
Abstract
Background:
Medial meniscus root tear (MMRT) is a recently recognized yet frequently missed meniscal tear pattern that biomechanically creates an environment approaching meniscal deficiency.
Hypothesis/Purpose:
The purpose of this study was to assess the effect of MMRT on tibiofemoral kinematics and arthrokinematics during daily activities by comparing the injured knees of subjects with isolated MMRT to their uninjured contralateral knees. The hypothesis was that the injured knee will demonstrate significantly more lateral tibial translation and adduction than the uninjured knee, and that the medial compartment will exhibit significantly different arthrokinematics than the lateral compartment in the affected limb.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Seven subjects with isolated MMRT were recruited and volumetric, density-based 3-dimensional models of their distal femurs and proximal tibia were created from computed tomography scans. High-speed, biplane radiographs were obtained of both their affected and unaffected knees. Moving 3-dimensional models of tibiofemoral kinematics were calculated using model-based tracking to assess overall kinematic variables and specific measures of tibiofemoral joint contact. The affected knees of the subjects were then compared to their unaffected contralateral knees.
Results:
Affected knees demonstrated significantly more lateral tibial translation than the uninjured contralateral limb in all dynamic activities. Additionally, the medial compartment displayed greater amounts of mobility than the lateral compartment in the injured limbs.
Conclusion:
This study suggests that MMRT causes significant changes in in vivo knee kinematics and arthrokinematics and that the magnitude of these changes is influenced by dynamic task difficulty.
Clinical Relevance:
Medial meniscus root tears lead to significant changes in joint arthrokinematics, with increased lateral tibial translation and greater medial compartment excursion. With complete root tears, essentially 100% of circumferential fibers are lost. This study will further our knowledge of meniscal deficiency and osteoarthritis and provide a baseline for more common forms of medial meniscal injuries (vertical, horizontal, radial), with various degrees of circumferential fiber function remaining.
Arthroscopic meniscal surgery (Current Procedural Terminology [CPT] codes 29881, 29880) is the most common procedure reported in the orthopaedic literature. 6,10,12 While an injury to the meniscus most commonly occurs in the main body of the tissue, tears to the posterior root are becoming increasingly recognized in orthopaedic practice. 1,14 These injuries have the potential to trigger a debilitating course of osteoarthritis, and patients presenting with this injury have been found to exhibit a rapid progression of osteoarthritis in the injured knee. 9,11,16 Additionally, posterior medial meniscal root tears (MMRTs) are frequently misdiagnosed and left untreated. 14
Of the literature, most work examining MMRT focuses on treatment options and less on those left untreated. Few studies have examined the biomechanical implications of MMRT. In vitro work has found cadaveric knees to exhibit decreased contact area and increased pressure after a tear to the posterior root of the medial meniscus. 15,17 Additionally, cadaveric knees demonstrate increased lateral tibial translation and varus alignment with MMRT. 2 Surgical repair has been shown to restore normal loading conditions in an in vitro setting. 2,15,17 There are no in vivo studies examining the kinematics resulting from an untreated medial meniscal root tear.
The purpose of this study was to examine the in vivo knee kinematics and arthrokinematics (kinematics of the articulating joint surfaces) resulting from an untreated tear to the posterior root of the medial meniscus during 3 different activities. We hypothesize that the injured knee will demonstrate significantly more lateral tibial translation and adduction than the uninjured knee during all 3 activities. Additionally, we hypothesize that the medial compartment will exhibit significantly different arthrokinematics than the lateral compartment in the affected limb.
