
Abstract
Background:
Labral tears often occur in the same quadrant of the acetabulum at a small depression previously referred to as the psoas valley. Understanding the anatomic variations of this depression could help us understand the etiology of labral tears.
Purpose:
To describe the location and dimensions of the depression located in the anterosuperior acetabular rim. The hypothesis was that the location of this depression would be consistent with the common location of acetabular labral tears described in the literature.
Study Design:
Controlled laboratory study.
Methods:
A total of 240 pelvic specimens were divided into 2 groups (n = 120 for each) according to age (younger age group: 21.36 ± 3.12 years [range, 14-24 years]; older age group: 42.30 ± 10.27 years, [range, 25-60 years]).Specimens were also categorized based on sex (mean age: 31.93 ± 12.31 years [male]; 32.08 ± 13.66 years [female]) and race (mean age: 31.45 ± 13.16 years [black]; 32.57 ± 12.82 years [white]). The depth and width of the acetabular depression were measured using a digital caliper, and the location was measured using a goniometer.
Results:
The psoas valley was observed in every specimen and was located in the anterosuperior quadrant of the acetabulum. Its depth was significantly greater (P < .001) in males (5.35 ± 1.60 mm) than in females (3.95 ± 1.31 mm). The width of the psoas valley was also greater (P < .001) in males (29.39 ± 3.98 mm) than in females (24.49 ± 4.80 mm). There were no differences in size or location of the depression between races or age groups. The psoas valley was located between 3.92 ± 0.42 o’clock anteriorly and 2.12 ± 0.77 o’clock posteriorly.
Conclusion:
The differences observed in the study data are believed to be a result of the different anatomic morphologies of the pelvis in males and females. This loss of bony support, caused by the depression, could be the underlying cause of weakening of the acetabular labrum as people age.
Clinical Relevance:
The loss of bony support in the anterosuperior acetabular depression could contribute to the labral tears that commonly occur in this area. Understanding the normal anatomy of this area could be important in determining the risk of labral tears as well as treatment options.
Keywords
The acetabular rim has been investigated in computed tomography scan reconstructions to compare the hemispheric implants used in total hip arthroplasty with the native acetabular rim morphology. 17 In previous studies by Vandenbussche et al, 16,17 this depression in the anterior acetabular ridge was described as the psoas valley due to the involvement of the iliopsoas tendon in this region. The psoas valley acts as a groove for the iliopsoas muscle as it tracts over the anterior of the acetabular rim. This anterosuperior location of the psoas valley is an area commonly associated with acetabular labral pathologies.
Previous studies by our research team have noted a depression in the anterosuperior quadrant of the acetabulum that may be linked to labral abnormalities. To the best of our knowledge, the psoas valley has been mentioned in only 2 previous studies describing the morphology of the acetabular rim and its contribution to total hip arthroplasty. 16,17 The shape of the psoas valley has not been defined due the complexity of the acetabular orientation and architecture. 17 Understanding the anatomic properties of this depression can help clinicians to further understand the mechanical structure and demand of this important area of the acetabular rim.
The etiology of labral tears has been an area of increased investigation in the past decade. The leading cause historically has been nontraumatic events of varying intensity, but Lage et al 9 have described 4 categories of labral tears: traumatic, congenital, degenerative, and idiopathic. Recent studies have also shown that a majority of patients with labral tears had an osseous dysmorphism consistent with femoroacetabular impingement. 6,14,18 Labral tears most commonly occur in the anterosuperior portion of the acetabular rim. 3,5,13 This area of the acetabulum has been described as an at-risk zone due to its relative hypovascularity, inferior mechanical properties, and higher mechanical demands. 11 The labrum is wider and thinner in the anterior region of the acetabulum and, as a result, is more fragile in this area. 7,8 The prevalence and significance of labral tears are unclear, as studies have shown that abnormalities and tears without hip pain were seen to increase with age, 1,2,10 suggesting that labral abnormalities are a natural part of aging.
