
Abstract
Background:
Several studies have been performed suggesting that a superolateral approach to cortisone injections for symptomatic osteoarthritis of the knee is more accurate than anteromedial or anterolateral approaches, but there are little data to correlate clinical outcomes with these results. Additionally, there are minimal data to evaluate the pain of such procedures, and this consideration may impact physician preferences for a preferred approach to knee injection.
Purpose:
To determine the comparative efficacy and tolerability (patient comfort) of landmark-guided cortisone injections at 3 commonly used portals into the arthritic knee without effusion.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
Adult, English-speaking patients presenting to a sports medicine clinic with knee pain attributed to radiographically proven grades I through III knee osteoarthritis were randomized to receive a cortisone injection via superolateral, anteromedial, or anterolateral approaches. Patients used a visual analog scale (VAS) to self-report comfort with the procedure. Western Ontario and McMaster Universities Arthritis Index (WOMAC) 3.1 VAS scores were used to establish baseline pain and dysfunction prior to the injection and at 1 and 4 weeks follow-up via mail.
Results:
A total of 55 knees from 53 patients were randomized for injection using a superolateral approach (17 knees), an anteromedial approach (20 knees), and an anterolateral approach (18 knees). The mean VAS scores for procedural discomfort showed no significant differences between groups (superolateral, 39.1 ± 28.5; anteromedial, 32.9 ± 31.5; anterolateral, 33.1 ± 26.6; P = .78). WOMAC scores at baseline were similar between groups as well (superolateral, 1051 ± 686; anteromedial, 1450 ± 573; anterolateral, 1378 ± 673; P = .18). The WOMAC scores decreased at 1 and 4 weeks for all groups, with no significant differences in reduction between the 3 groups.
Conclusion:
Other studies have shown that the superolateral portal is the most accurate. This study did not assess accuracy, but it showed that all 3 knee injection sites studied have similar overall clinical benefit at 4-week follow-up. Procedural pain was not significantly different between groups.
Patients commonly present to primary care providers with musculoskeletal complaints. Landmark-guided intra-articular (IA) corticosteroid injections are common procedures performed in the routine practice of both musculoskeletal specialists and general practitioners. The most common indication for injection is osteoarthritis, with the knee being the most common site. 14 The clinical utility of IA injection for short-term pain relief has been well established in the treatment of knee pain due to osteoarthritis. Furthermore, increasing evidence regarding safety suggests that steroid injection, including judicious use of repeat injections, will continue to play a significant role in outpatient, nonsurgical management of mild to moderate osteoarthritis. 1
Several studies have examined accuracy with regard to landmark-guided knee injections with the supposition that accuracy will lead to improved clinical outcome in addition to minimizing side effects. Accuracy is of utmost importance for joint aspiration and viscosupplementation. The data for IA cortisone for the knee are not as definitive, showing no clear correlation between accuracy of injection and clinical improvement. Recent reviews have tried to summarize the data on cortisone injections for the arthritic knee. Variable criteria for clinical improvement, a multitude of anatomic portals, use of live versus cadaveric subjects, as well as a multitude of techniques (image-guided vs landmark-guided) and equipment used (eg, needle length) have made this comparison more difficult across studies and have caused some conflicting reviews of the literature. 5,7,10 Most of the individual studies included in these reviews use 2 or more injection portals and compare their accuracy using air/contrast radiography, aspiration/back flow techniques, or direct visualization via arthroscopy, ultrasound, or dissection. Few studies have associated clinical outcomes data, and only 2 known studies assessed the procedural pain associated with knee injections at these sites. 2,12
These reviews suggest that for landmark-guided knee injections without effusion, the superolateral (SL) approach is more accurate, at around 90%. Anterior approaches were found to be only about 70% accurate, although some of these studies used a 1.5-inch needle and others used a 2.0-inch needle. 6,8,15 Magnetic resonance imaging (MRI) data may suggest that an average of 1.8 to 2.2 inches of soft tissue must be traversed to achieve IA injection using an anterior approach. 8
Our study was designed to directly assess clinical outcomes (not accuracy) within a clearly verifiable period of efficacy (4 weeks) for IA cortisone in the “dry” knee (without effusion) with radiographically proven grades I through III osteoarthritis. Three commonly used approaches (superolateral [SL], anteromedial [AM], and anterolateral [AL]) were compared in terms of pain associated with the procedure using a visual analog scale (VAS) as well as clinical improvement with the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) 3.1 scale (100-mm VAS). Given the data on accuracy related to needle length, a 2-inch needle was used for all injections.
