
Abstract
Background:
Previous studies have reported on the promising effects of changing running style in patients with chronic exertional compartment syndrome (CECS) using a 6-week training program aimed at adopting a forefoot strike technique. This study expands that work by comparing a 6-week in-house, center-based run training program with a less extensive, supervised, home-based run training program (50% home training).
Hypothesis:
An alteration in running technique will lead to improvements in CECS complaints and running performance, with the less supervised program producing less dramatic results.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Nineteen patients with CECS were prospectively enrolled. Postrunning intracompartmental pressure (ICP), run performance, and self-reported questionnaires were taken for all patients at baseline and after 6 weeks of running intervention. Questionnaires were also taken from 14 patients (7 center-based, 6 home-based) 4 months posttreatment.
Results:
Significant improvement between preintervention and postintervention rates was found for running distance (43%), ICP values (36%), and scores on the questionnaires Single Assessment Numeric Evaluation (SANE; 36%), Lower Leg Outcome Survey (LLOS; 18%), and Patient Specific Complaints (PSC; 60%). The mean posttreatment score on the Global Rating of Change (GROC) was between +4 and +5 (“somewhat better” to “moderately better”). In 14 participants (74%), no elevation of pain was reported posttreatment, compared with 3 participants (16%) at baseline; in all these cases, the running test was aborted because of a lack of cardiorespiratory fitness. Self-reported scores continued to improve 4 months after the end of the intervention program, with mean improvement rates of 48% (SANE), 26% (LLOS), and 81% (PSC). The mean GROC score improved to +6 points (“a great deal better”).
Conclusion:
In 19 patients diagnosed with CECS, a 6-week forefoot running intervention performed in both a center-based and home-based training setting led to decreased postrunning lower leg ICP values, improved running performances, and self-assessed leg condition. The influence of training group was not statistically significant. Overall, this is a promising finding, taking into consideration the significantly reduced investments in time and resources needed for the home-based program.
Lower extremity overuse injuries are common in occupations that involve prolonged weightbearing and repetitive lower limb activities, such as those in the military. Army recruits and infantry soldiers typically have a high prevalence of lower extremity overuse injuries, which vary from 15% to 40%. 9,21,23,40 These types of injuries may result in significant lost duty and training time and greatly increased costs of medical care. 28
Injuries to the leg such as medial tibial stress syndrome (MTSS), chronic exertional compartment syndrome (CECS), and stress fractures are among the most common forms of lower extremity overuse injuries seen in the military. High-impact running activities may particularly lead to increased bone-related injuries such as stress fractures and MTSS, while both running and low-impact marching activities may induce myofascial problems such as CECS. Our study focuses on the latter condition.
Chronic exertional compartment syndrome is an idiopathic pain condition that is frequently associated with a sudden or significant increase in activities such as walking, (forced) marching, or running—as is often the case when young and relatively untrained military recruits start their basic training. Other speculated risk factors for CECS include muscle hypertrophy from the use of anabolic steroids, creatine supplementation, and biomechanical deviations in running (eg, overstriding, overpronation). 5,8 The classic symptoms of CECS include lower leg pain and tightness following exertion, with a complete absence of physical signs and symptoms at rest. 7 As the problematic activity (typically running) continues, compartment pressures progressively increase, causing increased lower leg pain, sensory abnormalities, and muscle weakness, which eventually results in a premature cessation of the activity. 3,13,16 –18,24,35 Symptoms normally subside within 15 minutes of activity cessation, but classically return at the same or slightly shorter interval/intensity during the next training session. 7,18
While several hypotheses exist that explain the development of CECS pain, the exact pathophysiology of CECS is not understood. The primary accepted theory is that exercise increases intracompartmental pressure (ICP), which in turn compromises circulation, prohibits muscular function, and causes pain and disability in the lower leg. 4,7,13,15,31,34 CECS may occur unilaterally or bilaterally and may be present in a single compartment or all 4 compartments of the lower leg (anterior, lateral, superficial posterior, and deep posterior). The anterior and deep posterior compartments are the most commonly affected (45% and 40%, respectively). 38 ICP measurement using needle manometer technology is the currently accepted gold standard for confirming the CECS diagnosis, although the validity and reliability of this measurement is not entirely unchallenged. 2,23