Methods
Subjects
Nine subjects with recent but not acutely symptomatic, magnetic resonance imaging–identified MMRT participated in this institutional review board–approved study. Subjects were recruited for the study if they showed the presence of an isolated posterior horn MMRT seen on magnetic resonance imaging and exhibited minimal joint space changes in the medial compartment and normal joint space in lateral compartment on plain radiographs compared with the uninjured, contralateral limb (flexion weightbearing, lateral merchant, and long-standing cassette radiographs were obtained in all patients). All participants were free from any other lower body injury and exhibited normal joint alignment (within 3° varus) that was symmetrical to the uninjured, contralateral limb. Data from 2 subjects were discarded because of limping during testing and excessive dynamic joint space narrowing (seen in dynamic testing but not on plain films), leaving 7 subjects for analysis (6 females, 1 male; mean age, 57.4 ± 9.3 years).
Kinematic Testing
Kinematic testing consisted of 3 activities: level walking, decline walking, and squatting. Each task was repeated for 3 trials, and both the injured and contralateral limbs were tested. Gait trials were performed with an instrumented treadmill (Bertec Corp) that was set to a velocity of 1.0 m/s for both level and decline walking. For squatting trials, subjects were instructed to bend their knees as far as possible without significant pain. One of the subjects was unable to bend their knee for all of 25° to 70° of flexion, so 6 subjects were used for the squatting trials to capture a large range of flexion.
Testing was performed within the dynamic stereo x-ray (DSX) system, which uses biplane radiography during dynamic trials to characterize joint motion. The lab setup for each activity can be seen in Figure 1.

Laboratory setup: high-speed, biplane radiography system, including dual-belt, instrumented treadmill and customizable safety railings. (Top left) Stacked configuration for level walking; (top right) oblique configuration with treadmill inclined and treads running in reverse for decline walking; (bottom left) horizontal configuration for knee-bending exercise.
Dynamic stereo x-rays were generated using a protocol of 90 kV, 160 mA (or less, depending on subject size), with 1-ms pulsed exposures. Images were acquired for either 1 second at 100 Hz (gait) or 2 seconds at 50 Hz (squat), using 40-cm image intensifiers (Thales Inc), coupled to 4-megapixel, 14-bit digital video cameras (Phantom 10; Vision Research Inc), with a source-to-detector distance of 180 cm. The effective radiation exposure for all dynamic imaging trials (estimated using direct entrance exposure measurements and PCXMC dose estimate software; STUK–Radiation and Nuclear Safety Authority, http://www.stuk.fi/pcxmc) was less than 0.2 mSv. Bilateral computed tomography (CT) scans added approximately 1 mSv (estimated from CT scanner DLP reports), for a total of 1.2 mSv. This is considerably less than the average exposure of approximately 3 mSv per year from natural sources, such as cosmic rays and radon gas.18(pp53-55)
Data Processing
In addition to kinematic testing, all subjects underwent a bilateral CT scan using a GE LightSpeed CT Scanner (LightSpeed Pro 16; GE Medical Systems) with a slice spacing of 1.25 mm and a field of view that extended from 15 cm below to 15 cm above the joint line. Single slices through the hip and ankle centers were also acquired to enable definition of anatomic coordinate systems for the tibia and femur. The scans were then segmented with Mimics (Materialise Inc) to create patient-specific bone models of the femur and tibia using a previously described method. 5,19 To enable region-specific analyses, subregions of the articulating surfaces were defined from the 3-dimensional (3D) surface models, as shown for the femoral condyles in Figure 2 and tibial plateau in Figure 3.

Regions for the medial femoral condyle divide the articular surface into 3 medial-lateral zones and 5 longitudinal zones, defined by planes at 20° increments relative to a sphere fitted to the condyle.
The medial and lateral tibial plateaus are both divided into 3 medial-lateral regions and 5 anterior-posterior regions. These regions are then subdivided into 9 subregions. The figure also shows the defined anatomical axes.
