
Abstract
Objective
To understand perceptions of sexuality and care needs from the perspective of women living with human immunodeficiency virus (HIV) and health professionals.
Method
This exploratory qualitative study was conducted in 2 specialized secondary-care services in Brazil. Participants included women living with HIV (WLHIV) aged ≥18 years receiving ongoing follow-up and healthcare professionals involved in their care for at least 6 months. Semistructured interviews were conducted between September and November 2024. Data were analyzed using inductive thematic content analysis, and interpretation was informed by Bronfenbrenner's ecological model to integrate individual, relational, and structural dimensions. The final sample comprised 13 WLHIV and 9 healthcare professionals, with recruitment completed upon theoretical saturation.
Results
two themes were identified. The first indicated that WLHIV frequently experience sexuality as a domain marked by fear, guilt, and anticipated judgment rooted in HIV-related stigma and strained intimate relationships. Concerns related to transmission, rejection, and disclosure limited sexual activity, generated emotional distress, and hindered new partnerships. Some women, however, described processes of reframing sexuality through emotional support, strengthened self-care, and renewed trust in partners. The second theme highlighted insufficient professional preparedness, including limited training, discomfort discussing sexual health, and reliance on biomedical and preventive guidance. Conversations about sexuality were typically patient-initiated and constrained by time pressures, cultural norms, and generational differences.
Final considerations
Findings underscore the need to integrate sexuality into HIV care for WLHIV, addressing the impacts of stigma and gaps in professional training. Advancing sexual health in this population requires public policies and ongoing capacity-building to support comprehensive, humanized, and nonjudgmental care.
Introduction
Human immunodeficiency virus (HIV) infection has become, over recent decades, one of the major global public health challenges, requiring continuous, multisectoral, and human rights oriented responses. 1 Advances in public policies addressing HIV, the expansion of access to early diagnosis, health technologies, and antiretroviral therapy have contributed to the recognition of HIV infection as a chronic condition. However, these advances have not been equitably distributed and the trajectory of the epidemic remains shaped by structural inequalities that disproportionately affect women. 2 In 2024, women and girls accounted for 45% of new HIV worldwide. In Brazil, 46,495 new cases were reported in 2023, with 77.7% of infections among women occurring in those of reproductive age, and a progressive increase among women aged 50 years or older, rising from 12.8% in 2013 to 21.1% in 2023.3,4 These data underscore the need for strategic actions directed toward women, recognizing that responses must address not only clinical management but broader social and relational dimensions.
Human sexuality is understood as a constitutive dimension of development and subjective experience, involving well-being associated with the free and autonomous expression of affection, desire, and intimacy across the life course. It encompasses feelings of pleasure, sensuality, safety, and freedom, and is shaped by social, cultural, and gender-related factors that influence how sexuality is perceived and lived. Thus, sexuality is not limited to biological aspects, but constitutes a relational and symbolic phenomenon that contributes to health and quality of life.5,6
In this context, studies have shown that the sexuality of women living with HIV (WLHIV) involves affective, identity-related, and symbolic dimensions, and is often marked by fear of transmission, reduced sexual desire, difficulties negotiating condom use, concerns regarding disclosure of serostatus, and challenges in forming and sustaining intimate relationships.7,8 Experiences of social and internalized stigma influence self-esteem, perceptions of attractiveness, and experiences of intimacy, directly affecting emotional well-being and the exercise of sexual and reproductive rights.9,10
From the perspective of Bronfenbrenner's ecological model 11 these individual experiences (microsystem level) are embedded in a network of interdependent influences that include interactions with healthcare professionals and services (meso- and exosystem), as well as public policies, cultural norms, and gender inequalities (macrosystem). This perspective allows sexuality and care for WLHIV to be understood as bioecological phenomena, in which subjective and contextual processes are intertwined, and health responses depend on the articulation between personal, relational, and structural dimensions.
