
Abstract
Background:
Few studies have evaluated the effect of existing articular cartilage damage and sex on joint space measurements after isolated degenerative medial meniscus tears.
Purpose:
To determine what factors affected joint space width and narrowing in patients after removal of isolated degenerative medial meniscus tears.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 62 patients (15 women and 47 men) with all ligaments intact, no previous surgery to either knee, and an isolated degenerative medial meniscus tear removed in 1 knee were examined. The mean age at examination was 58.2 years at a mean follow-up of 9.4 years (range, 4-20 years). Subjective results were obtained with the International Knee Documentation Committee (IKDC) knee survey. Radiographs were taken using 45° weightbearing posteroanterior views. Midpoint and perceived minimum joint space width of the medial and lateral compartments of both knees were measured to the nearest 0.1 mm by 2 observers at different times, and they were blinded as to the previous measurements (Pearson intra- and interclass correlations, >0.93). Joint space narrowing was found by calculating the difference in joint space width between knees. Percentage of normal joint space loss was calculated by dividing joint space narrowing by the joint space width in the contralateral knee. Other factors considered were patient sex and Outerbridge grading of articular cartilage.
Results:
Women had a mean 1.5 mm less normal joint space width than men in the involved and noninvolved knees (P < .01). Mean joint space narrowing was 0.7 mm for both measurements. The mean ± standard deviation narrowing was 0.4 ± 1.2 mm for patients with grade 0-2 damage and 1.1 ± 1.3 for patients with grade 3-4 damage (P = .04). Five women (33%) and 3 men (6%) had narrowing of >50% of the normal joint space as measured in the noninjured knee (P = .016). The mean IKDC total score was 66.1 points for women, which was statistically significantly lower than the mean of 82.7 points for men (P < .01).
Conclusion:
Patients undergoing partial medial meniscectomy have greater joint space narrowing and lower subjective scores after surgery if they also have existing Outerbridge grade 3-4 damage. Women have less normal joint space than men, and more women than men experience >50% joint space narrowing after surgery.
Few long-term studies have been performed examining the outcomes of partial meniscectomy in stable knees with variable degrees of articular cartilage damage. In older populations, especially with intact anterior cruciate ligaments (ACLs), the medial meniscus is more prone to injury and is associated with degenerative tears more often than the lateral meniscus. 17 Menisci are a critical component of knee load transmission. 10,14 Thus, when performing a meniscectomy, it is advised to retain as much of the menisci as possible. 9 Meniscectomies can lead to joint space (JS) narrowing, femoral condyle flattening, and tibial ridge formation. 12
It has been reported that articular cartilage damage and meniscal degeneration are intertwined events. 17 However, little research has been conducted using radiographic and clinical results evaluating the disparities between partial meniscectomies for degenerative medial meniscus tears with varying severities of articular cartilage damage. Articular cartilage damage, or osteoarthritis (OA), can trigger decreased range of motion as well as low subjective satisfaction. 15,20 –22 Therefore, the purposes of this study were to measure JS width for involved and noninvolved knees in patients after isolated partial meniscectomy and to evaluate the factors of sex and articular cartilage damage on objective and subjective results.
Methods
As part of ongoing clinical outcome research, patients undergoing knee arthroscopy between April 1986 and March 2006 were entered into a database that included both demographic data and clinical information regarding specific intra-articular injuries and treatment (meniscus tears and treatment, articular cartilage damage, loose bodies, ligament injuries, sex, and date of birth). Articular cartilage damage was graded during arthroscopy based on Outerbridge 18 criteria (Table 1).
Outerbridge Classification of Articular Cartilage

All patients treated underwent identical postoperative rehabilitation programs for partial medial meniscectomy on stable knees. Rehabilitation emphasized the use of cold/compression therapy to limit a postoperative hemarthrosis, exercises to obtain full knee range of motion, early weightbearing, and a gradual strengthening program. 23
Power Analysis
Normative values obtained from 32 normal knees showed that the mean medial JS width at the perceived minimum (PM) location was 6.2 ± 0.8 mm, with a range of 4.2 to 8.0 mm. An a priori power analysis was performed to determine the required sample size needed to be able to detect 0.5 mm of JS width difference between the involved and noninvolved knee. Based on a 2-tailed test at 90% power, a significance level of .05, and a standard deviation of 0.8, a mean difference of 0.5 mm can be detected with a sample size of 48.