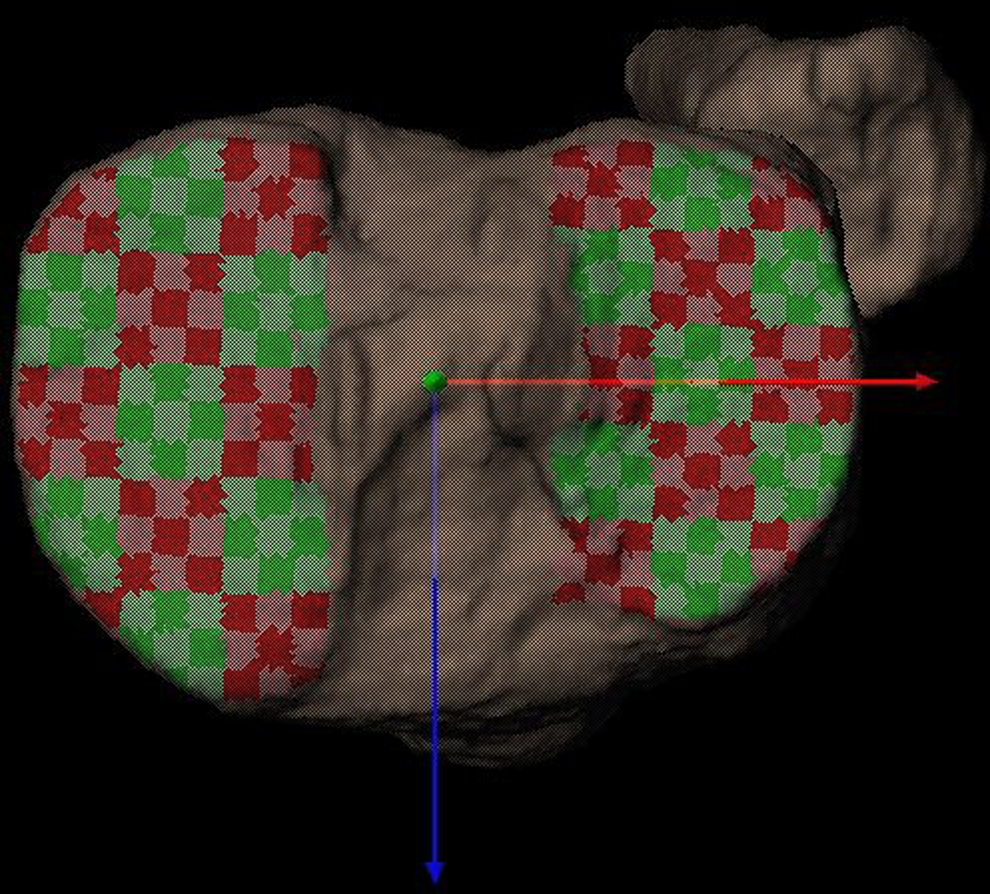
The segmented bone models were then matched to the x-ray images gathered during kinematic testing using a computerized, model-based tracking technique. 7,8 Briefly, custom software created a virtual reconstruction of the testing environment, in which the segmented bone models were manually positioned via ray-traced projections of digitally reconstructed radiographs (DRRs). These manually placed DRRs were then used as an initial guess for the computer to automatically manipulate the bone to a position that maximized the correlations between the DRRs and actual radiographs from kinematic testing. This process was repeated for all frames in a trial. The location and orientation of the femur and tibia were then projected into 3D space, and their motions and positions relative to one another were calculated. Figure 4 shows the final product, with a representative joint contact analysis from a single-level walking trial. The performance of this system has been extensively validated, with precision in the order of 0.1 mm for in vitro testing 8 and averaging 0.6 deg/0.5 mm for in vivo tibiofemoral kinematics during running. 4

Representative joint contact analysis from a single trial. The image shows affected and unaffected knees opened to compare joint contact patterns. Color maps demonstrate instantaneous joint space (bone-to-bone distances), while black dots demonstrate instantaneous location of joint contact (location of closest bone-to-bone distance), and white lines show the contact path throughout the chosen range of movement.
