
Abstract
Background:
Landings in fatigue conditions are considered to be one of the factors that cause noncontact anterior cruciate ligament (ACL) injury. Additionally, it is known that fatigue alters lower extremity landing strategies and decreases the ability to attenuate shock during landing.
Purpose:
To determine characteristics of knee kinematics and shock attenuation during the landing phase of a single-leg vertical drop jump in a fatigued condition. The hypothesis was that knee kinematics during the landing phase of a single-leg vertical drop jump would demonstrate a significant difference between before and after fatigue.
Study Design:
Controlled laboratory study.
Methods:
Thirty-four college females participated in this experiment. They were randomly assigned to either the fatigue (n = 17) or control group (n = 17). The fatigue group performed the single-leg vertical drop jump before and after the fatigue protocol, which was performed on a bike ergometer. Knee kinematics data were obtained from the 3-dimensional motion analysis system. The ratio of each variable (%) was calculated, comparing the pre- to postfatigue protocol. Unpaired t tests were used to compare changes in kinematic variables between the fatigue-induced group and control group.
Results:
Peak knee flexion angular velocity increased significantly in the fatigue group (106.1% ± 8.0%) in comparison with the control group (100.7% ± 6.6%) (P < .05). However, peak knee flexion angle and acceleration had no differences between each group. Peak knee adduction/abduction angle, velocity, and acceleration also had no differences between each group.
Conclusion:
Fatigue decreased the ability to attenuate shock by increasing angular velocity in the direction of knee flexion during single-leg drop jump landing. These findings indicate the need to evaluate the ability to attenuate shock by measuring knee flexion angular velocity when fatigue is considered.
Clinical Relevance:
Measuring knee angular velocity during landings might be an important evaluation parameter in the consideration of the knee injury prevention.
The anterior cruciate ligament (ACL) is frequently injured during basketball, soccer, and many other sporting activities. In recent studies examining ACL injury, the mechanism of injury is widely considered to involve biomechanical factors 10,34 as the majority of injuries involve little or no contact with other players. 20,28 In those studies, it was reported that up to approximately 70% of all ACL injuries occurred in noncontact situations while only approximately 30% of ACL injuries occurred with contact. 1,4,19 For these reasons, ACL injury prevention programs have been widely incorporated into a variety of different sporting activities. 13,14,26,27,29,32 Based on a range of biomechanical studies, landing from a jump and other movements with rapid deceleration have been reported as 2 major causes of noncontact ACL injury. 1,4,28 These studies have identified a number of risk factors for ACL injury, including increased knee abduction and internal rotation angle and decreased trunk flexion angle. 14,22,23
It has been shown that some injuries, such as noncontact ACL injury, have a greater risk of occurring in the final period of a game or at the end of a practice session, indicating fatigue may be a component of the problem. 11,12,30 Altered movement patterns as a result of fatigue may explain noncontact ACL injuries and other injuries during sporting activities. Indeed, fatigue has been indicated as one of the main causative factors for lower extremity injury in recent years. 7,22,25 Similarly, altered movement patterns under fatigue conditions decrease the ability of the lower extremity to attenuate shock and cause a lack of stability during landing. 17,21,24,36
Recent reports have suggested that altered lower extremity kinematics during landing might increase ACL injuries. 2,22,24,28,36 However, knee flexion, abduction kinematics, and shock attenuation in the knee joint during the landing phase during fatigue conditions have not been previously investigated. The purpose of this study was to investigate characteristics of knee kinematics and shock attenuation by comparing these variables between fatigued and nonfatigued conditions during the landing phase of a single vertical drop jump. The hypothesis was that knee kinematics during the landing phase of a single vertical drop jump would demonstrate significant difference between fatigued and nonfatigued conditions.