The feminization of the HIV epidemic, with the increase in infection among women, is the result of interrelated social, cultural, and economic factors. Gender inequalities, sexual violence, and poor access to education and health care increase women's vulnerability and hinder comprehensive care. The interplay of these factors at the individual, social, and programmatic levels shows that exposure to HIV is not limited to personal choices but stems from structural conditions that limit women's autonomy and the whole exercise of their sexuality and citizenship. 8
In this sense, assistance to WLHIV must consider the particularities of this population to guarantee respect for sexual rights, access to reproductive health, and adequate support for the experience of sexuality. Additionally, providing precise and up-to-date information is crucial for enabling informed decisions, preventing vertical transmission, and promoting prenatal care in national guidelines. 12
The sexuality of WLHIV is therefore a fundamental aspect of comprehensive care, as it involves not only sexual health, but also the right to pleasure and sexual freedom, free from discrimination and violence. 5 After an HIV diagnosis, sexuality becomes more relevant, as seropositivity can bring additional challenges, such as stigma, discrimination, difficulties in establishing emotional relationships, and fear of transmitting the virus. These factors directly affect the experience of sexuality and the quality of life of these women approaching sexuality as a necessity. 13
Despite the growing body of research on HIV and gender, there remains a shortage of studies that integrate the perspectives of women and healthcare professionals regarding sexuality and care, which limits the development of person-centered and comprehensive practices. Historically, women's health approaches have prioritized reproductive and biomedical aspects—such as pregnancy, contraception, and illness—while relegating sexuality to a secondary or instrumental dimension. 13 This reproductive emphasis contributes to the invisibility of affective–sexual experiences and the sexual rights of women, particularly those living with HIV, whose narratives about pleasure, desire, and intimacy are often silenced in healthcare settings. Considering sexuality as a central component of women's health broadens the understanding of living with HIV and reinforces the need for policies and practices that transcend the biomedical focus.
Comprehensive care for WLHIV requires recognizing sexuality as a constitutive dimension of health and ensuring access to information, autonomy, supportive care, and services free from stigma.5,14 Given this context, it is essential to investigate the care demands related to the sexuality among WLHIV. Therefore, the following research questions were formulated: How do WLHIV and health professionals perceive sexuality after diagnosis? What are the care demands related to sexuality from the perspective of WLHIV and health professionals? The objective of this study was to understand perceptions of sexuality and care demands from the perspective of WLHIV and health professionals.
Method
Design, Study Setting and Population
Exploratory study with a qualitative approach. The Brazilian Unified Health System (SUS) in Brazil offers free and universal public healthcare, organized into levels of care based on the principles of comprehensiveness, equity, and regionalization. 15 Primary care, operated by the Family Health Strategy, serves as the primary gateway to the system, with actions aimed at promoting health, preventing disease, diagnosing, treating, rehabilitating, and reducing harm. 16 Secondary care encompasses specialized services essential for the clinical management of chronic conditions. In care for PLHIV, these services include diagnosis, antiretroviral treatment, psychological support, and prevention of complications. 17 They are part of the SUS specialized care network and play a central role in longitudinal follow-up and coordination of continuous care.
The study was conducted in 2 specialized secondary care services; 1 located in the outpatient department of a public university hospital and the other linked to a municipal referral unit.
Study Participants and Selection Criteria
WLHIV aged 18 years or older who were receiving follow-up care at specialized reference services were included in the study, as well as healthcare professionals who had been providing care to these women for at least 6 months. Women who were incarcerated or presented neurocognitive impairments that could hinder their participation in the study were not included. Likewise, healthcare professionals who were on medical leave, maternity leave, participating in external training activities, or on vacation during the data collection period were excluded.
The final sample comprised 13 WLHIV and 9 healthcare professionals. In the MVHIV group, 20 were invited to participate in the study, of whom 4 declined and 3 withdrew before the start of data collection. The number of participants was determined based on the criterion of theoretical saturation, which is appropriate for exploratory qualitative studies aimed at understanding meanings and lived experiences. This sample size is consistent with similar research conducted in specialized HIV care settings, in which narrative depth and analytical density are prioritized over numerical breadth. Saturation was assessed continuously and when, after the 11th interview with WLHIV and the 7th interview with professionals, the research team came to the judgment that new insights were significantly diminishing. Two additional interviews were conducted in each group after this point which further reinforced this view.
