
Abstract
Background
Unhealthy alcohol use is common among people affected by HIV and is associated with poor treatment outcomes, but its impact among adolescents and young adults living with HIV (AYAH) in Africa is rarely explored. This study aimed to estimate the prevalence of unhealthy alcohol use and examine its association with HIV viral suppression among AYAH in Uganda and Kenya.
Methods
We conducted a cross-sectional survey among AYAH enrolled in the intervention arm of the SEARCH Youth study, a life stage based trial evaluating an intervention to improve viral suppression among youth aged 15 to 24 years. At their 30 to 36 month follow-up visit, AYAH were interviewed for self-reported alcohol consumption using the Alcohol Use Disorders Identification Test—Consumption (AUDIT-C, modified to cover the last 3 months) and tested for phosphatidylethanol (PEth), a blood-based biomarker of prior month alcohol consumption. Unhealthy alcohol use was defined as AUDIT-C ≥ 3 for females, ≥4 for males or PEth≥50 ng/mL. We estimated underreporting of alcohol use among those with PEth ≥50 ng/mL and examined the association between unhealthy alcohol use and viral non suppression (≥400 copies/mL) using logistic regression, adjusting for gender, age, and country.
Results
Unhealthy alcohol use was assessed in 715 AYAH; 409 (57.0%) in Uganda and 309 (43.0%) in Kenya. Eighty percent were female, median age at the time of the survey was 24 years (interquartile range: 21-26), and 95.0% were virally suppressed. The prevalence of unhealthy alcohol use was 25% overall, higher among males than females, Ugandan than Kenyan AYAH and increased with age. Unhealthy alcohol use was associated with nearly 3-fold higher odds of viral nonsuppression (adjusted odds ratio = 2.80, 95% CI [1.19-6.58], P = .02). Almost half (46.0%) of those with PEth≥50 ng/mL underreported unhealthy alcohol consumption.
Conclusions
After adjusting for sex, age, and country, unhealthy alcohol use was associated with viral nonsuppression among AYAH receiving the multilevel SEARCH Youth intervention, suggesting a need for targeted interventions. However, underreporting of unhealthy alcohol use may be a barrier to identifying those at risk. The rising prevalence of unhealthy alcohol use with age suggests there may be a window for early intervention.
Plain Language Summary Title
The Effect of Unhealthy Alcohol use on HIV Viral Suppression Among Adolescents and Young Adults Living with HIV in Kenya and Uganda
Plain Language Summary
Why did we conduct this study?
Unhealthy alcohol use is common among people living with HIV, and is known to interfere with treatment in adults, but it has rarely been explored among youth in Africa with HIV. Unhealthy alcohol use means drinking in a manner or quantities that increase health risks. In this study we examined how common unhealthy alcohol use was among youth living with HIV in Kenya and Uganda, and whether it was linked to viral non suppression. We also compared self reported use with blood tests to see if young people report their drinking accurately.
How was the study conducted?
We studied youth who started receiving improved HIV services when they were between 15 and 24 years. We asked them to answer questions about their drinking over the past three months and also tested them using a blood test that can detect recent unhealthy drinking. We then estimated how common unhealthy drinking was based on age, sex and country as well as its connection with viral suppression.
What did we find?
We found that one in four youth engaged in unhealthy drinking which was more common among males, and Ugandan youth, and increased with age. Nearly half did not report their alcohol use accurately when asked about it. Unhealthy alcohol use was linked to a much higher likelihood of having viral non suppression.
What lessons do we learn from these findings?
These findings show that unhealthy alcohol use is common and undermines HIV control warranting inclusion of alcohol use interventions in HIV services. However, underreporting could undermine interventions. The fact that unhealthy alcohol use increases with age suggests that there is room for early intervention.
Introduction
Despite global efforts to improve access to antiretroviral therapy (ART), in 2024, nearly 2 million people receiving ART did not achieve viral suppression.1,2 Adolescents and young adults living with HIV (AYAH) aged 15 to 24 years consistently achieve lower rates of care engagement and viral suppression compared to adults.3–5 Improving viral suppression in this age group is critical for achieving global HIV targets and reducing onward transmission. 6
Growing evidence shows that unhealthy alcohol use, defined as drinking in a manner or quantities that increase the risk for health consequences, is a key barrier to achieving viral suppression.7,8 Among adult populations, unhealthy alcohol use is associated with a lower probability of HIV testing, failure to start ART once diagnosed, and poor adherence to ART.8–10 It is also implicated in progression to AIDS related illnesses, including tuberculosis.8,11 However, despite these established effects in adults, the effect of unhealthy alcohol use on outcomes among AYAH in Africa is largely unexplored.