Methods
Participants
Thirty-four females (mean age, 20.7 ± 1.8 years; mean height, 159.9 ± 5.6 cm; mean weight, 52.7 ± 5.9 kg) volunteered to participate in this study. For inclusion, participants were required to have no history of orthopaedic hip, knee, and ankle surgery and equal leg length. The dominant foot was the right in 30 subjects and the left in 4 subjects. The dominant foot was determined based on which foot was used to kick a ball. All participants gave written informed consent for participation prior to testing. Participants were randomly assigned to either the fatigue group (n = 17; mean age, 21.2 ± 2.1 years; mean height, 160.5 ± 5.0 cm; mean weight, 52.9 ± 7.1 kg) or the control group (n = 17; mean age, 20.2 ± 1.4 years; mean height, 159.3 ± 6.3 cm; mean weight, 52.6 ± 4.5 kg) by using cards. This study followed the Declaration of Helsinki and was approved by the Ethics Committee at the Saitama Medical University, Saitama, Japan (M-54).
Instrumentation
A 3-dimensional (3D) motion analysis system with 8 cameras (Vicon MX; Vicon Motion Systems) was used to record lower extremity kinematic data during the single-leg vertical drop jump. The sampling rate for kinematic data was set at 240 Hz. Thirty-five reflective markers were placed on specific anatomical landmarks (left and right front heads, left and right back heads, 7th cervical vertebrae, 10th thoracic vertebrae, clavicle, sternum, right back, shoulders, lateral epicondyles of elbow, medial wrists, lateral wrists, second metacarpal heads, anterior superior iliac spines, posterior superior iliac spines, lateral thighs, lateral epicondyles of knee, lateral thigh tibias, lateral malleoli, second metatarsal heads, and heels). The Vicon Plug-in-Gait model was used to drive lower extremity kinematic data. Two force plates (AMTI MSA-6) were used to record ground reaction force during the landing phase of each single-leg vertical drop jump. The sampling rate for ground reaction forces was set at 1200 Hz.
Experimental Procedures
All participants wore closely fitted dark shorts to aid data collection. Each participant performed a single-leg vertical drop jump on her dominant leg. A single-leg vertical drop jump consists of landing after dropping down from a 40-cm box and then landing after a maximal vertical jump rebounding from the drop (Figure 1). All participants were shown the testing sequence by an assistant researcher. Several practice trials were conducted to enable the participants to perform the vertical jumps in the correct fashion. Subsequent trials were repeated until data from 5 successful trials were achieved. Trials were excluded if the participant lost her balance during the landing process.

Single-leg vertical drop jump. The single-leg drop vertical jump consisted of a first landing (B) after dropping down from the starting position (A) and a second landing (D) after a maximal vertical jump rebounding from the drop (C).
After the first series, all participants were required to pedal a bike ergometer (COMBI). Participants in the fatigue group pedaled at 100 W/min for 5 minutes or until they exceeded 17 (very hard) on the Borg scale. 6,37 A poster showing the Borg scale was set in front of a bike ergometer. The level of fatigue on the Borg scale was recorded at 30-second intervals. In contrast, all participants in the control group pedaled a bike ergometer without load (<10 W) for 5 minutes. Fatigue level was also verified by the Borg scale.
After pedaling on the bike, all participants repeated the vertical drop jump task (the second series), following the same procedure as the first series.
Data Collection
The landing phase of the single-leg vertical drop jump was defined as the period from initial ground contact to take-off. The initial ground contact was defined as the point when force plate data indicated that the vertical ground reaction force had reached more than 10 N. Take-off was defined as the point when force plate data indicated that the vertical ground reaction force was less than 10 N. All outcome measures were analyzed with an average of 3 trials for the first and second series. All variables were measured at the first landing phase of first and second series.
Knee flexion and adduction angles, angular velocities, and angular accelerations were analyzed during the first landing phase of each series. Knee flexion and adduction angles were calculated from the filtered 3D coordinate data and were calculated as positive values. Knee flexion and adduction angles were defined on the basis of static anatomical position. To reduce data fluctuation, knee flexion and adduction angular velocities were calculated by differentiating mean knee flexion and adduction angles from 5 frames using a moving average. Knee flexion and adduction angular accelerations were calculated in the same fashion.
Peak knee flexion angle during the first landing phase of the first series was dichotomously categorized into either a large knee flexion subgroup (mean knee flexion angle, 70.1° ± 5.4°; fatigue group, n = 5; control group, n = 8), where subjects had a knee flexion angle above the mean, or a small knee flexion subgroup (mean knee flexion angle, 54.7° ± 6.3°; fatigue group, n = 12; control group, n = 9), where subjects had a knee flexion angle below the mean according to distribution of our results.