Prior to 2012, conservative treatment for CECS was focused on addressing the extrinsic and intrinsic factors that may contribute to this condition and typically included prolonged rest periods, a decreased level of physical activity, anti-inflammatory agents, orthotics, ultrasound, massage, stretching, and electrical stimulation. 5,17 The efficacy of these conservative treatment options was extremely poor, with no suggestion of consistently positive outcomes. In the absence of effective conservative treatment, recruits and soldiers who were unable to abstain from or modify their problematic activities typically underwent surgical management by means of a fasciotomy. This type of surgery has proven to be an effective treatment modality in CECS, especially in the anterior and lateral compartments. 29,33 While the majority of patients do well after surgery, approximately 3% to 17% experience less than favorable outcomes such as pain, decreased sensation or hypersensitivity to touch at the incision site, paresthesia, infection, and hemorrhage. 7,13,19,30,37 Additionally, even individuals who do well initially may have a risk of symptom recurrence, which is reported to be as high as 50% over 5 years. These less favorable operative outcomes and the morbidity burden that postoperative rehabilitation has on military readiness gives great relevance to discovering alternative strategies for effective nonoperative CECS management.
In 2 recent studies, Diebal et al 12,13 reported on the promising effects of changing running technique in US military members with CECS indicated for surgical release. A 6-week forefoot running instruction program led to decreased postexercise ICP values, significant reductions in pain and disability, and improved performance outcomes on running tests, and these results were maintained and/or improved after 1 year of follow-up. Surgical intervention was avoided for all patients at the 1-year follow-up.
The rationale behind this intervention is that most runners have a habitual rearfoot strike pattern, which is often accompanied with a long stride length and prominent dorsiflexion of the foot at ground contact. This leads to a marked increase in the eccentric activity of the anterior structures of the lower leg, in particular the tibialis anterior muscle. 32 The running technique concept that was used in the studies by Diebal et al 12,13 focused on a forefoot strike pattern (ie, landing on the ball of foot) by applying shorter strides and a significantly increased step rate (180 steps per minute or more). These adaptations reduce ground reaction impact forces by minimizing ground contact time and vertical displacement, but, more important, they shift the eccentric loading of the anterior compartment musculature of the leg to the posterior lower leg structures such as the Achilles tendon and the gastrocnemius-soleus muscle complex. These structures have demonstrated higher elastic recoil potential and may be better suited to absorb eccentric impact forces during landing. 1,10,11,25,26
This study expands the work by Diebal et al 12,13 into non–US military members. Our primary aim was to evaluate, in 3 consecutive case series, the effectiveness of a 6-week intervention program aimed at changing running technique in Dutch military service members with CECS of the lower legs. In the first 2 training iterations, the program was conducted at the Military Sports Medical Center in Utrecht, the Netherlands. In the third iteration, a less extensively supervised treatment program (50% center-based training, 50% home training) was evaluated. We hypothesized that alterations in running technique would lead to improvements in CECS complaints, decreased ICP values, and increased running performance. In addition, we hypothesized that both extensively and less extensively supervised programs would lead to decreased compartment pressures and improved running performance, but that the less supervised program would produce less dramatic results.
Methods
Design and Study Population
A single-group prospective cohort design was used in this study, closely following the study design used by Diebal et al. 13 Members from the Royal Netherlands Army, both recruits and active duty soldiers, diagnosed with CECS by a general surgeon of the Dutch Military Hospital, were sent to the Military Sports Medical Center in Utrecht to be included in the study after providing written informed consent.
To be included in this study, patients had to be military members required to pass the annual 12-minute running test. They had to report a minimum of 2-month history of recurrent anterior and/or lateral leg pain and tightness in 1 or both legs that worsened with running. Pain had to occur within the first 15 minutes of running and lead to cessation of desired exercise. In addition, all symptoms had to completely resolve within 15 minutes on cessation of running. The physical examination findings had to be normal at rest (ie, no tenderness or compartment tightness to palpation and full functional ability to squat and hop without symptoms).