Data Collection
Data were collected between September and November 2024 by a sole researcher with no employment or personal ties to the participants. Initially, visits were made to the services in order to present the study's objectives, invite professional to participate, and request their support in disseminating the research to WLHIV during routine care. Approaches to WLHIV varied by service: in service A, women were invited during routine consultations or walk-in appointments; in service B, recruitment occurred among women attending weekly CD4+ testing. In both settings, healthcare professionals introduced the study, and—if interest was expressed—women were referred to a private room for a detailed explanation and a formal invitation to participate. After receiving information about the study and providing consent, participants could choose to complete the interview immediately or schedule it for a data and location of their preference. However, only 3 participants (WLHIV) opted to be interviewed in their homes. In both places, data collection proceeded smoothly and without interruption. There was no presence of third parties during the interviews.
A semistructured interview guide was developed based on the study objectives. For WLHIV, we used: “Describe what it is like to experience your sexuality after receiving an HIV diagnosis,” “How did you feel about expressing your sexuality after the diagnosis?” and “Describe the health-care guidance you received at the time of your diagnosis.” For healthcare professionals, the interview explored their perceptions, clinical practices, and professional preparedness. The questions included: “How do you perceive and address sexuality in the care of WLHIV?,” “How do you define sexual health care and sexuality?,” and “Do you feel prepared to address sexuality in this context? If not, what would be required to strengthen your preparedness?” To ensure clarity and appropriateness, the questions were discussed within the research group and subjected to pilot testing. Interviews were audio-recorded using a smartphone and the “Voice Recorder” application, and lasted an average of 30 min. No repeat interviews were conducted with the participants.
Research Team and Reflexivity
The reporting of this study followed the Consolidated Criteria for Reporting Qualitative Research guidelines, 18 as outlined in the checklist presented in Supplemental Material S1.
The lead researcher was a master's student in nursing with experience in public health, responsible for conducting all in-depth interviews. Her lack of prior relationship with participants may have made them less inclined to share their perceptions and experiences concerning sexuality. To mitigate this, active recruitment of potential participants was carried out within the services themselves, with the support of healthcare professionals who assisted in disseminating the study invitation. Once participants agreed to take part, the lead researcher began the interviews by building rapport to ensure they felt comfortable and confident during the conversations.
Moreover, the fact that the lead researcher was a woman may have facilitated the creation of a trustworthy atmosphere, particularly when addressing intimate issues related to female sexuality. To minimize interpretive bias, reflective memos were used, in which the researcher documented her perceptions, expectations, and potential subjective influences throughout data collection and analysis.
To ensure credibility and dependability, the study supervisor—an experienced nurse researcher with extensive expertise in the qualitative method employed—also analyzed the material independently. The 2 then discussed any discrepancies until consensus was reached. Preliminary results were discussed among members of the research group, helping to reduce risks to descriptive and interpretive validity. 19 In addition, the final categories were once again compared with raw excerpts from the interviews which gave the research team further confidence that the outcome of the analysis had remained grounded in the evidence gathered. These strategies strengthened methodological rigor, reduced individual bias, and ensured consistency in the interpretation of the findings.
Data Analysis
The interviews were fully transcribed and submitted to inductive thematic content analysis (Bardin, 2016). After repeated, immersive reading, 68 meaning units were identified; aggregation by similarity resulted in 10 meaning clusters, which followed by analysis guided by the study objectives, yielded 2 thematic categories. Figure 1 summarizes our activity in response to the stages of analysis as described by Bardin. 20
Codes, meaning units and thematic categories.
Data interpretation was guided by Bronfenbrenner's ecological model of human development, 11 adopted as a theoretical framework to integrate individual, relational, and structural dimensions of the participants’ experiences. This framework allowed the analysis to connect micro-level processes (personal experiences and immediate interactions) with macro-level influences (health policies, cultural norms, and institutional contexts).
Ethical Approval and Informed Consent
The study was approved by the Research Ethics Committee of the Federal University of Mato Grosso do Sul and the Health service (Opinion n° 7.063.583). Aware of the objectives, benefits, and risks of the research, all participants signed the Free and Informed Consent Form in duplicate. The study was conducted in accordance with all ethical principles outlined in Resolution 466/12 of the National Health Council. To preserve the anonymity of the participants, they were identified by the letter "W" (Woman) and a unique number, followed by their age (eg, W2, 55 years old). The letters HP (Health Professional) and an identifying number, followed by their age and professional category (eg, HP2, 40 years, Nurse).