Peak knee adduction/abduction angle (adduction in relation to abduction angle) during the first landing phase of the first series was dichotomously categorized into either a peak knee adduction subgroup (mean knee adduction angle, 15.8° ± 7.6°; fatigue group, n = 9; control group, n = 7), where subjects had peak knee adduction angle, or a peak knee abduction subgroup (mean knee abduction angle, 13.1° ± 5.3°; fatigue group, n = 8; control group, n = 10), where subjects had peak knee abduction angle.
Peak knee flexion angle and angular velocity were determined from each maximum value during the first landing phase of each series. Maximum and minimum angular acceleration values, as well as peak knee adduction angular velocity, were determined during the first landing phase of each series. In addition, we calculated the ratio (%) of the first to the second series of each kinematic variable.
The vertical position, velocity, and acceleration of the center of gravity were analyzed during the first landing phase of each series. The vertical position of the center of gravity was calculated from the filtered 3D coordinate data during the first landing phase of each series. To reduce data fluctuation, the vertical velocity of the center of gravity was calculated by differentiating mean vertical position in 5 frames using the moving average method. The vertical acceleration of the center of gravity was also calculated in the same fashion but using the vertical velocity. Minimum vertical position and velocity, which were defined as the lowest position and peak velocity in the ground direction, were determined from each minimum value during the first landing phase of each series. Peak vertical acceleration was determined from the maximum values recorded during the first landing phase of each series. The ratio of the first to the second series for each variable with respect to the center of gravity was calculated.
The total ground contact time (ms) from initial ground contact to take-off and the peak angle time period (ms) were recorded during the first landing phase of each series. The ratio of the first to the second series for the peak angle duration of knee flexion and adduction/abduction to the total ground contact duration was calculated.
Statistical Analysis
All data were analyzed using SPSS version 19.0 (IBM Corp). Unpaired t tests were used to compare changes in kinematic variables between the fatigue group and control group, 2 groups categorized into either a large knee flexion group or a small knee flexion group and 2 groups categorized into either a peak knee adduction group or a peak knee abduction group. Significant differences were set at a level of .05.
Results
Knee flexion angle, angular velocity (Figure 2), and angular acceleration of the fatigue and control groups are shown in Table 1. The ratio of peak knee flexion angular velocity from the first to second series increased significantly in the fatigue group (106.1% ± 8.0%) in comparison with the control group (100.7% ± 6.6%) (P < .05). This indicates that knee flexion angular velocity during landings increased after the fatigue protocol. The knee flexion angle was not altered after the fatigue protocol (fatigue group, 99.5% ± 5.6%; control group, 101.5% ± 5.9%; P > .05). Maximum and minimum knee flexion accelerations were not altered after the fatigue protocol at maximum value (fatigue group, 125.4% ± 40.7%; control group, 92.1% ± 67.1%; P > .05) and minimum value (fatigue group, 113.2% ± 21.9%; control group, 107.0% ± 15.9%; P > .05). Furthermore, comparison of the large knee flexion and small knee flexion subgroups during the first series indicated that there were no differences between the fatigue and control groups in the degree of knee flexion angle, angular velocity, or angular acceleration.

Means and standard deviations of knee flexion (solid lines) and adduction (dotted lines) velocities prior to (black line) and after (gray line) the fatigue protocol. Knee flexion and adduction angular velocities are indicated with positive values, while knee extension and abduction angular velocities are indicated with negative values.