Exclusion criteria included a postexercise ICP in the anterior compartment of the lower leg <35 mm Hg, a history of previous fasciotomy or other lower extremity surgery, any condition that would cause lower extremity swelling, creatine supplementation in the previous 2 months, any injury that would affect running tolerance besides CECS, any respiratory issue that could affect running tolerance, and current use of nonsteroidal anti-inflammatory drugs (NSAIDs) that would interfere with test outcomes. Approval for the center-based intervention program was granted by the institutional review board of the University Medical Center Utrecht.
Preintervention Measurements
Intracompartmental Pressure Measurements
To objectify and confirm the clinical diagnosis of CECS, 1-minute postexercise ICPs of the anterior compartments were measured, according to Verleisdonk. 36 All measurements were performed by the same sports physician using a Stryker pressure monitor. During ICP measurements, the patient was supine, with the legs dangling over the edge of the table in a free, nearly vertical position. ICPs were measured directly after CECS symptoms forced the individual to cease a running test on a treadmill (Technogym SPA), following a standardized running protocol with progressive increases in speed and inclination. These postrunning preintervention ICP values were also used to evaluate the effectiveness of the treatment program. Additionally, after each minute of running, patients scored their “pain profile,” that is, the level of pain in 4 lower leg regions (right lateral, right medial, left medial, left lateral) on a 10-point rating of pain scale. The test was aborted at a score of 7 out of 10 in at least 1 region. This running test design for CECS complaints has been previously described by Zimmermann. 41
Demographic Measurements
A baseline biometric screening included measurements of body height, body weight, fat percentage (skinfold measurement according to Durnin and Womersley 14 ), waist circumference, and blood pressure. Measurements were done by the same practitioner to avoid inter-rater reliability issues. Moreover, sex, age, and duration of complaints were recorded at baseline.
Self-Assessed Leg Condition
Participants filled out 3 self-report questionnaires, composed of the following: (1) the Single Assessment Numeric Evaluation (SANE), 39 a 1-item question rating the lower leg condition on a 0 to 100 scale, with 100 being normal; (2) the Lower Leg Outcome Survey (LLOS), 13 a 20-item scale questionnaire that specifically evaluates leg conditions such as CECS, with a range of scores between 0 and 60, with a score of 60 being normal; and (3) the Patient Specific Complaints (PSC) questionnaire, 6 in which, from a list of different daily activities, patients had to select the 1 to 3 most important activities that were hampered by their leg complaints in the past week, and rate them on a 100-mm visual analog scale (VAS).
Running Performance and Kinematic Measurements
At baseline, participants performed a running test on a treadmill (Woodway) at the Military Sports Medical Center. Prior to the running test, participants were asked to select a speed they thought they could normally maintain for approximately 25 minutes at a steady pace. This self-selected pace was used during the running test. Pain profile scores were asked after every minute of the running test. The test was aborted if 1 of the following occurred: a pain score of 7 out of 10 in at least 2 of the lower leg regions, after the participant ran 5 km without scoring a 7, or when the participant himself asked to stop due to reaching their cardiorespiratory limit. Running distance was used as 1 of the outcome variables. The Woodway treadmill was equipped with the Optojump Next system (Microgate), which is an optical measurement system consisting of a transmitting and receiving bar for measuring spatiotemporal parameters such as step length, step frequency, contact time, and flight time. At both pre- and postintervention running tests, the participants wore the same running shoes.
Intervention
A team of specialists, consisting of a running specialist, a physical therapist, and 2 human movement scientists, conducted a 6-week group-training program aimed at altering running technique. The primary aim of the program was to have participants adopt a forefoot strike running gait where they would land on the ball of foot (BOF) and demonstrate principles from the Pose Running Concept (Pose Tech Corp). Key features of this running strategy are to run at a minimum of 180 steps per minute, decrease stride length, and to actively use the hamstring muscle group to pull the support foot from the ground while “falling” forward under a gravitational torque (the center of mass moves in front of the support limb, thereby using gravity to propel movement). 25
The training program started with a 1-hour theory class in which background information was given about the intervention program. During the 6-week program, subsequent training sessions of approximately 60 minutes each were conducted 3 times a week at the Military Sports Medical Center for the center-based (CB) group. The home-based (HB) group trained twice a week in the first 3 weeks and once a week in the last 3 weeks at the center. For the remaining sessions, 1 in the first 3 weeks and 2 in the last 3 weeks, participants had to train at their own military base or at home. No other training activities were allowed in both groups during the 6-week intervention period.
