
Abstract

Historically, arthroscopic anterior cruciate ligament (ACL) reconstruction has a low rate of infection, with a reported prevalence of 0.14% to 5.7%. 12,14,21 While uncommon, these infections generally occur early and are characterized by either cellulitis at the graft insertion site and/or septic arthritis. 5 Subacute infections are less well characterized.
Although bioabsorbable interference screws have the potential advantages of osseointegration, limited postoperative imaging artifact, and decreased hardware removal rates, the potential for acting as the nidus for a sterile abscess, which can both mimic and/or set the stage for infection, exists. 2 Typically, distinguishing a sterile abscess from infection is clinically apparent. However, we describe 2 patients with subacute postsurgical medial tibial pain in which this distinction was not evident. Application of a novel culture protocol taken from the prosthetic joint infection literature 6 identified infection by a low-virulence organism and directed therapeutic treatment.
Cases
Initial Presentation and Treatment
A 25-year-old male pedestrian (patient 1) was struck by an automobile and sustained an isolated right knee ACL tear. A 54-year-old woman (patient 2) sustained a right knee ACL tear while dancing. Both patients underwent arthroscopic ACL reconstruction performed by the same surgeon using an identical transtibial technique with suspense fixation (Endobutton; Smith & Nephew) and tibial fixation using the bioabsorbable Bio-INTRAFIX (DePuy Mitek) system. The bioabsorbable implant was composed of a proprietary combination of polylactic acid and tricalcium phosphate. Tibialis anterior allograft (Community Tissue Services) was used in both cases. The procedures were uncomplicated and were followed by routine rehabilitation and uneventful recovery with unrestricted activity at 6 months.
Patient 1
Eight months postoperatively, patient 1 developed new onset erythema and swelling around the tibial incision (2 × 2 cm) with a central eschar and associated tenderness. He had no fever, effusion at the knee, or systemic signs of infection. Radiographs (Figure 1) and magnetic resonance images (Figure 2, A and B) were obtained. The presence of diffuse hyperintense signal within the proximal tibia (Figure 2), in contrast with soft tissue edema, and minimal signal in the uninfected proximal tibia (Figure 3, A and B) suggested the presence of infection, and the infectious disease (ID) service was consulted. Recommended blood tests were obtained, and results were within normal limits (Table 1).

