
Abstract
Background:
Shoulders of throwing and swimming athletes are highly stressed joints that often show structural abnormalities on magnetic resonance imaging (MRI). However, while water polo players exhibit a combination of throwing and swimming movements, a specific pattern of pathological findings has not been described.
Purpose:
To assess specific MRI abnormalities in shoulders of elite water polo players and to compare these findings with a healthy control group.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
After performing a power analysis, volunteers were recruited for this study. Both shoulders of 28 semiprofessional water polo players and 15 healthy volunteers were assessed clinically (based on the Constant score) and had bilateral shoulder MRIs. The shoulders were clustered into 3 groups: 28 throwing and 28 nonthrowing shoulders of water polo athletes and 30 shoulders of healthy control subjects.
Results:
Twenty-eight male water polo players with an average age of 24 years and 15 healthy subjects (30 shoulders) with an average age of 31 years were examined. Compared with controls, significantly more MRI abnormalities in the water polo players' throwing shoulders could be found in the subscapularis, infraspinatus, and posterior labrum (P = .001, P = .024, and P = .041, respectively). Other structures showed no statistical differences between the 3 groups, including the supraspinatus tendon, which had abnormalities in 36% of throwing versus 32% of nonthrowing shoulders and 33% of control shoulders. All throwing shoulders showed abnormal findings in the MRI, but only 8 (29%) were symptomatic.
Conclusion:
The shoulders of semiprofessional water polo players demonstrated abnormalities in subscapularis and infraspinatus tendons that were not typical abnormalities for swimmers or throwing athletes.
Clinical Relevance:
The throwing shoulders of water polo players have specific MRI changes. Clinical symptoms do not correlate with the MRI findings.
Water polo is an Olympic sport with high demands on the shoulder joint as the players swim in rapid sprints suddenly changing direction, have physical contact with other players, and repetitively throw a 400- to 450-g ball. This activity generates considerable stress in the glenohumeral joint by 2 main factors, both requiring significant muscular strength. The first component is throwing, which is executed with a maximum angular velocity of 1137 deg/s and a ball velocity of up to 19.7 m/s. 17 The second component is swimming, performed with a constant and lower angle velocity but greater numbers of repetitions than throwing.
Although shoulder injury and overuse patterns vary by sport and position, there are common movements for all overhead athletes. Concerning throwing, many of the injury patterns and biomechanical motions in water polo players are similar to other throwing athletes. To our knowledge, no studies have been published in which the shoulders of water polo players were assessed by magnetic resonance imaging (MRI) and compared with a control group.
The shoulder problems of professional swimmers are typically caused by freestyle and butterfly strokes, resulting in a microinstability with a cranial shift of the humeral head, leading to subacromial impingement and bursitis, and affecting the supraspinatus tendon. 8 Jerosch et al 9 found various pathological changes in MRIs of water polo players’ shoulders, even in athletes who were completely asymptomatic. In symptomatic water polo players, posterosuperior impingement of the glenoid seems to be the main reason for shoulder pain. 5
The purposes of the study were to assess shoulder MRIs of water polo players, correlate pathological findings to eventual clinical symptoms, and to compare MRI findings with a matched control group. Another aim was to find a specific pattern of pathological changes typical for water polo players.
Materials and Methods
The study was conducted in accordance to the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. All participants signed an informed consent form. An institutional review board approved the study protocol. The study was registered on www.ClinicalTrials.gov (NCT00959543).
This study was designed as a retrospective cohort study. After performing a power analysis, an appropriate number of volunteers were recruited. The study population was selected from male semiprofessional water polo players between the ages of 18 and 35 years from the National Water Polo League and Promotion Water Polo League of Switzerland. We recruited 28 athletes with symptomatic and asymptomatic shoulders. Exclusion criteria were playing the position of goalkeeper and previous shoulder surgery. The control group included 15 male volunteers (n = 30 shoulders) between the ages of 18 and 35 years. All members of the control group participated in recreational sports activities but no high-level competitive sports, no swimming, and no sports with overhead throwing movements. Further exclusion criteria were previous shoulder surgery or persons who pursued a profession with overhead activity.