A typical training session consisted of the following consecutive elements: head-to-toe joint flexibility exercises, specific running technique drills aimed at specific running movement patterns, running integration drills, running bouts of increasing length, and a cool down. Drills focused on issues such as perception of body weight and pressure on BOF, changing support, leaning forward while running, and pulling the support foot from the ground directly under the hip. Combinations of these elements were applied in the running integration drills. The specific running technique (integration) drills used in our intervention are described elsewhere in detail. 12,13,27 The intensity and duration of the running integration drills and running bouts increased throughout the time frame of the program. For proprioception purposes, all training activities in the first 3 weeks were performed barefoot. Thereafter, shod running was gradually incorporated into the program. In addition to verbal cues (eg, “shorter strides,” “increase step rate,” “run quietly”), digital metronomes were used to pace the cadence at 180 steps per minute or more. Individual running performance was videotaped weekly and discussed as a visual feedback tool at the beginning of the next training session. For the HB group, all videos (including slow-motion replays and coaching cues) were uploaded on the Internet for personal use during their home training. The training sessions were all performed indoors. Participants of the HB group received a training log with information on how to perform each home training session. The training log contained flexibility exercises, drills, and an indoor running program. The content and principles of the delivered running technique program comply with that of the US Army study by Diebal et al. 13
Postintervention Measurements
One week after the last training session, all baseline measurements (ie, biometry, questionnaire, ICP, running performance) were repeated. The protocols were identical to those used to obtain the baseline measurements (ie, running tests were executed using identical speed values, inclinations, and running times). One item was added to the questionnaire: the Global Rating of Change (GROC), 20 a 15-point scale to measure the patients’ perceived change and overall improvement, from “a very great deal worse” (score, −7) to “a very great deal better” (score, +7). The postintervention running test prior to the ICP measurements was executed using the same protocol from baseline, that is, participants ran the same amount of time at the same elevation and speed.
Information on surgical intervention after the 6-week training program was not included in this study since the military hospital policy on fasciotomy changed during the study period toward predominantly conservative treatment modalities. At 4 months postintervention, participants were asked to fill in a follow-up questionnaire consisting of the SANE, LLOS, PSC, and GROC.
Statistics
Following the study by Diebal et al, 13 running distance and postexercise ICP values (left-right mean values for the patients with bilateral symptoms) were chosen as the primary outcomes variables of this study. In addition, self-assessed outcome variables (SANE, LLOS, PSC, GROC) and kinematic variables (step length, step rate) were evaluated, the latter to quantify whether running form had indeed changed toward a forefoot striking pattern.
Pre- to postintervention differences in outcomes were checked using paired samples statistics. The assumption of normality was checked by using a Shapiro-Wilks test, as well as by visual inspection of the q-q plots and box plots of the data within the groups. Nonparametric testing was used if the assumption of normality was violated. No random sampling distribution was used because of the small sample size of this study.
The effects of training program (CB vs HB) on all outcome measures were examined using a 2-way repeated-measures analysis of variance, with training group as the between-subjects variable and pre- to postintervention changes in outcomes as the within-subjects variables. The level of significance was set at P < .05. All statistical analyses were performed using SPSS statistics software (version 18; SPSS Inc).
