
Abstract
Background:
Numerous clinical examination maneuvers have been developed to identify meniscus tears of the knee. While meniscus injuries vary significantly in type and severity, no maneuvers have been developed that help to distinguish particular tear characteristics.
Purpose:
This nonconsecutive case series highlights a distinctive clinical finding that correlates with inferiorly displaced flap tears of the medial meniscus that become trapped in the medial gutter of the knee, as identified through magnetic resonance imaging (MRI) and arthroscopy.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
Eight patients with trapped medial meniscus tears were identified from a single surgeon’s academic orthopaedic sports medicine practice between January 2009 and January 2012. Each patient underwent clinical evaluation, MRI, and arthroscopic treatment for meniscus injury. Clinical notes, MRI images, radiology reports, and operative findings were reviewed and compared in a descriptive fashion.
Results:
Each patient displayed a positive clinical examination finding of medial knee pain inferior to the joint line with flexion and the application of valgus stress in the setting of a torn medial meniscus and intact medial collateral ligament (MCL). Preoperative MRI revealed a distinctive flap tear of the medial meniscus flipped inferiorly to lay trapped between the tibia and deep fibers of the MCL. On arthroscopy, flap tears were found displaced inferiorly and trapped in the medial gutter in 6 of the 8 patients. Displaced meniscal fragments in the remaining 2 patients were found within the medial compartment.
Conclusion:
Inferiorly displaced flap tears of the meniscus that have been displaced to the medial gutter can be localized through a careful examination technique.
Clinical Relevance:
Early identification of this injury pattern may help reduce the likelihood that the trapped fragment will be missed during arthroscopy.
Keywords
Knee arthroscopy for a meniscus tear is one of the most commonly performed surgical procedures in the United States. 10 Medial tears are reported more commonly than lateral tears 3,13,18 and are classified according to the ISAKOS (International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine) Meniscal Documentation Committee as longitudinal-vertical, horizontal, radial, vertical flap, horizontal flap, or complex. 2 Vertical tears may result in locked and detached fragments, while horizontal tears result in superior and inferior flaps. 6 Horizontal tears can produce fragments that become inverted and subsequently “trapped” between the medial aspect of the tibial plateau and the deep fibers of the medial collateral ligament (MCL). This particular type of medial meniscal tear may be more difficult to recognize during arthroscopy, and if missed, results in ongoing knee pain postsurgery. 14
In the clinical setting, provocative maneuvers that cause compression of meniscal fragments between the tibia and femur will often lead to pain. Thus, pain with varus stress may suggest medial meniscal injury. This concept is supported by maneuvers such as the Payr and Bohler tests, described in the earlier literature; in the former maneuver, the patient sits cross-legged placing a stress on the medial meniscus, and in the latter, a simple varus and valgus stress elicits pain with compression of the meniscus. 20 It is further suggested through more modern tests in which weightbearing is incorporated into rotatory movements, such as in the Thessaly test. 1,12 However, when the meniscal fragment is flipped and interposed between the deep fibers of the MCL and the tibia, valgus stress will lead to compression of the fragment between these structures and medial pain.
Medial pain with valgus stress is classically associated with MCL injury. MCL injury is most commonly associated with insertional pain and ligamentous laxity. In the case of the trapped medial meniscus tear, pain is localized to the point where the fragment is interposed just inferior to the joint line. The aim of this nonconsecutive case series was to highlight that the finding of medial-sided pain with knee flexion and the application of a valgus stress, in the setting of an intact MCL, may indicate an inferiorly displaced flap tear of the medial meniscus. We have observed that this examination finding often correlates with the trapped medial meniscus on magnetic resonance imaging (MRI) and subsequent arthroscopy, providing a means for early detection of this injury pattern.
Methods
Eight patients (8 knees) were drawn from the academic orthopaedic sports medicine clinic of the senior author (D.C.T.) between January 2009 and January 2012. Patients had undergone initial workup, and MRI findings were consistent with the earlier described “trapped” medial meniscus tear. Routine tests during physical examination were used to detect meniscal injury, including joint line tenderness, pain with hyperflexion, and the McMurray test. As these patients had atypical presentation of medial-sided pain, flexion with application of valgus stress was applied. This maneuver was performed with the patient supine while the knee was flexed between 30° and 120° in a dynamic fashion. A valgus stress was applied to the lateral aspect of the knee with the examiner’s free hand. In a positive test, the patient would experience a new or significant increase in pain directly adjacent and inferior to the joint line on the medial side of the tibia. This pain did not correspond with MCL insertion sites and was not present with flexion alone (Figure 1 and Video Supplement).

