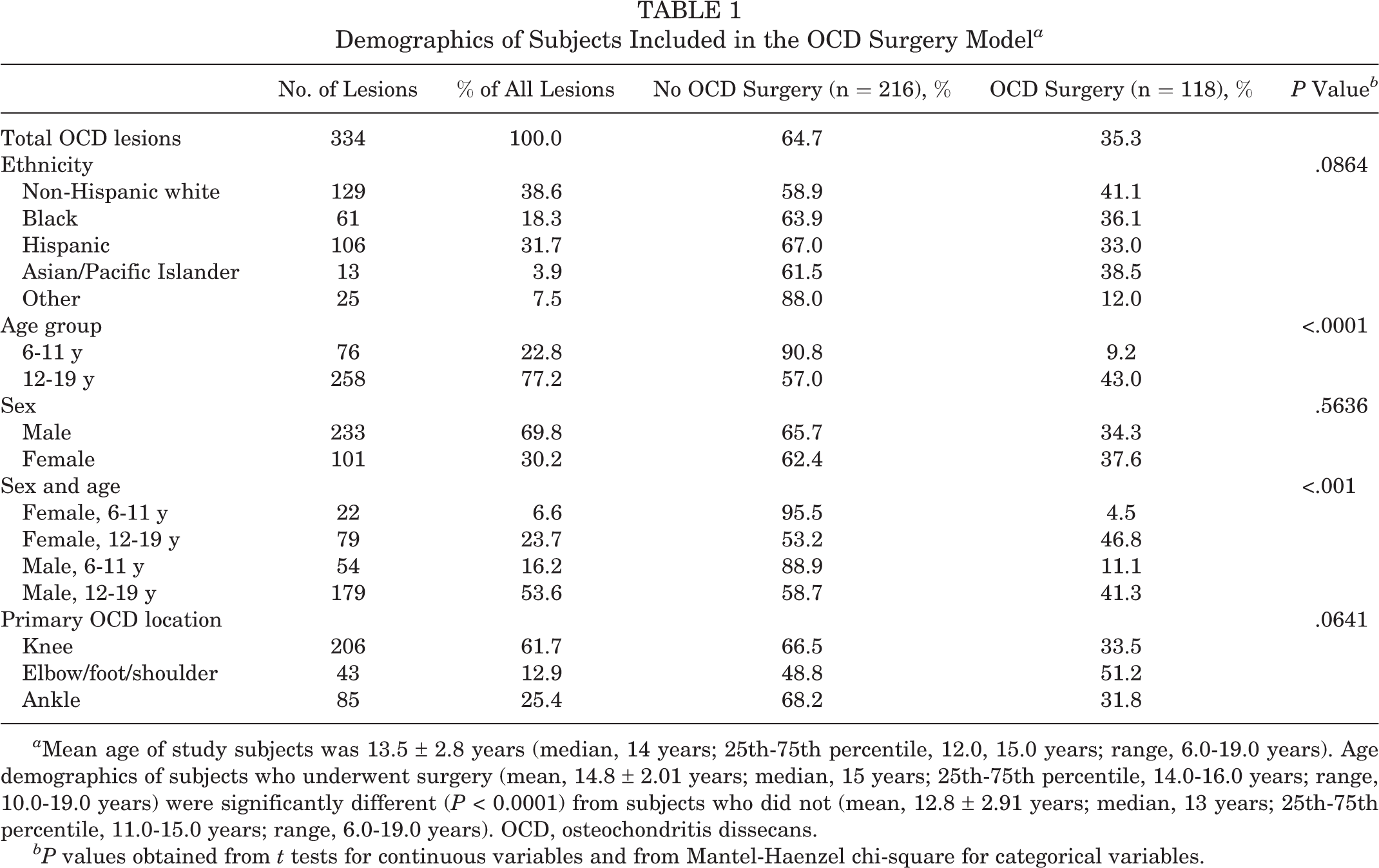
a Mean age of study subjects was 13.5 ± 2.8 years (median, 14 years; 25th-75th percentile, 12.0, 15.0 years; range, 6.0-19.0 years). Age demographics of subjects who underwent surgery (mean, 14.8 ± 2.01 years; median, 15 years; 25th-75th percentile, 14.0-16.0 years; range, 10.0-19.0 years) were significantly different (P < 0.0001) from subjects who did not (mean, 12.8 ± 2.91 years; median, 13 years; 25th-75th percentile, 11.0-15.0 years; range, 6.0-19.0 years). OCD, osteochondritis dissecans.
bP values obtained from t tests for continuous variables and from Mantel-Haenzel chi-square for categorical variables.