Results
Overall Patient Group
Baseline Characteristics
In total, 22 patients with CECS received an informed consent form for 1 of 3 training cycles (January 2013, April 2013, and September 2013). Two patients did not start the program due to logistic reasons (ie, not available for 6 consecutive weeks), and 1 patient was excluded because of additional ankle problems. The number of patients per treatment group was limited to 7 patients, both due to logistic constraints (staff capacity, facilities) and because this group size would suit our training purposes best. Baseline demographics and clinical characteristics of the 19 included patients are shown in Table 1. All patients reported a history of CECS symptoms for a minimum of 2 months, and all but 2 patients had bilateral CECS symptoms. For those patients with bilateral symptoms, there were no significant differences in postexercise ICPs between left and right legs (not presented). Combined MTSS and CECS symptoms were present in 47% of the overall group, with CECS being the dominant injury. Fourteen patients (11 CB, 3 HB) chose running as their main PSC complaint, 2 patients (HB) chose speed marching (ie, a combination of running and marching), 2 patients (1 CB, 1 HB) chose executing military work, and 1 patient (CB) chose prolonged standing. Reported earlier treatment modalities included rest, physical therapy, NSAIDs, orthotics and/or modified shoes, and training without running technique instructions specific to the Pose Method. All patients in this study were soldiers with a “remedial” status, that is, soldiers who were waivered for their regular unit physical training program due to their physical condition. Prior to the initiation of the study, none of the patients were able to successfully complete their mandatory annual military service 12-minute running test due to their lower leg complaints. Baseline running assessments revealed that, in all but 2 participants, lower leg pain occurred within the first 2 minutes of running and progressively worsened while running. In the other 2 participants, both from the CB group, pain emerged after 3 and 5 minutes of running, respectively. All participants visually ran with a rearfoot striking gait pattern.
Baseline Patient Characteristics and Scores on Outcome Measures for the Overall, Center-Based, and Home-Based Groups a

a Numbers of individuals are presented, unless otherwise stated. CB, center-based; CECS, chronic exertional compartment syndrome, HB, home-based; MTSS, medial tibial stress syndrome; NSAID, nonsteroidal anti-inflammatory drug.
b Based on skinfold measurement: healthy weight, up or below normative value; overweight, ≤5% above normative value; obesity, >5% above norm value. Age- and sex-adjusted normative values according to Durnin and Womersley. 14
c Average health risk, circumference between 79 and 94 cm (men) or 68 and 80 cm (women); raised health risk, circumference between 95 and 102 cm (men) or 81 and 88 cm (women); strongly raised health risk, circumference >102 cm (men) or >88 cm (women). Normative values according to Lean et al. 22
Pre- to Postintervention Results
All patients complied with the 6-week program; no patient had to withdraw due to complications or an inability to tolerate the running intervention. In the overall group of 19 patients, significant differences between pre- and postintervention scores were found for all outcome measurements but step rate. Figure 1 presents the results for the primary outcomes: running distance (mean increase of 43%) and postexercise ICP (mean decrease of 36%). Table 2 presents the results for the self-reported outcomes, with mean improvement rates in SANE, LLOS, and PSC scores of 36%, 18%, and 60%, respectively. The mean postintervention GROC score was between +4 and +5, which correspond with “somewhat better” to “moderately better.” Step length decreased significantly from pre- to postintervention (mean difference, 3.8 cm), while mean step rate remained unchanged. Moreover, biometric measurements and blood pressure measurements did not change over time in the overall group (not presented). In 14 participants (74%), no elevation of pain was reported during the postintervention running test, compared with 3 participants (16%) whose pain values did not elevate at the baseline running test. In all these cases, the running test was aborted due to a lack of cardiorespiratory fitness. No complications (eg, stress fractures) were reported in either study group during the intervention period. The pre- to postintervention differences in running styles of several participants are available as an online Video Supplement to this article.