Differences in Knee Flexion Variables Before and After Fatigue a
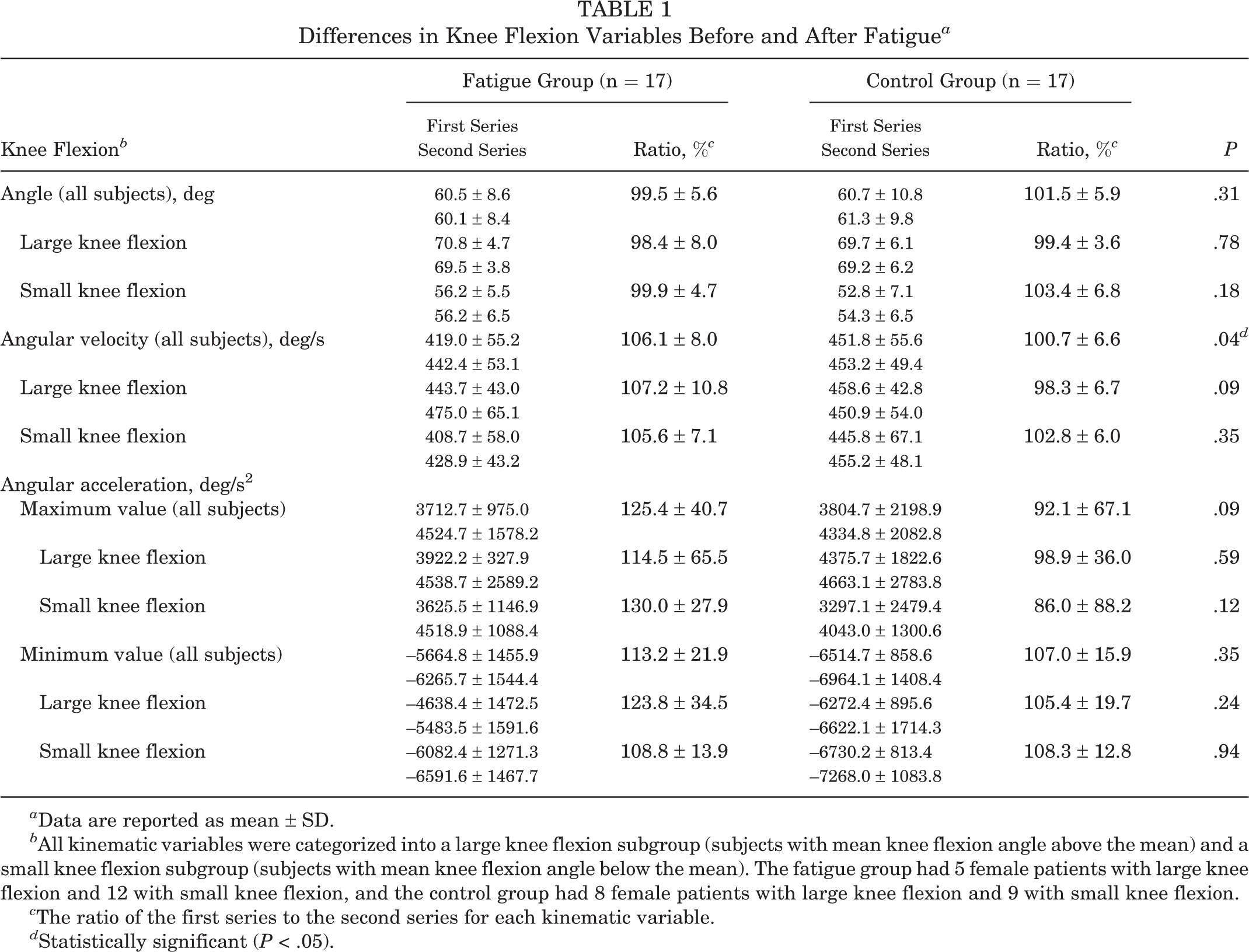
a Data are reported as mean ± SD.
b All kinematic variables were categorized into a large knee flexion subgroup (subjects with mean knee flexion angle above the mean) and a small knee flexion subgroup (subjects with mean knee flexion angle below the mean). The fatigue group had 5 female patients with large knee flexion and 12 with small knee flexion, and the control group had 8 female patients with large knee flexion and 9 with small knee flexion.
c The ratio of the first series to the second series for each kinematic variable.
d Statistically significant (P < .05).
Knee adduction/abduction angles and angular velocities and angular accelerations of the fatigue and control groups are shown. A comparison of the peak knee adduction and peak knee abduction subgroups during the first series indicated that there were no differences between the fatigue and control groups (P > .05).
Vertical position, velocity, and acceleration of the center of gravity of the fatigue group and control group are shown in Table 2. The ratios of each variable from the first to second series were not altered by the fatigue protocol (P > .05).