OCD Surgery by Joint and Age Category a

a OCD, osteochondritis dissecans.
bP values obtained from t tests for continuous variables and from Mantel-Haenzel chi-square for categorical variables.
In the breakdown by both age and joint, in patients aged 12 to 19 years, surgeries were performed for 147 OCD lesions of the knee (42.9%), 26 surgeries were performed on 72 OCD lesions of the ankle (36.1%), and 22 surgeries for 37 OCD lesions of the elbow (59.5%) (Table 2). Thus, 43% of patients in this age group failed nonoperative treatment and progressed to surgery. In patients aged 6 to 11 years, 6 surgeries were performed out of 59 OCD lesions of the knee (10.2%), 1 surgery was performed out of 13 OCD lesions of the ankle (7.7%), and no surgeries were performed out of 3 OCD lesions of the elbow. The overall progression to surgery for this younger age group was 9.2%, which was significantly lower than the progression to surgery among the older patients (P < .0001). Surgical progression in the knee, elbow, and ankle were also significantly higher in each individual group among the older patients than the younger patients, all with P < .0001.
In terms of the breakdown by joint location, progression to surgery for knee OCD was as follows: In the MFC, 37 surgeries were performed out of 131 lesions (28.2%), while in the lateral femoral condyle, 27 surgeries were performed out of 67 lesions (40.3%) (Table 3). Three of 4 femoral trochlear lesions went on to surgery. Surgery was performed on the single OCD lesion of the lateral tibial plateau. One surgery was performed out of the 3 patellar OCD lesions. For the knee as a whole, right-sided lesions failed conservative treatment 29.4% of the time and left-sided lesions 38.9% of the time.
OCD Lesion Location and Progression to Surgery a

a n/a, not applicable ; OCD, osteochondritis dissecans.
b Fisher exact test.
In the ankle, medial and lateral talar lesions required surgery in 20 of 61 (32.8%) and 6 of 19 (31.6%) lesions, respectively, while central talar lesions and tibial plafond lesions failed conservative treatment in 1 of 3 and 0 of 2 lesions (Table 3). These differences were not statistically significant. In the elbow, 56.4% (22/39) of capitellar lesions progressed to surgery, while the single humeral trochlear lesion did not progress to surgery. No surgeries were performed for the 2 OCD lesions in the shoulder and 1 OCD lesion of the foot (metatarsal head).
In the analysis by sex, no significant differences were seen for any joints (Table 4). In the elbow, 57.6% of males and 42.9% of females failed conservative treatment, while in the knee, progression to surgery was relatively equal at 33.3% and 35.7% for males and females, respectively. For OCD of the ankle, progression to surgery was 38.5% among females and 21.2% among males, which, despite the difference, was not statistically significant (P = .25). In the breakdown by ethnicity, non-Hispanic white patients had the greatest likelihood of progression to surgery (Table 4). White, non-Hispanic patients were more likely to progress to surgery than patients of “other” ethnicity (P = .0092).
Likelihood of Progression to Surgery for All Joints

The types of surgeries performed in this study are summarized in Table 5. For the group as a whole, most patients had only 1 surgery (109/115, 94.8%), while 3 patients each had 2 (2.6%) and 3 surgeries (2.6%). The number of procedures done per surgery varied from 1 (28 patients, 23.7%), 2 (45 patients, 38.1%), 3 (38 patients, 32.2%), and 4 (7 patients, 5.9%). In the multivariable logistic regression analysis, patients aged 12 to 19 years were significantly more likely to progress to surgery than 6- to 11-year-olds for OCD of all locations combined (OR, 8.25; 95% CI, 3.57-19.10; P < .0001) and OCD of the knee only (OR, 7.44; 95% CI, 2.89-19.21; P < .0001). For OCD of the ankle, this older group had an increased risk of surgery, but this risk was just shy of statistical significance (OR, 7.08; 95% CI, 0.85-58.95; P = .07) (Table 4). In terms of sex, males and females were not statistically different in progression to surgery for OCD of any of the individual joints.