The purposes of this study were to quantify the dimensions and location of the psoas valley in skeletal specimens and determine the variation across ages, sexes, and races. We hypothesized that the psoas valley would be located in the anterosuperior quadrant of the acetabulum and be present in all individuals studied. Our secondary hypotheses were that the psoas valley would be larger in the male population and larger in the older population, which could help future studies to explain the increased incidence of labral tears seen in older populations. The increase in size of the psoas valley could be due to a number of factors, including bone erosion over time from the iliopsoas tendon or as a result of persistent microtrauma from day-to-day physical activity. An improved understanding of this acetabular morphology could give us a better knowledge base about acetabular anatomy and help us better understand the pathophysiology underlying acetabular labral tears in the future.
Materials and Methods
Sample Selection
We obtained preserved human pelvises (n = 240) from the Hamann-Todd Collection located at the Museum of Natural History in Cleveland, Ohio, USA. The specimens used for our study were between the ages of 14 and 60 years. The cutoff age used to distinguish between young and old specimens was 24 years. This cutoff was used as a way to group our sample population so that we would be able to have equal distributions of sex and race. Specimens older than 60 years were more likely to have osteoarthritis and calcification that could affect the anatomy of the acetabular rim, while specimens younger than 14 years were observed to have an incomplete development of the acetabulum. The specimens were classified on the basis of age (young or old), male or female sex, and race (white or black), and then further classified into 8 demographic categories (eg, young, white, female; and young, black, male) (Table 1). The pelvises were inspected for abnormalities in anatomy as well as full development of the acetabulum.
Location of the Psoas Valley a

a Location varied significantly only between the male and female populations at the anterior boundary. Values are expressed as mean ± SD.
b Statistically significant difference (P < .05).
Psoas Valley Measurement
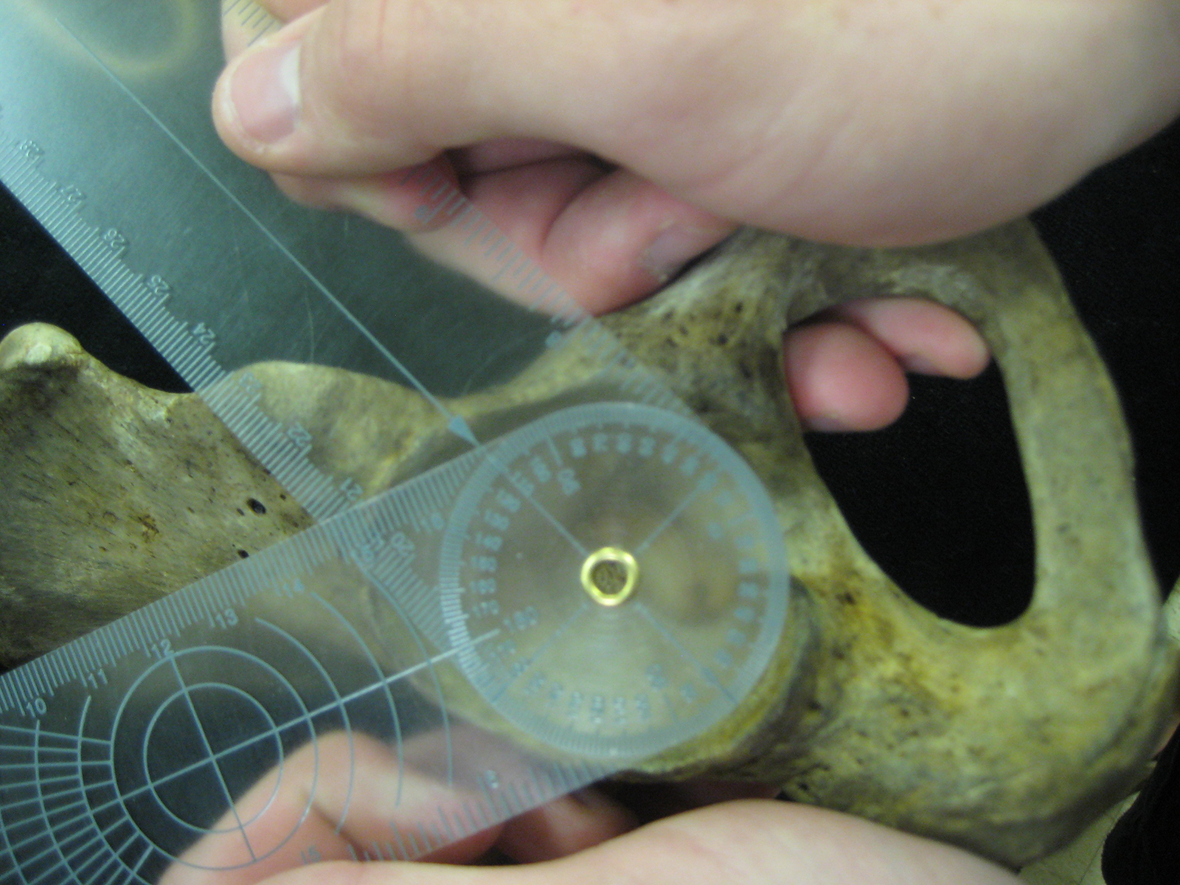
The depth of the psoas valley was measured using a 6-inch digital caliper. Electronic digital calipers were used to take advantage of the unique ex vivo samples that were available for this study. This unique technique was used to compare physical ex vivo measurements to measurements taken from radiographs and magnetic resonance imaging techniques present in the literature. A ruler was placed lateral to the 2 bony peaks that border the psoas valley on the acetabular rim, and the digital caliper was used to measure the depth and width of recession of the acetabular rim (Figure 1). The measurements were completed multiple times, and the depth and width recorded were a mean of all measurements performed.

Measurement process, as shown from the superior aspect of the right acetabulum. Depth of the psoas valley was measured using a digital caliper. The depth was defined as the distance between the ruler and the deepest point of the valley. The width was defined as the distance between the 2 peaks on each side of the valley.
Location Measurement
