
Abstract
Background:
Methods of objectively measuring rotational knee laxity are either experimental or difficult to use in daily practice. A new method has been developed to quantitatively assess rotatory laxity using an open MRI system and new tool, the KneeM device.
Purpose/Hypothesis:
To perform a preliminary evaluation of a novel knee rotation measurement device to assess knee kinematics during flexion in an MRI field, in both anterior cruciate ligament (ACL)–deficient and healthy contralateral knees. The hypothesis was that the KneeM device would allow in vivo reproduction and analysis of knee kinematics during flexion in healthy and ACL-deficient knees.
Study Design:
Controlled laboratory study.
Methods:
Ten subjects (7 men and 3 women; mean age ± standard deviation, 32.3 ± 9.4 years) with ACL-deficient knees and contralateral uninjured knees participated in the study. An open MRI was performed with the KneeM device at a mean 4.9 months (range, 3.0-7 months) after ACL injury. The device exerted on the knee an anterior drawer force of 100 N, with an internal rotation of 20°, through the range of flexion (0°, 20°, 40°, and 60°). Both ACL-deficient and healthy contralateral knees were analyzed using the Iwaki method.
Results:
There was no statistical difference of anterior translation in the medial compartment between intact and ACL-deficient knees at all degrees of flexion. However, significant differences in the anterior translation of the lateral compartment were observed between ACL-deficient and intact contralateral knees at 0° and 20° of flexion (P = .005 and P = .002, respectively). Between 20° and 40°, the lateral plateau of ACL-deficient knees translated 7.7 mm posteriorly, whereas the medial compartment remained stable, reflecting a sudden external rotation of the lateral plateau under the femoral condyle.
Conclusion:
This preliminary study suggests that measurement of tibiofemoral movements in both compartments during flexion using the KneeM device was useful for quantifying rotatory laxity in ACL-deficient knees. Moreover, this device seemed to allow a “mechanized pivot shift” and allowed reproduction of the “pivot” phase in the MRI field between 20° and 40° of flexion.
Clinical Relevance:
This device could be used for diagnostic purposes or to investigate the outcomes of ACL reconstructions.
Anterior cruciate ligament (ACL) injuries induce sagittal and rotatory instabilities. 9,17,57 Rotational laxity correlates with patient satisfaction, functional outcomes, and degenerative evolution of the knee. 5,25,26,32 The most specific clinical test to evaluate rotatory instability is the pivot-shift test. 30 A positive pivot-shift test is indicative of an ACL-deficient knee. However, this test remains subjective and operator dependent and has a poor interobservator reliability. 11,22,38
Authors of clinical studies 15,23,28 discussing results of ACL reconstruction believe that a reliable and objective method is necessary to evaluate the rotational laxity of affected knees. 55 So far, methods of measuring rotational laxity are either experimental or difficult to use in daily practice.
As the KT-1000 arthrometer became a reliable method for measuring anteroposterior laxity, 12 we believe that a simple and reliable tool using open magnetic resonance imaging (MRI) can be developed to minimize flaws and to consistently quantify rotational laxity of the knee. Indeed, MRI is a reliable method of documenting knee anatomy and kinematics during flexion. 49
We developed a new tool for the purpose of quantitatively assessing rotatory laxity using an open MRI system, the KneeMRI (KneeM) device. This tool holds knees in the MRI field and applies both an anterior draw and internal tibial rotation force during knee flexion.
The purpose of this study was to perform a preliminary analysis of in vivo kinematics during flexion in the MRI field of both ACL-deficient and healthy contralateral knees constrained by the KneeM device. The hypothesis was that this MRI device would demonstrate a difference in knee kinematics between normal and ACL-deficient knees.
Materials and Methods
Patients
Ten patients (7 men and 3 women; mean age ± standard deviation [SD], 32.3 ± 9.4 years) with an ACL-deficient knee but contralateral uninjured knee participated in the present study. Exclusion criteria included an associated collateral ligament injury, a symptomatic contralateral knee, fractures, grade III or IV radiological degenerative changes, and/or the presence of hip or ankle pathology. Patients had complete unilateral ACL rupture with or without meniscal pathology less than 12 months prior to testing and were symptomatically unstable and awaiting reconstruction. ACL rupture was confirmed by clinical examination and MRI. Clinically, rotatory laxity of the knee was evaluated manually by 1 experienced clinician using the pivot-shift test at a mean 4 months (range, 2.0-6.0 months) after ACL injury. All patients presented a gross (++) or marked (+++) pivot-shift test at clinical examination. KT-1000 arthrometer measurement at 134 N demonstrated a mean difference of 6.4 mm (SD, 2.1 mm) in anterior translation between the ACL-deficient and normal knees for all patients. The study protocol was reviewed and approved by the institutional review board, and all patients gave their informed consent before they were included. The mean time between ACL injury and the MRI was 4.9 months (range, 3.0-7.0 months).
