
Abstract
Background
Hepatitis B virus (HBV), hepatitis C virus (HCV), and diabetes mellitus are major global public health concerns associated with significant morbidity and mortality. However, there is no pooled evidence on the seroprevalence of HBV and HCV among diabetic patients in Africa. This study aimed to estimate the pooled seroprevalence and associated factors.
Methods
A systematic search of PubMed, Google Scholar, the Cochrane Library, and African Journals Online was conducted to identify relevant studies published from May 2012 to July 2025. Heterogeneity and publication bias were assessed using I2 and Egger's test, respectively. A DerSimonian-Laird random-effects model was used to estimate pooled prevalence, with sensitivity analysis performed.
Results
Among African diabetic patients, pooled HBV prevalence was 5.19%, while HCV prevalence was 11.34%. Multiple sexual partners increased HBV risk, whereas blood transfusion and prior hospitalization were associated with HCV.
Conclusion
HBV and HCV infections remain important public health concerns among patients with diabetes mellitus in Africa. Strengthening screening, vaccination, infection control, safe transfusion practices, and risk reduction education is essential.
Plain Language Summary Title
How Common are Hepatitis B and C Infections Among People With Diabetes in Africa, and What Increases the Risk?
Plain Language Summary
Hepatitis B and hepatitis C are viral infections that affect the liver and can cause serious illness or death if untreated. People with diabetes may be at higher risk of getting these infections due to frequent medical care, such as blood tests or hospital visits. However, there has been no clear overall estimate of how common these infections are among people with diabetes in Africa. In this study, we reviewed and combined results from multiple research studies conducted across Africa to better understand how widespread hepatitis B and C infections are among adults with diabetes. We found that about 5 out of every 100 people with diabetes had hepatitis B, while about 11 out of every 100 had hepatitis C. This shows that hepatitis C is particularly common in this group. We also looked at factors that increase the risk of infection. For hepatitis B, having multiple sexual partners was an important risk factor. For hepatitis C, the risk was higher among people who had received blood transfusions or had been hospitalized in the past. These findings highlight the need for better prevention efforts, including routine screening for hepatitis, improving infection control in healthcare settings, ensuring safe blood transfusions, expanding hepatitis B vaccination, and educating patients about how to reduce their risk.
Introduction
Diabetes mellitus (DM) is a long-term metabolic disorder marked by sustained high blood glucose levels. 1 It poses a significant global health challenge and is increasingly common, particularly in developing nations.2,3 The International Diabetes Federation (IDF) estimated that in 2024, diabetes affected approximately 589 million individuals worldwide, with 24.6 million cases reported in Africa. 4 Furthermore, the IDF anticipates a substantial rise in diabetes cases across the African continent by the year 2045. 5
Patients with DM exhibit a heightened vulnerability to infectious diseases, including viral infections such as hepatitis B (HBV) and hepatitis C (HCV), due to multiple immune system impairments associated with their metabolic condition. 6 DM-related chronic hyperglycemia compromises both innate and adaptive immunity, leading to dysfunctional neutrophil activity, reduced antigen-presenting cell function, impaired T-cell responses, and systemic inflammation, all of which diminish the body's ability to defend against infections.7–9 Individuals with type 2 diabetes are at increased risk of acquiring HBV and HCV infections; HCV infection risk is elevated approximately 3.5-fold compared to those without diabetes, and patients with diabetes often face worse clinical outcomes when infected, including higher rates of liver fibrosis, cirrhosis, and hepatocellular carcinoma.5,10–12 This immunosuppression, combined with more frequent exposure to healthcare settings such as finger-stick blood glucose testing, blood draws, and hospitalizations, further increases the likelihood of HBV/HCV transmission in diabetic populations.13–15
Hepatitis B and C viruses are primary viral causes of liver inflammation, which can develop into severe conditions such as cirrhosis, liver cancer (hepatocellular carcinoma), and even death. 16 As a result, they are significant drivers of chronic liver disease and its associated global health challenges. 17 According to the World Health Organization, 18 approximately 354 million people worldwide were living with chronic hepatitis B or C infections in 2022, including around 254 million with hepatitis B and 50 million with hepatitis C, while an estimated 6000 new cases are reported daily, nearly 60% of which occur in Africa, contributing to about 1.3 million deaths annually.9,18
Hepatitis B and C viruses share several important features, including their global distribution, especially in low- and middle-income countries, and similar transmission pathways, primarily involving exposure to infected blood and bodily fluids. 19 Common modes of transmission include sharing contaminated needles or syringes, receiving unscreened blood transfusions, and undergoing medical or dental procedures with inadequately sterilized equipment.20,21 Sexual contact and perinatal (mother-to-child) transmission also contribute to the spread, particularly in areas where preventive measures like vaccination and safe medical practices are limited. 20 In some regions, notably parts of Africa and Asia, transmission has been further fueled by inadequate infection control, traditional medical practices, and the reuse of medical equipment. 22 Both viruses show a strong affinity for hepatocytes (liver cells) and have the potential to cause long-term, chronic infections that may remain asymptomatic for years.23,24 If left untreated, these chronic infections can lead to severe liver-related complications such as cirrhosis, liver failure, and hepatocellular carcinoma, making them major global public health concerns. 25
Among diabetic patients, repeated exposure to medical interventions, such as finger-stick blood glucose testing, insulin injections, and frequent blood sampling, can increase the risk of HBV and HCV acquisition, especially in healthcare settings where infection prevention and control measures are suboptimal. 26 In addition, immunosuppression associated with chronic hyperglycemia may impair viral clearance and exacerbate disease progression in this population. 27
Despite a growing number of primary studies across African countries, the seroprevalence of HBV and HCV among individuals with DM, as well as the factors influencing these infections, remains inconsistently reported.28–30 In a region where both viral hepatitis and diabetes are significant and expanding public health challenges, the lack of a consolidated, region-wide estimate for HBV and HCV seroprevalence in this population hinders the development of effective, evidence-based interventions.31–33 This absence of synthesized data limits policymakers’ and healthcare providers’ capacity to implement targeted strategies for prevention, early detection, and management. Therefore, this systematic review and meta-analysis aims to address this critical gap by generating pooled prevalence estimates and identifying key risk factors associated with HBV and HCV infections among patients with DM in Africa.