Kinematic measures were calculated as motion of the tibia relative to the femur, as previously described. 20 Translations were defined as the 3D distance between the centers of the tibial and femoral coordinate systems, and were separated into anterior-posterior, medial-lateral, and superior-inferior directions. Rotations were similarly calculated of the tibia relative to the femur, and included flexion-extension, abduction/adduction, and external-internal rotation.
Arthrokinematic parameters were determined for the medial and lateral compartments of both knees, as previously described. 5 The instantaneous point of closest contact was calculated for both compartments as the distance-weighted centroid of the region of closest proximity between the femoral and tibial subchondral bone surfaces. Anteroposterior (AP) excursion was defined for both medial and lateral knee compartments as the distance along the AP axis between the most anterior and posterior tibial contact points. Similarly, mediolateral (ML) excursion was defined as the distance along the ML axis between the most medial and lateral tibial contact points over the same time interval. Contact path length was calculated as the sum of frame-to-frame differences in contact point location.
Statistics
Limb-to-limb kinematic differences and changes over time or flexion angle were assessed with SPSS software using a 2-way repeated-measures analysis of variance (ANOVA). Both gait trials were assessed over time, using the interval from 0 to 0.2 seconds following heelstrike (corresponding to the loading response phase of gait). While data were collected at 100 frames/s, comparisons were made at 0, 0.06, 0.1, 0.16, and 0.2 seconds after heelstrike. Squatting trials were assessed as a function of flexion angle, from 25° to 70° (the maximum range of data available across all subjects), and comparisons between limbs were made at 25°, 35°, 45°, 55°, and 65°. If the ANOVA reported a significant limb-to-limb difference (P < .05) or a significant limb-by-time/flexion angle interaction (P < .10), post hoc paired t-tests were performed at all time points/flexion angles (with Holm corrections for multiple pairwise comparisons 13 ) to clarify areas of significance. Arthrokinematic differences were assessed using paired t-tests between the medial and lateral compartments of the affected limb (P < .05).
Results
Tibiofemoral Kinematics
During level walking, lateral tibial translation was greater in the meniscus-injured limb relative to the contralateral, uninjured limb, as shown in Figure 5 (repeated-measures ANOVA; P = .035). Specifically, there were greater amounts of lateral tibial translation in the affected limb at 0.15 and 0.20 seconds after heelstrike (post hoc t-tests; P = .017 and P = .018, respectively).

Lateral translation of the tibia with respect to the femur during level walking. Error bars represent standard deviation. !, trending differences (P < .05). The medial meniscus root tear (MMRT) knee is consistently more laterally translated throughout the range of motion than the contralateral limb.
Results for decline walking were similar to those for level walking, with significantly more lateral translation in the affected limb (repeated-measures ANOVA; P = .015), as seen in Figure 6. Post hoc testing revealed that the affected limb demonstrated more lateral tibial translation at heelstrike and 0.05 and 0.1 seconds after heelstrike (post hoc t-tests; P = .008, P = .035, and P = .019, respectively).

Lateral translation of the tibia with respect to the femur during decline walking. Error bars represent standard deviation. *Significant differences between limbs (P < .01); !, trending differences (P < .05). Again, the medial meniscus root tear (MMRT) knee is consistently more laterally translated than the contralateral limb throughout the range of motion, and the differences are significant shortly after heelstrike.
Squatting also induced significantly more lateral tibial translation in the MMRT limb (repeated-measures ANOVA; P = .039), as seen in Figure 7. Significant differences between limbs are seen at 65° of flexion (post hoc t-test; P = .01). Additionally, the MMRT limb is more adducted than the contralateral limb throughout the range of motion (Figure 8), though these differences did not reach statistical significance (repeated-measures ANOVA; P = .155). No other kinematic parameter reached statistical significance in any of the other activities.

Lateral translation of the tibia with respect to the femur during squatting. Error bars represent standard deviation. *Significant differences between limbs (P < .01). Once again, the affected limb exhibits significantly more lateral tibial translation than the contralateral limb.