MRI Scanning Method
The in vivo measurement of rotatory laxity was performed using the KneeM device placed in the open MRI field. The subjects laid on the contralateral side in an open MRI scanner (0.35-T Sigma Ovation HD; General Electric Healthcare, Milwaukee, Wisconsin, USA). The custom-built KneeM device strained the lower limb with 2 straps, 1 on the thigh and 1 on the calf, exerting a manual anterior drawer force of 100 N measured by a dynamometer (Figure 1). All measurements were obtained with the lower limb in a fixed internal rotation of 20° and with the muscles relaxed. The knee was successively flexed from full extension to 20°, 40°, and 60° of flexion. A rigid fixation in each position was held by screws. Four MRI acquisitions were performed in extension and at 20°, 40°, and 60° of flexion (scan parameters: T2-weighted fast spin echo sequences, 40 slices of 0.6-mm thickness; field of view, 240 mm; matrix size, 512 × 256; repetition time [TR], 6220 ms; echo time [TE], 102 ms). Both injured and healthy contralateral knees were successively analyzed. It took approximately 45 minutes for each patient to complete the scan, including the 8 sequences. The examination was painless and therefore without risk of additional injury to the limb.
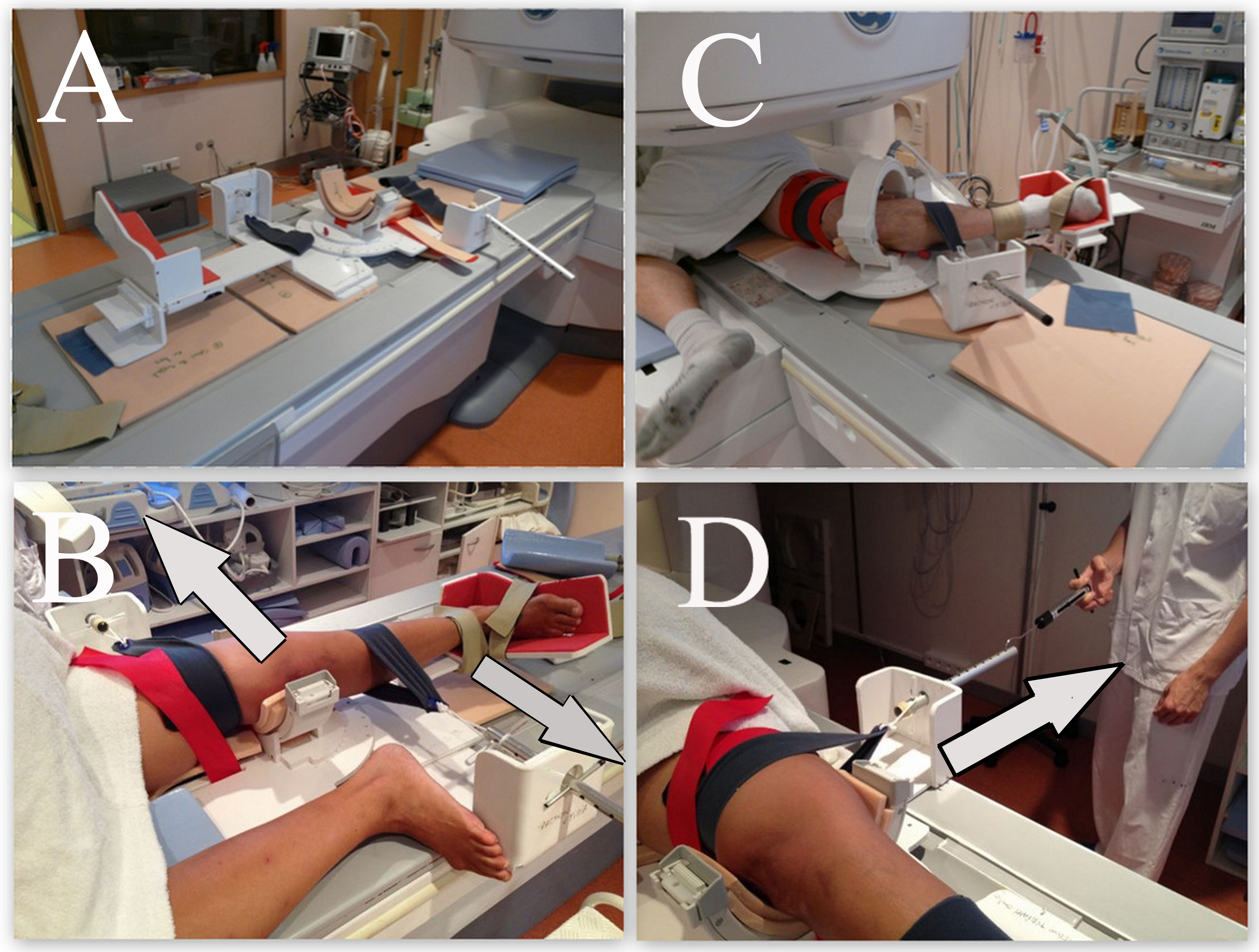
The patient is tested using the KneeM device (A) in the open MRI. (B) The knee is anteriorly constrained by 2 straps, with the lower limb fixed in internal rotation (20°). (C) Four degrees of flexion (0°, 20°, 40°, and 60°) can be adjusted. (D) A dynamometer was used to exert an anterior drawer force of 100 N.
MRI Data Analysis
We used Osirix software (Pixmeo, Geneva, Switzerland) to measure, according to the Iwaki method, 20 the anteroposterior tibial translation with respect to the femoral condyles (distance “D”) at all angles of flexion for both ACL-deficient and healthy knees. The distance was recorded on sagittal T1-weighted images scanned at each center of the medial and lateral compartments by measuring the distance between the tangent line of the posterior tibial cortex and the center of a circle materializing the femoral condyle, called the flexion facet center (FFC) 20 (Figure 2). To determine the center of each compartment, we used an initial 3-dimensional multiplanar reconstruction scan to choose the slice that included the