Materials and Methods
Reporting and Registration Protocol
The review protocol was submitted to the Prospero database and assigned the registration number https://www.crd.york.ac.uk/PROSPERO/view/CRD420251103971. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist 34 was followed, as detailed in (Supplemental file 1).
Search Strategy
This systematic review included studies reporting the seroprevalence of hepatitis B and C viral infections and their associated risk factors among patients with DM in Africa, covering publications from May 2012 to July 2025. Relevant literature was comprehensively searched across multiple electronic databases, including the Cochrane Library, PubMed, Google Scholar, and African Journals Online. The search strategy employed combinations of keywords related to the population, condition/outcome, context, and exposures. Additionally, a snowballing approach was utilized to identify relevant references from selected articles. Boolean operators such as “AND” and “OR” were applied both individually and in combination with search terms. The comprehensive search protocol was first developed for PubMed and then adapted for implementation across other electronic databases. The strategy employed a structured combination of keywords and Boolean operators as follows: ((((seroprevalence) OR (prevalence)) OR (burden)) AND ((“hepatitis B virus”) OR (HBV) OR (“hepatitis C virus”) OR (HCV)) AND ((“diabetes mellitus”) OR (DM) OR (hyperglycemia)) AND (Africa)). EndNote version 8 was employed to organize retrieved citations and eliminate duplicates.
Eligibility Criteria
The inclusion and exclusion criteria were developed using the CoCoPop (Condition, Context, and Population) framework, defined as follows:
Inclusion Criteria
This review included only observational studies with cross-sectional or case-control designs that were conducted in African countries and published in English. Studies were considered eligible if they reported the seroprevalence of hepatitis B and/or C virus infections among individuals with DM or investigated at least one related risk factor. Only studies that used hepatitis B surface antigen (HBsAg), anti-HCV antibody testing, or enzyme-linked immunosorbent assay (ELISA) for diagnosing HBV and HCV were included. The review was restricted to studies published in the English language.
Exclusion Criteria
Studies without an abstract or full text, qualitative research, and anonymous reports were excluded.
Outcome Variable and Operational Definition
The primary outcome of interest was the seroprevalence of HBV and HCV infections among patients with DM in Africa. HBsAg serves as an indicator of active HBV infection, whether recent (acute) or chronic (long-standing). 35 In contrast, anti-HCV antibodies typically develop within 2 to 6 months following initial exposure during the acute phase and generally persist lifelong. A positive anti-HCV test indicates either a current (acute or chronic) or past resolved infection, whereas a negative result suggests the absence of active infection. 36
Study Selection
To efficiently manage and remove duplicate records, all retrieved studies were imported into EndNote version 8, a reference management software. Studies published from May 2012 to July 2025 were considered for inclusion in this review. Prior to full-text assessment of full-text articles, 5 reviewers independently screened the studies based on their titles and abstracts. Following this initial screening, the full-text articles were assessed according to predefined inclusion criteria. In cases where disagreements arose regarding the final selection of studies for the systematic review and meta-analysis, the reviewers held a consensus meeting with a 6th reviewer to resolve any discrepancies.
Data Extraction
Data were independently extracted by 5 reviewers using a structured extraction form. When discrepancies arose that could not be reconciled, a 6th reviewer facilitated a consensus discussion to resolve any outstanding disagreements. From each study, the following information was systematically collected: first author, year of publication, country and study location, sample size, target population characteristics, sampling approach, study design, and diagnostic methods. Outcome variables included seroprevalence of HBV and HCV infections measured by serological markers, and associated factors were extracted. The variables in this review were selected based on the fact that they were reported as significant factors in at least 2 studies.