Results
The study involved 22 participants: 13 WLHIV and 9 healthcare professionals. The WLHIV were aged between 27 and 73 years (mean age approximately 47 years), with time since diagnosis ranged from 8 months to 19 years. Table 1 presents the characteristics of WLHIV.
WLHIV Characterization. Campo Grande, MS, 2024.

Source: Elaborated by the author (2025).
Abbreviation: WLHIV: women living with human immunodeficiency virus.
Among the healthcare professionals, 8 were women, aged between 35 and 71 years, with most reporting more than 10 years of professional experience. Table 2 shows the characteristics of professionals.
Characterization of Health Professionals. Campo Grande, MS, 2024.
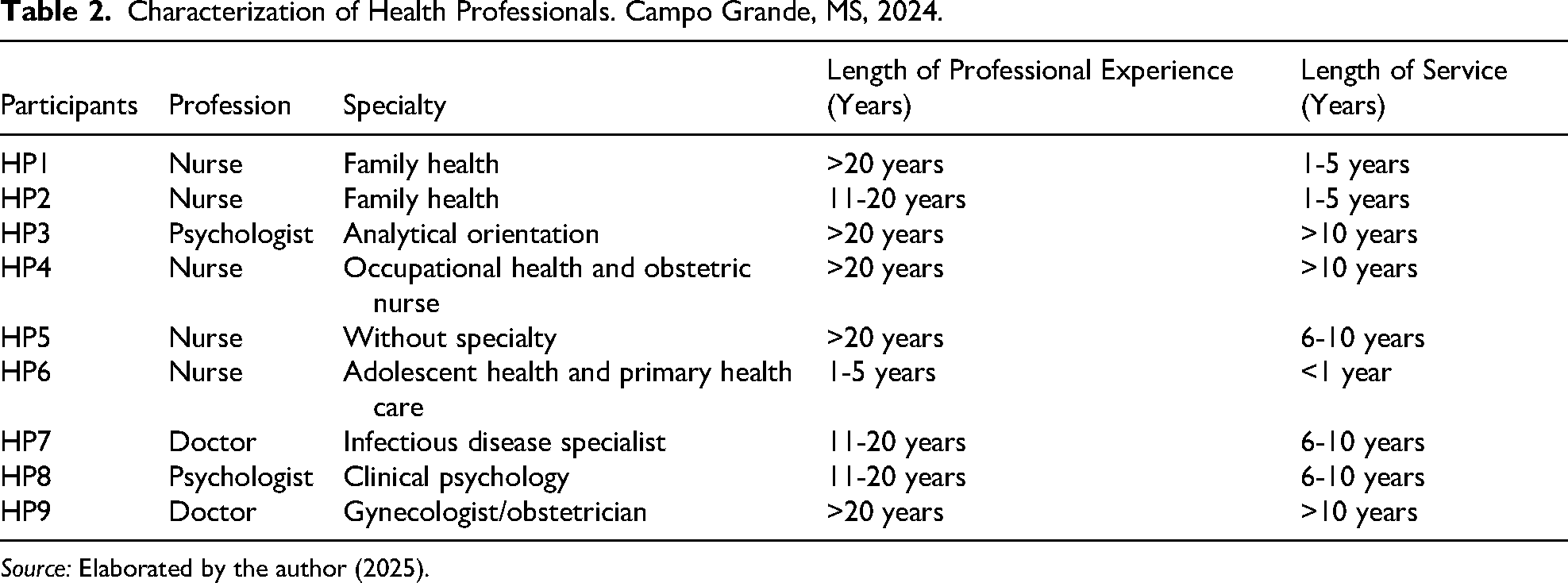
Source: Elaborated by the author (2025).