Application of valgus stress to the right knee while flexing between 30° and 120° with the patient in the supine position.
Magnetic resonance imaging and arthroscopic reports were analyzed to confirm the specific nature of meniscal injury. Interpretation by a musculoskeletal radiologist was compared with independent review, with focus on language depicting the nature or location of the meniscal fragment. Review of arthroscopic reports also focused on the specifics of the meniscal tear. Institutional review board approval was granted for this retrospective study.
Case Study
A 54-year-old automobile dealership manager injured his knee while running on the treadmill. He presented with complaints of swelling and a sharp medial-sided knee pain. Physical examination revealed normal gait with minimal effusion. There was distinct tenderness to palpation along the medial joint line, and positive McMurray testing, where both patient and examiner recognized a painful mechanical click during testing that corresponded with symptoms. Lachman and posterior drawer testing were negative, and there was no pain or opening with varus stress. Valgus stress elicited medial pain without laxity. Pain was focused just distal to the joint line, and palpation of the MCL showed no significant pain at the proximal and distal insertions. Medial-sided pain was most significant when the knee was taken through a range of motion between 30° and 120° while applying valgus stress.
Subsequent MRI showed high signal within the body of the medial meniscus extending into the posterior horn, indicative of medial meniscus tear. A musculoskeletal radiologist noted an “undersurface and radial tear of the body and posterior horn of the medial meniscus with flipped fragment into the inferomedial gutter” (Figure 2).
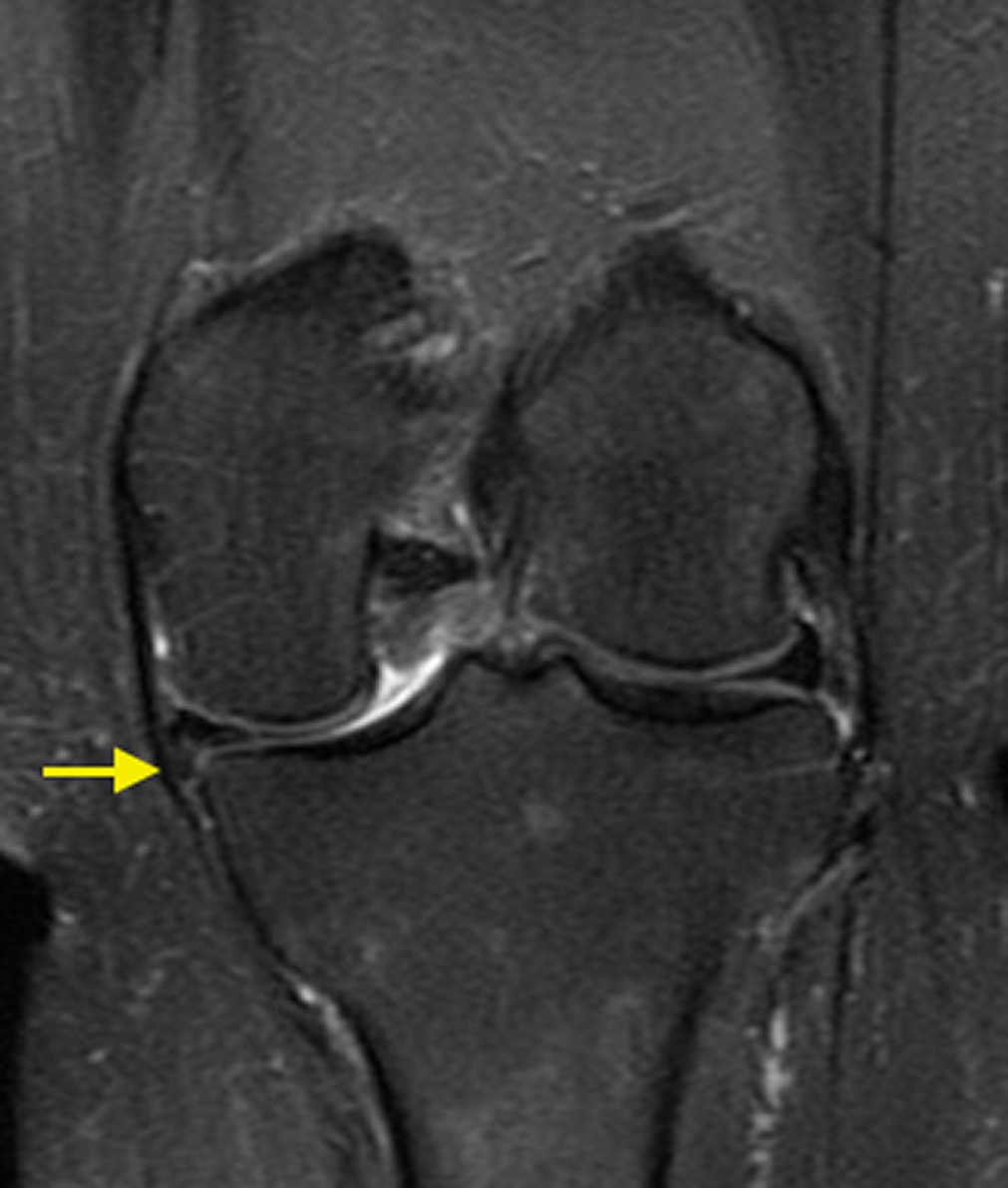
Coronal T2-weighted magnetic resonance image displaying inferiorly displaced flap tear of the medial meniscus interposed between the deep fibers of the medial collateral ligament and the tibia (arrow).
