
Abstract
Background:
Superficial skin injuries are considered minor, and their incidence is probably underestimated. Insight into the incidence and mechanism of acute skin injury can be helpful in developing suitable preventive measures and safer playing surfaces for soccer and other field sports.
Purpose:
To gain insight into the incidence and severity of skin injuries related to soccer and to describe the skin injury mechanism due to player-surface contact.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
The prevention model by van Mechelen et al (1992) combined with the injury causation model of Bahr and Krosshaug (2005) were used as a framework for the survey to describe the skin injury incidence and mechanism caused by player-surface contact.
Results:
The reviewed literature showed that common injury reporting methods are mainly based on time lost from participation or the need for medical attention. Because skin abrasions seldom lead to absence or medical attention, they are often not reported. When reported, the incidence of abrasion/laceration injuries varies from 0.8 to 6.1 injuries per 1000 player-hours. Wound assessment techniques such as the Skin Damage Area and Severity Index can be a valuable tool to obtain a more accurate estimation of the incidence and severity of acute skin injuries.
Conclusion:
The use of protective equipment, a skin lubricant, or wet surface conditions has a positive effect on preventing abrasion-type injuries from artificial turf surfaces. The literature also shows that essential biomechanical information of the sliding event is lacking, such as how energy is transferred to the area of contact. From a clinical and histological perspective, there are strong indications that a sliding-induced skin lesion is caused by mechanical rather than thermal injury to the skin.
Soccer, or football, is the most popular sport practiced worldwide, with 265 million active players and expanding. 43 As the game’s global popularity increases, the climate plays a greater part in limiting its development. In adverse weather conditions, the use of natural grass fields is limited, and athletic performance suffers. Current generations of artificial turf mirror the playing characteristics of natural grass and are resistant to inclement weather. The International Football Association Board (IFAB) has recognized the advances in artificial surface technology and decided to introduce artificial turf into the laws of the game in July 2004. 20
From epidemiological injury studies, it can be concluded that the majority of football injuries (41%-81%) are caused by physical contact. 18,19,22,25,26,32,41 The physical contact is mainly attributed to player-to-player contact during tackling actions. Only Fuller et al 25 separately reported the incidence rate of player-surface contact. Of all reported injuries of male players, 6.6% of those on artificial turf are from player-surface contact versus 7.5% on natural grass. 25 Unfortunately, Fuller et al 25 did not correlate the type of injury to this player-surface injury mechanism. Until now, there are no published data available on the skin injury incidence rate caused by player-surface contact.
When player-surface contact involves too much energy, the skin is likely to fail, resulting in an abrasion. 12
Acute skin injuries have been reported to be more common when playing on earlier generations of artificial turf. 18,30 In a more recent study, Ekstrand et al 16 concluded that burns and friction injuries caused by third-generation artificial turf pitches are not a problem anymore.
On the other hand, interviews done by Yamaner et al 69 and the Royal Dutch Football Association (KNVB) 34 showed that up to 84% of players reported abrasions, indicating that these injuries are by far the most frequent type of injury when playing on artificial turf. Yamaner et al 69 attribute these abrasion injuries to different conditions of playing fields. Unfortunately, the different conditions were not described. Zanetti 70 interviewed 1600 amateur players who generally judged the artificial turf better than natural grass, with the exception of the risk of abrasion by sliding tackles in 3 of the 8 investigated fields. Although the injury incidence obtained from epidemiological research suggests otherwise, the perceived risks of abrasion and discomfort when playing on artificial turf calls for a deeper understanding of the acute skin injury mechanism due to player-surface contact.
The aim of this survey was 2-fold: (1) to gain insight into the incidence of reported skin injuries related to soccer and (2) to describe the skin injury mechanism due to player-surface contact.
Materials and Methods
The injury prevention model described by van Mechelen et al 65 was taken as the framework for this survey. According to this model, the extent of the skin injury (incidence and severity) and mechanisms are the starting points to introduce preventive measures and assess its effectiveness. Different risk models for sport-related injuries have been proposed to study injury mechanisms. 23,28,48,51 The Bahr model 8 combines the epidemiological model of Meeuwisse 51 and the biomechanical perspective as described by McIntosh. 48 Furthermore, this model takes the characteristics of the sports into account. Bahr and Krosshaug 8 combined internal risk factors related to the athlete, external risk factors, and the event leading to the injury. This comprehensive model for injury causation was used to assess the risk factors for skin injuries caused by player-surface contact during soccer.