All subjects were examined clinically by 1 board-certified senior orthopaedic surgeon (M.B.) and 1 resident in orthopaedic surgery (M.K.). The examination included range of motion (neutral-zero method), rotator cuff tests, tests for impingement and biceps tendinitis, instability test, and isometric measurement of strength using the ISOBEX dynamometer (MDS AG, Burgdorf, Switzerland). Furthermore, the Constant-Murley score was assessed. 2,3
All athletes as well as the control subjects received a MRI without arthrography of both shoulders. The MRIs were performed using 1.5-T scanners (Magnetom Avanto and upgraded Magnetom Symphony with shoulder-array coils; Siemens, Erlangen, Germany) in a standardized protocol with fixed sequence parameters (TR, time of repetition in milliseconds [ms]; TE, time of echo in milliseconds [ms]; ET, echo train; STH, slice thickness in millimeters [mm]; M, matrix; FOV, field of view in millimeters [mm]). In the coronal oblique plane, a T2-weighted (TR, 4250 ms; TE, 93 ms; ET, 14; STH, 4 mm; M, 384 × 384; FOV, 150 × 150 mm) and an intermediate-weighted fast spin echo sequence with fat saturation (TR, 3320 ms; TE, 27 ms; ET, 7; STH, 4 mm; M, 576 × 768; FOV, 150 × 150 mm) were obtained.
In the sagittal oblique plane, a T1-weighted spin echo sequence (TR, 450 ms; TE, 11 ms; ET, 1; STH, 3.5 mm; M 506 × 768; FOV, 150 × 150 mm) and an intermediate-weighted fast spin echo sequence with fat saturation (TR, 3050 ms; TE, 44 ms; ET, 7; STH, 3.5 mm; M, 256 × 256; FOV, 150 × 150 mm) were acquired. In the transverse plane, intermediate-weighted fast spin echo images with fat saturation were obtained (TR, 3500 ms; TE, 29 ms; ET, 7; STH, 3.5 mm; M, 256 × 256; FOV, 150 × 150 mm). Two senior radiologists experienced in musculoskeletal radiology evaluated the images. As the first step, the evaluation was performed blinded for grouping and dexterity. In a second step, differing results were reviewed, discussed, and reevaluated to obtain a consensus regarding interpretation of abnormal findings. Rotator cuff lesions were divided into tendinopathies (signal abnormalities), partial tears, and full-thickness tears of the supraspinatus, infraspinatus, and subscapularis tendons, respectively. Further structures and pathologies of interest were: the labrum, ganglion cysts, the long biceps tendon, changes of the cartilage, osteochondral defects, osseous abnormalities, and abnormalities of the acromioclavicular joint, the capsule, and the subacromial bursa.
The data were organized into 3 groups: the throwing shoulders of water polo players (group 1; n = 28), their nonthrowing shoulders (group 2; n = 28), and shoulder joints of the control group (group 3, n = 30).
Statistical analysis consisted of descriptive statistics and tests for statistical differences between the groups. Depending on the type of variables, Wicoxon or McNemar tests were applied for paired data and the chi-square test or Mann-Whitney U test for unpaired data. The interobserver variability was tested with the kappa test. The statistical analysis was performed using SPSS software (version 11.5; SPSS Inc, Chicago, Illinois, USA).
Results