Methods
Study Design and Population
This was a single-center, prospective, randomized controlled trial with 3 study arms of equal size. The study was approved by the local institutional review board. Indications for knee injection were patients presenting in routine clinical practice with knee pain or stiffness with arthritis as the suspected reason for pain/dysfunction. Patients with prior injections were eligible as long as they had not received an injection in the past 3 months. Radiographs confirming grades I through III arthritis via the Kellgren-Lawrence (K-L) scale were required within the past year and were interpreted by the treating physician. Patients with overlying skin infection, other inflammatory arthropathies affecting the knee, prior injection within 3 months, severe arthritis (K-L grade IV), clinically evident knee effusion, those requiring image guidance for any reason, and those younger than 18 years were excluded from the study. Non–English-speaking patients were excluded as the measurement tools used are available only in English. For patients requiring bilateral knee injections, each knee was randomized separately. Prior to the study, there was no standard injection site among providers in the clinic.
Injection Procedure
Consented, enrolled patients were randomized to 1 of the 3 procedure approaches (SL, AM, AL) using sequential randomization via secured, opaque, closed envelopes. Injections were performed by 1 of 7 physicians in the sports medicine clinic, all of whom had specialty training in sports medicine and in performing knee injections. All attended an educational session to review injection techniques relevant to this study. For the procedure, patients were positioned as described below, and the site was prepped in a sterile fashion using chlorhexidine. The site was anesthetized with ethyl chloride immediately prior to needle introduction. For all injections, 60 mg of Depo-Medrol (Pfizer) and 5 mL of 1% lidocaine without epinephrine were delivered using a 22-gauge 2-inch needle. For both anterior approaches, the patient was seated upright with the target knee hanging over the examination table at approximately 90° of flexion without support for the foot. The injection sites were determined by anatomical landmarks. The needle was inserted approximately 1 cm below the inferior patellar pole and immediately medial or lateral to the patellar tendon, with the needle tip targeted obliquely toward the intracondylar notch. For SL injections, the patient was positioned supine with the knee supported at approximately 10° of flexion. The injection was placed approximately 1 cm lateral and superior to the superolateral corner of the patella, directed medially toward the patellofemoral joint space. For all methods, once the injection was completed, the site was cleaned and a sterile bandage applied. The knee was passively brought through 20° of gentle range of motion, after which the patient was advised to stand and walk 20 to 30 feet on a flat surface. Each patient was provided with standardized postinjection care instructions that included suggestions for icing, oral analgesia, and activity restrictions.
Data Collection
Demographic information was obtained from the clinical record after consent. Outcomes were measured using a 100-mm VAS for pain directly before and after the procedure, as well as a baseline WOMAC 3.1 VAS scale. Two follow-up WOMAC questionnaires were given to the patient at the time of injection, to be completed and returned by mail 1 and 4 weeks after the injection, respectively. Participants were called or emailed at 1 and 4 weeks postinjection as a reminder to return forms.
Data Analysis
Our primary outcome was immediate postinjection pain as measured by the 100-mm VAS. With 80% statistical power and a significance level of 5%, our study was powered to detect a small effect size (0.25 standard deviation from the mean), and 45 participants were required (15 in each of 3 study arms). The minimal clinically important difference on VAS scales was a 20% change. Intention-to-treat analysis was performed using SAS version 9.2 (SAS Institute). Baseline characteristics in the treatment groups were compared using analysis of variance (ANOVA) for continuous variables and chi-square tests for categorical variables. One-way ANOVA was used to compare postinjection VAS means in the treatment groups. One-way repeated-measures ANOVA was used to compare change over time in the treatment groups, with the time × treatment interaction serving as the hypothesis test. We then conducted a sensitivity analysis excluding the second knee for the 2 subjects who had both knees randomized in the study.
Results
A total of 54 patients were recruited, consented, and randomized. One was excluded post hoc after baseline data revealed unusable answers due to an inability to follow instructions for the VAS scale format. Fifty-five knees from 53 patients completed all aspects of the procedure and baseline data collection: 17 in the SL group, 20 in the AM group, and 18 in the AL group. In total, 47 participants completed all follow-up surveys for a total of 49 knees studied (16 in the SL group, 18 in the AM groups, and 15 in the AM group) (Figure 1).