The PubMed database was searched using the keywords injury, football, and artificial turf. Inclusion criteria for this survey were provided as follows: (1) data about skin injury incidence and severity in combination with the applied injury definition and (2) possible epidemiology, mechanisms, and risk factors of skin injury related to player-surface contact in football. We used the following exclusion criteria: (1) unavailable in English or (2) skin injury data that were unable to be recalculated to suit this article.
Article reference lists and relevant Dutch publications were used as additional supportive articles. A further search was conducted using the keywords wound definition and assessment, tackle, and fall studies in combination with sports and thermal skin injury in order to find papers that described potentially relevant skin injury mechanisms related to player-surface contact in soccer.
Skin Injury Definition and Incidence
In the past, different definitions for injury were used, which made it difficult to compare results of injury incidence studies. Therefore, an Injury Consensus Group, under the auspices of the Féderation Internationale de Football Association Medical Assessment and Research Centre (F-MARC), produced a consensus statement.
27
According to this statement, an injury is defined as any physical complaint sustained by a player that results from a football match or football training, irrespective of the need for medical attention or time loss from football activities. An injury that results in receiving medical attention is referred as a “medical attention” injury, and an injury that results in a player being unable to take full part in a future football training or match as a “time loss” injury.27(p193)
Furthermore, this statement contains categories for classifying the type of injury. According to this statement, contusions are considered as a separate class of skin injuries compared with lacerations and abrasions. Unfortunately, definitions of these types of skin injuries are not included in the statement. An overview of the definitions and appearance of the relevant acute skin injuries described in literature are summarized in Table 1.
Overview of Definitions and Clinical Appearance of Soccer-Related Acute Skin Injuries

As stated in the review study of Junge et al, 39 the injury definition directly influences data collection and thereby the reported incidence of skin injuries. If duration of time loss is taken as the only criterion, minor injuries and injuries “cured” by analgesics or other medications will be neglected, and the incidence of injury will be underestimated. 39 This is known as the “tip of the iceberg” phenomenon. 65 As an example, when the incidence of skin injury using time loss injury criteria is compared with medical attention criteria (Table 2), the incidence of abrasions and lacerations using time loss varies between 0.4 to 1.81 injuries per 1000 player-hours. However, with the medical attention definition alone, abrasions and lacerations are more frequently reported, varying from 0.8 to 6.1 injuries per 1000 player-hours. The differences in contusion incidence are even greater than lacerations and other skin injuries. Only Fuller et al 25 found a significant difference between artificial turf and natural grass during soccer matches with male players. More skin injuries were reported on artificial turf compared with natural grass. 25 No significant differences of incidence of skin injuries were found between surface and sex in other studies.
Skin Injury Rate of Different Types of Skin Injuries Depending on Sex and Playing Surface Using Time Loss and Medical Attention as Injury Definition

a Data are expressed as number of incidences per 1000 hours of exposure. A dash indicates that the specific incidence data were not described in the study.
bP < .01.
c Data in original articles were recalculated to suit the format.
Severity of Traumatic Skin Injuries
The Injury Consensus Group has formulated the injury severity as follows: “The number of days that have elapsed from the date of injury to the date the player returns to full participation in team training and availability for match selection.”27(p194)
Studies that reported the severity of skin-related injuries are summarized in Table 3. These data indicate that skin injuries such as abrasion and laceration are mainly qualified as slight to minimal injuries, which seldom lead to long absence from training or matches.