The clinical results including the Constant score data are shown in Table 1. The mean age was higher in the control group, but the range in both groups was equal (range, 18-35 years). The results of the clinical assessment between the 2 examiners were highly correlated (P < .001). For the Neer, Hawkins, and Jobe tests, there was a mean kappa value for the interobserver correlation of 0.853.
Age, Clinical Tests, Strength Measurements, and Constant Score for the Study Groups a
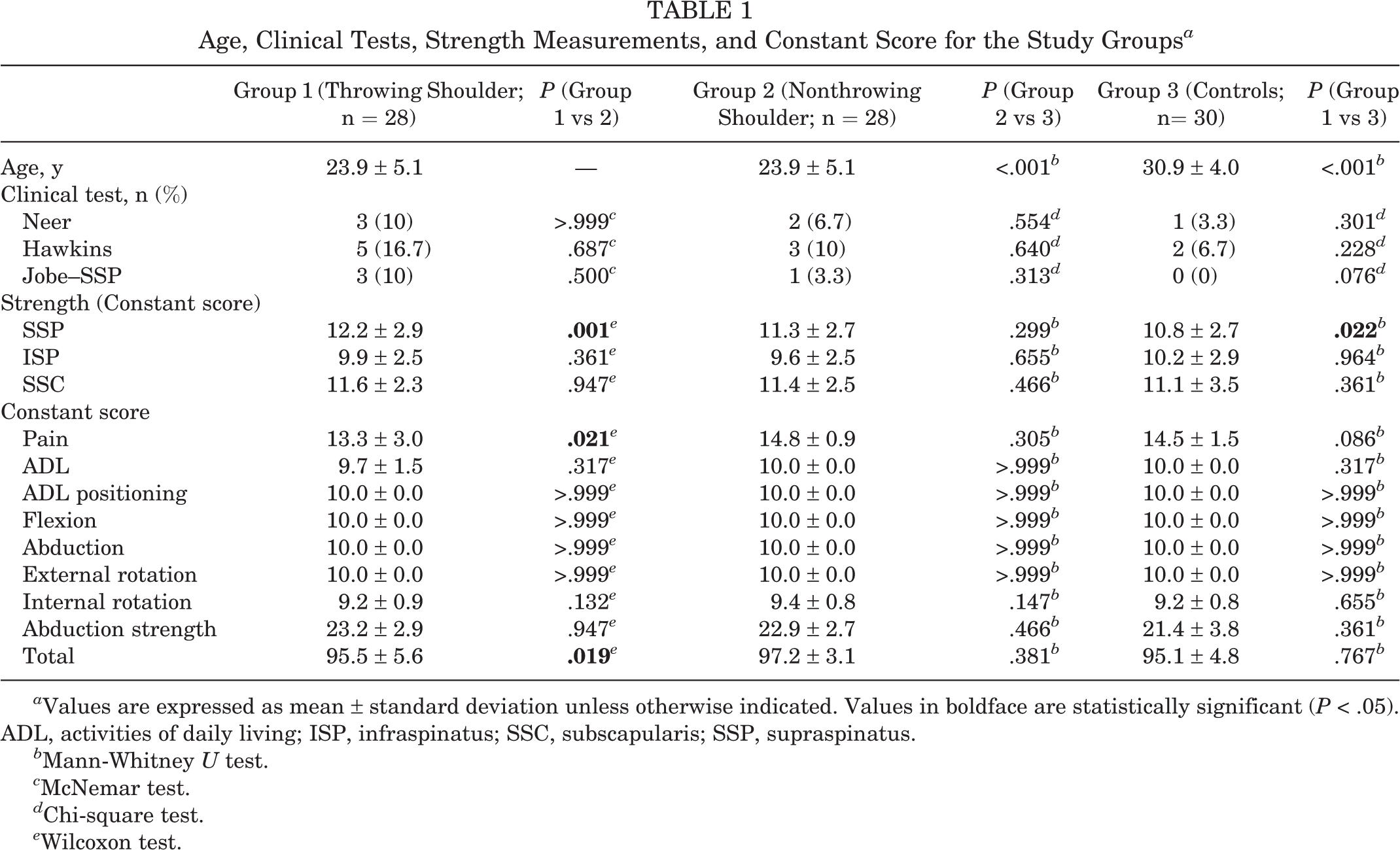
a Values are expressed as mean ± standard deviation unless otherwise indicated. Values in boldface are statistically significant (P < .05). ADL, activities of daily living; ISP, infraspinatus; SSC, subscapularis; SSP, supraspinatus.
b Mann-Whitney U test.
c McNemar test.
d Chi-square test.
e Wilcoxon test.
Overall, the shoulders of the athletes and the control subjects were clinically normal, but pain symptoms lowered the Constant scores for throwing shoulders. Nevertheless, the abduction power was greater in the throwing shoulder when compared with the nonthrowing shoulder or control group.
Frequency of Abnormal MRI Findings: Comparison of Throwing, Nonthrowing, and Control Shoulders a

a Values are expressed as n (%). Values in boldface are statistically significant (P < .05). MRI, magnetic resonance imaging.
b Wilcoxon test.
c Mann-Whitney U test.
d McNemar test.
e Chi-square test.
Regarding MRI analysis, we found significantly more MRI abnormalities in the subscapularis and infraspinatus tendons when the MRI of the throwing shoulder was compared with healthy volunteers (Table 2). Although there was a difference for those 2 variables between the throwing and nonthrowing shoulders, this difference was not statistically significant. We found significantly more lesions of the posterior labrum in the throwing shoulders when compared with the nonthrowing shoulders (P = .001) and a less significant but still clear difference when compared with the control group (P = .041). There was no statistically significant increase of supraspinatus lesions in MRI of the throwing shoulder compared with the other 2 groups. There was also no correlation between MRI findings and clinical parameters. All throwing shoulders did show some pathological findings on MRI, but only 8 (29%) were symptomatic.
Discussion
Water polo is an Olympic sport where the athletes are moving in 1 medium (water) but are throwing and passing the ball in another medium (air). In both spaces (above and below the water surface), considerable work seems to be performed by the shoulder muscles (Figure 1). This could affect the dominant shoulder in a specific way by combining throwing loads and high-frequency swimming strokes. Furthermore, water polo players exhibit forced flexion and adduction movements to bring the upper body as high as possible above the water surface. This is unusual compared with other contact or ball sports where body weight is not apparently reduced because of immersion in water. Whereas swimmers continuously repeat their strokes during training or competition, water polo players change their swimming speed, direction, and stroke styles. 4 In this study, a homogenous group of high-level water polo players was examined clinically and with bilateral shoulder MRI and compared with a control group of young and healthy volunteers. The aims of our study were to assess MRI abnormalities in this specific group of athletes and to correlate these findings with clinical symptoms.

