
Abstract
Background:
Complications related to hip arthroscopy are rare, with a current rate of <2%. Some complications are related to fluid extravasation, which has been associated with life-threatening conditions such as abdominal compartment syndrome, cardiopulmonary arrest, hypothermia, and atelectasis.
Purpose:
To identify risk factors for fluid volume extravasation in hip arthroscopy and to determine the relationship between anatomical location on computed tomography (CT) and extravasated volume.
Study Design:
Case series; Level of evidence, 4.
Methods:
We performed a prospective cohort study of 40 consecutive arthroscopies for femoroacetabular impingement. Patient demographics and procedures performed (ie, acetabuloplasty and its size, femoral osteoplasty, and psoas tenotomy) were recorded. The extravasated volume was estimated by the difference between the infused volume and the intraoperatively collected volume. Within 12 hours after the procedure, the pelvis was scanned by CT. We created a 3-stage radiological classification based on progressive involvement of anatomical structures attributed to liquid extravasation. Statistical analyses were performed with a 95% CI and a significance level of 5%.
Results:
No relevant clinical symptoms related to fluid extravasation were recorded. The mean extravasated volume was 3.06 L at a rate of 1.05 L/h, corresponding to nearly 10% of the infused volume. There was a trend toward greater extravasated volume with longer operative time and longer time in the peripheral compartment (without axial traction); however, there was no statistical significance. The anatomical classification on CT imaging was directly related to the extravasated volume and compromised the thigh, gluteus, and retroperitoneum and intraperitoneal spaces. There was a 6-fold greater probability of female patients having an advanced stage extravasation on CT classification.
Conclusion:
In our series, 10% of the infused volume was extravasated in uncomplicated hip arthroscopy. Risk factors for extravasation were related to operative time, particularly during peripheral compartment intervention (ie, without traction). The anatomical classification proposed in this study reflects the progressive involvement of the thigh, gluteus, iliopsoas, and retroperitoneal and intraperitoneal spaces after increase in extravasated volume. Compared with males, females were associated with more severe anatomical compromise for the same extravasated volume.
In recent years, hip arthroscopy has been established as a useful tool for the treatment of different prearthritic conditions. 6,9,11,16 Complications related to this procedure are rare, with current rates of less than 2%, 5,8,11,18,20,24 which highlight lesions attributable to traction (eg, perineal and neurapraxia injuries), surgical access (eg, scuffing, labral damage, breakage of instruments), and fluid management (eg, extravasation). 1,7,10,13,25,28
Fluid management is essential when performing arthroscopy, which primarily includes knee and shoulder procedures; however, few studies focus on the issue of fluid management. 3,14,15,17,19,22,23 In the hip, these complications are feared because they have been linked to life-threatening conditions such as abdominal compartment syndrome, cardiopulmonary arrest, hypothermia, and atelectasis. 1,7,10,12,13,25,28 However, most complications have been reported in case reports. Two cohort studies have recently been published on the subject: One study 26 tried to determine the volumes of extravasation, and the other study 27 showed no significant renal impairment or electrolyte changes associated with this procedure. However, no study has systematically determined the anatomical location of this extravasation.
Since we perform hip arthroscopy in our institution, we have patients undergo a computed tomography (CT) scan after the procedure to evaluate the quality of the acetabuloplasty and the femoral osteoplasty. Patients are aware of the radiation risk of this examination. While reviewing the CT, we found edema in different compartments, so we proposed this study. The aims of our study were to identify the risk factors for extravasated volume (EV) and to determine the relationship between it and the anatomical location on CT.
Materials and Methods
This study obtained the approval of the hospital ethics committee. We conducted a prospective study in a consecutive series of 40 hip arthroscopies, performed during 2011 by a single surgeon, on 36 patients with femoroacetabular impingement (FAI). All procedures were performed under combined anesthesia (epidural and general) with the patient supine on a traction table under fluoroscopic guidance. In all patients, the anterolateral, anterior, and midanterior portals were used, as described by Robertson and Kelly. 21 The central compartment was treated under continuous traction. 4 The peripheral space was approached without traction with hip in 30° to 45° of flexion. A T-shaped capsulotomy was performed in all patients. Acetabuloplasty, labral reinsertion, femoroplasty, psoas tenotomy, and capsular closure were performed, when appropriate. We used Ringer lactate solution (3-L bags) with epinephrine (1 mg per bag), which was infused by a Dyonics 25 Fluid Management System pump (Smith & Nephew) with pressures between 40 and 90 mm Hg and a 1.5 L/m flow. 2
We recorded the operative time with and without traction, as well as the performance of acetabuloplasty and its size (according to a clockwise fashion), femoral osteoplasty, and psoas tenotomy.