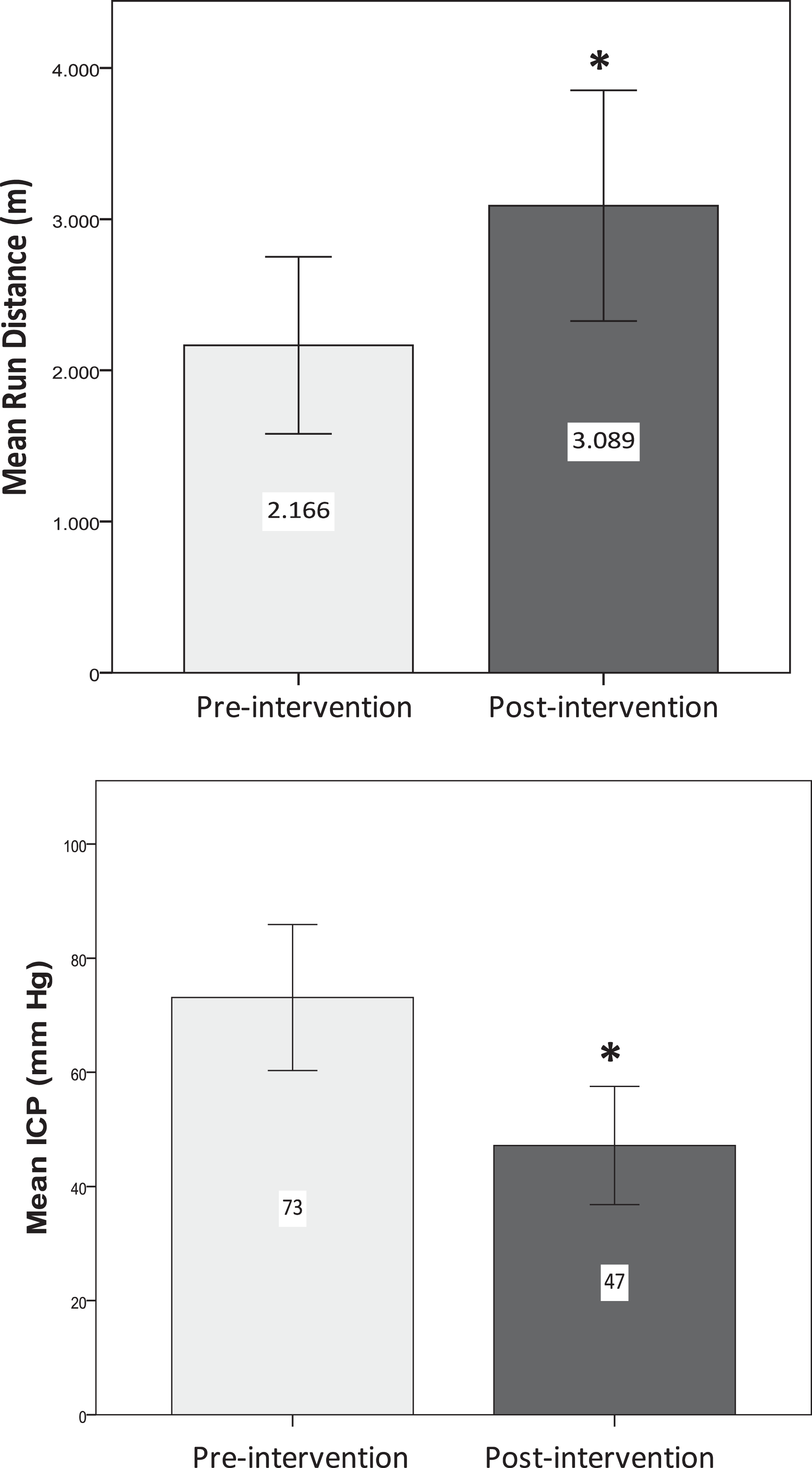
Pre- and postintervention mean scores on the primary outcome measures (running distance, postexercise intracompartment pressure [ICP]) for the overall study group (N = 19). Error bars denote 95% CI. *Statistically significant difference between pre- and postintervention (P < .05).
Analyses of Differences (Paired-Samples Test) Between Pre- and Postintervention Scores on Self-Assessed Leg Condition and Kinematic Measurements for the Overall, Center-Based, and Home-Based Groups a

a Mean ± SD scores are presented per group. CB, center-based; GROC, Global Rating of Change (range of scores: −7 to +7); HB, home-based; LLOS, Lower Leg Outcome Survey; Post, postintervention; Pre, preintervention; PSC, Patient Specific Complaints; SANE, Single Assessment Numeric Evaluation.
b Difference between preintervention and postintervention scores.
c A follow-up measurement at 4 months postintervention was taken from the 2 last shifts: April 2013 (CB, n = 7) and September 2013 (HB, n = 6).