Water polo player in a throwing motion. Note the strong shoulder girdle muscles. A similar arm position can be observed when handball players perform a jump shot.
We could not find the pattern of MRI abnormalities that is usually associated with throwing or swimming shoulders. The results of this study demonstrate that the MRI findings in throwing shoulders of water polo players showed relatively more subscapularis and infraspinatus abnormalities than expected. A comparative analysis of our results and a similar study on the throwing shoulders of handball players 10 is shown in Figure 2. Jost et al 10 described significantly more pathological MRI findings (P = .008) in the supraspinatus muscle of throwing shoulders than was found in our study. The other groups (nonthrowing athletes and healthy volunteers) and changes in the other 2 muscles (subscapularis and infraspinatus) did not differ significantly.

Comparative analysis of our data and results reported by Jost et al. 10 HB, handball players; ISP, infraspinatus; ns, not significant; SSC, subscapularis; SSP, supraspinatus; WP, water polo players. *Mann-Whitney U test, P = .008.
Connor et al 1 found up to 40% false positive rotator cuff abnormalities in MRIs of asymptomatic shoulders in overhead athletes. Furthermore, in their study, the athletes remained asymptomatic at 5 years of follow-up. Our study confirms that in top overhead athletes, in this case, water polo players, the abnormalities in MRI of the dominant throwing shoulder should be interpreted with caution. Depending on definition, such an abnormality could be defined as a “false positive” or “true positive but clinically asymptomatic” and thus irrelevant. Whether these MRI abnormalities become symptomatic in the long term remains to be studied. The impact of our study on treatment of a water polo player with a painful shoulder is that an abnormal MRI finding does not necessarily indicate a pathological condition and should not be treated automatically. This is in accordance with other studies on MRI abnormalities in shoulders of overhead, throwing, or pitching athletes such as baseball players, kayakers, or handball players. 6,7,10,11,14
Sein et al 16 reported that supraspinatus tendinopathy induced by intense training is a major cause of shoulder pain in swimmers. On the contrary, McMaster et al 13 found a statistically significant correlation between glenohumeral laxity and pain in senior national and elite swimmers. This instability-related shoulder pain is common in swimmers (up to 42%). It is difficult to treat because arthroscopic capsular plication impedes the athletes ability to return to their previous level of competition. 15 In our study, we could not find signs of instability, and the supraspinatus pathology was not relatively elevated.
One interesting result in the clinical part of our study was the elevated abduction strength of the throwing shoulder in comparison with the nonthrowing and control groups. This is in contrast to the findings of Jost et al 10 in a similar study of the shoulders of handball players, who found equal strength of 11.0 kg on both sides, which is even less than the nonthrowing (ie, nondominant) side of water polo players (11.3 kg). The water polo players seem to need more abduction/elevation strength to play at the professional level than handball players do. Another explanation could be that because of pain caused by increased wear (and consequently more supraspinatus pathology in MRI), the handball players lose some abduction strength. McMaster et al 12 found relatively stronger adduction and internal rotation in water polo players. Jerosch at al 9 investigated 11 top water polo players and found no signs of subacromial impingement or pathology. Both studies are in accordance with our results that water polo players develop a specific pattern of pathology, primarily not in the subacromial space. When compared with the study by Jerosch et al, 9 our study includes more athletes; involves the MRI of the opposite, nonthrowing shoulder; and provides a comparison with a healthy control group.
Our study also has some limitations. The number of individuals in our control group was relatively small. However, it is the largest reported in the literature. Although the age of the control group was greater than the age of the study group, more overuse degenerative changes were not found in the control group. Therefore, this age difference (in favor of athletes) did not affect the outcome of our study. The third limitation is that MRI was done without arthrography because of personal and institutional ethical concerns. This reduced the diagnostic discrimination power for intra-articular lesions such as labral, biceps tendon, or chondral lesions. However, it would have been difficult to recruit enough volunteers for MRI with arthrography.
Conclusion
Shoulders of elite water polo players did not show the typical MRI findings of the shoulders of swimming or throwing athletes. The water polo player’s throwing shoulder seems to have a specific pattern of abnormal MRI findings that are more pronounced in the subscapularis and the infraspinatus tendons. There was no correlation between clinical symptoms and the MRI findings.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.