
Abstract
Background:
The anteromedial portal technique for drilling of the femoral tunnel during anterior cruciate ligament (ACL) reconstruction has been advocated by many surgeons as allowing improved access to the anatomical footprint. Furthermore, suspensory fixation of soft tissue grafts has become popularized because of complications associated with cross-pin fixation. Concerns regarding the use of both have recently arisen.
Purpose:
To raise awareness of the increased risk of graft failure when using the anteromedial portal technique with suspensory femoral fixation during ACL reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
From November 1998 to August 2012, a total of 465 primary ACL reconstructions were performed using quadrupled hamstring autograft tendons, with drilling of the femoral tunnel performed via the transtibial portal. Graft fixation on the femur was achieved with cross-pin fixation, while interference screw fixation was used on the tibia. From September 2012 to October 2013, there were 69 reconstructions performed through an anteromedial portal. While there was no change in graft choice, a change was made to using suspensory femoral fixation. No other surgical or postoperative rehabilitation changes were made.
Results:
During the 14-year period in which ACL reconstructions were performed via the transtibial portal and with cross-pin fixation, 2 graft failures (0.4% failure rate) were reported. After switching to the anteromedial portal with suspensory fixation, 7 graft failures (10.1% failure rate) were reported over a 13-month period. These were 5 male and 2 female patients, with a mean age of 18.8 years—all elite athletes. The same surgical technique was used in all patients, and all patients had at least an 8 mm–diameter graft. Patients were cleared to return to sport at an average of 8.4 months postoperatively, after completing functional performance tests. Of the 7 patients, 6 sustained a rerupture of the graft within 2 weeks of returning to full competition. The final patient sustained a rerupture 10 months after being cleared to play.
Conclusion:
Compared with the transtibial technique with cross-pin graft fixation, there is an increased risk of graft failure when performing autologous hamstring ACL reconstructions using the anteromedial portal technique with cortical suspensory fixation.
Keywords
The less invasive arthroscopic transtibial technique for anterior cruciate ligament (ACL) reconstruction was popularized in the early 1990s after comparable results to the open 2-incision technique were obtained. 17 However, with increased use, concerns arose regarding the ability of this technique to restore the native anatomy and function of the ACL. Although the procedure was highly effective in limiting anterior tibial translation as a result of re-establishing the anteromedial bundle, it often failed to restore the posterolateral bundle, resulting in residual rotatory instability. 4,8,15,27 As a result of these concerns, the anteromedial portal technique for preparation of the femoral tunnel was developed, 16 with the notion that drilling of the femoral tunnel independent of the tibial tunnel allows for improved access to the native origin. This ensures re-creation of both bundles of the ligament, restoring both anteroposterior as well as rotational stability. 18 Promising clinical results have been noted with the anteromedial technique, 26 and it was recently shown that transtibial femoral tunnel preparation increases the odds of repeat ipsilateral knee surgery. 13 In spite of the positive outcomes, apprehension regarding independent femoral tunnel drilling has come to light. In stark contrast to the above mentioned findings, results from the Danish knee ligament registry demonstrated an increased risk of revision after anteromedial compared with transtibial drilling of the femoral tunnel during primary ACL reconstruction. 25
In addition to tunnel preparation technique, increased attention has been given to the method of femoral-sided soft tissue graft fixation. At the advent of soft tissue ACL reconstruction, fixation was obtained with interference screws that often damaged the graft. Corticocancellous cross-pin fixation was subsequently designed to circumvent this issue, 11 and biomechanical studies showed it to be equivalent or even superior to interference screws. 1 However, there have been numerous complications associated with its use, including implant breakage with subsequent graft laxity 10 and lateral meniscal tearing, 12 intra-articular protrusion, 23 iliotibial band friction syndrome, 24 medial-sided pin prominence, 22 and stress fractures of the femur. 5 In light of these concerns, suspensory cortical fixation was developed and has been consequently adopted by many surgeons due to its ease of use. Nevertheless, increased tunnel widening with suspensory as compared with cross-pin fixation has been noted, 6,9 resulting in graft loosening with 2 to 3 mm of motion during physiologic loads. 21 The purpose of this study was to report a case series of 7 soft tissue graft failures over a short time period after a technical change was made from transtibial drilling with cross-pin fixation to anteromedial drilling with suspensory fixation. Given that there were only 2 graft failures with the prior technique over a 14-year period, we hypothesized that there would be an increased risk of ACL graft failure when using the anteromedial portal technique with cortical suspensory fixation.