Differences in the Vertical Component of the Center of Gravity Before and After Fatigue a
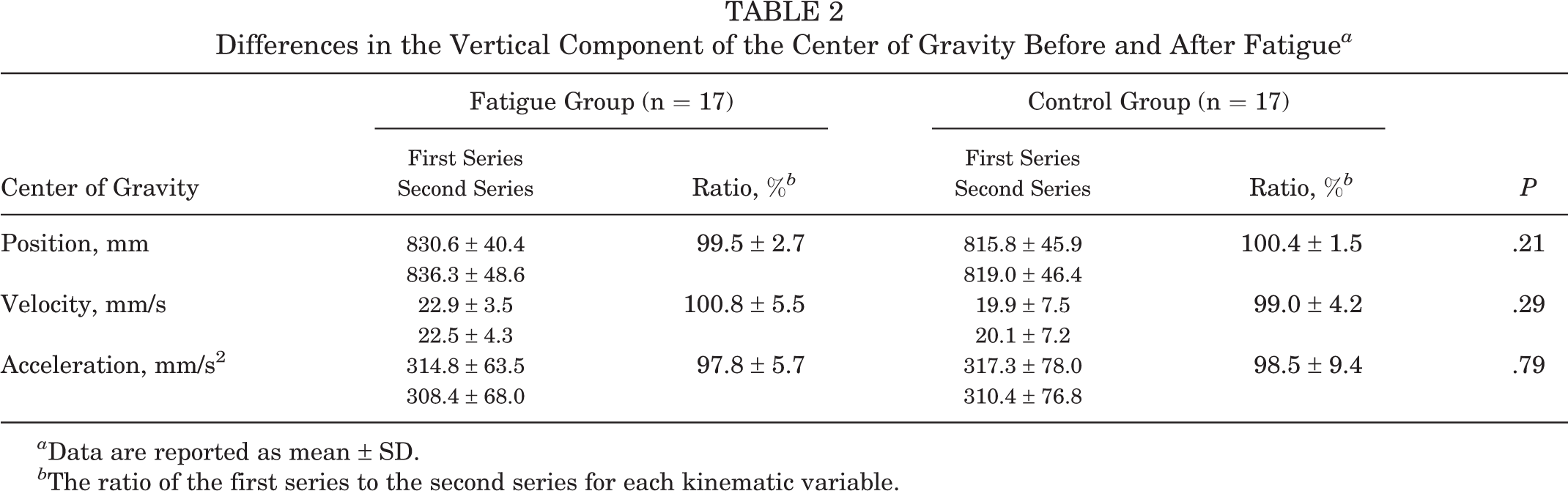
a Data are reported as mean ± SD.
b The ratio of the first series to the second series for each kinematic variable.
The time period (ms) from initial ground contact to peak knee flexion and adduction/abduction angles are shown in Table 3. The ratios of maximum time of peak knee flexion and adduction/abduction to total ground contact time were also calculated. There were no differences in these variables between the fatigue and control groups (P > .05). Even though kinematics such as knee flexion angular velocity and adduction/abduction angular accelerations changed after the fatigue protocol, the time periods from initial ground contact to peak knee flexion and adduction/abduction were unchanged.