Africa accounts for nearly 80% of AYAH. 12 The scarcity of data on unhealthy alcohol use in this demographic represents a critical gap that hinders targeted interventions. Adolescence and young adulthood are periods of marked cognitive and social transition characterized by disinhibition and peer influence, often leading to risky behaviors, including unprotected sex and unhealthy drinking.13,14 Indeed, unhealthy alcohol use is the predominant form of drinking among adolescents and young adults in Africa, and several studies have linked unhealthy alcohol use and risky sexual behavior.15–18 Young people's alcohol use is commonly influenced by exposure to alcohol marketing, the desire for conformity as well as coping with psychosocial stressors.15,19,20 For AYAH who must navigate the challenges of a stigmatized chronic disease, these psychosocial stressors are likely amplified.15,21 Additionally, evidence of under reporting of alcohol use among adults living with HIV suggests that this behavior may also be underreported among AYAH. 22
To address these evidence gaps, we conducted a study to explore alcohol use and viral non suppression among AYAH enrolled in the intervention arm of the SEARCH Youth study, which evaluated a life stage informed intervention designed to address psychosocial, behavioral, and structural barriers to HIV care seeking among AYAH in Kenya and Uganda. 23 The aims of the alcohol use survey were (a) to estimate the prevalence of unhealthy alcohol use among AYAH by self-report and objectively by the blood alcohol biomarker, phosphatidylethanol (PEth); (b) to evaluate the association between unhealthy alcohol use and viral nonsuppression, and (c) to determine the level of under reporting of unhealthy alcohol use. We hypothesized that AYAH with unhealthy alcohol use would have lower HIV viral suppression rates than those without unhealthy alcohol use.
Materials and Methods
Study Design and Context
We conducted a cross sectional study on alcohol use among AYAH who were enrolled in the intervention arm of the SEARCH Youth study (NCT03848728). Data for the alcohol use substudy was collected between October 2021 and April 2022, after participants had completed 30 to 36 months of follow up in the parent SEARCH youth study. The reporting of this study is in accordance with the “Strengthening the Reporting of Observational Studies in Epidemiology” checklist (supplements).
The SEARCH Youth study was a cluster randomized trial that evaluated the effect of a multilevel intervention on viral suppression among AYAH in rural south western Uganda and western Kenya. The intervention arm showed significantly higher rates of viral suppression (HIV RNA< 400 copies/mL) at 2 years of follow up compared to the control (relative risk = 1.10, 95% CI [1.03-1.16]). 23 Briefly, the clusters consisted of 28 rural health clinics providing free HIV treatment services. Clinics were randomly assigned to the intervention or control arms (n = 14 each), with equal distribution between Kenya and Uganda. AYAH were eligible for enrollment in the parent SEARCH Youth study if they were 15 to 24 years old and willing to receive HIV care in the study clinics.
In the intervention arm, AYAH received standard HIV services which included peer to peer support in addition to the SEARCH Youth intervention as follows. During routine visits every three months, AYAH were assessed for the presence of recent life events, alcohol use, substance use, social support, and HIV disclosure needs. 23 Viral load tests were conducted every six months and AYAH with virologic nonsuppression received counseling within 72 hours of the test. The viral load test was repeated every 2 to 4 weeks with counseling until AYAH achieved virologic suppression. Support for virologic non suppression included counseling to identify barriers to medication, referral for mental health services, home visits for assisted disclosure, and alternative clinic access options. At the time of data collection for this alcohol use substudy, counseling for alcohol use was provided in accordance with the HIV treatment guidelines in both countries and consisted of general advice encouraging AYAH to reduce alcohol consumption. 24
Participants and Procedures
Eligibility
All AYAH enrolled in the intervention arm (14 clinics) of the parent SEARCH Youth study were eligible to participate in the alcohol use substudy if they had neither transferred out care to another clinic nor withdrawn from the study and could provide written informed consent to participate.