Abduction/adduction of the tibia with respect to the femur during squatting. Error bars represent standard deviation. Differences between limbs were not statistically significant, but the medial meniscus root tear (MMRT) limb is consistently more adducted than the contralateral limb.
Arthrokinematics
There were no arthrokinematic differences between the affected and contralateral limbs in any of the tested activities. In the affected limb, however, the medial compartment was found to display more mobility than the lateral compartment. These differences are illustrated in Table 1. Specifically, during level walking, the medial compartment exhibited significantly greater total contact path length when compared with the lateral compartment (P = .021). During decline walking, the medial compartment exhibited significantly more AP excursion (P = .008) and contact path length (P = .03) than the lateral compartment.
Compartmental Differences in Arthrokinematics (AP Excursion, ML Excursion, and Total Path Length) in the MMRT Limb in the 3 Activities a
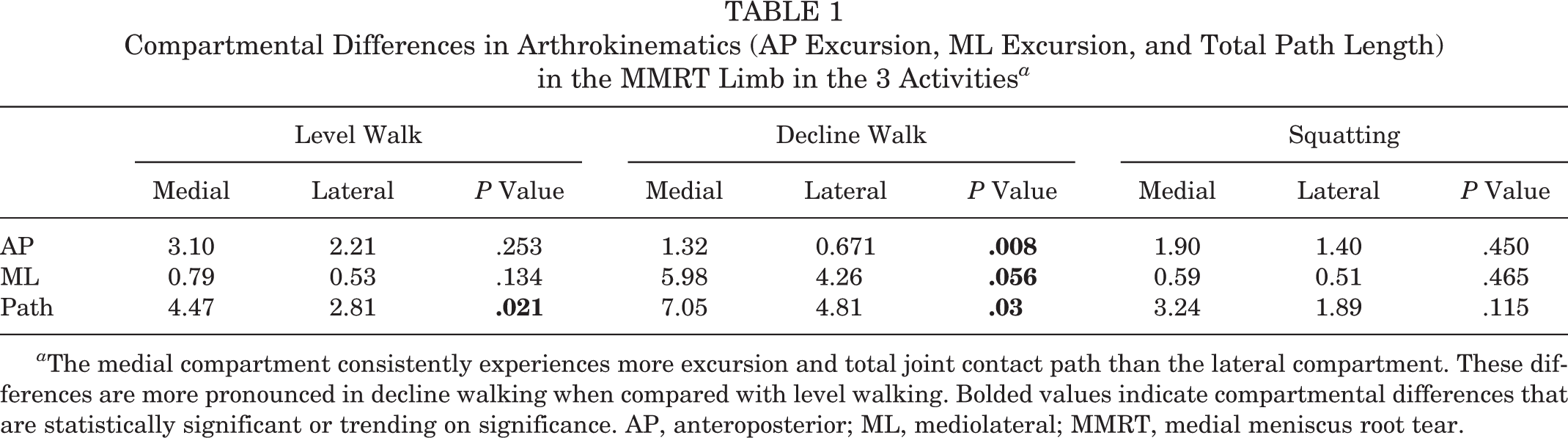
a The medial compartment consistently experiences more excursion and total joint contact path than the lateral compartment. These differences are more pronounced in decline walking when compared with level walking. Bolded values indicate compartmental differences that are statistically significant or trending on significance. AP, anteroposterior; ML, mediolateral; MMRT, medial meniscus root tear.
Discussion
The most notable result of this study is that all activities elicited lateral tibial translation in the affected limb. This was also found in the in vitro cadaver studies. Allaire et al 2 attributed this lateral tibial translation to the lack of a meniscal buttress against the medial femoral condyle, which allows for the tibia to translate laterally relative to the femur. This explanation appears to hold true in vivo. Although it was not found to be significant, the magnitude of lateral tibial translation and arthrokinematic differences were greater in decline walking when compared to level walking. This may suggest that joint instability as a result of MMRT is task dependent.