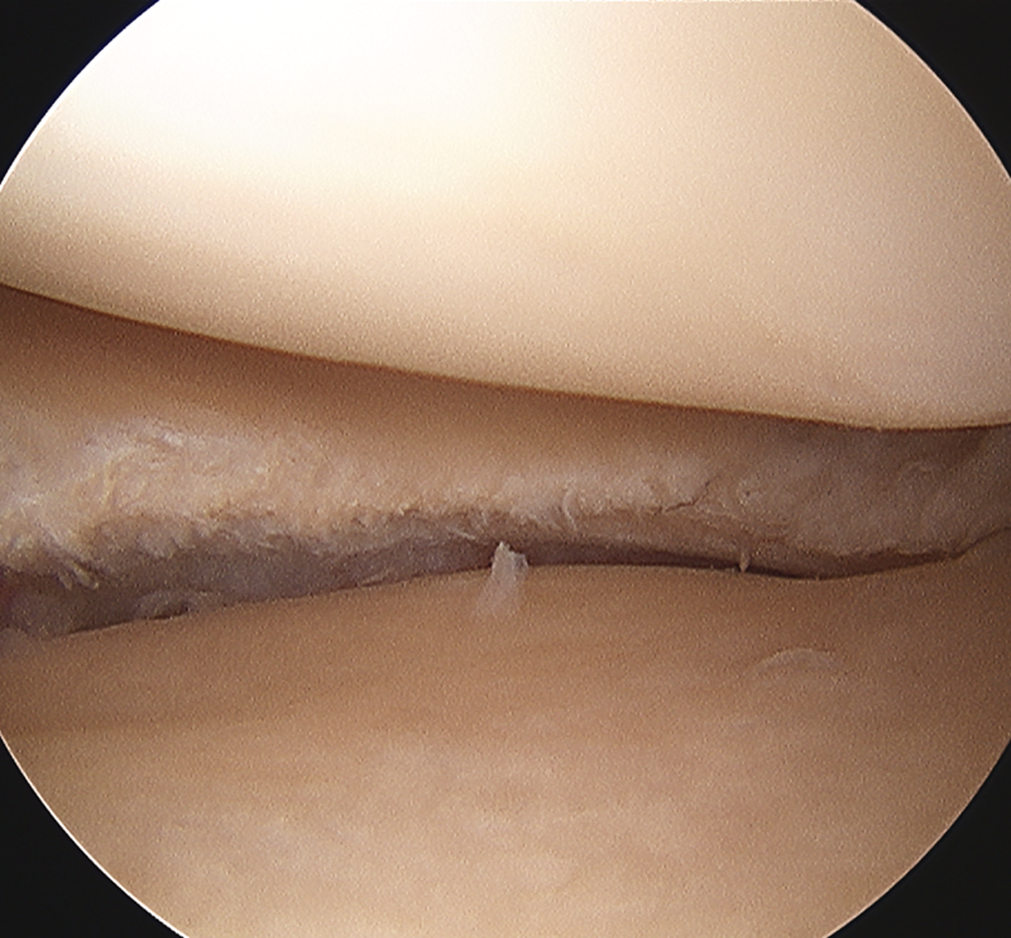
An arthroscopy was performed 2 weeks after the MRI. With the exception of the medial meniscus tear, diagnostic arthroscopy was unremarkable (Figure 3). On probing the meniscus, an undersurface component of the tear was noted to have flipped inferiorly. This fragment was reduced with the probe into the compartment (Figures 4 and 5). Debridement was carried back to a stable rim, with a 5-mm meniscus remaining at the narrowest point (Figure 6).