Injury Severity Classifications a
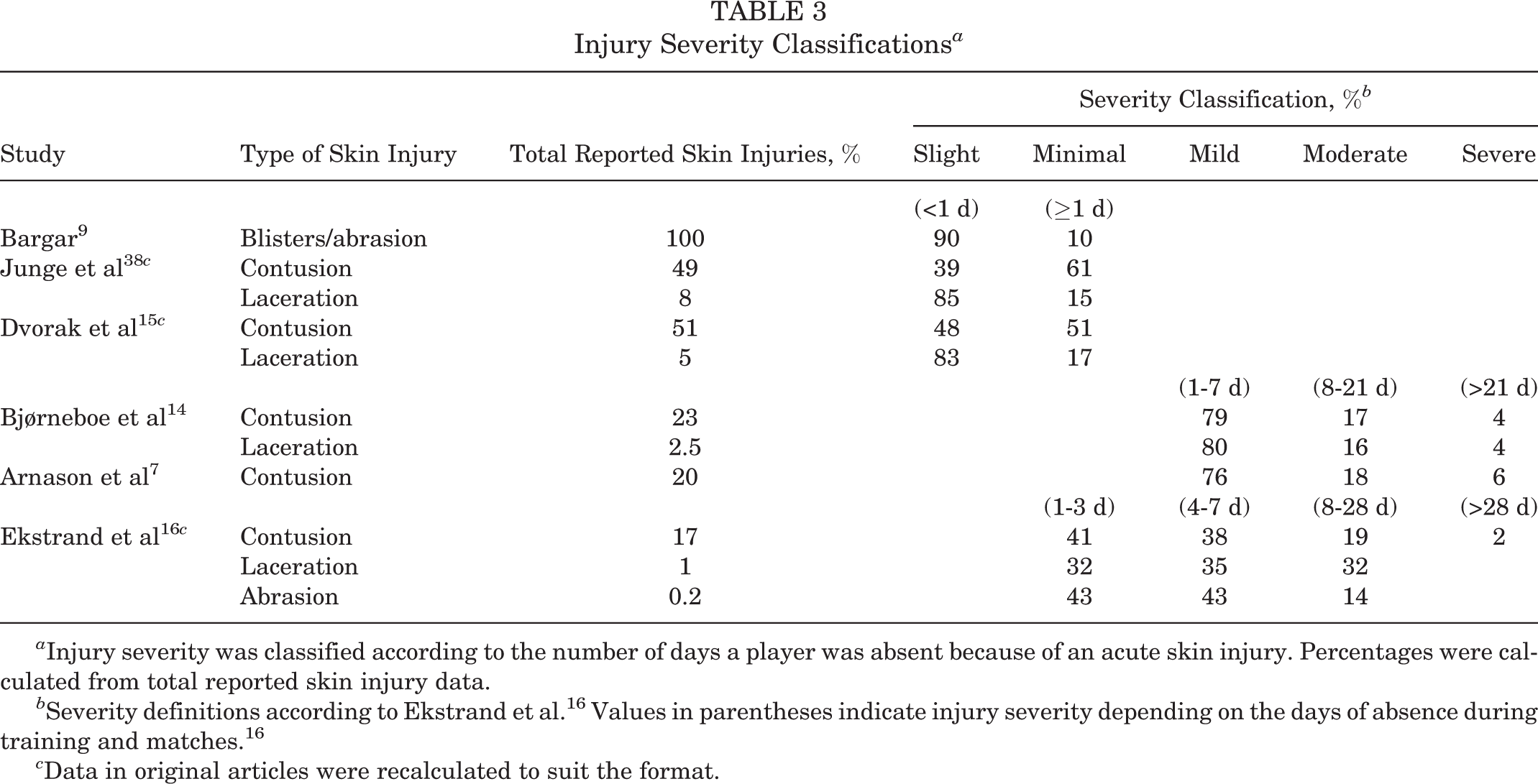
a Injury severity was classified according to the number of days a player was absent because of an acute skin injury. Percentages were calculated from total reported skin injury data.
b Severity definitions according to Ekstrand et al. 16 Values in parentheses indicate injury severity depending on the days of absence during training and matches. 16
c Data in original articles were recalculated to suit the format.