Materials and Methods
Institutional review board approval was obtained for this study. From November 1998 to August 2012, all primary ACL reconstructions were performed by the senior author (W.N.L.) using quadrupled hamstring autograft tendons. The surgical procedure was as follows. An examination under anesthesia was initially performed not only to confirm the diagnosis of an ACL tear but also to assess for any concomitant injuries such as varus, valgus, or posterolateral instability. After a routine gracilis and semitendinosus harvest, the tendons were taken to the back table and sized and prepared accordingly. There was no pretensioning performed at this stage. Diagnostic arthroscopy was then carried out from an anterolateral portal, and any intra-articular pathology, such as meniscal tears or chondral lesions, were appropriately addressed. Following a minimal notchplasty allowing for visualization of the back wall and stump debridement, a tibial tunnel of equal diameter to the graft was drilled just posterior to the anterior horn of the lateral meniscus. Subsequently, with the knee in 90° of flexion, the appropriate size transtibial over the top positioner allowing for at least 1 mm of back wall was placed on the femur at the 10 and 2 o’clock positions. The beath pin was drilled out the thigh, and a femoral tunnel of the same diameter as the graft was created, measuring approximately 25 to 35 mm in length. The cross-pin drill guide (Biotransfix; Arthrex) was next placed on the femur, and a guide pin was drilled lateral to medial. After reaming of the outer cortex, the guide pin was used to pass a nitinol wire through the femur. The soft tissue graft was passed in routine fashion. After placement of the cross-pin, the graft was assessed for impingement in full flexion and extension. The knee was then cycled 16 times to eliminate creep and placed into full extension. A posterior drawer was applied, and an appropriate size soft tissue interference screw (Intrafix; Mitek) was placed into the tibial tunnel.
From September 2012 to October 2013, a change was made in the surgical technique for primary ACL reconstructions to suspensory fixation. Once again, after an examination under anesthesia and routine hamstring graft harvest, a standard diagnostic arthroscopy was carried out from an anterolateral portal. After addressing any intra-articular pathology, with the knee in 90° of flexion, a far anteromedial portal was made with an 18-gauge spinal needle. Care was taken to avoid iatrogenic injury to the medial femoral condyle while still allowing access to the 10 or 2 o’clock femoral tunnel position. A routine notchplasty was performed, and all soft tissue debris was removed from the ACL origin. The knee was then hyperflexed to 120° and the appropriate size anteromedial over the top positioner (Athrex) was placed, once again allowing for at least 1 mm of remaining back wall. A guide pin was subsequently advanced through the lateral femoral condyle and out through the anterolateral thigh. A low-profile reamer of the same diameter as the graft was placed over the pin and carefully advanced past the medial femoral condyle and PCL and reamed to approximately 25 mm. Next, a shuttle suture was placed onto the guide pin and retrieved through the anterolateral thigh, with the looped end placed within the femoral socket for later retrieval. The knee was then brought to 90° of flexion, and the tibial guide was placed just posterior to the anterior horn of the lateral meniscus. A solid core reamer of the same diameter as the graft was used to create the tibial tunnel. The suture shuttle was retrieved from the tibial tunnel, and the sutures attached to the suspensory device were placed through the suture shuttle and advanced into the femoral tunnel (RT Tightrope; Arthrex). Fluoroscopy was used to confirm that the button (RT Tightrope; Arthrex) flipped and was secured appropriately on the outer femoral cortex. After the button was secured, the graft was advanced into the femoral tunnel. Arthroscopic visualization was used to confirm lack of impingement in full flexion and extension, and the knee was cycled 16 times and tibial fixation was obtained as described.
Following ACL reconstruction, all patients are placed into a hinged knee brace and physical therapy was initiated according to the standard protocol. The goals for the first 2 weeks of therapy were to eliminate swelling, maintain full extension, and regain quad control. From weeks 2 to 4, the primary goals were to increase range of motion, increase total leg strength, and normalize gait. From weeks 4 to 6, therapy was aimed at normalizing activities of daily living, increasing functional capacity, and increasing strength. Following this, the next 4 weeks were directed at increasing functional strength and normalizing balance and proprioception. Subsequently, weeks 10 to 14 aimed to increase agility and speed of training, normalize strength, and increase muscular endurance. Finally, the principal goals from months 4 to 6 were to allow gradual return to athletic activity by commencing agility drills, running, and cutting. At the 6- to 9-month mark, patients were allowed to return to full activity or competition if they had quadriceps tone equal to the contralateral side and had passed all of the required functional performance tests. From the time of surgery to being cleared to participate in all activities without restrictions, patients were seen in the office every 4 to 6 weeks.