Selection of study participants. VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Baseline demographic characteristics are shown in Table 1. There was no significant difference between the study groups with respect to age, sex, or frequency of prior injections. The mean (±SD) VAS scores for procedural discomfort were 39.1 ± 28.5 (SL), 32.9 ± 31.5 (AM), and 33.1 ± 26.6 (AL) (P = .78), showing no significant difference between groups (Figure 2). Body position comfort was similar between injection sites as well (P = .30). WOMAC scores at baseline were similar between groups (1051 ± 686 [SL], 1450 ± 573 [AM], and 1378 ± 673 [AL] (P = .18). WOMAC scores decreased at 1 and 4 weeks for all groups, with no significant differences between the 3 groups’ reductions (P treatment = .38, P time < .0001, P time × treatment interaction = .06) (Figure 3). WOMAC scores for the SL, AM, and AL groups were 701 ± 687, 593 ± 555, and 891 ± 714 (P = .42) at 1-week follow-up and 600 ± 610, 665 ± 683, and 954 ± 699 (P = .30) at 4-week follow-up, respectively. When we excluded the second knee for the 2 subjects who had 2 knees involved, results were consistent with overall results (P time × treatment interaction = .13).

Injection pain and body position comfort by injection site, as measured by visual analog scale (VAS).
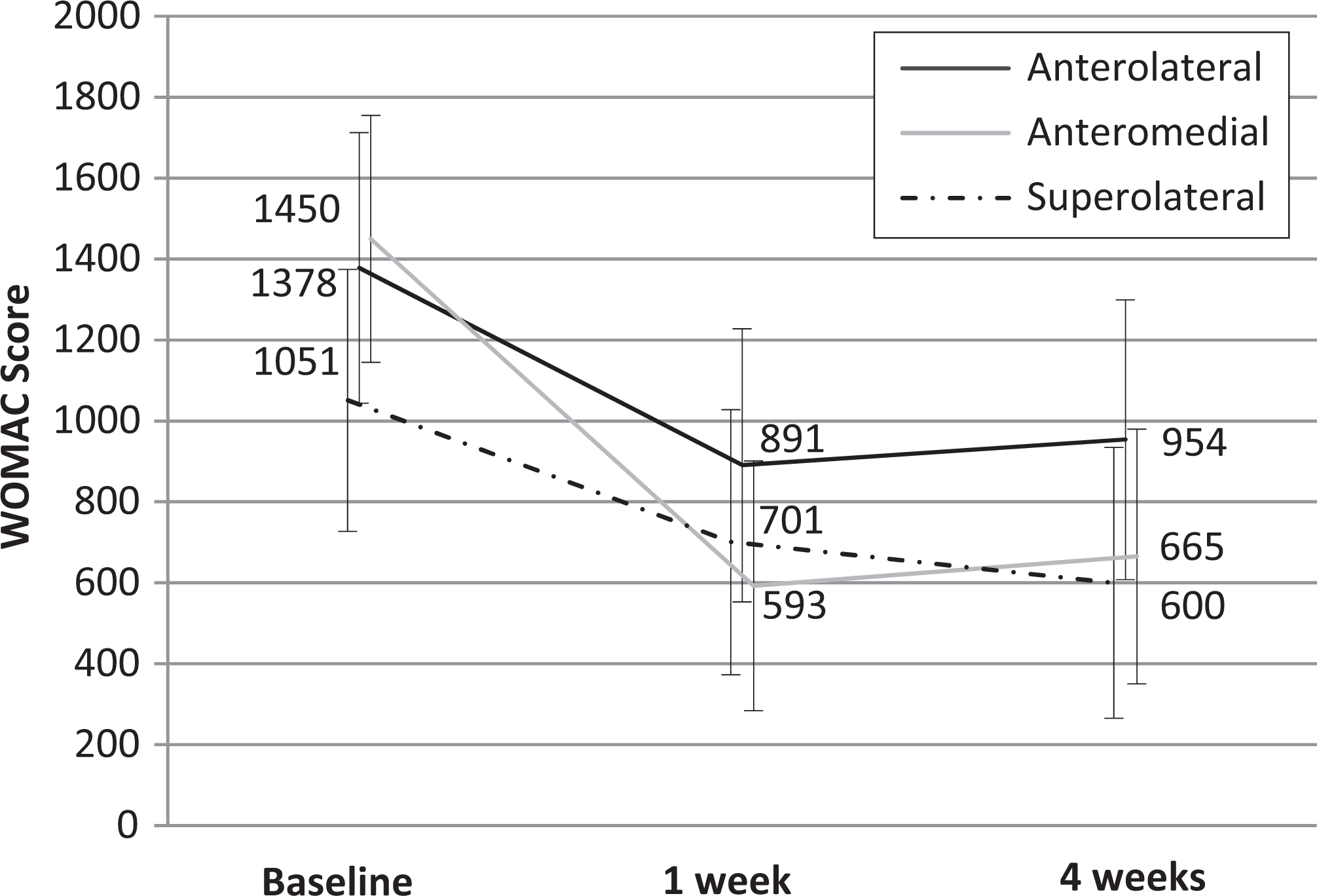
Western Ontario and McMaster Universities Osteoarthritis Scale (WOMAC) scores at baseline, week 1, and week 4 after anterolateral, anteromedial, or superolateral knee injection.