medial edge of the fibular head as a landmark for the center of the lateral compartment and the attachment of the medial head of the gastrocnemius for the medial compartment. To determine the FFC, we took the center of a circle that encompassed the posterior aspect of each condyle, medial and lateral, that has been shown to have a relatively circular form in the sagittal plane. 53 The FFC can be used as a reliable reference point for the position of each condyle. 20 The reference point for the tibia was the tangent line to the posterior tibial cortex, perpendicular to a horizontal line parallel to the tibial plateau. It is important to note that according to the Iwaki method, the distance “D” is inversely proportional to the anterior tibial translation. The distance “D” is smaller for ACL-deficient knees than for healthy knees. Analysis by an experienced examiner took approximately 10 minutes for the 8 measures (2 knees × 4 angles).

Measurement of the femorotibial relationship using the Iwaki method. Distance “D” is measured in the lateral compartment of an extended knee. Measurement of D is taken from the flexion facet centers (FFCs) to the vertical line drawn from the posterior tibial cortex.
Reproducibility
All images were measured 3 times by 2 senior orthopaedic surgeons, who were blinded to the results of the physical examination, with a minimum interval of 1 week between each measurement.
Statistical Analysis
Analysis was conducted using the R software version 2.13.1 (R Foundation for Statistical Computing, Vienna, Austria). The Mann-Whitney test was used to compare the anterior tibial translation between the ACL-deficient knees and intact knees in the lateral and medial compartments at all degrees of flexion. A P value of ≤.05 was considered to be statistically significant.
The intra- and interobserver reproducibility was assessed using the intraclass correlation coefficient (ICC). A Bland and Altman plot was also constructed for each compartment and each knee (healthy or deficient) to visually assess the interobserver agreement (Figure 3).

Bland and Altman plot for interobserver agreement. HKLC, healthy knee, lateral compartment.
Results
The results of the anterior tibial translation during flexion, for both knees, are presented at the center of the medial and the lateral compartments (Table 1 and Figure 4).