Our database showed 602 patients underwent partial meniscectomies for degenerative flap medial meniscus tears at the junction of the anterior two thirds and posterior one third of the meniscus. Each tear had a horizontal cleavage component, and the portion removed involved the inner two thirds of the posterior two thirds of the meniscus, leaving an intact superior peripheral rim. All ligaments were intact, and no other meniscal pathology was present. Of the 602 patients, 110 patients were randomly selected (SAS Survey Select; SAS Institute Inc, Cary, North Carolina, USA) and contacted via telephone to ask if he or she had any history of injury to the noninvolved knee or had undergone previous or subsequent surgery to either knee since initial partial meniscectomy. These criteria were used to ensure that the contralateral knee could be used for control comparisons, and the status of the contralateral knee was further deemed to be uninjured at the time of evaluation by confirming the patient’s history and the status of the joint to be normal on radiographs according to Fairbank 12 grading.
The project was approved by the institutional review board at our institution, and all patients gave informed consent to participate in this study. Fourteen patients were excluded at the time of contact because they stated they had a subsequent injury or surgery to the noninvolved knee, and 2 patients were excluded at the time of evaluation because radiographs showed arthritic changes in the noninjured knee. Eighteen patients could not be located, and 14 patients did not want to participate in the study. Thus, 62 patients were evaluated.
Subjective Follow-up
As part of the normal follow-up of patients undergoing knee arthroscopy, patients were asked on an annual basis after surgery to complete subjective surveys. The Cincinnati Knee Rating Score (CKRS) knee survey 24 was mailed annually since 1986, and the International Knee Documentation Committee (IKDC) subjective knee survey 13 was mailed annually since 2000. All surveys were self-administered to avoid biased responses and provided information on the symptoms and functional limitations induced by activities of daily living and sports. The most recent survey obtained from the patient at the time of radiographic follow-up was used for analysis.
Objective Follow-up
On clinical examination at long-term follow-up, patients were evaluated radiographically with a 45° flexion weightbearing posteroanterior (PA) view. 19 Two independent observers measured digitally enhanced radiographs for medial and lateral midpoint measurements 6,16,21 and PM measurements 2,3,5 to the nearest 0.1 mm perpendicular to the femur. Midpoints were determined by measuring the width of the medial and lateral femoral condyles and bisecting the line. The PM measurements were the narrowest gap viewed between the femorotibial joint, avoiding tibial ridges. Measurements of the involved and noninvolved compartments were made twice at different sittings by both observers, and the values were averaged. In all cases, the observer evaluated JS without knowledge of the side of meniscectomy or previous measurements. Pearson intra- and interclass correlation coefficient values were greater than 0.93 and 0.94, respectively.
Joint space width was reported as a raw value, while JS narrowing was calculated by subtracting the involved knee JS width from the noninvolved JS width. The percentage of JS narrowing for each patient was calculated by dividing the calculated JS narrowing value by the JS width value of the noninvolved knee and multiplying by 100.
Statistical Analysis
The status of the articular cartilage in the medial compartment was analyzed as a categorical value. Using the grading scale of Outerbridge, 18 patients with grade 0-2 damage were grouped as “normal,” and patients with grade 3-4 damage were grouped as “abnormal.” Descriptive statistics were obtained for mean JS width, mean JS narrowing, subjective scores, and demographics. A paired t test was used to determine if there were any differences between medial and lateral compartment JS width for patients. Student t tests were used to determine any statistically significant differences between Outerbridge grade categories for JS width in each compartment and between sexes for JS width and JS narrowing in each compartment. The Fisher exact test was used to determine whether there was a statistically significant difference between men and women for the percentage of patients with >50% JS narrowing. Statistical significance was set at P < .05. The data were analyzed using Base SAS, SAS Access, and SAS statistical software (SAS Institute Inc).
Results
Sixty-two patients returned for evaluation, and men accounted for 47 of the cases (76%), which is a similar distribution to the 75% of male patients who had surgery for degenerative medial meniscus tears during the same time period at our clinic. The mean age of patients at surgery was 50.3 ± 10.3 years (range, 18-73 years) for men and 44.4 ± 14.3 years (range, 15-60 years) for women, with a mean follow-up time of 9.4 ± 4.6 years (range, 4-20 years). The number of patients with existing Outerbridge grade 3-4 damage of the medial femoral condyle at the time of surgery was 6 of 15 women (40%) and 23 of 47 men (49%; P = .764).