Quality Assessment
The quality of the included studies was rigorously evaluated using the Joanna Briggs Institute (JBI) critical appraisal checklists (available at https://jbi.global/critical-appraisal-tools). 37 Two independent reviewers conducted a thorough assessment of each eligible study, carefully scoring them based on the reliability and validity of their findings. For observational studies, each domain within the checklist was rated as either 1 (Yes) or 0 (No), and the total score was calculated by summing these values. Using the critical appraisal checklist, methodological quality was evaluated for all included studies. Articles scoring <50% were categorized as low quality, 50% to 75% as good quality, and >75% as high quality. This cumulative score was then used to classify the overall quality of each study (Supplemental File 2). This structured appraisal ensured a consistent and objective evaluation across all included studies, thereby strengthening the credibility of the review's findings.
Statistical Analysis
The extracted data were first organized in Excel and then imported into STATA version 11 for statistical analysis. To estimate the pooled seroprevalence of hepatitis B and C viral infections and to identify associated factors among individuals with diabetes in Africa, a random-effects model was employed using the DerSimonian-Laird method. 38 The overall effect size, represented by the pooled seroprevalence with its corresponding 95% confidence interval (CI), was illustrated using a forest plot. To assess variability across studies, heterogeneity was evaluated using the I2 statistic,39,40 which quantifies the proportion of total variation due to true differences between studies rather than chance. I2 values range from 0% to 100%, with thresholds of 0%, 25%, 50%, and 75% indicating no, low, moderate, and high heterogeneity, respectively. Subgroup analyses were conducted based on study country, study design, and diagnostic techniques to explore potential sources of heterogeneity. In addition, a sensitivity analysis was performed to examine the influence of individual studies on the overall results. To evaluate publication bias, both visual inspection of funnel plots and statistical tests for small-study effects were used, 41 ensuring robustness and transparency of the findings.
Results
Study Selection and Identification
A systematic search across multiple databases was conducted for studies published between May 2012 and July 2025, yielding 2184 records: 1664 from PubMed, 433 from the Cochrane Library, 4 from Google Scholar, and 83 from African Journals Online (AJOL). After removing 1251 duplicate entries, a total of 933 unique studies remained for initial screening. Following the screening of titles and abstracts, 625 records were excluded due to irrelevance. Next, 308 articles were excluded for the following reasons: 87 were conducted outside the study setting, 11 were not published in English, 175 focused on non-diabetic populations, and 17 did not report prevalence data. Ultimately, 18 studies satisfied all inclusion criteria and were incorporated into the final systematic review and meta-analysis assessing the seroprevalence of hepatitis B and hepatitis C viral infections and their associated factors among patients with DM in Africa (Figure 1).

Flow diagram describing the selection of studies for systematic review and meta-analysis on the seroprevalence of HBV and HCV among patients with diabetes mellitus in Africa.
Characteristics of Included Studies
This review included 18 studies conducted across different African countries. The sample size for each study ranges from 100 to 1769. Of the 18 studies included, 9 were conducted in Ethiopia,14,29,30,42–47 2 in Egypt,48,49 2 in the Democratic Republic of Congo,11,50 2 in Cameroon,51,52 and 1 each in Ghana, 28 Nigeria, 53 and Tanzania. 54 Out of the 18 studies included, the majority (15 studies) used a cross-sectional design, while 3 used a case-control design. Regarding sampling techniques, 8 studies applied systematic random sampling, 6 studies adopted simple random sampling, and 2 studies relied on convenience sampling. Of the 18 reviewed studies, 7 reported on the prevalence of both HBV and HCV, 8 focused exclusively on HCV, and 3 assessed only HBV. Out of the total, 13 studies assessed seropositivity for HBsAg and anti-HCV using rapid test kits, while 5 studies relied on ELISA for the same markers (Table 1).
Summary of the Studies Included in the Systematic Review and Meta-Analysis on the Seroprevalence of Hepatitis B and Hepatitis C Viral Infections and Their Associated Factors Among Patients With Diabetes Mellitus in Africa (N = 18).

M/F, male:female; M, median; DM, diabetes mellitus; HBV, hepatitis B virus; HCV, hepatitis C virus; ELISA, enzyme-linked immunosorbent assay; HBV%, seroprevalence of HBV; HCV%, seroprevalence of HCV; NA, not applicable; FBCS, facility-based cross-sectional study; CBCS, community-based cross-sectional study.
The Pooled Seroprevalence of Hepatitis B and Hepatitis C Viral Infections Among Patients With DM in Africa
This systematic review and meta-analysis included 18 eligible studies to estimate the pooled seroprevalence of HBV and HCV infections among individuals with DM. The prevalence of HBV ranged from 2.2% in Tanzania 54 to 12.8% in Ethiopia. 43 For the HCV, the reported prevalence varied from 0% in Ghana 28 to 38.7% in Egypt 49 (Table 1).