Diagram of the femoral condyle overlaid with solid lines representing the posterior tibial cortices at each degree of flexion (0°, 20°, 40°, and 60°) of the healthy knees (A) and the anterior cruciate ligament–deficient knees (B). The Y-axis represents the average distances (mm) from the ipsilateral posterior tibial cortex to the FFC (distance “D”). X, axis of rotation.
Distance “D” for Each Angle of Flexion for Healthy and ACL-Deficient Knees a
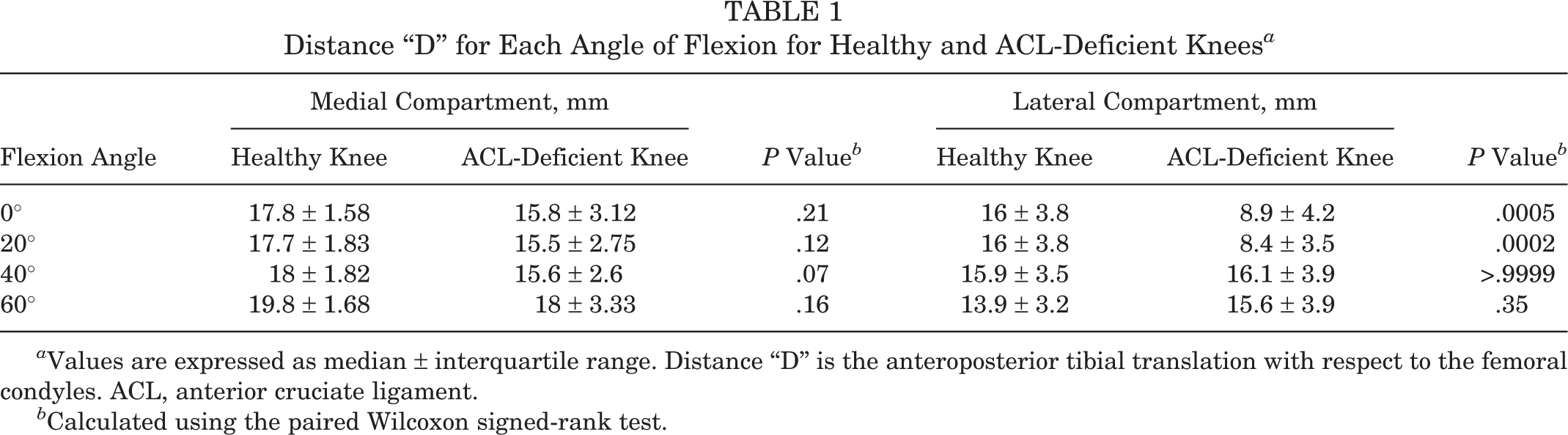
a Values are expressed as median ± interquartile range. Distance “D” is the anteroposterior tibial translation with respect to the femoral condyles. ACL, anterior cruciate ligament.
b Calculated using the paired Wilcoxon signed-rank test.
There were no statistical differences for anterior translation in the medial compartment between intact and ACL-deficient knees at all degrees of flexion (Table 1). At 0° of flexion in ACL-deficient knees, there was a nonsignificant anterior tibial translation of 2 mm in the medial compartment compaired with healthy knees that remained almost stable during flexion, from 0° to 60° (Table 1). However, in the lateral compartment, we observed significant differences in the anterior tibial translation between ACL-deficient and intact contralateral knees. At 0° and 20° of flexion, in ACL-deficient knees, there was an excessive anterior translation of the lateral tibial plateau compared with that of the healthy knee (7.1 mm, P = .0005 and 7.6 mm, P = .0002, respectively) (Table 1). Between 20° and 40°, the lateral plateau of ACL-deficient knees translated 7.7 mm posteriorly, whereas the medial compartment remained stable, reflecting a sudden external rotation of the knee around an axis of rotation that shifted medially (Figure 4). Between 40° and 60°, the tibia again began its internal rotation. However, in healthy knees, there was a progressive internal tibial rotation around a medial axis of rotation during flexion, especially from 40° to 60° (Figure 4).
For interobserver reliability, the Bland and Altman test showed good agreement between the 2 observers (Table 2). We had 16 conditions: 2 (healthy/ACL-deficient knees) × 4 (angles) × 2 (lateral/medial compartments). For each condition, the ICCs were homogeneous. The ICC was lower but acceptable for the medial compartment measures of healthy knees, between 0.8241 and 0.8638. The ICC was good for all the other conditions (>0.90).