Types of Osteochondritis Dissecans Surgery a
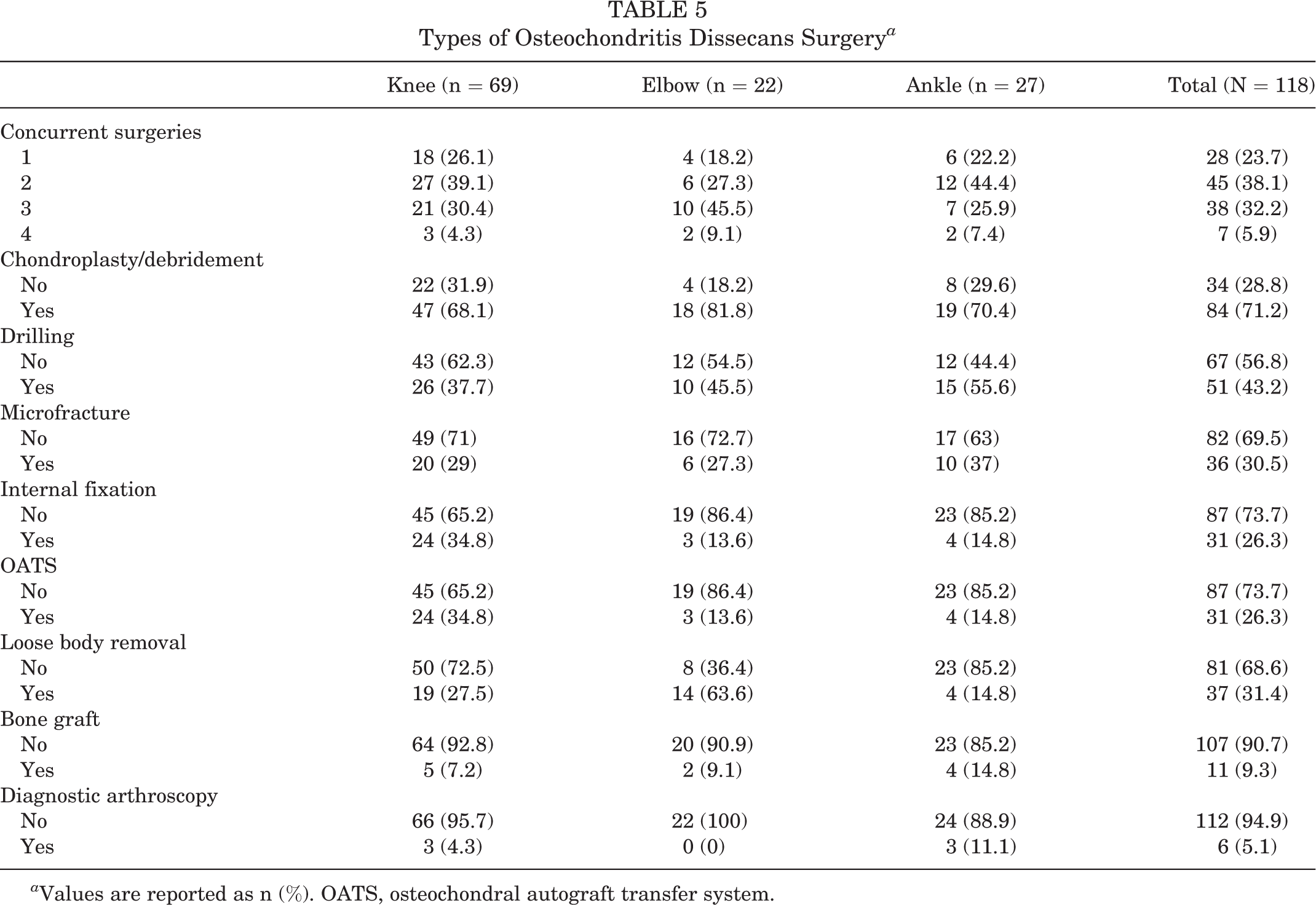
a Values are reported as n (%). OATS, osteochondral autograft transfer system.