A meta-analysis of 10 studies estimated the pooled seroprevalence of HBV among individuals with DM at 5.19% (95% CI: 3.14-7.23), with significant heterogeneity among the studies (I2 = 79.8%; p < .001) (Figure 2).

Forest plot showing the pooled seroprevalence of hepatitis B virus infections and their associated factors among patients with diabetes mellitus in Africa, 2025.
Similarly, a meta-analysis of 15 studies assessed the pooled seroprevalence of HCV infection at 11.34% (95% CI: 7.19-15.49) using a random-effects model. This analysis also revealed substantial heterogeneity, with an I2 statistic of 97.6% (p < .001) (Figure 3).

Forest plot showing the pooled seroprevalence of hepatitis C virus infections and their associated factors among patients with diabetes mellitus in Africa, 2025.
The I2 statistics from the forest plots demonstrate significant heterogeneity among the studies for both infections, with values of 79.8% (p < .001) for HBV and 97.6% (p < .001) for HCV. Due to this high degree of variability, sensitivity and subgroup analyses were performed to identify possible sources of heterogeneity.
Sub-Group Analysis
Based on the study design, diagnostic method, and study area, subgroup analysis was carried out. Subgroup analysis by study country indicated that Ethiopia reported the highest pooled prevalence of HBV at 6.36% (95% CI: 3.27-9.45), accompanied by substantial heterogeneity (I2 = 86.1; p < .001) (Figure 4).

Subgroup analysis of seroprevalence of hepatitis B virus infections among patients with diabetes mellitus in Africa based on country, 2025.
Similarly, the highest prevalence of HCV was observed in studies from Egypt, at 23.5% (95% CI: 6.2-53.19), with extremely high heterogeneity (I2 = 99.6%; p < .001) (Figure 5). In contrast, the lowest HCV prevalence was reported in a study conducted in Tanzania, where no cases were identified (Figure 5).

Subgroup analysis of seroprevalence of hepatitis C virus infections among patients with diabetes mellitus in Africa based on country, 2025.
In addition, we performed a subgroup analysis according to the study design. The combined seroprevalence of HBV among patients with DM varies by study design. Community-based cross-sectional studies (CBCS) showed a higher pooled seroprevalence of 8.5% (95% CI: 5.37-11.63); however, this estimate is based on a single study. In contrast, facility-based cross-sectional studies (FBCS) demonstrate a lower pooled seroprevalence of 4.81% (95% CI: 2.72-6.91), derived from multiple studies. Despite considerable heterogeneity within this subgroup (I2 = 78.8%, p < .001), the larger number of studies provides a more reliable and generalizable estimate of HBV seroprevalence among diabetic patients (Figure 6).

Subgroup analysis of seroprevalence of hepatitis B virus infections among patients with diabetes mellitus in Africa based on study design, 2025.
Moreover, the highest combined seroprevalence of HCV was observed in studies employing a case-control design (13.29%, 95% CI: 8.92-17.66; I2 = 74.2%, p = .021), which also exhibited substantial heterogeneity (Figure 7). This was followed by FBCS (11.60%, 95% CI: 5.36-17.84; I2 = 98.2%, p < .001), which showed considerable heterogeneity, and CBCS (11.34%, 95% CI: 7.19-15.41; I2 = 0.0%, p = .585), with no observed heterogeneity (Figure 7).

Subgroup analysis of seroprevalence of hepatitis C virus infections among patients with diabetes mellitus in Africa based on study design, 2025.
To explore variations in diagnostic approaches, this meta-analysis also performed a subgroup analysis based on the testing methods used. For HBV, the pooled seroprevalence was 4.99% (95% CI: 2.67-7.30; I2 = 81.3%, p < .001) in studies utilizing rapid diagnostic test (RDT) kits and 5.19% (95% CI: 3.14-7.23; I2 = 77.6%, p = .035) in those using ELISA, both indicating substantial heterogeneity (Figure 8).

Subgroup analysis of seroprevalence of hepatitis B virus infections among patients with diabetes mellitus in Africa based on diagnostic techniques, 2025.
In the case of HCV, the highest pooled prevalence emerged from studies employing ELISA, at 19.06% (95% CI: 7.05-31.08; I2 = 97.8%, p < .001), followed by those using rapid tests at 7.27% (95% CI: 3.94-10.60; I2 = 95.5%, p < .001). These findings highlight not only the variability in prevalence but also the influence of diagnostic methods on reported outcomes, with both categories showing considerable heterogeneity (Figure 9).

Subgroup analysis of seroprevalence of hepatitis C virus infections among patients with diabetes mellitus in Africa based on diagnostic techniques, 2025.
Publication Bias
Publication bias was assessed both visually, using funnel plots, and statistically, using Egger's test. The HBV funnel plot displayed a relatively symmetrical distribution of studies, indicating minimal publication bias (Figure 10).

Funnel plot assessing publication bias of HBV among patients with DM in Africa, 2025.
In contrast, the HCV funnel plot revealed noticeable asymmetry, suggesting potential publication bias and small-study effects (Figure 11).