No significant abnormalities were seen on anteroposterior knee radiographs in patient 1. The interference screw is apparent, without significant bone resorption.
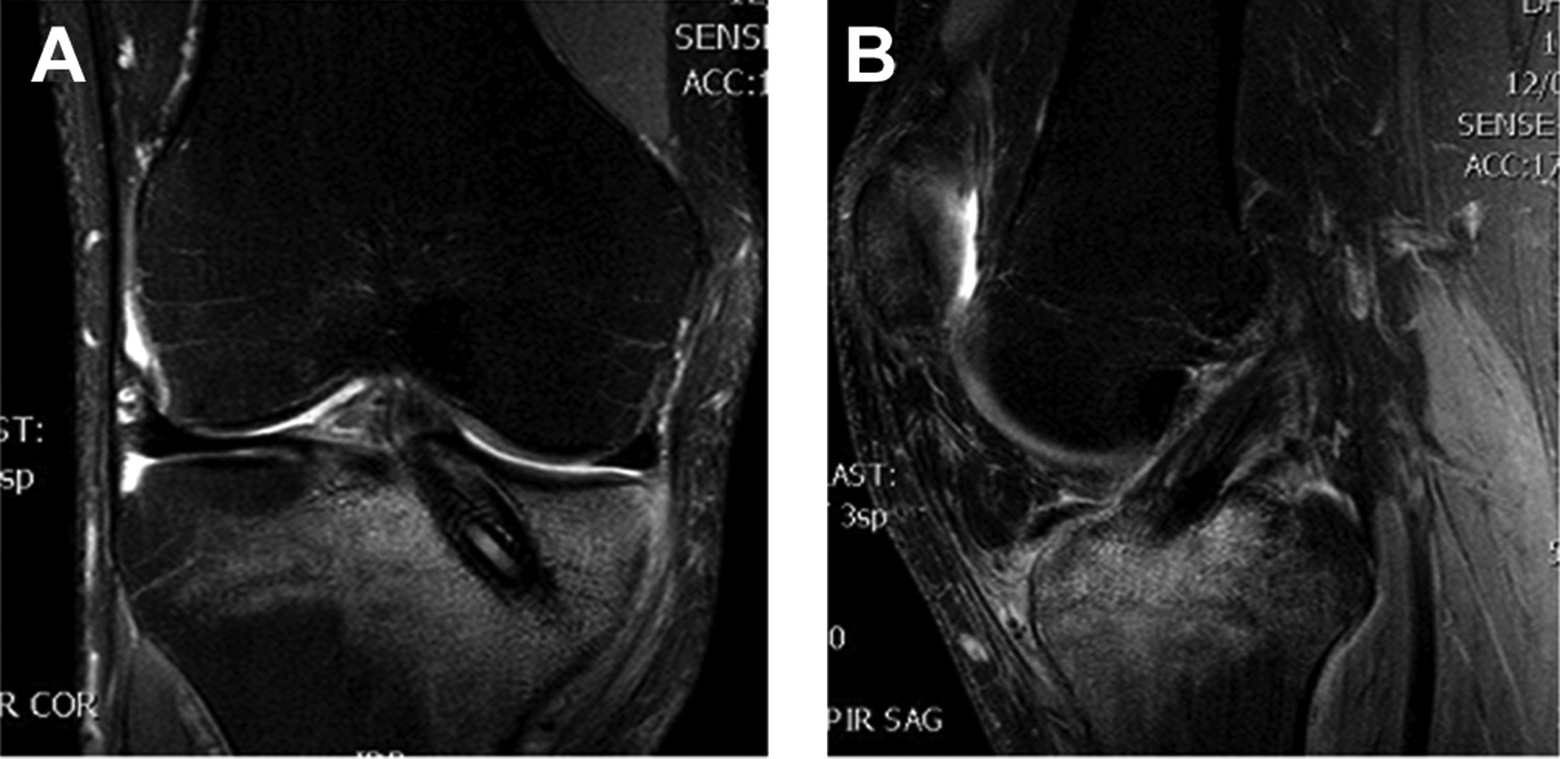
(A) Coronal and (B) sagittal plane T2-weighted magnetic resonance images for patient 1 indicating subtle changes adjacent to the interference screw and presenting an extensive hyperintense signal within the proximal tibia adjacent to the implant.
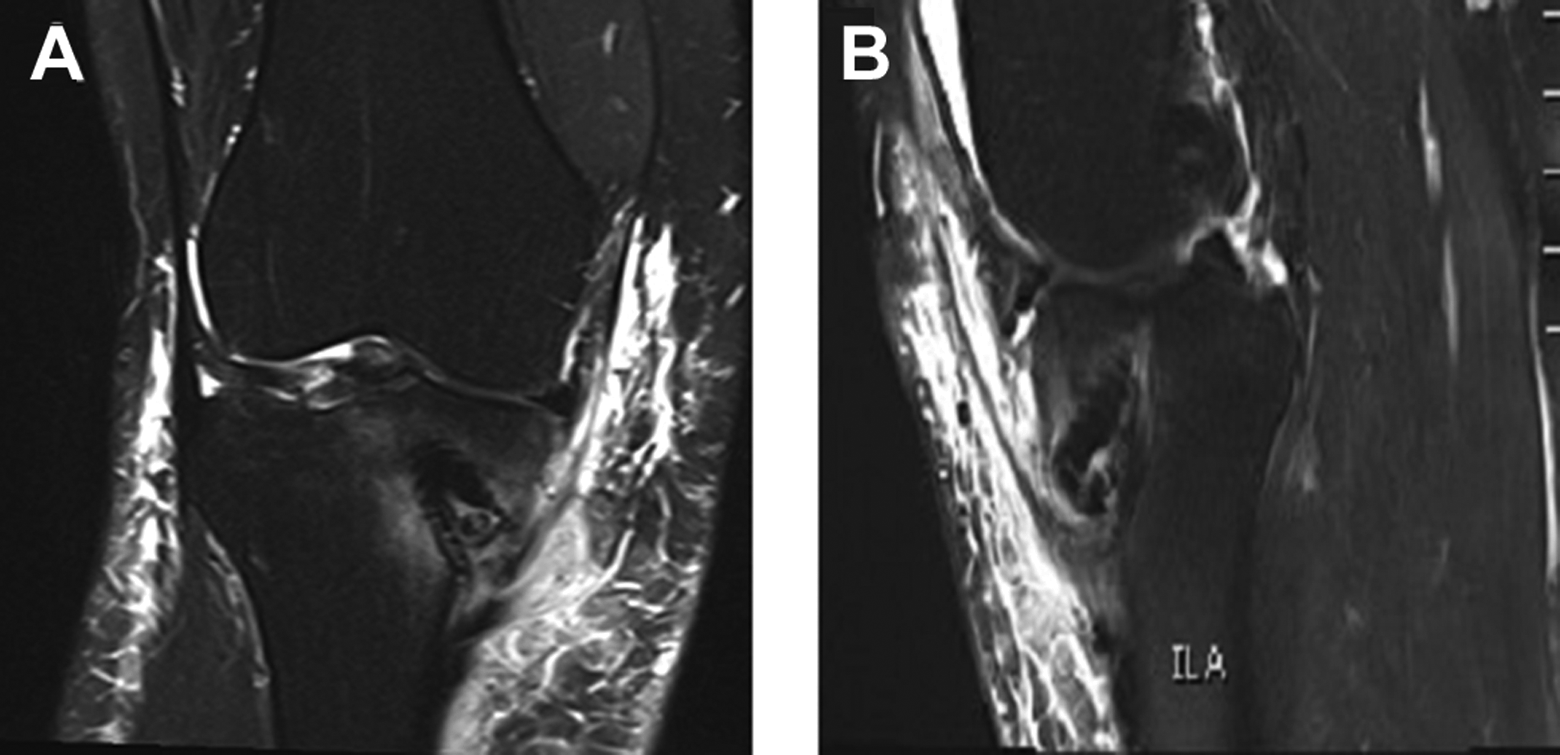
Example of (A) coronal and (B) sagittal plane T2-weighted magnetic resonance images that exhibit a fragmented distal screw in association with soft tissue edema and minimal hyperintense signal in the proximal tibia.
Presurgical Laboratory Blood Test Results a

a BASO, basophil count; EOS, eosinophil count; ESR, erythrocyte sedimentation rate; WBC, white blood cell count.
Surgical debridement of the tibial tunnel and interference screw removal proceeded within 1 week. At surgery, healthy bleeding tissue was found with no evidence of purulence or necrosis. The intact interference screw was removed in 1 piece with its surrounding sheath adjacent to minimal serous-appearing fluid. The graft was healed to bone, and no evidence of intra-articular extension of fluid or infection was apparent. Multiple cultures and pathology specimens were taken from the adjacent granulation tissue using our standard orthopaedic biopsy protocol (Oregon Health and Science University), which is an institution-wide tissue culture protocol specifically developed to improve detection of occult infections in association with orthopaedic implants. 