The mean JS width was 3.9 ± 1.6 mm and 4.7 ± 1.9 mm for the involved medial PM and midpoint measurements, respectively (Table 2). The lateral compartment had statistically significantly more JS width than the medial compartment on average (P < .001).
Mean Joint Space Width Measurements a
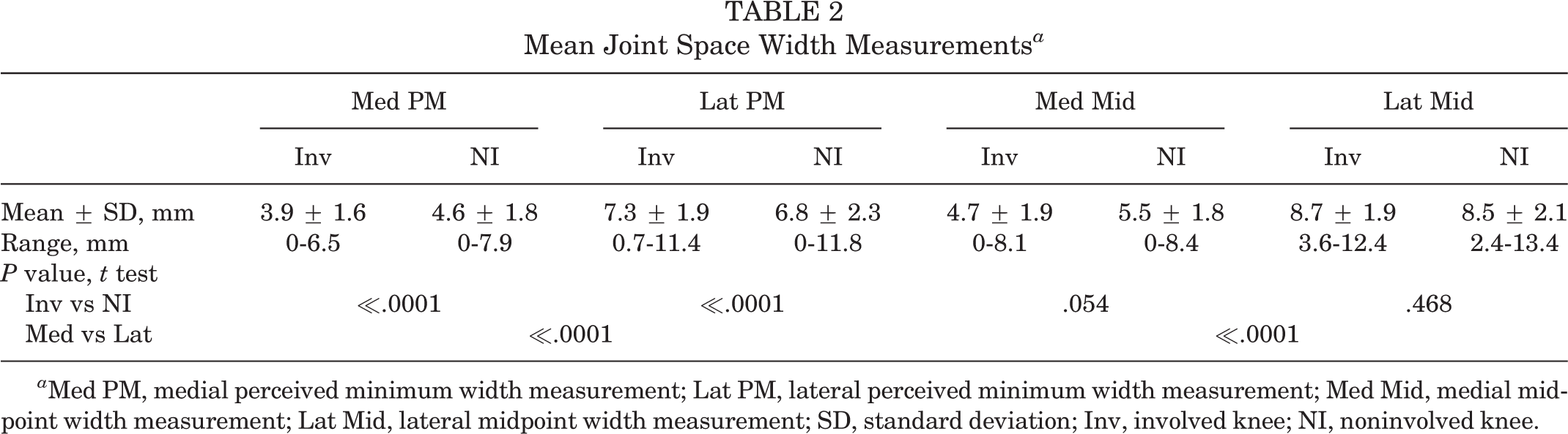
a Med PM, medial perceived minimum width measurement; Lat PM, lateral perceived minimum width measurement; Med Mid, medial midpoint width measurement; Lat Mid, lateral midpoint width measurement; SD, standard deviation; Inv, involved knee; NI, noninvolved knee.
The average JS narrowing for both medial PM and midpoint measurements was 0.7 mm (Table 3). Less than 20% of patients had >2.0 mm of JS narrowing compared with the opposite knee. Patients demonstrating grade 3-4 damage exhibited a mean of 0.7 mm more JS narrowing than patients experiencing grade 0-2 damage (PM measurement, P = .044; midpoint measurement, P = .024).
Mean Joint Space Narrowing a

a Joint space narrowing (JSN) was calculated by subtracting the joint space width of the involved knee from the noninvolved knee. JSN Med PM, difference of medial perceived minimum measurements between knees; JSN Med Mid, difference of medial midpoint measurements between knees; SD, standard deviation.
There was no correlation between age at the time of follow-up and total subjective scores (IKDC, r = −0.1771; CKRS, r = −0.1764). There was a moderate positive correlation between older age at time of follow-up and increased JS narrowing (PM measurement, r = 0.350; midpoint measurement, r = 0.330).
Sex Differences
When the patient population was analyzed according to sex, many statistically significant differences appeared. In comparison with men, women showed 2.3 mm and 1.6 mm less JS width for the medial PM and midpoint measurements, respectively (Table 4), in the affected knee. A similar difference between men and women was found for JS width in the noninvolved knee. Despite the significant difference in JS width between sexes, both groups had statistically similar JS narrowing measurements, which made JS narrowing proportionately greater for women than men. Five women (33%) and 3 men (6%) had JS narrowing of >50% of the normal JS width as measured in the uninjured knee (P = .016).