Characteristics of Study Participants by Site of Injection a

a Includes 2 subjects with both right and left knees injected.
Discussion
Intra-articular use of cortisone for the knee continues to be an important modality for short-term pain reduction in persons suffering from arthritis. Short-term efficacy has been well demonstrated. This study shows that the overall clinical outcome, as measured by the WOMAC scale, was not significantly different when injecting a dry knee using an SL, AL, or AM portal with a 2-inch needle. This suggests that, despite prior evidence of differing accuracy rates for these portals, there is similar short-term clinical efficacy for these injection sites. It is possible, however, that a 2-inch needle improved anterior accuracy, and therefore clinical benefit, to a level greater than that previously reported. Accuracy itself was not measured in this study, and a direct comparison between accuracy and efficacy can only be inferred from these data. Another possibility is that the injection portals differ in accuracy but have similar clinical outcomes due to local absorption via the synovium. Hence, exact placement of cortisone may not be necessary as cortisone diffuses through the synovium affecting intra-articular pathology. 13
Previous studies have compiled data from practitioners of various clinical backgrounds and experiences (radiology, rheumatology, general practice, orthopaedic surgery), typically 1 to 3 providers per study. Previous data have shown that for landmark- or palpation-guided injections, experienced clinicians may be more likely to be accurate. 4,9 Our study pooled data from 7 different sports medicine physicians ranging from more than 20 years of clinical experience to fellows in training. The difference in experience but similar training may have affected accuracy rates of knee injections but does offer data from a wide range of experiences.
In contrast to several previous studies, we used a 2-inch (51-mm) needle for all injections. Jackson et al 8 altered protocol of their accuracy study, using a 2-inch needle, after 9 of 13 injections performed with the AL approach during the pilot phase were found to be extra-articular. The use of a 2-inch needle is different from many routine clinical practices and is based on MRI data showing distance to the joint space from an AL approach. 8 Thus, use of a 2-inch needle may provide greater accuracy and improved clinical outcome as extra-articular anterior injections have been found to lay within the Hoffa fat pad. 7,15
Procedural discomfort, as measured by pain of the actual injection after freezing with ethyl chloride, in combination with body position (supine vs seated) was perceived as similar. Therefore, patients that may require a specific position due to comorbidities seem to tolerate the procedure similarly.
Limitations of this study include a relatively short follow-up, although prior studies have shown a clear short-term benefit with this procedure. We chose a 4-week follow-up to improve compliance and completion of the study and to ensure that the study period fell well within the expected duration of clinical benefit. 11 It is possible that less accurate anterior portals may show less clinical benefit in longer term follow-up, as suggested by previous studies that have linked accuracy with duration of effect. 3,7,10 In regular practice, intervals of 3 to 4 months between injections are more typical. Grade IV arthritis was excluded in this study, so data may not be applicable to patients with severe osteoarthritis. Adherence to postinjection care, activity, and medication use was not assessed; however, similar instructions were given to each participant, and adherence would likely not differ by injection site. This study did not have a mechanism to assess or control for the exact dates that participants mailed in their responses. While there were no grossly mistimed responses, some could have been answered outside the recommended periods, introducing recall bias; again, this was unlikely to differ by injection site. Among patients with grades I through III osteoarthritis of the knee, our study provides strong randomized controlled trial data that AM, AL, and SL corticosteroid injections provide similar clinical benefit up to 4 weeks postinjection.
Conclusion
AM, AL, and SL injections into arthritic knees without effusion seem to provide similar clinical benefit across a broad range of clinical experiences. All methods are well tolerated by patients. Clinicians may use their discretion in providing landmark-guided corticosteroid knee injections when providing care for knee arthritis patients.
Footnotes
One of more of the authors has declared the following potential conflict of interest or source of funding: B.S.W. received a grant from the Maine Medical Center Research Institute for study materials.
Acknowledgment
The authors thank Liz Robinson for her help implementing the study.