Arthroscopic image of the medial compartment of the knee displaying a frayed, but what appears to be intact, medial meniscus.

Arthroscopic image of the medial compartment of the knee displaying an inferiorly displaced flap tear of the meniscus as revealed by the probe.

Arthroscopic image of the medial compartment of the knee displaying an inferiorly displaced flap tear of the meniscus returned to the compartment with the assistance of a probe.
Arthroscopic image of the knee after debridement of the inferior flap tear.
The patient progressed well postoperatively with gradual return to activity. A summary of the clinical, MRI, and arthroscopic findings of all cases is presented in Table 1.
Patient Demographics and Examination, Magnetic Resonance Imaging (MRI), and Arthroscopy Findings
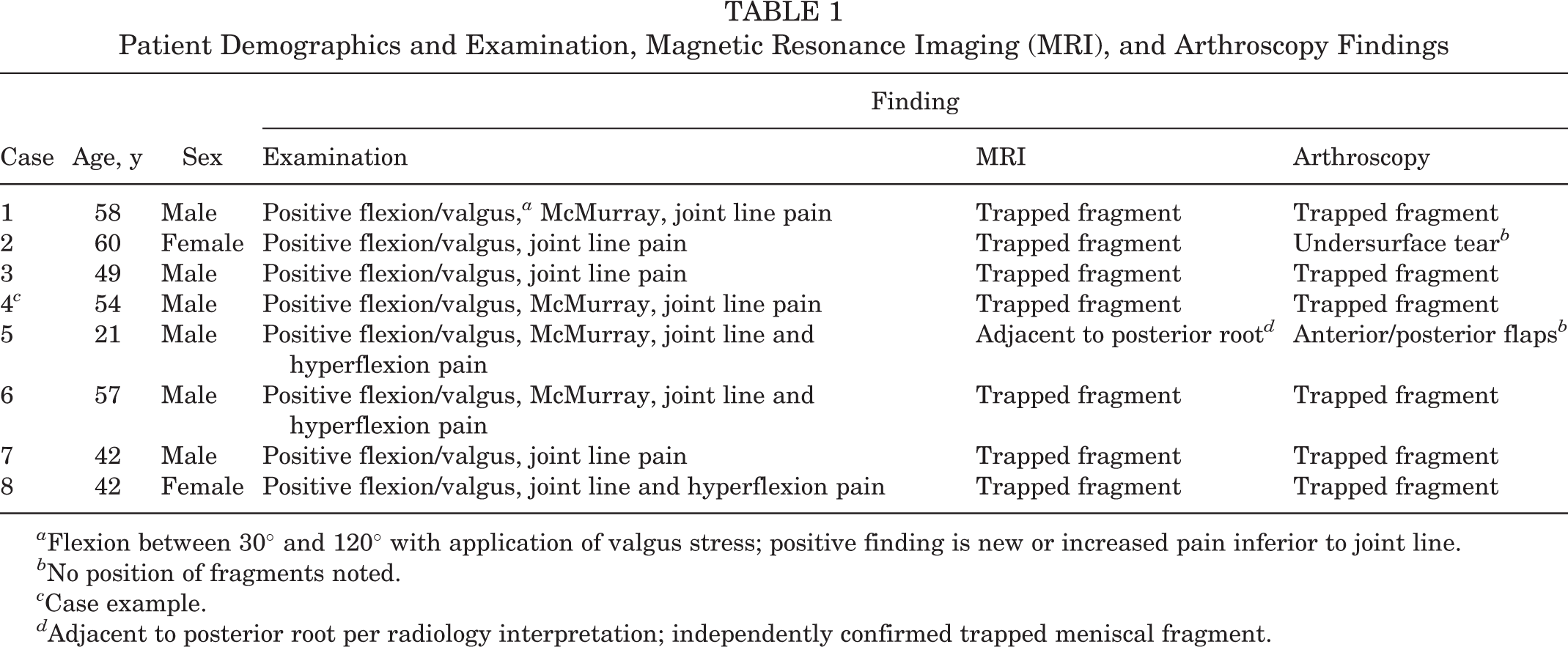
a Flexion between 30° and 120° with application of valgus stress; positive finding is new or increased pain inferior to joint line.
b No position of fragments noted.
c Case example.
d Adjacent to posterior root per radiology interpretation; independently confirmed trapped meniscal fragment.