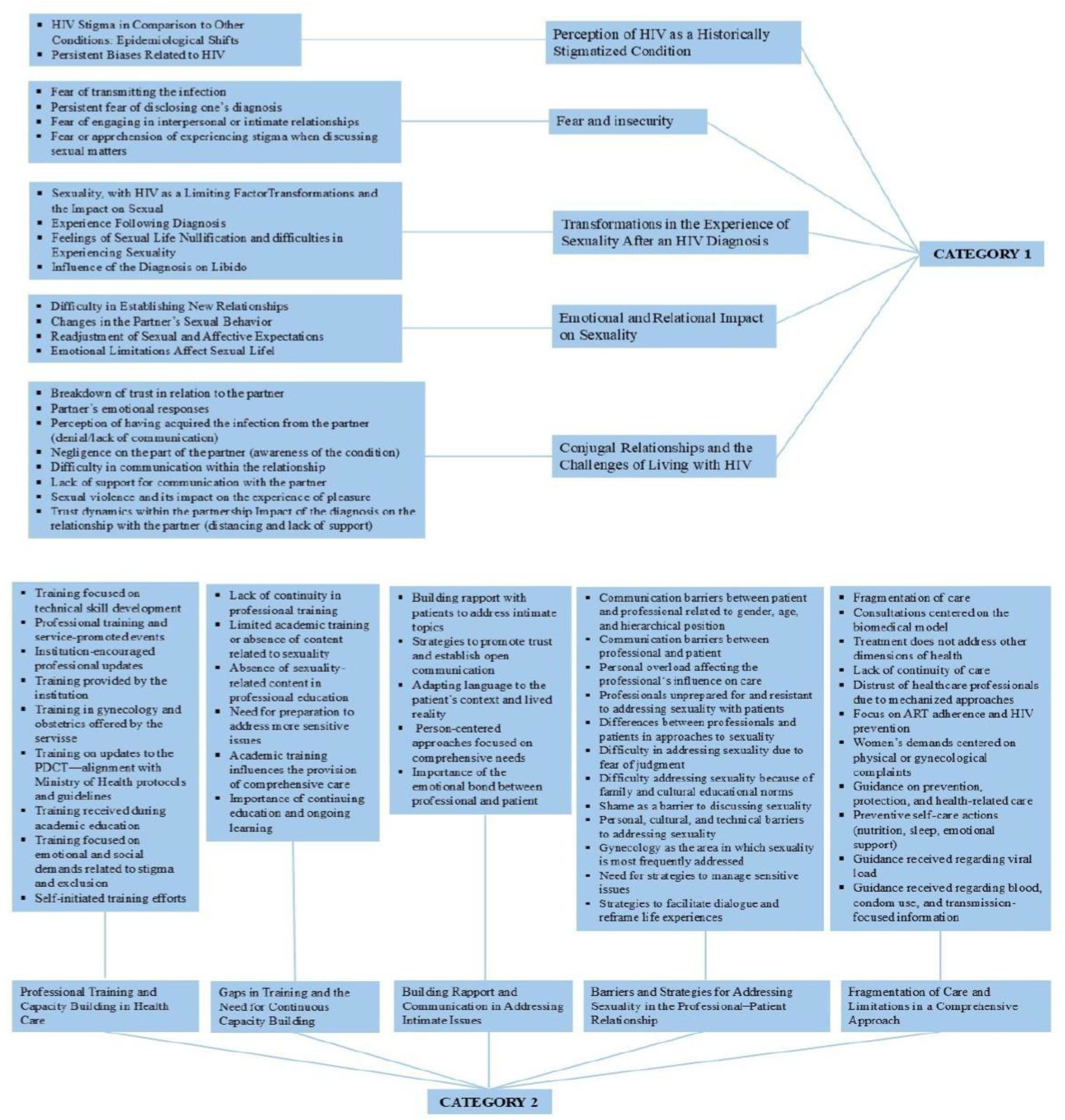
The qualitative analysis of the data resulted in the identification of 2 categories. Figure 2, represents the conceptual diagram of the interrelationship among thematic categories.

Conceptual diagram of the interrelationship among thematic categories.