Funnel plot assessing publication bias of seroprevalence HCV among patients with DM in Africa, 025.
Egger's test confirmed publication bias in studies reporting HCV prevalence (p = .013), while no significant bias was observed for HBV (p = .120).
Sensitivity Analysis
Sensitivity analysis was conducted to assess the influence of individual studies on the overall meta-analysis results. The estimates largely cluster around the original pooled prevalence, with overlapping CIs, indicating that no single study significantly alters the overall result when omitted. This suggests that the meta-analysis findings for HBV are stable and robust, with no outlier study exerting undue influence on the pooled estimate (Figure 12).
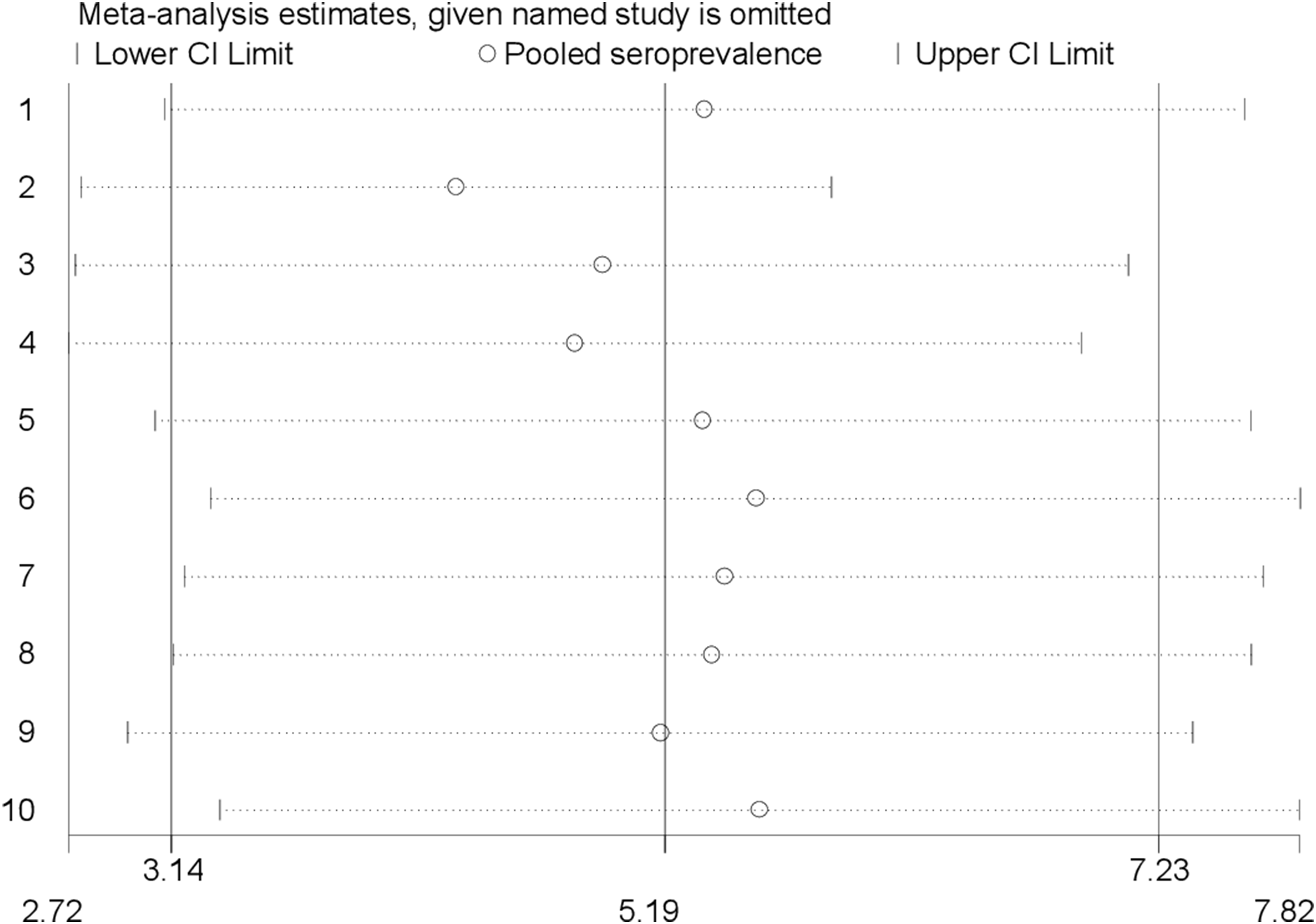
Sensitivity analysis for HBV to detect the effect of a single study on the pooled estimate, 2025.
Similarly, the meta-analysis for HCV demonstrates overall stability and reliability, as exclusion of most individual studies does not substantially change the pooled estimate (Figure 13).

Sensitivity analysis for HCV to detect the effect of a single study on the pooled estimate, 2025.