Interobserver Intraclass Correlation Coefficients (ICCs) for Measurements by the 2 Observers a
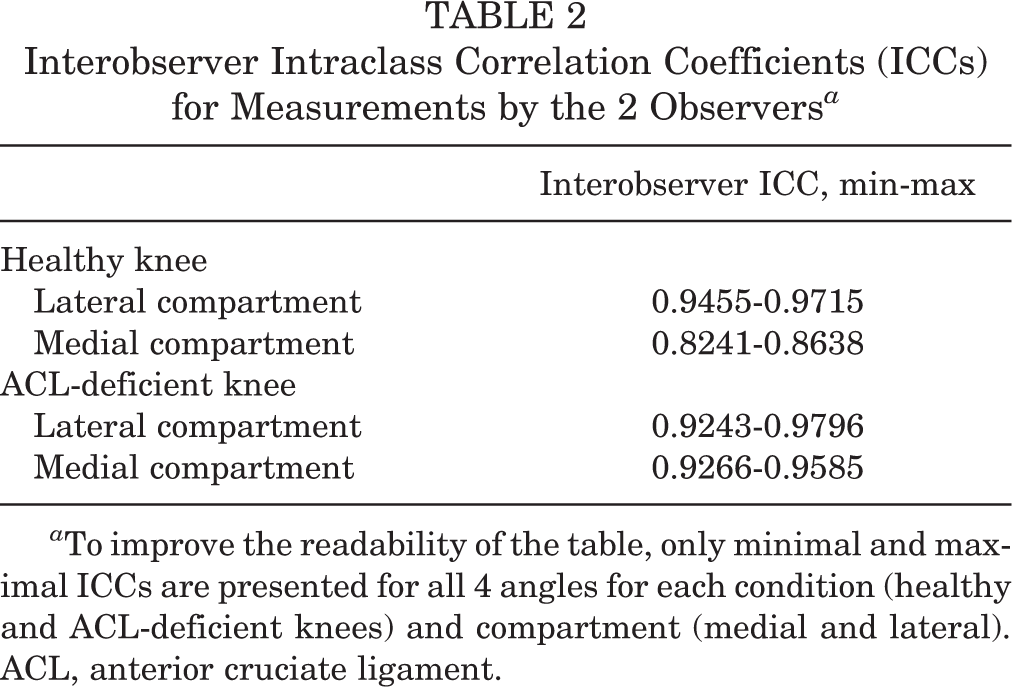
a To improve the readability of the table, only minimal and maximal ICCs are presented for all 4 angles for each condition (healthy and ACL-deficient knees) and compartment (medial and lateral). ACL, anterior cruciate ligament.
For intraobserver reproducibility, the ICC indicated good agreement for all measurements, between 0.8523 and 0.9871 (Table 3).
Intraobserver Intraclass Correlation Coefficients (ICCs) for Measurements by the 2 Observers a
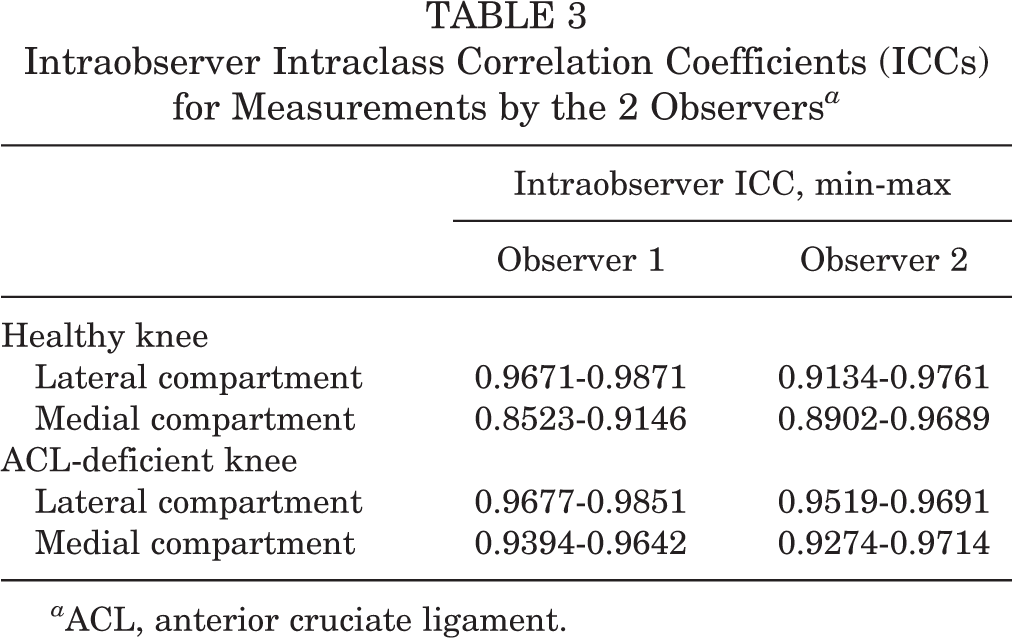
a ACL, anterior cruciate ligament.