The EV was calculated by the difference between the infused volume and the collected volume. The infused volume was estimated by counting the bags of Ringer lactate solution and subtracting the remnants in the bags and in the infusion system catheters. The collected volume was measured as the sum of the volume from a bag placed on the surgical drapes, the contents of the receptacles connected to the instruments, and floor suction systems.
Within 12 hours after the procedure, a pelvic CT without contrast was performed in all patients by a Somatom Sensation 64 CT scanner (Siemens) to determine the quality of correction of the FAI and the anatomical involvement attributable to fluid extravasation. Once all CT studies were available, we asked the radiologists to describe the changes attributable to fluid occupation. This allowed the categorization of patients into 3 different groups based on the severity and structures involved: mild (subcutaneous and interfascial thigh edema), moderate (interfascial thigh and/or gluteal fluid collection), and severe (iliopsoas edema and/or retroperitoneal-intraperitoneal fluid collection) (Figure 1).

Computed tomography classifications. (A) Mild: interfascial thigh edema; (B) moderate: thigh-gluteal fluid collection; (C) severe: iliopsoas edema and retroperitoneal and intraperitoneal fluid collection.
In 4 patients who received bilateral surgery, each side was operated on with at least a 3-week interval between procedures. Each hip was analyzed as a separate procedure.
Data analysis was performed in 2 stages. In the first stage, we conducted an analysis to identify factors associated with the amount of extravasation volume. For this, the Shapiro-Wilk test was initially applied to check if the EV could assume a normal distribution. It was considered adequate if the probability was >0.15.
We then calculated the Pearson correlation between EV and age, surgical time, length of time with traction, and time without traction. An unpaired t test with Welch adjustment was applied to analyze EV by sex, operated side, and capsulotomy. The patients who underwent acetabuloplasties were separated into 4 groups: patients without acetabuloplasty (group 1), patients with acetabuloplasty between 1 and 2 hours (group 2), patients with acetabuloplasty between 3 to 4 hours (group 3), and patients with acetabuloplasty 5 hours or more (group 4). The analysis of variance test was applied to analyze the association between acetabuloplasty size and EV.
In the second stage, analysis was conducted to find factors associated with radiological classification of EV occupation on CT. First, a univariate ordinal regression was performed using the CT stages as dependent variables. A multivariate ordinal regression model was then estimated using the variables that showed statistical significance in the univariate model estimation. The post hoc probabilities were calculated. Ordinal regression models for estimation require a parallelism assumption. This was checked with the Brant test and considered acceptable if the probability was >0.15.
A confidence interval of 95% and a significance level of .05 were used. Data were processed using STATA v.11.1 software (Stata Corp).
Results
Demographics
Of the 40 arthroscopies, 23 (57.50%) procedures were performed on women and 17 procedures were performed on men. The mean age of the patients was 36.30 ± 9.04 years. Age was directly related to EV, but without statistical significance (Pearson correlation = –0.17, P = .28). Seventeen procedures were performed on the left side and 23 on the right side. The operated side had no relation to the EV (P = .38).
Operative Time
The mean surgical time was 171.2 ± 32.49 minutes. During the surgery, the mean time with traction was 115.13 ± 27.73 minutes and without traction was 56.00 ± 31.03 minutes.
Fluid extravasation was greater with a longer surgical time, but this did not reach statistical significance (Pearson correlation = 0.25, P = .11) (Figure 2). The EV decreased with a longer period of traction (Pearson correlation = –0.03), and the volume increased with a longer period without traction (ie, peripheral compartment) (Pearson correlation = 0.29). However, this difference was not statically significant (P = .86 and .07, respectively).