Discussion
Progression to surgery for OCD of the knee, elbow, and ankle strongly correlated with patient age at the time of diagnosis. This correlation was found to be statistically significant for each individual joint and also as an overall progression to surgery rate. OCD has long been understood to be a process that may progress to surgical intervention for lesions that do not heal, especially in older patients. There is still incomplete understanding, however, as to what patient factors may correlate with success or failure of conservative management and the frequency of particular procedures. We are unaware of any previous literature that specifically assessed age, race, lesion location, and sex as risk factors for progression to surgery as is done in this study. Prior to this work, the most comprehensive studies on OCD progression to surgery came from Hefti et al 20 and Lefort et al. 31
In 1999, Hefti et al 20 and the European Pediatric Orthopedic Society provided the largest study of pediatric OCD of the knee and progression to surgical intervention. Although this was not a natural history or epidemiologic study in a closed population, it did assess progression to surgery, among other things, in a large multicenter study. Of the 509 affected knees, 154 were treated conservatively and 355 were treated surgically (many with multiple operations). Surgery was more likely when the lesion was sclerosing or “dissected,” if the patient was older with growth plates closing or closed, and if the lesion was anywhere other than the lateral aspect of the MFC. 20
In 2006, Lefort et al 31 studied 892 cases of OCD of the knee in a mixture of adults and children. The authors noted that although prognosis of success with nonoperative treatment was better among the skeletally immature, not all lesions in this age group did well. They based surgical recommendations on stability of the lesion, and suggested that transchondral perforation should be considered early. A number of other studies on smaller numbers of patients have evaluated surgical results in OCD of the knee, ankle, and elbow, with mixtures of adult and pediatric patients. 1,2,4 –8,10
In this study, we found surgical progression in knee OCD—the most common location for OCD—was nearly equal to that of the group as a whole, progressing 33.5% of the time versus 35.3% of the time for the group as a whole. This is a much lower rate of progression to surgery compared with the studies of Backes et al 9 and Hefti et al 20 assessing both conservative and surgical treatment of knee OCD, in which the authors found progression to surgery in the vast majority (74% and 70%, respectively) of patients. However, the study by Hefti et al 20 included both adults and children and did not specifically assess surgical progression by age group. In the present study, surgical progression for all OCD was markedly increased in the teenage group (age 12-19 years) versus 6- to 11-year-olds via logistic regression analysis. This indirectly supports the findings of multiple authors 13,19,20,28,31,33 who found worse clinical results in older children or those with closing physes as compared with children with open physes. In fact, Lefort et al 31 state that “complete cure is frequent before the age of 12 years.” However, none of the aforementioned studies actually assessed or documented a greater progression to surgery in younger OCD patients or those with open physes, and none specifically looked at surgical progression by age group in pediatric patients. Only Jurgensen et al 24 has noted a greater rate of surgery in adult OCD (determined to be OCD with closed physis) as compared with juvenile OCD. While a complete understanding of the factors that predict lesion healing has yet to be elucidated, it has long been noted that patients at or near skeletal maturity show a reduced capacity to heal after fractures or ligamentous injury compared with younger patients. Some of the mechanisms that control healing after traumatic injury may play a role in the healing of OCD lesions as well.
Patient sex was not found to correlate with likelihood of progression to surgery for OCD in any location. Except when comparing white and other (P = .0092), ethnicity did not show statistically significant correlation to progression to surgery. In terms of progression by location in the knee, OCD lesions of the MFC were less likely to progress to surgery (28.2%) than those in the lateral femoral condyle (40.3%). Due to the small sample numbers, statistically significant conclusions could not be reached based on lesions of the trochlea (3 of 4), tibial plateau (1 of 1), and patella (1 of 3) that progressed to surgery. However, our results indirectly support the findings of several authors who, though not necessarily documenting a lower rate of surgery in MFC lesions, have noted either a greater rate of healing in MFC lesions 9 or better clinical results in classic MFC lesions in the central or lateral MFC 21 as opposed to lesions elsewhere in the knee.
In the assessment of procedures performed in the knee, the majority of the surgeries involved chondroplasty/debridement (68.1%), with drilling in 37.1% of lesions. This is somewhat similar to the largest study done on OCD of the knee by Hefti et al, 20 who found drilling and chondroplasty (“operative resurfacing”) were also the most common procedures in 355 patients treated surgically. However, in this study, drilling was actually the most common of these 2 procedures performed (67% of patients). More than 1 type of procedure was performed in the vast majority (76%) of surgeries in the present study. This underscores the need for further well-designed study of surgical intervention for OCD of the knee, as recommended by the AAOS (American Academy of Orthopaedic Surgeons) study group guidelines published in 2011. 15,16 In terms of the need for revision or second surgeries, our study demonstrated that only 5% of patients with any type of OCD required 2 or more surgeries. In comparison, Pascual-Garrido et al 39 has shown a 14% rate of revision surgery and Kocher et al 27 showed a 33% rate of second surgeries for OCD of the knee. However, it is possible that with longer follow-up of the present patient cohort, a greater rate of revision surgery could be seen. Unfortunately, due to the retrospective nature of this study, we do not know attrition rates for the patients in this study, making it difficult to draw too many conclusions in terms of revision surgeries.