Discussion
Different devices have recently been developed to quantify in vivo rotational knee laxity, reflecting the desire to measure rotational laxity of the knee for diagnostic purposes and evaluation of surgical outcomes. 35 Static devices 41 such as the Rotameter, 36,37 the Robotic Knee Testing Device, 7 and the Musahl and Tsai device 43 are easy to use but do not completely reflect the complexity of knee kinematics. More complex dynamic systems were developed to evaluate knee laxity, such as computer-assisted surgical devices, 27,56 dynamic Roetgen stereophotogrammetric analysis (dynamic RSA), 19 and dynamic radiostereometry (DSX). 45 These dynamic knee laxity measurement devices allow for 3-dimensional femorotibial analysis with controlled loads and motions but are often invasive, 44 require expensive laboratory environments, and expose the patient to radiation. 52 The KneeM device was designed to objectively and accurately measure tibiofemoral kinematics based on a reliable method available in daily practice, the MRI. The hypothesis was that the KneeM device would allow in vivo reproduction and analysis of knee kinematics during flexion of healthy and ACL-deficient knees.
In vivo knee kinematics observed in healthy and ACL-deficient knees with the KneeM device corroborated the results already described in experimental studies. The analysis of anterior tibial translation in each compartment demonstrated that the medial plateau for both ACL-deficient and healthy knees followed a nearly similar pattern of movement during flexion from 0° to 60°. It appears to be the stable compartment, as it was already described in the literature. 2,4,13,33,54 ACL deficiency had a small impact on the medial compartment.
However, the lateral compartment of the ACL-deficient knees allows more displacement, especially close to extension (0° and 20° of flexion). The absence of the ACL allows unchecked internal rotation to occur following the application of 100 N of anterior stress and 20° internal rotation from the KneeM device. This internal rotation occurs around a medial axis, close to the medial collateral ligament, as already described. 39,40,42 This medialization of the rotational center in ACL-deficient knees magnifies the displacement of the lateral tibial plateau.
The most interesting point was the lateral compartment kinematic between 20° and 40° of flexion in ACL-deficient knees. We observed a sudden external rotation of the tibia when the knee exceeds 20° of flexion despite the internal rotation and anterior tibial translation exerted by the splint. This phenomenon could be interpreted as a beginning pivot shift in the MRI. Various studies described the pathologic motions of the pivot-shift test. Matsumoto 40 used biplanar photography to analyze movements under a valgus torque in 29 fresh cadaveric knees. He described the pivot shift as a lateral tibial plateau relocation between 20° and 40° after it subluxed anteriorly. Bull et al 8 used an electromagnetic device to measure movement of 10 knees during ACL surgery. They found that between 0° and 25° of flexion, there was a progressive anterior tibial subluxation with internal rotation that reversed suddenly around a mean position of 36° ± 9° of knee flexion. This sudden reduction of the lateral plateau, which was anteriorly subluxed at the start of knee flexion, corresponded to the “pivot” phase of the pivot shift, therefore the tibia translated posteriorly and rotated externally. Our results documented that the “clunk” of the pivot shift could be observed with the KneeM device during MRI. However, the pivot shift is a dynamic and subjective clinical test. MRI and the KneeM device only document successive static positions of the couple motions of the pivot shift. Between 40° and 60° of flexion, ACL-deficient knees behaved like healthy knees. The lateral plateau translated anteriorly, unlike the medial plateau, which moved posteriorly, once again causing an internal rotation of the tibia. This corresponded to the physiological internal rotation that occurred during knee flexion, which has been observed in previous studies 3,20,24 and accentuated by the KneeM device that applied a fixed internal rotation of 20°.