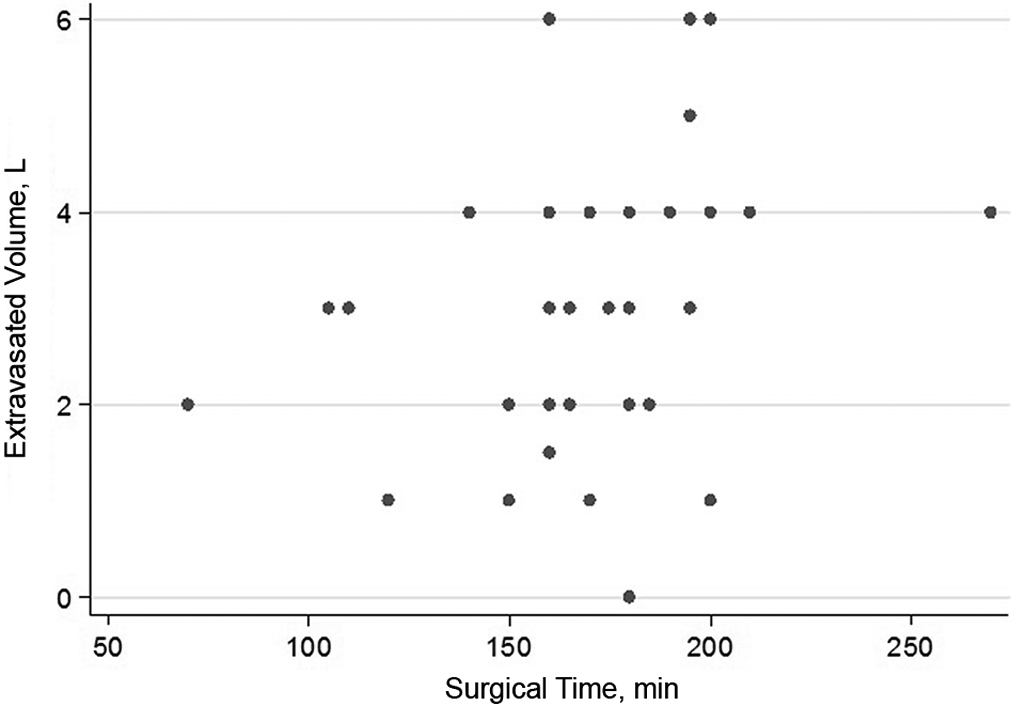
Scatterplot showing the relationship between the operating time and extravasated volume.
Surgical Technique
Acetabuloplasty was performed in 37 (92.50%) patients. The mean EV was 3.01 L when acetabuloplasty was performed and 3.67 L without acetabuloplasty (P = .45). When acetabuloplasty was performed, the median time of the operation was 4 hours (range, 0-6 hours). We found no differences between the acetabuloplasty time and EV (P = .47).
Femoral osteoplasty was performed in 33 (82.50%) patients. The average extravasated fluid was 3.23 L with femoral osteoplasty and 2.29 L without femoral osteoplasty (P = .12). Tenotomy was performed only in 2 (5.00%) patients and was associated with increased mean EV (4.00 and 3.01 L) but without reaching statistical significance (P = .34).
A femoral osteoplasty alone was performed in 3 patients, and acetabuloplasty alone was performed in 7 patients. Two patients underwent a psoas tenotomy in conjunction with acetabuloplasty and femoral osteoplasty.
Extravasation Volume
The mean EV was 3.06 ± 1.43 L, with an infused volume of 33.56 ± 10.41 and 30.5 ± 10.30 L of collected volume. Women had a higher mean EV (3.35 ± 0.25 L) compared with men (2.68 ± 0.40 L). However, there was no statistical significance (P = .15). No patient in this series had clinical complications attributable to the extravasation of fluid.
Anatomical Findings on CT
Table 1 shows the mean EV for each stage of the proposed CT classification. Figure 3 shows the distribution of EV in each group. Table 2 shows the frequency distribution of CT stages by sex.