6 This protocol dictates obtaining a minimum of 5 tissue specimens (from the region of greatest suspicion) to be sent for culture. Each specimen is taken with a separate clean instrument; no swabs are used. An additional specimen is sent for surgical pathology analysis. Each microbiology specimen is separately incubated on blood agar and chocolate media plates aerobically and anaerobically for 5 days (conventional incubation) and in thioglycolate broth anaerobically for 10 days. The 10-day incubation is to allow for growth of fastidious organisms such as Propionibacterium species. After completion of this protocol and manual debridement, the tissue was irrigated with 10 L of lactated ringers before skin closure.
The pathology specimen for patient 1 was negative for inflammatory cells on Gram stain and histopathological examination at day 10, but 6 of 6 cultures grew Propionibacterium acnes (P acnes) (Table 2). Of note, only 2 of 6 cultures grew P acnes after 4 days of incubation; it took 6 days for all cultures to become positive with the organism. Thus, with the conventional incubation of 5 days, the diagnosis might have been missed.
Culture Results Indicating Growth of Proprionibacterium acnesa

a No apparent abnormalities were found in blood tests in association with low-virulence P acnes in patient 1 or in association with the sterile abscess in patient 2.
As a therapeutic precaution, patient 1 was started on intravenous vancomycin (1.75 g every 12 hours) after the debridement surgery pending culture results, then switched to intravenous daptomycin (500 mg every 24 hours) due to an adverse reaction (skin redness). The ID consult recommended continued daptomycin treatment for 6 weeks. At 1 week postoperatively, the incision was without drainage, and by 2 weeks, the swelling and erythema resolved. Daptomycin was discontinued and replaced with oral amoxicillin (875 mg every 12 hours) treatment for 2 additional months, and the patient has remained without signs of infection for more than 1 year. Rifampin was not used due to adverse antibiotic side effects for the patient.
Patient 2
Three years postsurgery, patient 2 returned after several months of increased pain at the medial tibia. Examination revealed tenderness at the medial proximal tibia hardware fixation site, but no fever, effusion, or systemic signs of infection. Radiographs suggested a loose interference screw (Figure 4). A single cortisone injection at the time of presentation provided minimal relief, and elective removal of the tibial interference screw was recommended and scheduled.