Results
From November 1998 to August 2012, a total of 465 primary ACL reconstructions were performed by the senior author (W.N.L.) using autologous hamstring tendons. Drilling of the femoral tunnel was performed via the transtibial portal, and femoral graft fixation was achieved with corticocancellous cross-pin fixation. During this 14-year time period, 2 graft failures (0.4% failure rate) were noted. The first failure occurred in a 19-year-old college football player who at the 6-month postoperative visit had significant quadriceps atrophy. Despite not being cleared to resume sporting activities, the patient went on to play basketball and retore his graft. The second failure occurred in a 32-year-old woman who reinjured her knee in a skiing accident 5 years after her initial procedure. Of note, the patient was completely asymptomatic and had no residual instability prior to the accident. Furthermore, none of the patients without graft failure had subjective or objective findings of rotational instability after transtibial reconstruction. There were no cases of medial-sided pin prominence or iliotibial band friction syndrome secondary to cross-pin use.
From September 2012 to October 2013, there were 69 primary ACL reconstructions performed by the senior author (W.N.L.) using an accessory anteromedial portal for the preparation of the femoral tunnel along with cortical suspensory femoral fixation. During this 13-month time period, 7 graft failures (10.1% failure rate) were noted (Table 1). These occurred in 5 male and 2 female patients, with a mean age of 18.8 years. All patients were highly competitive high school or college athletes and sustained their initial injuries while participating in their sport. They all underwent physical therapy prior to reconstruction to regain range of motion and quadriceps strength, and underwent surgery at an average of 4 weeks after injury. All 7 patients underwent uncomplicated ACL reconstruction with at the least a size 8 mm–diameter quadrupled hamstring autograft, and none of them had concomitant meniscal or chondral injuries. In addition, there was no compromise of the posterior wall in any cases. The standard postoperative physical therapy protocol, as previously described, was used to guide rehabilitation, and patients were cleared to return to competition at an average of 8.4 months postoperatively. Of the 7 cases, 6 sustained a retear of the graft within 2 weeks of being cleared for full competition, at an average of 8.8 days. The final patient retore the graft 10 months after being cleared to return to sport. In all 7 cases, graft failure occurred while the patient was competing in their respective sport. Furthermore, in each of the cases, graft failure occurred in the central portion of the graft, corresponding to a midsubstance tear.
Demographics of Patients With Rupture of Anteromedial Portal Autologous Hamstring ACL Reconstruction With Corticocancellous Cross-Pin Fixation a

a ACL, anterior cruciate ligament; F, female; M, male.
Discussion
Residual rotational instability after transtibial ACL reconstruction led to the development of the anteromedial portal technique for femoral tunnel preparation. Proposed advantages of the technique include unconstrained femoral socket placement, and for femoral cannulated interference screw fixation, ensuring parallel socket and screw angle. Furthermore, it is essential for all-inside ACL reconstructions using tibial sockets without full tunnels and for anatomic placement of the posterolateral socket during double-bundle reconstruction. 20 Favorable clinical outcomes have been achieved with this technique, 3 and in a recent series, ACL reconstruction using a femoral tunnel drilled through an anteromedial portal provided better rotational stability and anterior translation than drilling of the femoral tunnel using the transtibial technique. 14 It has also been recently shown that transtibial reconstruction increases the odds of ipsilateral knee surgery relative to the anteromedial portal technique after controlling for patient age and activity level, graft type, and meniscal pathology at the time of reconstruction. 13
In contrast to numerous reports demonstrating superior results with independent drilling of the femoral tunnel, the results from our institution demonstrate a higher failure rate with anteromedial versus transtibial drilling (10.1% vs 0.4%, respectively). Recent literature from the Danish Knee Ligament Reconstruction Register parallels our results and noted an increased risk of ACL revision surgery when using the anteromedial portal (5.16%) as compared with the transtibial portal (3.20%). 25 These results are similar to a prior meta-analysis comparing the 2 techniques in bone-tendon-bone ACL reconstructions (5.7% vs 2.3% revision rate). 2 In a biomechanical study, Xu et al 28 showed that an anatomically reconstructed anteromedial bundle had a significantly higher in situ force than a nonanatomically placed bundle. Authors have also shown a decrease in tunnel length 19 and an increased risk of posterior wall compromise with the anteromedial technique. 7 The authors of the Danish registry attributed the increased load seen by an anatomically reconstructed graft along with a steeper learning curve with technical failures as the source of their increased failure rate. 25
Similar to the evolution of femoral tunnel preparation, there has been a paradigm shift in the method of soft tissue graft fixation on the femur. Because of the potential risk of graft damage with interference screw fixation, corticocancelleous cross-pin fixation became popularized. 11 Although biomechanical testing demonstrated equivalent to superior results compared with interference screw fixation, 1 various complications have also been reported. These include implant breakage, 10 intra-articular protrusion, 23 and stress fractures of the femur 5 among others. Secondary to these concerns, the use of suspensory cortical fixation has dramatically increased over the past 5 years. However, at our institution, there were no cases of medial-sided pin prominence or iliotibial band friction syndrome. Although suspensory fixation has become popular among many surgeons because of its ease of use and the avoidance of complications associated with interference screw and cross-pin fixation, it is not without its own set of problems. Since the site of fixation is more distant from the intra-articular portion of the graft, there is an increased risk of graft motion with successive tunnel widening. 9 This may subsequently predispose the reconstructed knee to increased pathologic motion during physiologic loading, 21 increasing the risk of graft failure and damage to the articular cartilage.