PEth Specimen Collection and Processing
Blood samples for both plasma viral load and PEth measurement were collected at the same study visit as the alcohol use survey. After a venous blood draw, we prepared dried blood spots to test for PEth. Three 50 µL drops of blood were pipetted onto a 1 Whatman 903 filter paper, dried for atleast 24 hours, and then stored with a desiccant in a −8 °C freezer at the research laboratories in Kenya and Uganda. The DBS were later transported to the U.S. Drug Testing Laboratory which used liquid chromatography in tandem with mass-spectrometry (LC/MS/MS) to test for the level of the PEth, using previously established methods. 25
Alcohol Use Measures
We assessed alcohol use through self-report with the Alcohol Use Disorders Identification Test—Consumption (AUDIT-C) which was modified to capture drinking in the last three months, and through the PEth blood biomarker. The AUDIT-C is a three item screening test used to identify individuals engaging in unhealthy drinking or with alcohol use disorders. It is scored from 0 to 12 and has demonstrated good sensitivity and high specificity for detecting alcohol use disorders in previous studies among adults.26,27 In males, an AUDIT-C score of 4 or more is considered positive for unhealthy alcohol use, while 3 or more is positive for females. 26
PEth is a whole blood biomarker of alcohol consumption correlated with prior month alcohol use.28–30 We defined a positive PEth test for unhealthy alcohol use as a PEth value of ≥50 ng/mL, consistent with previous research indicating that cutoffs of 40 to 60 ng/mL detect >1 to 2 drinks per day on average. This cutoff improved specificity for identifying moderate to heavy drinking compared to lower cutoffs used for abstinence or low alcohol consumption. 31 We created a combined PEth/self-report measure of unhealthy alcohol use as our primary predictor of interest, defined as a positive AUDIT-C or PEth, to increase sensitivity compared to using either measure alone.
Viral Nonsuppression
Viral nonsuppression on the day of survey completion was the primary outcome. Viral load was considered nonsuppressed if the value was ≥400 copies/mL. Briefly, a 5 mL venous blood sample was drawn, transported to the testing hubs, and centrifuged to separate plasma. Plasma RNA was evaluated using the Xpert HIV-1 viral load assay (Cepheid, Sunnyvale, CA, USA) with a lower limit of 40 copies/mL.
Statistical Analysis
We describe unhealthy alcohol use, viral non suppression, and demographic characteristics, including age at alcohol interview (≤20 years, 21-24 years, and 25-29 years), sex, and country of residence using frequencies and proportions. We used multivariate logistic regression to estimate the association between unhealthy alcohol use and viral nonsuppression. Models were adjusted for age and sex, selected a priori from literature. We also controlled for country because of the marked difference in alcohol use prevalence among AYAH in Uganda and Kenya and the potential for differing levels of viral non suppression by country.21,23 Our regression estimates, thus, evaluate how alcohol use predicts viral non suppression, after adjusting for age, sex, and country. We also estimated the prevalence of under reporting of unhealthy alcohol use by tabulating the proportion screening negative on AUDIT-C among those with PEth≥50 ng/mL.
Results
Participant Characteristics
Of 995 AYAH enrolled in the intervention arm of the SEARCH Youth trial between February 2019 and December 2020, we reached and completed surveys and PEth testing for 715 (72%), including 406 (57%) from Uganda and 309 (43%) from Kenya. Participants had experienced 30 to 36 months of follow up in the parent SEARCH Youth study, with a median age of 24 years (interquartile range [IQR] 21-26) at the time of the alcohol use sub study and 80% were female. Viral loads were available for 691 of 715 participants. Missing viral loads were due to test run failures (n = 19), indeterminate results (n = 3), and missing results (n = 2). At the time of conducting the alcohol use substudy, 37 (5%) of participants had viral nonsuppression.
Prevalence of Unhealthy Alcohol Use
Using the combined self-report and biomarker measure, the prevalence of unhealthy alcohol use was 25%. Within subgroups the prevalence was 36% among males and 22% among females. The prevalence increased with age, from 6% among participants aged 20 years or younger to, 24% in those aged 21 to 24, and 32% in those aged 25 to 29 years old. The prevalence of unhealthy alcohol use was more than 5 times higher among Ugandan AYAH (38%) compared to Kenyan AYAH (7%). See Table 1 for details.
The Prevalence of Unhealthy Alcohol Use by Several Characteristics Among Adolescents and Young Adults Living With HIV in Rural Kenya and Uganda.