However, as shown by Eliah et al, 54 the exclusion of their study resulted in a marked change in the pooled estimate, indicating that their findings had a substantial influence on the overall results.
Factors Associated With HBV and HCV
The review revealed that having multiple sexual partners, a history of blood transfusion, and prior hospitalization are important factors associated with an increased risk of HBV and HCV infections in patients with diabetes mellitus across African nations. A total of 2 studies were included in the pooled analysis for HBV,30,43 and 3 studies for HCV49,53,55 to estimate the odds ratios. Among the 10 studies reviewed, 2 reported a statistically significant association between having multiple sexual partners and HBV infection. The pooled seroprevalence odds ratio (POR) for HBV among individuals with multiple sexual partners was 7.23 (95% CI: 2.70-19.39; I2 = 70.1%, p = .067). This finding implies that individuals with multiple sexual partners are over 7 times more likely to be infected with HBV compared to those without this risk factor, although moderate variability exists among the studies. Of the 15 studies, 3 studies found a significant association between a history of blood transfusion and HCV infection, while 2 others identified a significant link between previous hospitalization and HCV infection. A previous history of blood transfusion was significantly associated with HCV infection, with a POR of 2.45 (95% CI: 1.44-4.17). This indicates that individuals with a history of blood transfusion were approximately 2.5 times more likely to be infected with HCV compared to those without such a history. The heterogeneity among the included studies was moderate (I2 = 59.2%, p = .086). Furthermore, 2 studies demonstrated a significant link between prior hospitalization and HCV infection. The POR was 1.7 (95% CI: 1.35-2.15), suggesting that individuals with a history of hospitalization were 1.7 times more likely to have HCV compared to those without such a history.
Discussion
This systematic review and meta-analysis aimed to estimate the pooled seroprevalence of HBV and HCV infections, as well as their associated risk factors, among patients with DM in Africa. A total of 18 studies were included to determine the pooled seroprevalence of HBV and/or HCV. The results showed a pooled HBV seroprevalence of 5.19% (95% CI: 3.14-7.23), while HCV seroprevalence was notably higher at 11.34% (95% CI: 7.19-15.49), underscoring a significant public health concern in this population. The observed HBV prevalence falls within the World Health Organization's classification of intermediate endemicity, defined by an HBsAg prevalence of 2% to 7%. 9 This finding is consistent with previous meta-analyses reporting HBV prevalence rates between 4% and 8% in the general African population. 56 Similarly, the HBV seroprevalence reported here closely mirrors findings from a systematic review in the general population of China, which reported a prevalence of 6.89% (95% CI: 5.84-7.95). 57 However, it remains significantly higher than the 2.2% reported among the general population in Iran 58 and also exceeds the 3% (95% CI: 2-4%) estimated by a chain meta-analysis of the global general population. 59 These differences in HBV prevalence may be due to variations in sample size, diagnostic methods, regional endemicity, and awareness of infection prevention. Furthermore, the burden of HBV in many African countries is compounded by the incomplete implementation of universal vaccination programs, which continues to limit effective control of the disease.60,61
The pooled HBV prevalence observed among diabetic patients was lower than the 10.5% reported among people living with HIV (PLHIV) in Africa, 62 slightly lower than the 6.8% reported among healthcare workers, 63 and comparable to the 5.9% reported among pregnant women in sub-Saharan Africa. 64 This variation may be attributed to multiple factors, such as differences in participant profiles, national public health priorities, methodological inconsistencies, cultural behaviors, geographic variability, publication timing, and sampling approaches. The persistently intermediate HBV prevalence among diabetic patients likely reflects ongoing endemic transmission. 65 Moreover, routine diabetes-related medical procedures, such as insulin injections and blood glucose monitoring, may increase parenteral exposure, further compounding the risk of infection in this vulnerable group. 66
Conversely, the current study reveals a notably high pooled seroprevalence of HCV infection at 11.34% (95% CI: 7.19-15.49%) among diabetic patients in Africa. This rate significantly exceeds the World Health Organization's threshold for high endemicity, set at over 3%, 67 and also surpasses the estimated seroprevalence in the general population across the continent, which ranges from approximately 2.3% (95% CI: 1.59-3.00%) to 4.2% (95% CI: 3.71-4.66%) across the continent. 68 Similarly, our finding is significantly larger than the general global HCV prevalence, which is approximately 1.8% (95% CI: 1.4-2.3%). 69 The fact that HCV prevalence among diabetic individuals is 5 to 6 times higher than regional and global averages indicates a significantly increased risk in this population. This heightened vulnerability may be linked to frequent exposure to invasive medical procedures such as insulin injections, blood glucose monitoring, hemodialysis, or blood transfusions that are often part of diabetes care in African settings. 52 Furthermore, growing evidence points to a bidirectional relationship: not only are people with diabetes more susceptible to HCV, but chronic HCV infection itself may contribute to the development of insulin resistance and type 2 diabetes, further increasing the likelihood of co-occurrence. 70