Durations and Ratios for Initial Ground Contact to Peak Knee Flexion and Adduction/Abduction Angles a
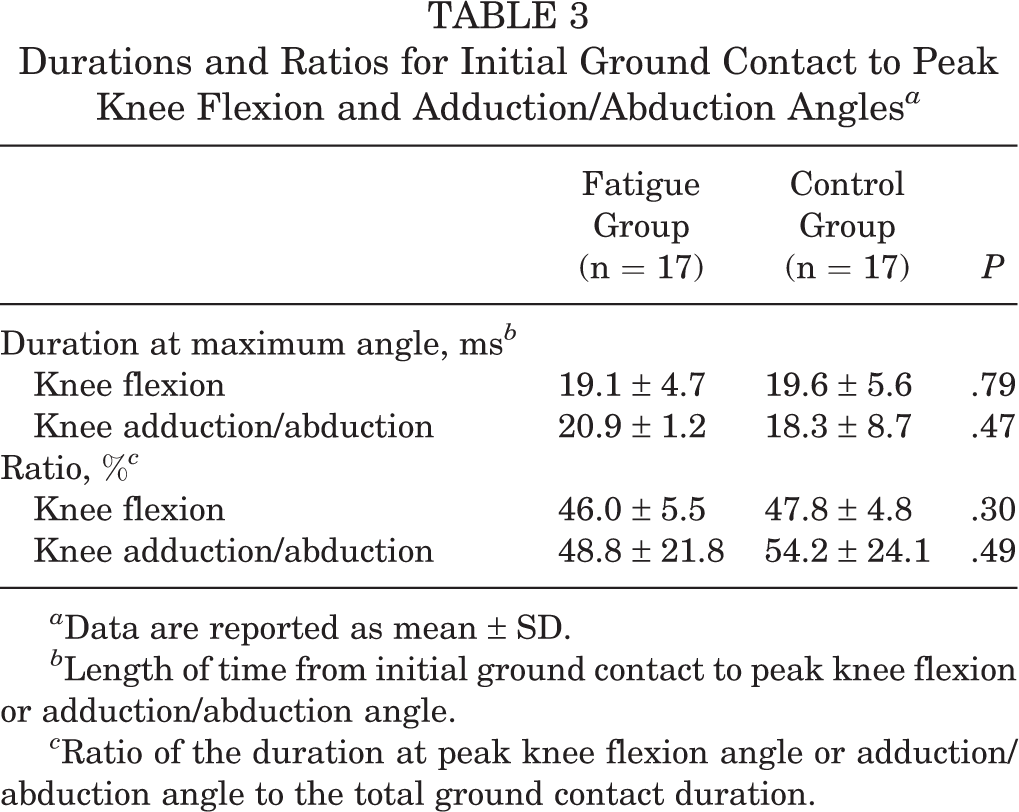
a Data are reported as mean ± SD.
b Length of time from initial ground contact to peak knee flexion or adduction/abduction angle.
c Ratio of the duration at peak knee flexion angle or adduction/abduction angle to the total ground contact duration.
Discussion
With regard to angular velocity, knee flexion angular velocity increased significantly after the fatigue protocol; however, the knee flexion angle was not found to be influenced by fatigue in our study. These results indicate that increased knee flexion angular velocity in the fatigue condition was caused by losing motor control of the direction of knee flexion during the landing phase. The shock experienced by the body during ground contact must be attenuated mostly by the lower extremity structure or kinematics. It is considered that the most of the shock attenuation is achieved by eccentric muscle contraction during landings. Many studies have also suggested that knee kinematics have an important role in attenuating shock during running or jump landings. 8,9,25,35 Additionally, many studies have reported that fatigue causes changes in knee kinematics such as peak knee angle during landings. 3,7,18,22,25 Furthermore, decreasing the capacity for knee joint shock attenuation in the fatigue condition may induce increased risk of acute knee injuries, including those to the ACL. Therefore, some kinematic factors of the knee joint should have been revealed for evaluating the capacity for knee joint shock attenuation. According to our results, kinematic changes to the knee joint induced by fatigue can be evaluated by measuring knee flexion angular velocity as a possible means of the ability of shock attenuation during landings. However, the rate of increased knee flexion angular velocity after fatigue protocol may depend on the level of fatigue or the type of the fatigue protocol. In the future, these assumptions in the degree of the rate of increased knee flexion angular velocity need to be discussed in more detail by changing the level of fatigue or the type of fatigue protocol.
Subjects had no change in knee adduction angular velocity and angular acceleration after fatigue. Furthermore, each subject group that had peak knee adduction or abduction during landing in the no fatigue condition did not show any significant characteristic differences on angular velocity and angular acceleration after fatigue. These results indicate that changes in knee kinematics in the frontal plane after fatigue do not depend on the direction of knee adduction or abduction.