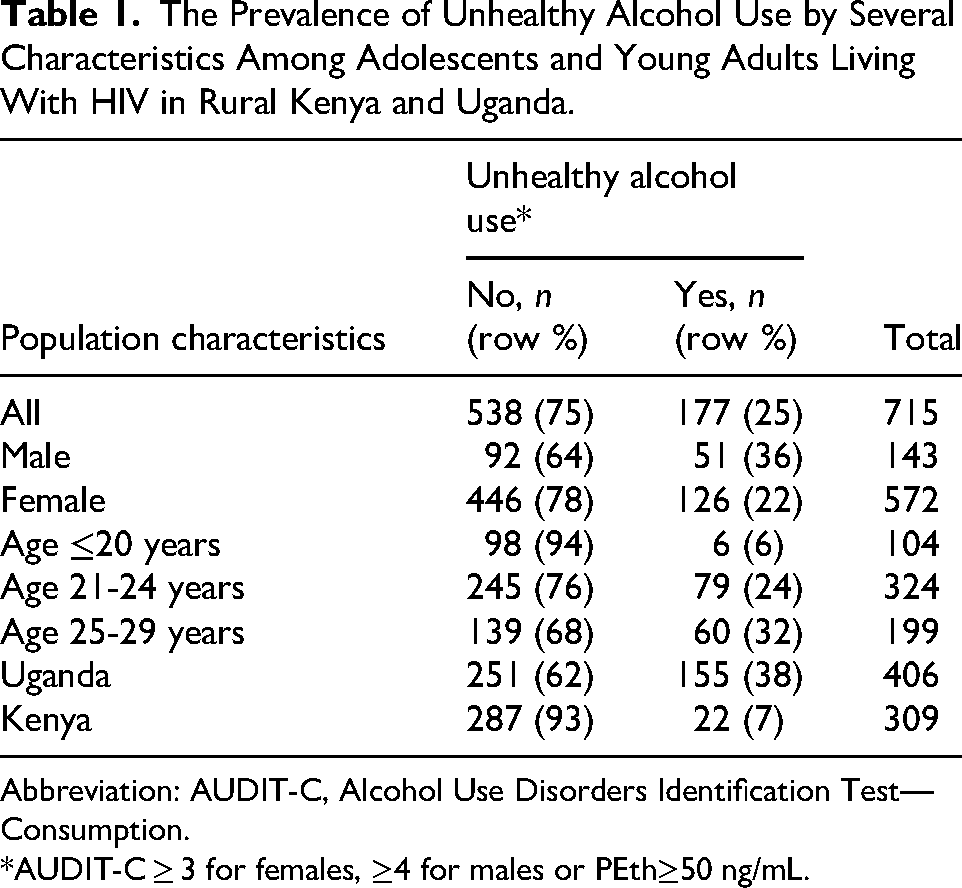
Abbreviation: AUDIT-C, Alcohol Use Disorders Identification Test—Consumption.
*AUDIT-C ≥ 3 for females, ≥4 for males or PEth≥50 ng/mL.
Association of Unhealthy Alcohol Use With Viral Nonsuppression
A higher proportion of participants with unhealthy alcohol use (8%) had viral non suppression (HIV RNA>400 copies/mL) compared to those who did not have unhealthy alcohol use (5%). When adjusted for age, country and gender, participants with unhealthy alcohol use had 2.8 times the odds of viral non suppression (adjusted odds ratio: 2.80, 95%CI [1.19-6.58], P = .02) compared to those who did not.
Underreporting Unhealthy Alcohol Use Overall and by Gender
There were 141 participants with PEth ≥50 ng/mL, of these, 46% were AUDIT-C negative, suggesting underreporting of unhealthy alcohol use (Table 2). Similar proportions of females (46%) and males (47%) underreported unhealthy alcohol use.
AUDIT-C Positive Versus PEth Positive results Among AYAH in Rural Kenya and Uganda.

Abbreviations: AUDIT-C, Alcohol Use Disorders Identification Test—Consumption; PEth, phosphatidylethanol; AYAH, adolescents and young adults living with HIV.
AUDIT-C positive is ≥3 for females, ≥4 for males.
*1 missing result.
Discussion
In this alcohol use substudy conducted among AYAH who were enrolled in the person centered SEARCH Youth intervention in Kenya and Uganda, the prevalence of unhealthy alcohol use was 25%. The prevalence was higher among males, AYAH from Uganda, and in older participants. Significantly, despite reaching an overall viral suppression rate of 95%, unhealthy alcohol use was associated with nearly three times higher odds of viral non suppression in this cohort. Moreover, using the blood biomarker, PEth, 46% of participants with unhealthy alcohol use underreported their alcohol consumption on the self-report tool.
Our findings have public health implications; first, this is one of the few studies to objectively describe the prevalence of unhealthy alcohol use among AYAH in Africa, highlighting the persistent and negative impact of alcohol use on viral suppression. Additionally, our results emphasize the need to address emerging unhealthy alcohol use and the limitations of relying solely on self-reported measures of alcohol use in this demographic.