The observed HCV prevalence also exceeded estimates reported among PLHIV (5.4%) and healthcare professionals (5.6%).62,63 These findings underscore a significantly higher burden of HCV infection in the diabetic population, suggesting a potential need for targeted screening and intervention strategies. This difference may be explained by multiple factors, including the frequent exposure of individuals with diabetes to medical procedures such as insulin injections, blood glucose monitoring, and other interventions involving blood contact or sharp instruments, which can increase the risk of HCV transmission, especially in healthcare settings where infection control practices may be inadequate. 71 Additionally, diabetes itself may compromise immune function, potentially increasing susceptibility to chronic infections like HCV. 8 PLHIV and healthcare professionals are often subject to targeted prevention and screening efforts, but diabetic patients are usually not routinely screened for HCV, leading to delayed diagnosis and higher cumulative prevalence. 72 These findings emphasize the necessity of integrated HCV screening and preventive strategies within diabetes care programs, especially in high-burden regions. This elevated seroprevalence points to concentrated risk factors such as unsafe medical practices, injection drug use, and inadequate awareness or testing, all of which require urgent public health attention. The considerable burden emphasizes the importance of scaling up HCV screening and enhancing linkage to care services, particularly in light of the availability of effective direct-acting antiviral treatments. 73
This systematic review and meta-analysis estimated the pooled seroprevalence of HBV and HCV infections and their associated risk factors among patients with DM in Africa. The findings showed a pooled HBV seroprevalence of 5.19% and HCV seroprevalence of 11.34%, indicating a considerable burden of blood-borne viral infections. These infections are particularly important in Africa, where overlapping epidemics of HIV, HBV, and HCV continue to pose major public health challenges. 74 Importantly, HBV, HCV, and HIV share common transmission routes, especially exposure to infected blood and unsafe medical practices. 75 This overlap increases the risk of co-infection, particularly in healthcare settings where infection prevention and control measures may be limited. 76 Therefore, the burden observed in this study should be interpreted within the broader context of HIV/AIDS care and co-infection management strategies in Africa. Patients with DM often require frequent healthcare visits, including blood glucose monitoring, injections, and hospital admissions, which may further increase their exposure to blood-borne pathogens. In settings with a high burden of HIV, these repeated healthcare interactions may amplify the risk of undiagnosed HBV and HCV co-infections, reinforcing the need for integrated chronic disease and infectious disease services. 77 Therefore, integrating HBV and HCV screening into HIV/AIDS programs and chronic disease management services could enhance early detection and help reduce the burden of co-infections across Africa.
Substantial heterogeneity was observed across the included studies for both HBV (I2 = 79.8%, p < .001) and HCV (I2 = 97.6%, p < .001), indicating considerable variability in prevalence estimates across studies. This heterogeneity may be attributed to differences in study design, sample size, geographic distribution, diagnostic methods used for viral detection, and publication period among the included studies. In addition, variations in healthcare access, infection prevention practices, HBV vaccination coverage, and the clinical characteristics of patients with DM across different African settings may have contributed to the observed inconsistencies.
Subgroup analysis by diagnostic method showed that the pooled HBV prevalence was 5.19% (95% CI: 3.14-7.23) in studies using ELISA and 4.99% (95% CI: 2.67-7.30) in those employing rapid test kits, suggesting similar detection rates between the 2 methods. In contrast, for HCV, a notable discrepancy was observed: the pooled prevalence among diabetic patients was significantly higher in studies using ELISA at 19.06% (95% CI: 7.05-31.08), compared to 7.27% (95% CI: 3.94-10.60) in those relying on rapid kits. This variation may reflect differences in test sensitivity, specificity, or study populations across diagnostic approaches.