The normal healing time of an acute skin injury, like an abrasion, is 3 weeks. During this period, inflammation, proliferation, and remodeling takes place. 6,42 It is likely that during the healing process, the skin lesion has an influence on playing behavior. Uncomfortable postures and movements will consciously or subconsciously be avoided. 40 However, this perceived discomfort and its effect on the football match have never been investigated. The number of sliding tackles performed during a match could be an indicator of altered player behavior depending on the playing surface. Based on video analysis, Andersson et al 4 found a significantly lower number of sliding tackles on artificial turf compared with natural grass. However, Wooster 68 did not find significant differences when analyzing games played in the Union of European Football Associations (UEFA) Champions League and UEFA Cup. The number of sliding tackles probably not only depends on the surface but also on other factors, like tactics and soccer skills.
Although the effects of skin trauma on participation seem minimal, skin injuries need proper treatment to prevent complications, in particular, infections. 1,21,42 Infections can be caused by fungi, viruses, and bacteria like methicillin-resistant Staphylococcus aureus (MRSA). 10,13,43,60 It must be emphasized that these infections are mainly spread by direct skin-to-skin contact, as reported for wrestling and American football. The risk of contamination due to playing surface–skin contact is low. McNitt and Petrunak 49 described that, in general, the numbers of microbes present in synthetic turf are lower than natural grass. The infectious Staphylococcus aureus bacterium was not found on any type of playing surface. 49
Skin Injury Mechanism due to Player-Surface Contact
To describe the skin injury mechanism due to player-surface contact, the results of the literature search were categorized as intrinsic factors, extrinsic risk factors, and event according to the comprehensive injury causation model of Bahr and Krosshaug 8 (Table 4).
Risk Factors Obtained From the Literature a
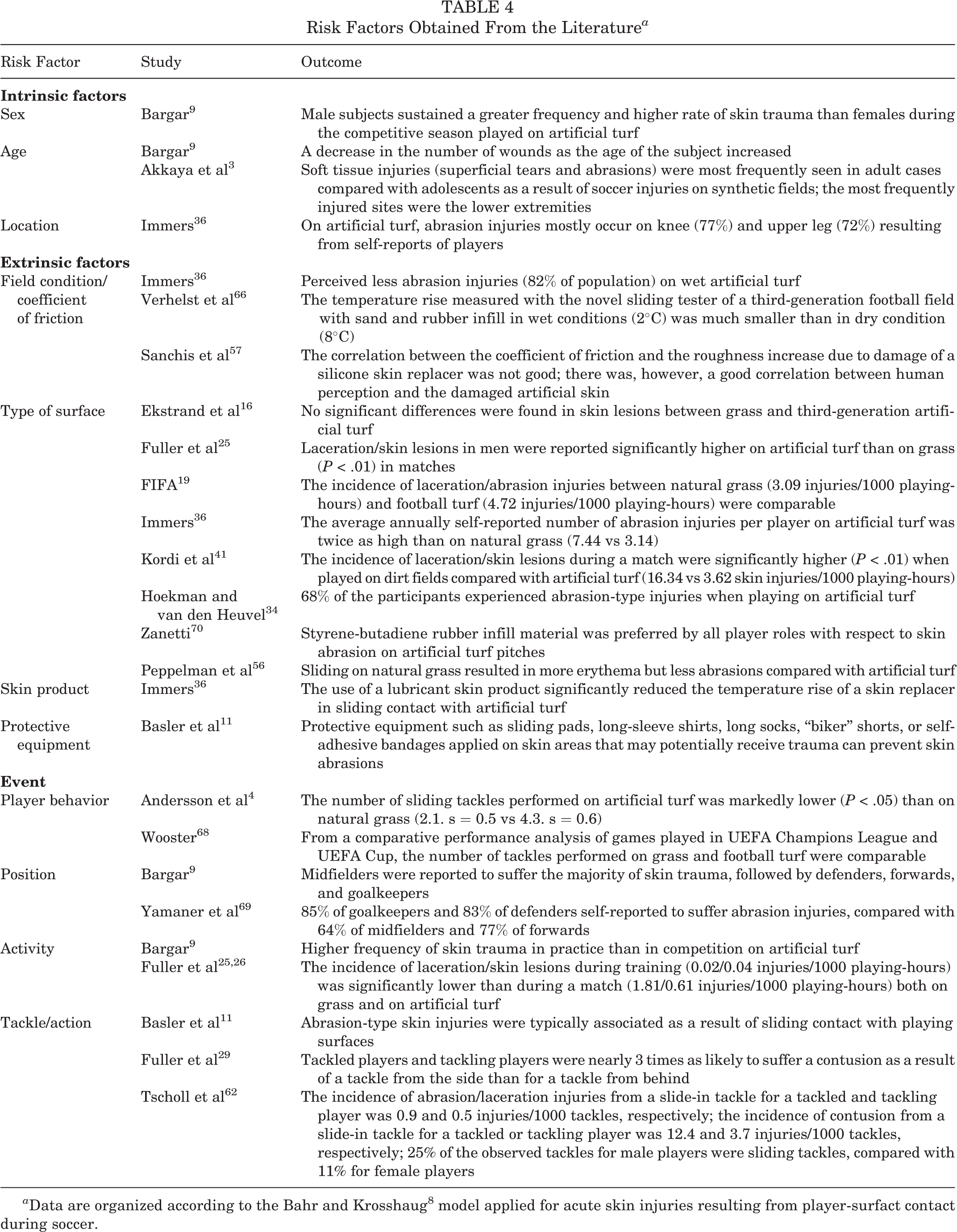
a Data are organized according to the Bahr and Krosshaug 8 model applied for acute skin injuries resulting from player-surfact contact during soccer.
These results demonstrate that wet playing surfaces, protective equipment, and the use of a skin lubricant decreases the incidence of abrasion injuries. Conflicting results are reported with regard to the influence of age, sex, type of surface, behavior, position on the field, and level of performance on the incidence of skin injuries.
Discussion