One out of 4 AYAH in this study had unhealthy alcohol use, a finding similar to that observed among 15 to 24-year-old fisherfolk (both with and without HIV) in south central Uganda using a lower PEth cut off of 20 ng/mL (compared to the 50 ng/mL cutoff that we used here). 32 Given our higher PEth threshold, our results are likely conservative estimates. Similarly, among adults living with HIV in Africa, self-reported unhealthy alcohol use ranged from 22% to 29%.10,33,34 Overall, while there is considerable variation in tools and measures used across studies, these data along with others, suggest a considerable level of unhealthy alcohol use in AYAH.
Globally, unhealthy alcohol use is lowest among adolescents aged 15 to 19 years and increases with age, peaking among young adults aged 20 to 24 years. 35 We observed a similar pattern in our study, with a 5-fold increase from late adolescence to young adulthood, suggesting heightened vulnerability during the transition to adulthood. While longitudinal studies may better explain these trajectories, our results highlight the importance of early screening and intervention, as well as strengthening age appropriate alcohol prevention and care continuity to reduce harm.
We found that the prevalence of unhealthy alcohol use was 5 times higher in Uganda than in Kenya. This disparity likely reflects broader social trends in population level alcohol consumption driven by public policy and enforcement. Uganda has one of the highest per capita alcohol consumption rates in the world. 18 When compared to Kenya, per capita drinking is 12.2 L of absolute alcohol in Uganda compared to 2.0 L in Kenya. 18 In addition, unrecorded alcohol, alcohol produced and used outside the formal market accounts for 86% of consumption in Uganda, compared to only 37% in Kenya. 35 Unrecorded alcohol is often more accessible than commercial alcohol, which may increase the likelihood that young people develop unhealthy patterns. 36 It is likely that Kenya's enforceable alcohol policy, with legally binding restrictions on marketing and sales, along with government supported community level interventions to limit access to alcoholic beverages contributes to a lower prevalence of alcohol use compared to Uganda.35,37 Uganda could perhaps introduce and enforce similar policies to reduce its high rates of alcohol use.
Globally, males report significantly higher rates of unhealthy alcohol consumption compared to females, driven by social norms that condemn female alcohol use. 35 In our study, male AYAH were 1.6 times more likely to engage in unhealthy alcohol use than their female counterparts. This disparity is similar to that seen in some adult populations although other studies among adolescents and young adults report smaller disparities. 33 For example, among fisher folk age 15 to 24 years in Uganda, the prevalence of unhealthy alcohol use was 24.6% in males compared to 15.9% in females, while among youth in an urban slum, there was no sex disparity.17,32
While 95% of participants in our study achieved viral suppression, alcohol use remained a significant barrier; participants with unhealthy alcohol use had nearly 3 times higher odds of viral non suppression. Considering that only AYAH who received the SEARCH Youth intervention and remained engaged in care after 30 to 36 months of follow up were interviewed, this association likely underestimates alcohol's true effect in this population. Similar findings were observed in a review of studies involving adult populations in Sub Saharan Africa.33,38 The persistence of alcohol-related barriers to viral suppression despite an effective multilevel intervention suggests that behavioral risk factors require dedicated, actively embedded interventions in youth HIV care models.
In our study, nearly half of the participants with biomarker-measured unhealthy alcohol use under reported their consumption, with similar proportions of males and females. Few studies have examined this phenomenon among AYAH; however, under reporting of alcohol use has been observed in adult studies of people living with HIV in Africa.7,39 In one study, twice as many participants underreported alcohol use when interviewed by a healthcare provider compared to research staff, which is likely related to social desirability bias, as may be the case with our study. 22 In Tanzania, people living with HIV preferred to discuss problematic alcohol use with their counselors rather than clinicians, suggesting that the job position should be considered when designing counseling interventions for unhealthy alcohol consumption. 40 Moreover, the prevalence of unrecorded alcohol and communal drinking norms likely influence self-reported screening, since concentrations and amounts consumed may not be known, leading to under estimation of consumption.36,41 Under reporting could hinder recognition of alcohol related problems in clinical care, resulting in missed opportunities for screening, as well as reducing the potency of alcohol related counseling and interventions. While routine use of biomarkers may not be feasible in all settings, these findings highlight the need for improved screening tools and counseling approaches that reduce social desirability bias.