Many studies have reported that peak knee abduction angle significantly increases after fatigue. 18,22 These findings suggest that an increase in knee abduction angle as result of fatigue may be a potential biomechanical factor for knee injury, such as that to the ACL. However, knee kinematics on the frontal plane were found to be unaffected by fatigue in this study. The fatigue protocol of our study involved a motion in the sagittal plane using a bike ergometer. For this reason, fatigue induced by a bike ergometer may be influential in a specific direction and an intermediate range of knee flexion and extension. In previous reports, fatigue protocols including a knee flexion or extension motion such as a parallel squat exercise 18 and landing activity 21 have been used. These reports have shown that only knee flexion and extension variables during landings were altered significantly by fatigue protocols. From these reports, it is suggested that the change of knee flexion and extension variables after fatigue protocols in the sagittal plane may be caused by applying loads to mostly the quadriceps and hamstrings. Additionally, in most sport activity, there is a possibility that fatigue occurs in all ranges of motion, including but not exclusive to intermediate range of knee flexion or extension—such as deep knee flexion during full squatting—or a change in direction. 18,22 Therefore, other fatigue protocols that include these motions may affect the biomechanical parameters in directions of knee adduction or abduction. Further studies are needed to investigate characteristics of these parameters in other fatigue conditions.
In our study, kinematics of the center of gravity and the time period from initial ground contact to maximum knee flexion and adduction/abduction angles were also measured. First, this study showed that fatigue did not affect the vertical position of the center of gravity. A higher position of the center of gravity decreases postural control during quiet standing. 31 Moreover, Sheehan et al 33 reported that the distance from the center of mass to the base of support was larger at the time of ACL injury. From these studies, the higher position of the center of gravity during landing may be one of the risk factors for ACL injury. Additionally, this study showed that the velocity and acceleration of the center of gravity did not change after fatigue. These findings indicate that kinematic changes may have been isolated to the knee joint and were not widespread, such as affecting the kinematics of the center of gravity. Second, the time period from initial ground contact to peak knee flexion and adduction/abduction also did not change after fatigue. These parameters are relevant to performance ability such as quick movements. These results indicate that changes in knee kinematics such as increasing knee velocity after fatigue occurred without decreasing agility. Despite these results, kinematics of the hip and other joints was not investigated in this study. It is important to evaluate this in future studies because some kinematic analysis studies indicate that alignment of the hip or trunk during ground contact is one of the biomechanical factors for ACL injury. 4,5,15,16,28
Our study shows that fatigue decreased the ability to attenuate shock by increasing angular velocity in the direction of knee flexion during single-leg jump landing. Additionally, kinematic changes to the center of gravity and the time period of maximum knee angles to the total ground contact duration were unaffected by fatigue. The results might indicate the need to evaluate the quality of movement over time by measuring knee flexion angular velocity when fatigue or other risk factors for knee injury are considered. Our results indicate that we may need to pay attention to the knee flexion angular velocity during single-leg jump landings, which might be missed if we only observe specific times, such as time from initial ground contact to peak knee angle, by visual feedback or video analysis.
There are several potential limitations of our study. First, a bike ergometer was used in the fatigue protocol. The knee movement in a bike ergometer is mainly in directions of knee flexion and extension. For this reason, fatigue induced by a bike ergometer may influence predominantly knee flexion or extension during the landing phase. Second, the fatigue protocol of our study was performed for only 5 minutes by using a bike ergometer and the degree of fatigue was verified by the Borg scale, which is a scale better used to measure exertion than fatigue. Therefore, landing trials of our study were not performed under fatigue conditions that duplicate the fatigue in sporting activities in which the ACL is injured. Finally, the outcome measure of our study was knee kinematics. Several kinematic analysis studies have reported that the alignment of the hip or trunk during the landing phase is one of the biomechanical factors for ACL injury. 5,15 We should take this into account when evaluating other biomechanical variables in the fatigue condition in future research.
Conclusion
The shock experienced by the body during landings must be attenuated by knee kinematics. Additionally, fatigue may alter some knee kinematics and decrease the ability of shock attenuation in the knee joint. After the fatigue protocol of our study, knee flexion angular velocity increased significantly; however, the knee flexion angle and acceleration were not influenced in the fatigue condition. Knee adduction/abduction kinematics were not influenced by the fatigue protocol of our study. From these results, it was indicated that fatigue decreased the ability to attenuate shock by increasing angular velocity in the direction of knee flexion during single-leg jump landings.
Footnotes
Acknowledgment
The authors thank Dr Toby Hall, who contributed to proofreading as a native English speaker and gave critical advice for this article.
The authors declared that they had no conflicts of interest in the authorship and publication of this contribution.