The findings of this study revealed that the seroprevalence of both HBV and HCV among diabetic patients was higher when detected using ELISA compared to rapid test kits. This difference is likely due to the higher rate of false negatives associated with rapid screening methods. 78 Multiple studies have shown that ELISA generally provides greater sensitivity and accuracy for detecting both HBV and HCV infections than RDTs,79,80 making it a more reliable tool in clinical and epidemiological settings. Moreover, because of their exceptional specificity and sensitivity, ELISA assays are capable of detecting even very low levels of viral antigens or antibodies in serum. 81
This systematic review and meta-analysis identified key risk factors contributing to the pooled seroprevalence of HBV and HCV infections among individuals with DM. The most prominent factors included a history of multiple sexual partners, previous blood transfusions, and previous hospital admissions. In the case of HBV, individuals with multiple sexual partners were found to have a significantly higher risk of infection, with a POR of 7.23 (95% CI: 2.70-19.39), consistent with findings from several previous studies.30,43,82 This elevated risk is primarily linked to HBV's main routes of transmission, exposure to infected blood and bodily fluids, including semen and vaginal secretions. Engaging with multiple sexual partners increases the likelihood of encountering these infectious fluids, thereby amplifying the risk of HBV transmission.82–84
In addition, a history of blood transfusion was found to be an independent and statistically significant risk factor for HCV infection, with a POR of 2.45 (95% CI: 1.44-4.17). This indicates that individuals who have received blood transfusions are more than twice as likely to be infected with HCV compared to those who have not. This finding is in line with previous studies conducted among high-risk populations in Egypt 85 and among blood donors in Gabon, 86 both of which reported similar associations with HCV infection. Blood transfusion represents a biologically plausible route for HCV transmission, particularly in circumstances where donor blood is not rigorously screened for viral RNA (ribonucleic acid) or anti-HCV antibodies. 61 The virus can be directly introduced into recipients via contaminated blood products, and without stringent testing; infected transfusions pose a significant transmission risk.87,88 Repeated healthcare exposure in patients with diabetes, coupled with possible immune dysregulation, further elevates this risk. 89 These mechanisms together underscore the need for safe transfusion practices, especially in DM patients who may already face increased vulnerability to HCV infection. 90 This finding underscores the risk of HCV transmission through blood transfusions, particularly in settings with inadequate screening protocols. 91
A history of hospitalization was also significantly associated with an increased risk of HCV infection among individuals with DM, with a POR of 1.7 (95% CI: 1.35-2.15). This supports the role of healthcare-related exposures in HCV transmission and aligns with findings from a study of the general population in central Tunisia. 92 Hospital stays often involve exposure to invasive procedures, contact with blood or bodily fluids, and the use of shared medical equipment, all of which can facilitate HCV transmission. 92 Contributing factors such as inadequate sterilization practices, poor infection control between patient discharges and admissions, insufficient bed hygiene, and lapses in environmental sanitation may further elevate the risk of infection within healthcare settings. 93
Limitations of the Study
This systematic review and meta-analysis has some limitations. Most of the included studies were conducted in Ethiopia, with many other African regions not represented, which limits how well the findings apply to the whole continent. There was high variability in the results for both HBV (I2 = 79.8%) and HCV (I2 = 97.6%), likely due to differences in study design, diagnostic methods, and the populations studied. Sensitivity analyses found some outliers, especially in the HCV data, which might have affected the overall results. Additionally, differences in diagnostic tests, such as ELISA versus rapid tests, contributed to the varying prevalence rates reported. To improve future research, studies should include more diverse locations, use consistent diagnostic methods, and consider following patients over time.
Conclusion and Recommendations
The findings indicate an intermediate seroprevalence of HBV (5.19%) and a higher seroprevalence of HCV (11.34%) among patients with DM in Africa. Importantly, HBV infection was found to be associated with having multiple sexual partners, while HCV infection was associated with a history of blood transfusion and previous hospitalization. These results accentuate the urgent need for robust infection control measures and the effective implementation of targeted prevention and control strategies for both HBV and HCV. Furthermore, ensuring comprehensive HBV vaccination coverage among individuals with diabetes is vital to reducing the burden of HBV infection across the African region.
Supplemental Material
sj-doc-1-jia-10.1177_23259582261456437 - Supplemental material for Seroprevalence of Hepatitis B and C Viral Infections Among Patients With Diabetes Mellitus in Africa: A Systematic Review and Meta-Analysis
Supplemental material, sj-doc-1-jia-10.1177_23259582261456437 for Seroprevalence of Hepatitis B and C Viral Infections Among Patients With Diabetes Mellitus in Africa: A Systematic Review and Meta-Analysis by Ayanaw Dinku Abebe, Worku Chekol Tassew, Agerie Mengstie Zeleke, Yeshiwas Ayale Ferede and Jember Ayelgne Beyene in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-doc-2-jia-10.1177_23259582261456437 - Supplemental material for Seroprevalence of Hepatitis B and C Viral Infections Among Patients With Diabetes Mellitus in Africa: A Systematic Review and Meta-Analysis
Supplemental material, sj-doc-2-jia-10.1177_23259582261456437 for Seroprevalence of Hepatitis B and C Viral Infections Among Patients With Diabetes Mellitus in Africa: A Systematic Review and Meta-Analysis by Ayanaw Dinku Abebe, Worku Chekol Tassew, Agerie Mengstie Zeleke, Yeshiwas Ayale Ferede and Jember Ayelgne Beyene in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Abbreviations
Acknowledgment
We would like to thank all authors of the studies included in this systematic review and meta-analysis.
Ethical Approval and IRB Statement
We confirm that this study is a systematic review and meta-analysis based exclusively on previously published studies. Therefore, no primary data collection was performed. Ethical approval was not required for this study because it is based entirely on previously published literature and does not involve direct human participants, animal subjects, or identifiable personal data. As such, Institutional Review Board (IRB) approval is not applicable.
Author Contributions
ADA: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing—original draft, and writing—review & editing. WCT, AMZ, YAF, and JAB: data collection, literature review, manuscript revision, data extraction, validation, methodological review, statistical analysis, interpretation of results, and manuscript editing, Literature search, data curation, and critical revision of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used in this study are available from previously published studies included in the systematic review and meta-analysis.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.