The location of the psoas valley was measured using a goniometer placed directly over the acetabulum, with the center of the acetabular notch located at 0°. The degree measurements were then converted to a clockface position, with 3 o’clock at the most anterior point of the acetabulum (Figure 2).
Location measurement process, as shown from the lateral aspect of the right acetabulum. The location of the psoas valley was determined using a goniometer. The degrees, on a 360° scale, of each of the peaks was recorded and then converted into a clockface position.
Statistical Analysis
Independent 2-tailed t tests were used to determine significant differences between groups of specimens (P = .05), and comparisons between all groups were analyzed using post hoc Bonferroni with 95% confidence intervals. Analyses were performed using SPSS 14.0 (IBM Inc) for Windows. All data are presented as mean ± standard deviation unless otherwise noted.
Results
Psoas Valley Depth and Width
Across all specimens, the psoas valley had a mean depth of 4.64 ± 1.62 mm and a mean width of 26.94 ± 5.03 mm. The mean depth (5.35 ± 1.60 mm vs 3.95 ± 1.31 mm) and width (29.39 ± 3.98 mm vs 24.49 ± 4.80 mm) of the psoas valley were significantly larger (P < .001) in the male population (n = 120) compared with the female population (n = 120) (Figure 3). The depth and width of the psoas valley did not show any significant variations when compared across age and racial groups.

The depth and width of the psoas valley varied significantly between males (open bars) and females (closed bars). Data are shown as mean ± SD.
Location of the Psoas Valley
The psoas valley was located in the anterosuperior quadrant of the acetabulum, with a mean location of 3.92 ± 0.42 o’clock anteriorly and 2.12 ± 0.77 o’clock posteriorly. The anterior boundary of the psoas valley was significantly more anterior in males (P < .001) than in females, but the posterior boundaries did not show any significant difference in location between sexes (P > .05) (Table 1). There were no significant differences (P > .05) in location when compared across age and racial groups.
Discussion
There is still little known about the etiology of labral tears, but better knowledge of the variations in the anatomy of the anterosuperior acetabular rim could help us better understand this important pathology. The psoas valley was observed in all specimens and was located in the anterosuperior quadrant of the acetabulum. The depth and width of the psoas valley measured on ex vivo specimens were very similar to previous measurements of in vivo specimens. 16,17 Our study quantified the dimensions of the psoas valley from ex vivo specimens and compared dimensions across different sexes, races, and ages. We also investigated the location of the psoas valley in an effort to link this loss of bony support in the acetabulum to acetabular labral tears. Congruent with our hypothesis, the psoas valley was similar in depth and width across races, but the male population showed a deeper and wider psoas valley than the female population. Contrary to our hypothesis, the depth and width of the psoas valley did not change with the age of our specimens. The location of the psoas valley varied only between males and females, and only at the anterior boundary. The location of the psoas valley described in our study is the same location in which labral tears are commonly seen in the population.