No significant abnormalities were detected on anteroposterior knee radiographs in patient 2. The interference screw is apparent with potential loosening but without significant bone resorption. Sclerotic changes are consistent with chronic remodeling.
In the 1-month interval prior to removal surgery, the patient presented with a 2-cm fluctuant erythmatous nodule over the healed proximal tibial incision. Concern for an abscess or newly onset infection led to an urgent ID consultation and immediate surgical irrigation and debridement. Laboratory blood tests results were within normal limits (Table 1).
Intraoperative examination of the tibia found the previous incision dehisced, open 1 cm with fibrinous tissue, with some serous drainage but no purulence. The wound was incised, no purulence was found, and the damaged skin was ellipsed. A fragmented interference screw, with 25% of the original unabsorbed volume, was removed. The orthopaedic biopsy protocol was followed, debris was removed, and the tissue was irrigated with 10 L of lactated ringers. In this case, 6 of 6 tissue cultures were negative for growth, and the pathology specimen was negative for acute inflammatory elements (Table 2).
After the procedure, the patient was started on intravenous daptomycin (500 mg every 24 hours) with the option of deescalation, and ceftriaxone (2 g every 24 hours) pending culture results. Despite results inconsistent with an active infection, ID recommended 6 weeks of antibiotic treatment as a cautionary measure. By 11 days postoperative, wounds were closed without signs of infection. Ultimately, treatment included 2 weeks of intravenous daptomycin followed by ceftriaxone for 4 weeks, and transition to oral doxycycline (100 mg every 12 hours) for 4 weeks. This course of antibiotics was shorter than the antibiotic regimen of patient 1. One year after treatment, the patient remains asymptomatic, without signs of infection.
Discussion
The 2 patients discussed in this report exhibited similar subacute postsurgical presentations related to bioabsorbable interference screws. Subtle differences in radiographic, surgical, and histopathological findings suggest that differentiating between a sterile abscess and infection based on clinical presentations alone may require additional specific steps. Clues, including the state of the bioabsorbable screws and, most important, bacterial growth from a proper set of culture specimens held for 10 days, can provide for specific diagnoses and allow tailored treatment for afflicted patients.
Use of bioabsorbable interface screws for graft fixation has become increasingly popular 7 and is generally well tolerated. However, reactions to these implants can occur in the subacute and chronic settings and mimic occult infection. The presentation of pain at the tibial fixation site of the bioabsorbable screws was the common postoperative complaint in these reports. Due to prolonged degradation of these essentially biocompatible materials, adverse effects may not present immediately. 13 In fact, as exhibited by patient 2, hydrolysis of the implant can result in sterile abscess formation that requires debridement and implant removal, which has been reported as late as 3 years after surgery. 2,22 Some studies have reported that the incidence of a tibial reaction to a biointerference screw is 5%, 10,18 and although these cases only mimic infection, they cause discomfort, require additional treatment, and add to the patient’s time away from activity.
Although uncommon, deep infections (osteomyelitis and septic arthritis) after ACL reconstruction represent serious and well-described complications. In such cases, organisms are often highly virulent and generally can be diagnosed clinically, through elevation of erythrocyte sedimentation rate and C-reactive protein, gross purulence at evacuation, and evidence of histopathological inflammation. 12 However, occult infection may present with minimal clinical or laboratory indicators, particularly in cases of low-virulence organisms. Inflammatory markers tested in our 2 patients were within normal limits, there was no evidence of gross purulence, and surgical pathology did not indicate acute inflammation. Such results are representative of a sterile abscess exhibited by patient 2 but were inconsistent with the presence of infection in patient 1. Thus, we suggest more extensive culture procedures in such settings, particularly when diagnosis of P acnes in association with implanted devices is suspected.
Propionibacterium is a common bacterium in surgical wounds and is well described during shoulder and spinal surgery procedures where implants are used. 1,4,8,9,11,16,17,20 Despite its recognition as a shoulder arthroplasty complication, the bacterium itself is considered low virulence and is not well recognized as a common cause of infection in outpatient knee surgery. A literature search revealed no previous reports indicating infection due to P acnes after arthroscopic ACL reconstruction. While P acnes is a common skin flora, detection as an infectious agent may be low due to the slow growth rate and inability to detect positive culture growth unless the culture is held for longer than 4 days. 3,15,17,19 Thus, due to the difficult isolation of P acnes, the bacterium may remain unidentified and therefore underestimated in implant-associated complications. Awareness of this bacterium as a potential culprit and use of the unique intraoperative culture algorithm we describe can help distinguish true P acnes in cases of suspected occult infection in association with orthopaedic implants.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.