Medial Joint Space Width and Joint Space Narrowing for Women and Men a

a Values are expressed as mean ± standard deviation. Joint space narrowing (JSN) was calculated by subtracting the joint space width of the involved knee from the noninvolved knee. Med PM, medial perceived minimum width measurement; JSN PM, difference in perceived minimum width measurements between knees; Med Mid, medial midpoint width measurement; JSN Mid, difference in medial midpoint width measurements between knees; Inv, involved knee; NI, noninvolved knee.
Women had statistically significantly lower subjective total scores than men for both the IKDC and CKRS subjective surveys (Table 5). The total scores for women were not statistically significantly different based on articular cartilage status, whereas men with abnormal damage had statistically significantly lower subjective scores than men in the normal articular cartilage group.
Subjective Total Scores for Women and Men a

a SD, standard deviation; IKDC, International Knee Documentation Committee.
b Statistically significantly different (P < .05).
Discussion
With radiographic and subjective survey follow-up at a mean of 9 years after partial medial meniscectomy of a degenerative medial meniscus tear, this is one of the few studies with long-term results that measured raw JS width and calculated narrowing compared with the normal knee and examined how existing articular cartilage damage in the knee affected results after surgery. The results showed that the difference between the involved and noninvolved knee for PM JS width was statistically significantly less and the medial midpoint measurement showed a trend toward significance. Thus, patients may be prone to JS narrowing and decreased articular cartilage after partial medial meniscectomy of a degenerative tear.
Previous studies have related the onset of OA to medial knee pain and articular cartilage damage using objective and subjective measurements. 1,11,15,22,25 A recurrent factor of these studies is that JS width and JS narrowing after meniscectomies are highly predictive of OA. 4 Other authors have also shown that women recover worse than men after meniscectomies and are more likely to develop OA. 7,11,15
The results of our study showed JS narrowing was statistically significantly greater in the abnormal articular cartilage group. On average, patients with grade 3-4 articular cartilage damage had 0.7 mm less JS width than did patients in the normal articular cartilage group. In a 15-year follow-up study of arthroscopic partial meniscectomies similar to our patient population, Burks et al 6 found medial JS narrowing to be 0.7 mm compared with the opposite knee, which corroborates our findings. Cicuttini et al 8 reported that degenerative changes in the medial compartment are 4 times more likely than in the lateral compartment. Thus, when degenerative meniscus tears in the medial compartment are accompanied by articular cartilage damage, there appears to be an increase in the amount of detectable JS narrowing. This increase in JS narrowing may increase the likelihood of OA progression, disabling symptoms, subsequent surgical intervention such as partial or total knee arthroplasty, and having a lower patient satisfaction as assessed by subjective surveys.
It is important to consider whether 0.7 mm of JS narrowing compared with the opposite normal knee for patients would be considered clinically significant. A measurement difference of 0.7 mm JS narrowing is proportionally greater for women because the raw medial JS width was on average 1.5 mm less for women than men. The IKDC objective criteria considers >50% of JS narrowing compared with the normal knee as “abnormal,” and we would consider it as clinically significant for the presence of OA. Thirty-three percent of women and only 6% of men in our study had >50% JS narrowing. The statistically significantly less JS width for women compared with men in our study might have a greater effect on women to absorb shock and withstand the wear and tear of everyday use. The decreased JS width for women may also explain why they consistently had lower subjective total scores than men, regardless of the presence or absence of existing articular cartilage at the time of surgery.
A potential weakness of this study was that only 15 women were included in the patient population. However, our patient population mix for men and women was similar to that of the entire group of patients undergoing knee arthroscopy for degenerative medial meniscus tears, with 75% being male. Burks et al 6 also found a low percentage of women (17%) in their study who underwent partial medial or lateral meniscectomy.
Conclusion
Patients undergoing partial medial meniscectomy experience greater JS narrowing at an average of 9.4 years after surgery if they also have existing Outerbridge grade 3-4 damage at the time of surgery. Women were shown to have less JS width than men, and more women than men had >50% JS narrowing compared with the normal knee. Men who had abnormal articular cartilage at the time of surgery had lower subjective scores than men who had normal articular cartilage, whereas women had consistently lower subjective scores than men regardless of the status of the articular cartilage.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.