Discussion
Magnetic resonance imaging is an effective tool for detecting large displaced lesions of the meniscus such as bucket-handle tears. 21 Displaced lesions are described either through identification of the free fragment or alteration of normal meniscal contour. The free fragment of a bucket-handle tear may be described as intracondylar (double posterior cruciate ligament sign) or anteriorly flipped. 11 Alteration in meniscal contour may be described as the absent bow tie or coronal truncation signs. Consideration of these signs in combination greatly improves diagnostic accuracy. 7 Likewise, the free fragment identified adjacent to the tibial plateau in the medial gutter as seen on the coronal view should be sought after and reported to help reduce the likelihood that this injury is missed during arthroscopic intervention. 14
As MRI accuracy improves, so does the risk of overreliance on this technology. Miller 17 found that sole reliance on MRI without application of clinical judgment would have led to inappropriate treatment in 35% of knees studied. Other studies suggest experienced examiners are superior to MRI in identifying surgically treatable meniscal lesions. 8,18 As fiscal constraints placed on medical management increase, MRI may be reserved for situations in which an experienced clinician requires further information before arriving at a diagnosis. 17,18
The clinical diagnosis of meniscal tears has been found to be more accurate when combinations of tests are used. 3,9,13 Traditional maneuvers such as the McMurray test 16 and the Apley compression test 4 have low diagnostic accuracy when performed in isolation. However, by combining joint line tenderness and the McMurray test, Konan et al 13 were able to lift sensitivity and specificity to over 90% for detection of a medial meniscus tear, and sensitivity to 75% and specificity to 99% for a lateral tear when the anterior cruciate ligament was intact. One composite score proposed by Lowery et al 15 in 2006 included a history of mechanical symptoms combined with 4 examination maneuvers. When the patient reported a positive history and experienced pain with hyperextension, maximum flexion, pain or click with the McMurray test, and joint line tenderness to palpation, there was a 92.3% positive predictive value of finding a meniscal tear. 15 Additional clinical tests continue to be proposed. For example, the medial-lateral grind test was introduced as a useful adjunct to the McMurray test because of a low reported frequency of false positive results. In this test, the patient lies supine while the examiner cradles the extremity in 1 arm. The index finger and thumb of the opposite hand palpate for a distinct grinding sensation at the medial and lateral joint line while the knee is flexed and a valgus force is applied, then extended with a varus force, producing a circular motion. 3 The Thessaly test 12 elicits pain with dynamic loading of the knee where the patient rotates internally then externally, standing on the ipsilateral leg in 5° and 20° of flexion; the Ege test 1 involves a squat in internal or external rotation. Finally, the knee compression-rotation test is where the tibia is compressed and rotated with respect to the femur. 19 All these more recent maneuvers were introduced with evidence of high sensitivity and specificity but have not supplanted the original tests, nor does consensus exist regarding a composite evaluation for meniscal injury. 5 The maneuver described in this article is not meant to supplant those described, but to complement these tests, and perhaps, add further information to help distinguish a specific type of tear.
This nonconsecutive observational case series highlights a small group of patients with a distinct clinical finding that correlates with a specific type of medial meniscal tear evident on MRI and arthroscopy. Weaknesses of the study include the lack of prospective design and control group, the small sample size, and the fact that the examiner was not blinded to MRI findings. With respect to the maneuver described, it should be noted that some of the deep fibers of the MCL are continuous with the capsule and meniscal rim, and a valgus stress that places the MCL under tension may also elicit pain with other tear patterns through appositional means. This would reduce the specificity of the test. Although not specifically examined in this study, we have also found that tenderness at the location of the trapped portion of the torn meniscus, which in thin patients can sometimes be palpated, will help confirm the diagnosis of a trapped medial meniscus tear. Based on the results of this small observational report, we feel further study is warranted to determine not only the incidence of this unique finding but also sensitivity and specificity of the test and how the test correlates with other established maneuvers.
Conclusion
Testing for medial-sided knee pain with flexion and application of valgus stress should be considered in patients for whom there is a concern of medial meniscal injury to avoid missing trapped inferiorly displaced flap tears on arthroscopy.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.