As previously mentioned, 2 graft failures (0.4% failure rate) were noted over a 14-year period when ACL reconstructions were performed with transtibial drilling of the femoral tunnel along with cross-pin femoral soft tissue graft fixation. None of the remaining patients on whom the transtibial technique was performed demonstrated subjective or objective findings of rotational instability, one of the most prevalent criticisms regarding the technique. Of the 2 revisions in the cohort of 465 transtibial patients, the first rupture was the result of premature return to sport, while the other patient reruptured the graft in a skiing accident. After changing the operative technique to include drilling of the femoral tunnel from the anteromedial portal along with suspensory cortical fixation, there were 7 reruptures in 69 patients (10.1% failure rate) over a 13-month period.
We performed a second-look arthroscopy during a separate procedure on a 36-year-old woman who had undergone anteromedial ACL reconstruction with cross-pin fixation 6 months prior but did not rupture her graft. Although the majority of the graft was intact, there was significant fraying of the lateral fibers of the graft (Figure 1). This was likely the result of impingement of the graft on the inferior aspect of the lateral wall. However, during the initial procedure, the lateral wall was debrided so that after graft passage, there was no impingement of the graft after careful examination in both full flexion and extension. It is interesting to note that of the 7 graft failures, 6 occurred within the first 2 weeks that patients were cleared to return to all sporting activities. All 7 graft failures underwent revision ACL reconstruction by the senior author, and all were noted to have a midsubstance tear with a component of lateral wall hypertrophy at the time of their second surgery. Although all patients demonstrated objective signs of healing on physical examination along with successful completion of functional evaluation tests, all failures likely had fraying of the graft similar to that described above, which predisposed them to rerupture. Given that 2 variables were changed, it is difficult to isolate the exact root of the drastically increased failure rate. We believe that the cause is multifactorial and a combination of both technical changes. While neither cross-pin fixation nor suspensory fixation is aperture fixation, the distance from the point of fixation to the intra-articular portion of the graft is significantly more with suspensory fixation, leading to increased graft motion. Our hypothesis as to the increased failure rate is as follows. Since the femoral tunnel is placed further down at the 2 or 10 o’clock position with the anteromedial technique, the graft is significantly closer to the lateral wall than when drilled transtibial. Even if no impingement is noted intraoperatively, the graft is situated within millimeters of the wall. As a result of graft motion and tunnel widening associated with suspensory fixation, there is movement of the graft into a position of lateral wall impingement that may be exacerbated by lateral wall hypertrophy. Repetitive impingement subsequently results in fraying of the graft fibers, causing an alteration in its mechanical properties and resulting in decreased load to failure. While this may not be apparent on clinical examination and functional testing, graft rupture occurs when patients return to high-demand pivoting activities.