Allaire et al 2 also found increased adduction resulting from MMRT, specifically at 30° of flexion. This adduction is attributed to the combination of lateral tibial translation with the loss of the medial meniscal spacer between the femur and tibia. This was mirrored in vivo, with the affected limb demonstrating increased adduction throughout the range of flexion during the squatting activity. MMRT results in the loss of hoop stresses, causing the observed varus angulation and a previously undescribed lack of dynamic restraint to adduction during loading. These changes may produce a decrease in dynamic medial compartment joint space and allow the knee to rotate into adduction during loading. This varus alignment resulting from MMRT could indicate the presence of early degenerative changes in the articular cartilage that are not yet visible on weightbearing radiographs.
There are notable differences between the present study and previous in vitro findings. Allaire et al 2 found increased external tibial rotation, which does not appear in vivo. This may be attributed to static versus dynamic loading conditions. In vitro studies looking at MMRT apply static loads to cadaveric knees at various flexion angles and thus examine the passive properties of the MMRT knee. These testing conditions are unable to account for the changes in muscle activation and joint motion seen in dynamic activity. Muscle contraction during dynamic activities may stabilize the MMRT joint and restrict tibial rotation.
The increased external rotation seen in vitro may dynamically manifest itself as increased joint contact in the medial compartment compared with the lateral compartment in knees with MMRT. These differences in arthrokinematics between compartments may suggest that the medial meniscus plays a large role in constraining femoral condyle motion on the tibial plateau rather than solely dissipating forces. Additionally, the lack of a significant difference between the overall AP translation of the tibia in the MMRT versus contralateral knees illustrates that some traditional measures of kinematics may be insufficient to describe the changes that occur with MMRT. The lack of meniscal restraint in the medial compartment seen with MMRT may produce a more complex motion in which the tibia rotates about the intact lateral compartment.
Lateral tibial translation and alterations in arthrokinematics appear to be emphasized in more difficult tasks, which again indicates that joint instability resulting from MMRT may be task dependent. Research has shown that the medial meniscus plays a significant role in restricting anterior tibial translation and tibial rotation. 3 Decline walking results in more shear forces than does level walking, which necessitates greater knee stability. The injured medial meniscus will have an impaired ability to guide knee motion, which leads to greater amounts of lateral tibial translation and medial compartment excursion during more demanding tasks.
There are a few limitations to our study. An a priori power analysis yielded a need of 10 subjects for statistical significance, though for reasons previously discussed, the sample size was cut to 7 for analysis. Additionally, there was large between-subject variability, which may be characteristic of MMRT injuries and impossible to minimize. This being said, it is possible that a larger sample size will lower the data’s variability and yield more statistically significant differences resulting from MMRT injury. As previously mentioned, the average age of the subjects was 57.4 years. Although the intended subject population was younger, all younger MMRT patients sustained concomitant injuries and were deemed ineligible for study participation. It should also be noted that this study aims to examine bone kinematics, and we do not include the menisci or articular cartilage in any of our analyses. Future work will examine the in vivo kinematics of MMRT repair. In vitro studies have found that MMRT repair adequately restores the contact mechanics and kinematics of the injured knee, and it is unknown if these results will also be seen in vivo.
This study is the first of our knowledge to investigate the in vivo kinematics of an unrepaired medial meniscal root tear. MMRT is severe in the spectrum of meniscal injuries in that it is often misdiagnosed and leads to a rapid progression of osteoarthritis. Knowledge of the kinematics and arthrokinematics resulting from this injury may shed light on the mechanism of osteoarthritis progression in this population and assist in the development of effective repair techniques.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was funded by a grant from the Western Pennsylvania Chapter of the Arthritis Foundation.
Acknowledgment
The authors acknowledge William Anderst, Sebastian Kopf, and Kanu Goyal for their technical assistance in this study.