Our study had some limitations. First, the cross sectional design means we cannot necessarily infer causation between unhealthy alcohol use and viral non suppression. Our goal was to evaluate how alcohol use predicted viral non suppression after adjusting for established risk factors such as age and sex, as well as controlling for the imbalance in alcohol use by country. Due to the rarity of some outcomes, we did not control for all possible confounders. Second, a formal sample size was not calculated for this substudy; however, the parent study's sample was powered for intervention effectiveness supporting the adequacy of the substudy for exploratory analyses. Third, underreporting alcohol consumption was likely magnified because the alcohol use survey was administered by the same providers who had been treating the participants over several months, and AYAH may not have wanted to disappoint their providers. Lastly, the generalizability of our results may be affected by the study population and timing of the alcohol use evaluations. Our analyses focused on AYAH who received the SEARCH Youth intervention and remained engaged in the study after 30 to 36 months of follow up. It is likely that rates of viral non suppression would be lower and the impact of alcohol use more pronounced in a broader population that had not received the SEARCH Youth intervention, and or had disengaged from care. Indeed, several studies have shown that unhealthy alcohol use is associated with nonengagement with HIV care services among adults and observing similar outcomes in this younger population would suggest that the problem is larger than what we found. Despite these limitations, this research was strengthened by a large sample size and objective measurement of alcohol use.
Implications and Conclusion
Our findings highlight the urgent need to implement targeted interventions addressing unhealthy alcohol use among AYAH, which should be integrated within youth-responsive person-centered care models, such as the SEARCH Youth intervention. Additionally, the considerable underreporting of unhealthy drinking in this population reveals the limitations of relying solely on self-reported screening tools. Moreover, structural interventions and services aimed at early alcohol use could prevent or limit progression to long-term unhealthy drinking habits. Therefore, while person-centered approaches improve adherence to HIV care, they must be complemented by tailored substance use interventions to achieve universal viral suppression among AYAH.
Footnotes
Acknowledgments
We are grateful to the youth who participated in this study along with their healthcare providers and SEARCH Youth staff. We thank the Ministries of Health of Uganda and Kenya and the National Child and Adolescent HIV Prevention and Treatment group in each country for their advice and support throughout this study. We also thank the Prevention and Treatment through a Comprehensive Care Continuum for HIV-affected Adolescents in Resource Constrained Settings (PATC3H) consortium (![]() ), of which this study was a part.
), of which this study was a part.
Ethical Approvals
The Uganda National Council of Science and Technology (UNCST, HS 2542), the Makerere University School of Medicine Research and Ethics Committee (REC REF 2019-014), the Kenya Medical Research Institute (KEMRI, 3834), and the University of California San Francisco (UCSF) Committee on Human Research (18-25703) all approved the SEARCH-Youth study.
Informed Consent
All participants provided written informed consent prior to enrollment into the alcohol use substudy.
Author Contributions
All authors contributed to the concept and design of the manuscript; conceptualization: F.M., S.P., J.P., M.N., H.N., G.O.O., D.B., E.B., L.B.B., J.A., M.R.K., D.H.,C.S.C., T.R., G.C., and J.A.H.; data curation: F.M., S.P., J.P., L.B.B., D.B., J.A.H., and T.R.; formal analysis: F.M., S.P., J.P., L.B.B., J.A.H, G.C.M.R.K.,D.H., and T.R.; funding acquisition: S.P.,T.R., G.C., J.A.H., M.R.K., and D.H.; investigation, F.M., M.N., N.H., G.O.O., D.B., J.A., J.P., and S.P.; methodology: F.M., S.P., J.P., L.B.B., J.A., J.A.H., G.C., M.R.K., D.H., C.S.C., and T.R.; project administration: F.M., S.P., D.B., J.A., J.A.H., M.R.K., D.H., C.S.C., G.C., and T.R.; software: J.P. and L.B.B.; supervision: F.M., S.P J.P., L.B.B., D.B., E.B.,J.A.,J.AH.,M.R.K., D.H., G.C, and T.R.; writing original draft; F.M., and J.A.H; review and editing: F.M., S.P., J.P.,M.N., H.N., G.O.O.,E.B., L.B.B., D.B.,J.A., M.R.K., D.H., C.S.C.,G.C., and T.R. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Common Fund (Grant Nos. R01 UG3 HD96915-01, K23 AA029045 , K24 AA022586, and K24AA031211).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Access Statement
The data that supports this manuscript can be available on reasonable request from Dr Judith A. Hahn at Judy.Hahn@ucsf.edu.