In terms of ankle OCD, progression to surgery in these 85 children was similar to that of the knee at 31.8%. The literature is quite variable regarding progression to surgery for ankle OCD, with a surgical intervention rate between 19% and 58% in multiple studies. 11,21,32 Looking specifically at children, Letts et al 32 found a surgical intervention in only 1 of 5 in children under the age of 12 years, Higuera et al 21 found a 33% surgical intervention rate in their study of pediatric ankle OCD, and the 20-year follow-up study by Bauer et al 11 on ankle OCD in a mixture of children and adults found that only 1 of 5 children had surgery. As with knee OCD, surgical progression for ankle OCD did not significantly differ based on either sex and, in contrast to knee OCD, location within the ankle did not seem to correlate with nonoperative treatment failure. Similar to knee OCD, the majority of procedures were chondroplasty/debridement (70.4%), and more than 1 type of procedure was performed in the vast majority of surgeries (78%). The variability and multiplicity of procedures performed for ankle OCD is reflective of the literature. Zwingmann et al 46 performed a systematic review of 54 studies and 1105 patients and concluded that in terms of recommended procedures for ankle OCD, “with over 1100 included patients in the present study, no strong recommendations based upon scientific evidence can be given.” Our study confirms that the surgical choice to address OCD of the ankle remains variable.
The literature is sparse regarding surgical progression of OCD of the elbow. The vast majority of studies on surgery for OCD of the elbow simply assess results of surgery in all patients # rather than assessing all results, both surgical and nonsurgical, in patients with elbow OCD. Takahara et al, 45 in a study of 106 adults and children with elbow OCD, found that 66% of patients failed conservative treatment and went on to have surgery. Similarly, in our cohort, just over half of the elbow lesions progressed to surgery. Likelihood of progression to surgery was slightly greater among males (57.6%) compared with females (42.9%), but this was not statistically significant. Similar to the recommendations of multiple authors, 12,14,23,30,35,36,41,42 a large number of surgeries performed in our series to treat OCD of the elbow were marrow stimulation techniques, including chondroplasty/debridement (81.8%), drillings (45.5%), and microfracture (27.3%). As opposed to OCD of the ankle and knee, loose body removal was also frequently performed (63.6%). This also is well described in the literature. 3,23,45 Surgery may be required more often in the treatment of OCD of the elbow due to presentation of the lesions in older patients at a higher, less stable grade. It may be that stable OCD in the skeletally mature population is less symptomatic and therefore less recognized, but proof of this is beyond the scope of this particular project and is an excellent future research question.
There are a number of weaknesses of the present study. First, it is retrospective in nature. As such, challenges exist in interpreting the data, and improper coding could have introduced selection bias. In addition, there is no uniformity in the treatment algorithms of the many physicians involved in the care of these patients, both in terms of the indications for surgery and the types of surgeries performed. It also does not elucidate any relationship between the types of surgeries performed and the intraoperative and radiographic findings. Last of all, the present study does not specifically address the success of surgery, although 95% of patients did not require any further surgery after follow-up of at least 2 years. Despite the study weaknesses, it does provide new information regarding the patient factors associated with progression to surgery and is based on a large patient population with a consistent electronic medical record.
Conclusion
This review of surgical intervention for pediatric OCD is one of the largest to date. This study confirms the markedly increased likelihood of progression to surgery among older patients for OCD as a whole and knee OCD specifically and confirms the findings of many prior studies that in each type of OCD, chondroplasty or debridement is the most common procedure performed. It also demonstrates that approximately one-third of pediatric patients with OCD as a whole and of the ankle and knee specifically progress to surgery, with a higher progression in elbow OCD patients. In terms of specific location within each joint, it also confirms that MFC lesions of the knee have a greater likelihood of nonoperative treatment success. The knowledge of likelihood of progression to surgery of OCD by location, sex, and age is useful in counseling patients and in planning treatment. In addition, this work provides a benchmark with which to compare treatment and intervention, with the goal of decreasing the need for surgical intervention in the future for this pathology.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.