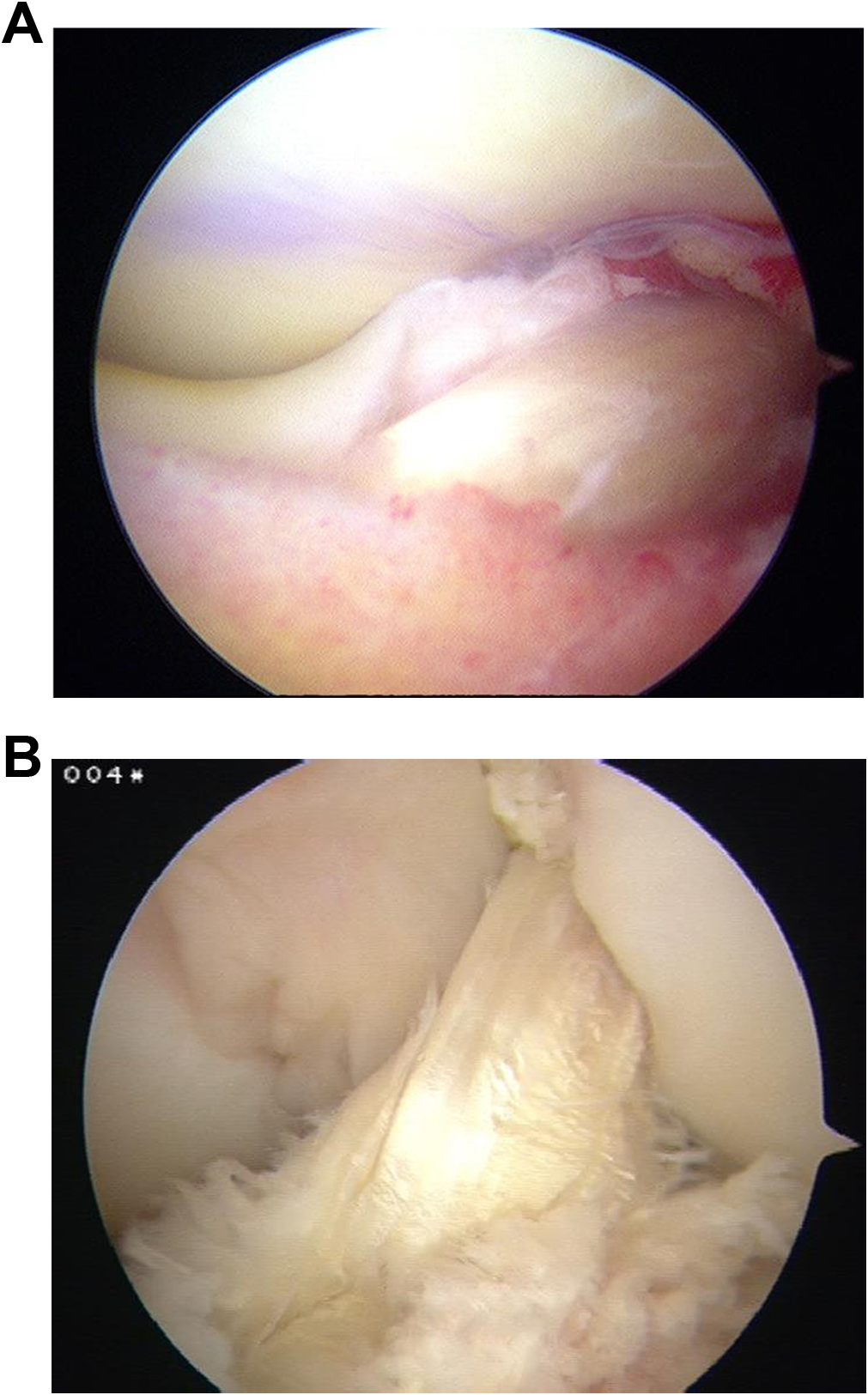
Images taken during (A) initial surgery and (B) second-look arthroscopy 6 months later on a patient who underwent anteromedial anterior cruciate ligament reconstruction with suspensory femoral soft tissue fixation. Significant fraying of the anterolateral fibers of the graft was noted at second surgery.
As a result of these failures, we have since returned to transtibial drilling of the femoral tunnel with corticocancellous cross-pin fixation. Although independent drilling of the femoral tunnel affords increased freedom in location, we believe that a properly performed transtibial ACL reconstruction restores anteroposterior as well as rotational stability with equal success. Further biomechanical studies are needed to precisely define the forces seen by the graft with the anteromedial portal technique.
Conclusion
The evolution of anatomic ACL reconstruction has led to the development of the anteromedial portal technique for drilling of the femoral tunnel. In addition, concerns regarding interference screw fixation and corticocancellous cross-pin fixation of soft tissue grafts have led to the development of suspensory cortical fixation. However, we caution against the use of the 2 in combination, as there has been a significant increase in graft failures at our institution with this technique. We hypothesize that as a result of graft motion and tunnel widening associated with suspensory fixation, there is movement of the graft into a position of impingement on the lateral wall. Subsequently, there is fraying of the fibers of the graft, decreasing its load to failure, and resulting in early graft rupture when patients return to full sporting activities.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.