Although skin injuries are uncomfortable and unpleasant, they seldom lead to absence from training or a soccer match. In addition, medical attention is not often needed. 14 –16,24,38 The commonly used injury definition, which is mainly based on time loss or need for medical attention, determines data collection during incidence studies. Therefore, it is not surprising that abrasions and lacerations are not often reported. The reported incidence of these injuries varies from 0.8 to 6.1 per 1000 player-hours. ∥ Retrospective studies in which players were questioned document that players sustained more abrasions than more severe injuries like strains, sprains, and fractures. 34,36,69,70
The difference between injury surveillance and retrospective player perception studies is noteworthy because previous studies demonstrate that injury reporting is more reliable and does not suffer from recall bias. 14 The difference between player perception of skin injuries and the injury criteria indicate that the time loss or medical attention injury definitions are not sensitive and accurate enough.
Wound assessments, common in dermatological practice, could be of increased value. 2,44 These assessments examine all aspects of an injury. In this perspective, the newly developed scoring system to quantify sliding-induced skin lesions described by van den Eijnde et al 63 is of interest. The Skin Damage Area and Severity Index (SDASI) is based on visual scaling of the clinical parameters abrasion, erythema, and exudation. The extent of the involved area complements the SDASI. 63 It must be noted that other new or additional methods of data collection could place greater time demands on the medical personnel involved in these studies. 27
The model described by Bahr and Krosshaug 8 was used to address risk factors for acute skin injuries caused by player-surface contact. Based on this study, it can be concluded that there is consensus with regard to the positive effect of a wet surface condition and the use of protective equipment or skin lubricant. There are conflicting results regarding the influence of age, sex, type of surface, behavior, position on the field, and level of performance on the incidence of skin injuries. More important, this overview shows that there are multiple risk factors for abrasions, confirmed by Zanetti, 70 who demonstrated that skin abrasions are influenced by the field configuration, role in the game, weather condition, and infill type. For a third-generation artificial turf field, the infill consists of rubber granules, which are used as filling material between the grass artificial fibers.
According to Meeuwisse, 51 the event itself is the main risk factor in acute injuries. External and/or internal risk factors contribute to a lesser extent to the cause of injury.