Four-Month Follow-up Results
Because of logistic restraints, only participants from the April 2013 group and later (CB group, n = 7; HB group, n = 6) filled out the follow-up questionnaire. Self-reported scores continued to improve 4 months after the end of the intervention program, with mean improvements of 48% (SANE), 26% (LLOS), and 81% (PSC). The mean GROC score improved to +6, which corresponds with “a great deal better” (Table 2).
Center-Based Versus Home-Based Group
Baseline Characteristics
The 2 training groups demonstrated different baseline values for the primary outcomes: The CB group showed higher mean postexercise ICP values and lower mean running distances than the HB group. Moreover, the CB group included 1 older participant (53 years of age), and showed a somewhat higher percentage of overweight participants as well as patients with long-standing CECS complaints. Most other baseline patient characteristics were comparable between the 2 groups (Tables 1 and 2).
Pre- to Postintervention Results
The CB group showed significant differences from pre- to postintervention on all outcome measures except step rate. In the HB group, all outcome measures changed significantly except running distance. We only found a significant interaction between group and pre- to postintervention scores on step rate, which indicates that training group had a significant influence on step rate. None of the other variables showed an interaction effect with group. In the CB group, 8 participants (62%) had to abort their postintervention running test due to a lack of cardiorespiratory fitness (vs 2 participants [15%] at baseline). In the HB group, all 6 participants (100%) stopped their postintervention running test due to a lack of cardiorespiratory fitness (vs 1 participant [17%] at baseline). Figure 2 displays the results for the primary outcome measurements; Table 2 includes the results for the other outcomes.

Pre- and postintervention mean scores of the primary outcome measures for the center-based group (n = 13) and the home-based group (n = 6). Error bars denote the 95% CI. *Statistically significant difference between pre- and postintervention (P < .05). ICP, intracompartmental pressure.
Four-Month Follow-up Results
As in the overall group, both the CB group and the HB group showed larger improvements in the self-reported outcomes 4 months after the end of program, compared with the postintervention measurements (Table 2).
Discussion
The effectiveness of a 6-week treatment program aimed at changing running technique was studied in Dutch military service members with CECS of the lower legs. Our hypothesis was that the running intervention would lead to improvements in CECS complaints in terms of decreased ICP values and increased running performance. Based on the results, this hypothesis can be confirmed. The primary outcomes of running performance and postexercise ICP showed significant improvements over time. Moreover, the patients’ self-assessed leg condition improved significantly. We additionally hypothesized that the home-based program (50% center-based training, 50% home training) would lead to less convincing results than the center-based program due to the decreased supervision. Our study demonstrated mixed results here, possibly due to the baseline differences between the 2 groups with regard to fitness level and leg complaints. Both the CB group and the HB group showed significant improvements in postexercise ICP values and self-assessed leg condition from pre- to postintervention, but only the CB group showed significant improvements in running performance.
Our main findings align with those from Diebal et al. 13 Our study is a (partial) replication of their case series conducted at the US Military Academy. Pre- to postintervention running distance significantly increased by 300% in the US study (1400 ± 600 vs 4800 ± 500 m). Our overall group showed somewhat lower improvements in running performance (43%), possibly due to its more heterogeneous character in terms of age, military job function, lower leg symptoms, and duration of complaints. The CB group showed a significant increase in running distance of 72%, whereas the HB group showed a small and statistically insignificant decrease of 6%. This difference may reflect the differences seen at baseline between the 2 groups: mean running distance was nearly twice as high and the mean postexercise ICP level was somewhat lower in the HB group. It is possible that their CECS complaints did not hamper their running performance as much and/or as soon as it did in the CB group. Consequently, the relatively high baseline level of running performance in the HB group may have given less room for improvement over time in terms of running distance. In terms of pain level, there was a clear improvement in the HB group: No participant of the HB group had to abort their postintervention running test due to pain, compared with 5 participants at baseline.