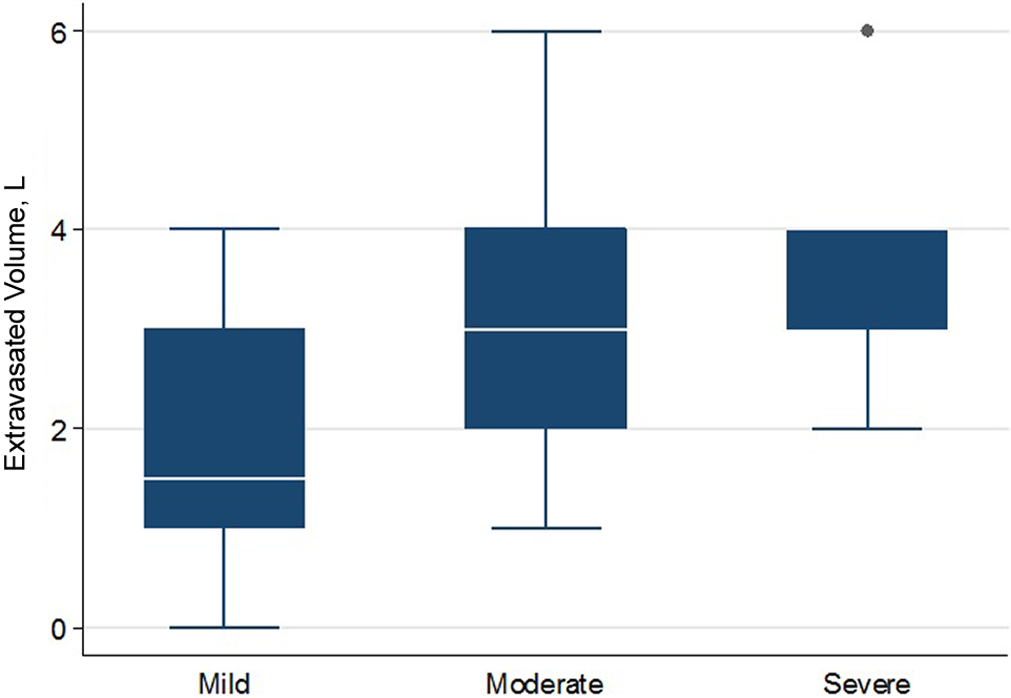
The distribution of extravasated volume by computed tomography stage. The dot indicates outliers from the distribution.
Extravasated Volume by CT Stage a

a Values are reported as mean ± SD. CT, computed tomography.
Distribution of CT Stage by Patient Sex a
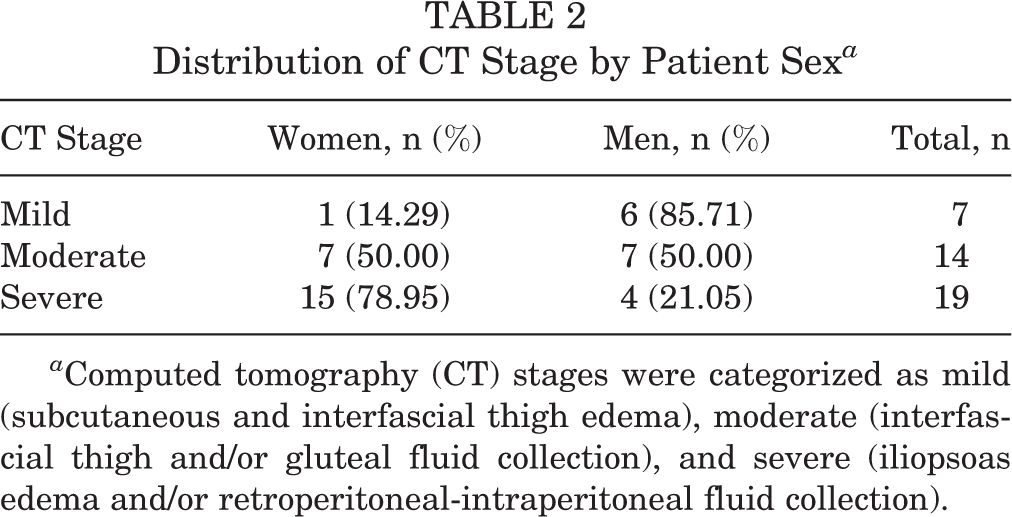
a Computed tomography (CT) stages were categorized as mild (subcutaneous and interfascial thigh edema), moderate (interfascial thigh and/or gluteal fluid collection), and severe (iliopsoas edema and/or retroperitoneal-intraperitoneal fluid collection).
On univariate analysis, women had an increased risk of having a more severe CT classification (odds ratio [OR] = 7.24; 95% CI, 1.90-27.49). As the EV increased, the risk of having a more severe CT stage also increased (OR = 2.01; 95% CI, 1.22-3.31). The powers of these findings were 0.63 and 0.53, respectively.
Ordinal multivariate regression showed that EV and patient sex were significant variables. The OR for EV was 1.89 (95% CI, 1.15-3.10), and the OR for females with a more severe CT stage was 6.60 (95% CI, 1.65-26.41). Table 3 shows the post hoc probabilities associated with each stage based on EV and patient sex.