A small contribution is required from other external and/or internal risk factors to cause an injury. 51 Few data are available on acute-type skin injury such as a sliding tackle. Only Fuller et al 29 compared the influence of tackle parameters to the propensity of injuries that required medical attention. Unfortunately, only player-to-player contact injuries were recorded. The lack of description of the biomechanical factors associated with the sliding tackle is another more essential limitation of this study. In the field of biomechanics, McIntosh 48 mentioned that injury analysis and prevention must explain how energy transfer arises, why it results in injury, and how it can be prevented. Several biomechanical studies were performed in the field of football skills like kicking, heading, throwing, running, and turning. 45,46,59,61 However, studies regarding the kinematics and energy transfer during a sliding tackle are lacking at the moment.
The types of biomechanical studies that are closely related to a sliding tackle are fall studies of walking or standing participants. Fall studies mainly focus on the risk factors of hip fracture and not skin injuries. Table 5 gives an overview of characteristic kinematic parameters such as vertical impact force and vertical impact velocity. Based on the findings of the study of Schmitt et al, 58 an impact pressure value of approximately 110 to 125 N/cm2 (4000-4500 N) could result in a contusion. Furthermore, it was demonstrated that the present literature lacks suitable values for contusion injury risk. 58 It is likely that the vertical kinematic parameters of a sliding tackle are comparable to a side jump of a goalkeeper. The horizontal initial speed of a sliding tackle even increases the total energy transfer during contact. Finally, the mechanical properties of the human skin, such as stiffness and ultimate strength, in combination with the physical condition of the skin determines how the skin will respond to physical loads during sliding. 8
Characteristic Kinematic Parameters Reported by Different Fall Studies a
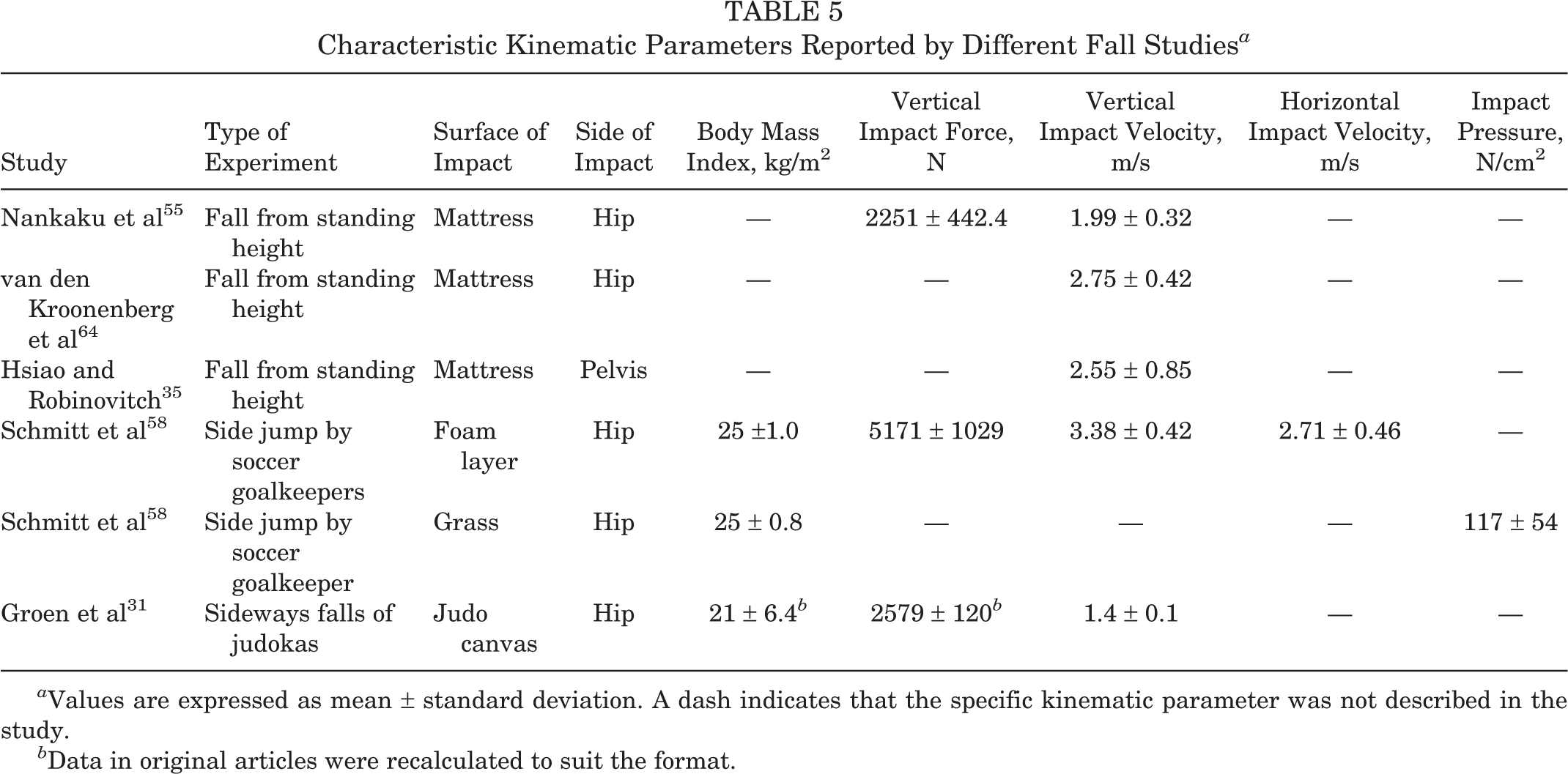
a Values are expressed as mean ± standard deviation. A dash indicates that the specific kinematic parameter was not described in the study.
b Data in original articles were recalculated to suit the format.
A more fundamental question with respect to energy transfer is whether skin damage is caused by mechanical or thermal injury due to friction, as the term turf burn suggests. Peppelman et al, 56 in a histological study, found only removal of the stratum corneum. The deeper skin tissue was undamaged. This suggests that a sliding tackle does not result in a deep dermal or full-thickness wound, which is characteristic for a deep second- or third-degree contact burn. 33 However in the same study, the expression of the thermal