Diebal et al 13 found that mean anterior ICPs after running showed significant postintervention decreases of 51% (78.4 ± 32.0 vs 38.4 ± 11.5 mm Hg), slightly higher than the significant ICP decreases of 37% seen in our overall group. These small differences in ICP improvements between the 2 studies may reflect the aforementioned differences between the study populations. Differences in the standardized measurement techniques used in both studies (eg, the position of the lower leg during pressure measurement, which was supine and supported in the US group vs hanging in the Dutch group) are less likely to explain the pre- to postintervention differences.
The significant improvements in self-reported outcome measures found in our overall group, ranging from 39% (mean SANE score) to 18% (LLOS) to 60% (PSC), were comparable or somewhat lower than the improvements found in the US study (81% for SANE, 21% for LLOS, 96% for VAS). Self-reported outcomes continued to improve 4 months after the end of the intervention period, which suggests that the effects of a 6-week program aimed at modifying running technique has longer term potential. The authors chose a follow-up period of 4 months for this study because, together with the injury time and intervention time, this covers a period of at least 6 months. This 6-month period is a meaningful time frame in the Dutch military setting due to national job security regulations.
The direction of changes in the kinematic parameters step length and step rate demonstrated in both studies were in direct correlation with the imposed running technique alterations, that is, decreased step lengths and increased step rates. Changes were more prominent in the US study, which suggests that the adaptation to the new running style was somewhat more successful in their population. This may explain the greater improvements in outcomes seen in this group.
In our experience, individuals often suffer from both CECS and MTSS symptoms. To our knowledge, research has yet to be done that investigates the impact of adopting a forefoot running technique in individuals with combined symptoms. Indicatively, our study, with half of the group reporting mixed problems, shows that modifying running style targeting the reduction of CECS complaints coincidentally does not provoke MTSS symptoms and may even result in beneficial symptom changes. Looking into the pain profiles of the overall group during the running test at baseline, 9 of 19 patients suffered from combined complaints, that is, scoring a 3 or more (out of 10) on the pain profile for the MTSS-related medial regions of the lower legs. At the end of the 6-week training program, this number dropped to 4 of 19 patients. Future research is needed to specifically address the effects of forefoot running on combined complaints of MTSS and CECS. Moreover, research in individuals who have developed CECS symptoms during (forced) marching activities, as opposed to running activities, may be an interesting topic with regard to military populations. Principles derived from the running technique that was used in the current study may be applied to change marching style in this target group. The authors are currently planning another study to confirm this hypothesis.
The main purpose of this study was to replicate the study findings by Diebal et al 13 in a different (military) setting. We have added information to the US case studies by including a home-based intervention program. Evidently, the study design has some weaknesses concerning the relatively small numbers per group (lack of power to determine group difference), short follow-up period, and the lack of a control group. Our study was built around 3 consecutive case series, for which patients were grouped during different time frames (January 2013, April 2013, September 2013). The number of patients per treatment group was limited to 7 patients, both due to logistic constraints (staff capacity, facilities) and because we anticipated that this group size would suit our training purposes best. We had to work with eligible patients (referred to us by the surgeon) within a certain time frame to prevent the first patients assigned to each group from waiting too long prior to treatment initiation. This explains why we had 7 patients in the second shift and 6 patients in the other 2 shifts. We have chosen to neither use a randomized nor a controlled design, since we thought this was not feasible considering the expected numbers of patients that would be referred to our center within a reasonable time frame. We realize that this choice weakens the methodologic power of our study and the intercomparability of the study groups.
To summarize, in 19 patients diagnosed with CECS, a 6-week forefoot running intervention performed in both a center-based and home-based training setting led to decreased postrunning lower leg ICP values and improved running performances. The pain and disability typically associated with CECS were significantly reduced, and scores improved even greater at 4 months postintervention. Both training programs showed significant improvements over time, and the influence of training group on all but one of our measurements (step rate) was not statistically significant. Overall, this is a promising finding, taking into consideration the significantly reduced investment in time and resources needed for the home-based program. Considering the small sample size and lack of control group in the study, future research with more power is needed to confirm these results.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Acknowledgment
The authors thank Mr Rik van Trigt, senior physical trainer of the Royal Netherlands Army and running specialist, for his assistance in the development and execution of the running intervention programs used in this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.