Probability of Being in a CT Stage Based on Extravasated Volume a

a Results of an estimated ordinal model. CT, computed tomography.
Discussion
In 1998, the first case of serious complications attributable to extravasation of fluid in hip arthroscopy was reported. 1 In this case, the patient developed cardiopulmonary arrest secondary to an abdominal compartment syndrome during removal of loose bodies from a recent acetabular fracture fixation. Surgical drainage of 9.6 L between peritoneal and chest fluid was reported in this patient. In subsequent publications regarding this complication, 7,10,25 the drained volumes were lower (reportedly 1.2-3 L), whereas in others, there was no drainage. 8,13,28
To our knowledge, there had been no systematic reports on the normal expected fluid extravasation in an uncomplicated hip arthroscopy until the study by Stafford et al. 26 In that study of 28 patients, an average of 1.1 L was reported. That finding is well below our study. On comparing both series, the series of Stafford et al 26 has a shorter duration of arthroscopy (68 vs 171 minutes). However, the extravasation rate is similar in both series (1.002 vs 1.050 L/h), which corresponds to approximately 10% of the infused volume (9.7 vs 33.5 L).
The magnitude of extravasation has also been associated with procedures such as capsulotomy size, femoral osteoplasty, and psoas tenotomy. Surgical time has also been strongly associated with the amount of extravasation. 26 In our series, there was a trend toward greater EV with longer operative times, but it did not reach statistical significance or correlation. It is notable that, although not reaching statistical significance, the time in traction appears to be a protective factor against extravasation. From a clinical point of view, this could be explained by the associated ligamentotaxis, which can impair fluid migration toward the endopelvis. This may also explain the fact that time without traction and hip flexion are associated with increased EV. This is also consistent with the observation that acetabuloplasty, which is performed in traction, is not associated with increased extravasation, and this is why femoral osteoplasty is actually associated with greater leakage. On the other hand, psoas tenotomy has been linked with increased extravasation. 7 This is also shown in the report by Stafford et al 26 ; however, in our series, psoas tenotomy was done only in 2 cases, so it was not possible to analyze the association.
All reports in which extravasation led to a clinical manifestation—including potentially fatal complications—mentioned the occupation of retroperitoneal, peritoneal, and/or pleural spaces. The anatomical involvement found in this study on CT secondary to fluid extravasation was progressive. In the “severe” stage, “mild” and “moderate” CT findings are both present. Therefore, we believe that the amount of EV is relevant because it is associated with involved anatomical structures in a progressive way, being more likely to affect vital structures on the abdomen or thorax.
Females presented a 6-times greater chance of developing a more advanced stage, based on CT imaging, compared with males at the same EV. This could be explained by the gynecoid pelvic anatomy and other factors such as tissue elasticity. This suggests that more caution should be taken with intraoperative volume management in this group of patients.
To our knowledge, this is the only study to date that addresses occupation by the anatomical fluid in relation to hip arthroscopy without clinical complications. In the report from Stafford et al, 26 a radiopaque contrast medium was used at the end of the procedure in less than 20% of patients. In our opinion, this does not necessarily represent what happens during the entire procedure.
When monitored by ultrasound, fluid extravasation disappears as early as 16 hours after surgery. 10 Our study uses CT, which can confirm adequate correction of FAI and can determine the anatomical structures affected by the fluid within that period. This showed that the most likely route of fluid extravasation occurs through the iliopsoas sheath space.
It was not our purpose to recommend the use of CT in all patients undergoing hip arthroscopy. Rather, our purpose was to make hip surgeons aware of the factors that are associated with fluid extravasation so they can take the necessary actions to prevent or make an earlier diagnosis of complications associated with EV.
Limitations
The most important shortcoming of our study is the small number of patients. This may explain why the vast majority of our observations did not reach statistical significance.
Conclusion
Extravasated fluid volume in our series of 40 uncomplicated hip arthroscopies was on average 3 L (range, 2.60-3.52 L), with an average rate of approximately 1 L/h. A longer operative time, longer time in the peripheral compartment (ie, without traction), and psoas tenotomy showed a trend toward greater fluid extravasation. The anatomical classification proposed in this study reflects the progressive involvement of the thigh, gluteus, iliopsoas, and retroperitoneal and intraperitoneal spaces after increases in EV. Females were associated with greater anatomical involvement on CT compared with males at the same EV.