stress protein HSP70 was increased on both dry artificial and dry natural grass but not on water-sprinkled natural grass. Therefore, the concept of reversible superficial burns cannot be excluded at the moment. The surface temperature threshold at which irreversible epidermal injury occurs is dependent on the contact time. The typical contact time of a sliding tackle is in the range of 1 second. The corresponding temperature threshold at which epidermal injury occurs is at least 60°C. 54 A temperature rise of 8°C, as measured by Verhelst et al 66 at 20°C laboratory conditions, indicates that friction energy is not high enough to cause burns. Furthermore, they reported that there was abrasion in dry conditions. This suggests that the skin failure mechanism caused by sliding is more mechanical than thermal. However, the environmental conditions are also important to take into account. It has been reported that the temperature of synthetic turf surfaces are significantly higher (range, 35°C-60°C) compared with natural grass surfaces when exposed to sunlight. 50,67 The temperature in the area of contact due to environmental conditions may be more important than the differences in sliding friction.
Conclusion
Current injury surveillance lacks information about the incidence of acute skin injury. The development of a noninvasive, reliable technique to assess skin injury such as the SDASI may help to obtain a more accurate estimation of the incidence and severity of acute skin injuries.
Clinical and histological data indicate that under normal environmental conditions, sliding-induced skin injuries are mainly caused by mechanical failure instead of thermal injury to the skin. Consequently, abrasion would be the correct term for a sliding-induced skin injury rather than turf burns. The chance of a reversible superficial burn cannot be excluded. A sliding tackle can cause a burning feeling but not a deep burn wound. Sprinkling water on synthetic turf makes sliding more comfortable; whether this also has a significant effect on the injury incidence has not been determined.
From this literature survey, it can be concluded that essential biomechanical information of a sliding tackle is lacking. A first step for future research is to quantitatively describe the kinematic parameters of a sliding tackle. These parameters are the boundary conditions for the mechanical stress to which the skin and body are exposed.
Finally, together with a sufficiently sensitive skin injury assessment method, multifactorial studies are necessary to identify the critical risk factors that contribute to a sliding-induced skin injury.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was conducted with a financial contribution from the Dutch Ministry of Economic Affairs, Agriculture, and Innovation and the provinces of Gelderland and Overijssel.