The depth of the psoas valley observed in our population was similar to measurements by Vandenbussche et al. 16,17 The results of our study showed that the psoas valley depth and width were larger in males. These results disagreed with 1 study by Vandenbussche et al 17 that found no significant sex-related variance in the depth of the acetabulum. However, in another study performed by Vandenbussche et al, 16 there was a significant sex-related variance in the depth of the acetabulum.
The prevalence of labral tears in the older population led us to hypothesize that there could be changes in the morphology of the psoas valley overtime. Our findings were contrary to our hypothesis and showed that the dimensions of the psoas valley did not vary with the age of the specimens. These findings coincided with a study by Vandenbussche et al, 17 which found that the dimensions of the psoas valley were not related to age. The posterior boundary of the psoas valley was not affected by the sex of the specimen, but the anterior boundary of the psoas valley was located more anteriorly in males. Our study showed that the male psoas valley was in fact larger, but this does not account for the results showing that it is only in the anterior direction. Previous work by Vandenbussche et al 16 showed that the female acetabulum is on average more retroverted when compared with that of males. The orientation of the female acetabulum causes the iliopsoas muscle to fall more posteriorly on the acetabulum, and as a result, the reactive formation of the acetabular rim lies more posterior on the acetabulum. The more anteriorly facing male acetabulum causes the opposite effect on the psoas valley. The orientation of the acetabulum could be the underlying cause of the different anterior locations of the acetabulum that are seen when comparing males and females.
The cause of acetabular labral tears in the human hip joint is still much debated. The anterosuperior quadrant of the labrum has been described as the most common area for acetabular labral tears due to multiple contributing factors. This area has been shown to have inferior mechanical properties, higher mechanical demands, and relative hypovascularity. 11,12 Studies have shown that the anterior aspect of the labrum has a rather marginal attachment to the acetabular cartilage with an intra-articular projection, compared with the continuous attachment seen in the posterior aspect of the labrum. The anterior chondrolabral transition zone is sharp and abrupt compared with the gradual posterior transition. This abrupt transition increases the risk of labral tear in this area and has been described to some extent as the so-called “watershed lesion.” The acetabular rim morphology in this area could give clues to a patient’s risk of developing a labral tear. Lage et al 9 described 4 categories of labral tears, most notably traumatic injuries. Recent studies have shown that labral tears are commonly due to traumatic events (range, 19%-55%) of varying intensity. 4,5,9,15 Traumatic injuries have been reported to involve traction injuries of the labrum by the intra-articular portion of the iliopsoas tendon as it transverses the psoas valley. 5,9 The variation of the dimensions of the psoas valley could increase a patient’s risks of labral tears. All specimens in our population were observed to have a psoas valley in this area of the acetabulum. This trade-off for stabilization of the iliopsoas muscle could result in weakening of the labrum in this area.
The goals of our study were to describe the psoas valley and compare our findings across different sexes, ages, and races. We were still limited by the availability of subjects for our study. All subjects were from northern Ohio and had died in the early 19th century. More studies need to be done on a wide variety of populations to either strengthen or refute our findings. Our data were also collected by multiple measurements by a single individual, which could be a cause of bias in the data collected. However, the results of our study confirmed the results of previous studies about the dimensions and location of the psoas valley. 16,17 We showed that studies using imaging on in vivo specimens achieve the same results as measurements on ex vivo specimens. The psoas valley dimensions and location only varied between sexes, and the version of the acetabulum could be the underlying cause. Acetabular labral tears occur in the same area of the acetabulum, and this possible lack of bone support could be the underlying cause, but future studies relating the dimensions of the psoas valley of patients presenting with labral tears to those without labral pathologies and the biomechanics of psoas valley are necessary to fully understand labral tear etiology.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study is provided by the University of Michigan Biomedical Science Research Program.
Acknowledgment
The authors thank Lyman M. Jellema from the Hamann-Todd Human Osteological Collection at the Cleveland Museum of Natural History for providing access to the skeletal specimens.