The KneeM in vivo device based on MRI may be compared with other in vivo methods. Accelerometers or electromagnetic tracking devices have been successfully used to describe knee kinematics, but their accuracy is diminished by skin marker artifacts. 6,31 Computer-assisted surgery (CAS) also allows for dynamic clinical evaluation, but it is an invasive procedure that requires bone fixation to be accurate. 44 The KneeM device is easy to use, provided there is access to an open MRI. The problem of lack of space in a conventional MRI 1 was solved by using an open MRI. The MRI-compatible devices of previous studies applied neither an axial compression load, reproducing gravity without additional stress, 10,48,50 nor a sagittal force on the knee. 14,34 Logan et al 33 and Al-Dadah et al 2 assessed the tibiofemoral relationship using weightbearing MRI. They found that the most pronounced effect of the ACL deficiency was the anterior displacement of the lateral tibial plateau relative to the lateral femoral condyle compared with that of the medial side. The medial tibiofemoral relationship was unchanged compared with normal knees. But in these studies, no rotational force was applied. Knee kinematics were first studied with MRI under rotatory loads using the Slocum anterior lateral rotary instability test to stress the tibia rotating anteriorly and internally at 10° of flexion in an open MRI scanner. 21,46,47,51 They found significantly increased displacement of the tibia in the lateral compartment in ACL-deficient knees. But in their study, the stress was applied manually, thus altering the displacement. Haughom et al 18 and Kothari et al 29 upgraded their device with a custom-built walking boot that allowed internal or external torque to the foot. Espregueira-Mendes et al 16 evaluated both anteroposterior translation and rotatory laxity of the knee with their Porto-knee testing device (PKTD) that applied forces on the posterior proximal calf region using inflating cuffs. The PKTD allowed internal/external rotation by a footplate, but their first published study 16 was only performed at 30° of flexion in neutral rotation. None of these studies evaluated knee kinematics under combined loads during flexion. To our knowledge, the KneeM device is the first device that allows in vivo femorotibial kinematic evaluation applying anterior and rotational loading on ACL-deficient knees at different degrees of flexion (0°, 20°, 40°, and 60°) in an open-field MRI scan.
This study had some limitations that should be considered when interpreting the results. First, we did not compare the KneeM device to a gold standard device. Second, the reproducibility of different trials using the KneeM device was not evaluated. This protocol documented the reproducibility of the measurements but not the technique. Third, the evaluation was not performed in acute injuries. In this situation, apprehension and muscle spasm due to pain may significantly alter the measurements. Fourth, the MRI scanning was a series of different static positions rather than a true dynamic evaluation. Nonetheless, the static nature of the measure was not an obstacle since the results were equivalent to those of truly dynamic studies. Fifth, the pivot shift remained a subtle and subjective clinical test, and was therefore difficult to reproduce and objectively measure. It would be pretentious to say that we re-created exactly the pivot shift in the MRI but we tried, with this combined loading, to analyze the complex movement of the pivot shift in the MRI field. Moreover, all the patients had a grade 2 or higher pivot shift that made discriminant analysis of the pivot-shift grade between 20° and 40° of flexion impossible. Sixth, 4 flexion angles were examined at 20° increments rather than the entire range of flexion. Finally, the number of patients was small, even if it was a preliminary study before clinical implementation.
Conclusion
This preliminary study suggests that measurement of tibiofemoral movements in both compartments during flexion using the KneeM device was useful for quantifying rotatory laxity in ACL-deficient knees. Anterior translation in the lateral compartment was significantly increased at 0° and 20° in ACL-deficient knees compared with the contralateral intact knees. Moreover, this device seemed to allow a “mechanized pivot shift” and to reproduce the “pivot” phase in the MRI field between 20° and 40° of flexion. Future studies including a larger sample size and patients with various pivot-shift grades will allow the determination of threshold values for the side-to-side difference of anterolateral translation that correlate with the clinical grade of the pivot-shift test. Thereby, we could use this device to investigate the outcomes of ACL reconstructions using various surgical techniques.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.