Sexuality and HIV: Between Stigmas, Impacts and Resignifications
This category explains sexuality as a care need in which the quality of the professional–patient relationship can be a decisive factor in the provision of care. It then highlights and shows the challenges and complexities faced by WLHIV and reveals how stigma and emotional challenges impact the experience of sexuality. In this context, support, nonjudgmental acceptance, and the assurance of confidentiality may influence women's willingness to return to the service and ensure that their needs are met. Amid fears, guilt, and prejudice, stories of overcoming adversity and reframing experiences also emerge, demonstrating the strength to rebuild relationships and rediscover pleasure. Participants reported that the sexual transmission of HIV exacerbates stigma and prejudice regarding the disease: … the stigma attached to this one (AIDS) is because it's linked to sex, which is seen as shameful, dirty, ugly … I think if I came home with a cancer diagnosis, I would be better received; everyone would try to find a way to make my life more comfortable… (W05, 43 years old) Who isn't weakened by any ICD [International Classification of Diseases] they get? So, imagine a disease that is sexually transmitted […]. (HP07, 42, Doctor)
Prejudice and stigma surrounding the disease also constitute barriers to communication about sexuality, with women sometimes avoiding talking about the subject so as not to be judged and even seeking to avoid relationships with other people after infection with the virus, mainly due to fear of transmission: Because people will start noticing, oh, she has HIV, she wants to have sex … I wonder if everyone with HIV thinks like me, but I don't talk to anyone. (W02, 43 years old) We had sex once or twice; a few days passed, and then he came down with the flu. You have no idea how I felt. He got it. And he said, “There's no way, But in our heads, we torment ourselves; we torture ourselves.” (W07, 51 years old) It makes it harder to get involved. Fear of passing on the virus, fear of being discovered, fear of your partner's prejudice, of saying something…. (HP08, 42, Psychologist)
Similarly, women with steady partners also pointed out the impact of the disease on their sexual experience: […] we kind of drifted apart, you know? We continued to have sex, but it was lukewarm, boring. I think that at that point I lost my desire…. (W07, 51 years old) When it happens, it happens (sex). But it's not what I want it to be. And I don't say anything because he gets outraged. (W02, 43 years old)
Especially in cases where transmission by the partner occurred in an extramarital relationship: At first, we used [condoms], but then I trusted him; he didn't tell me he had a problem, and he stopped using them, and that's when I got it. He already knew and didn't tell me … he knew he had it, but he didn't get treatment. (W10, 54 years old) …she is vulnerable, and often these are women who have had a serious relationship with a partner, had children, and were betrayed. So, there is not only the problem of contracting a disease, but also the betrayal…. (HP07, 42, Doctor)
Some participants highlighted the interruption of their sex lives after infection: …there are some who don't have sex anymore. Especially those who were married and whose husbands had sex with other women and brought HIV into the home. (HP03, 71, Psychologist) …I think I liked sex … I was traumatized because, besides doing that [getting HIV], he used to beat me a lot, you know? I don't want anything to do with it anymore. (W01, 45 years old)
However, some women experience ambivalence between the desire to have a relationship and the emotional and social barriers they face. […] I have [sexual desire], but at the same time, I am afraid. I try to let myself go, you know? Relax, and then it comes into my head, oh no, I have [HIV]. (W13, 53 years old)
And sometimes they seek ways to reframe their experiences, whether through self-care or by seeking emotional support, to overcome challenges: …in my mind, I said to myself: I'm not going to find anyone else, […] now that I've met someone and he said: it's you and me, whatever happens to me or you, we must talk to each other. Then I felt safe to speak…. (W09, 27 years old) I spent 10 years of my life just taking care of myself and my children. Because in my mind, if I were to date someone, I didn't want to deceive them, I had to tell them about the situation [HIV]. Nowadays it's wonderful …. Because it took so long to find the right person that I thought they didn't even exist, but they do…. (W11, 46 years old) …at first, when we were dating, I didn't enjoy it, I couldn't. I couldn't reach [orgasm] because I blocked it. So, it seems like I was afraid. Today, no. (W12, 33 years old)
Experience shows that, for many women, sexuality has become an experience marked by fear, guilt, and doubt. Still, it also highlights elements that contribute to reframing, mainly through emotional support and strengthening self-care.
Challenges and Prospects for Care: A Look at Sexuality Among WLHIV
This category addresses gaps and challenges in the education and training of health professionals to provide comprehensive care for the sexuality of WLHIV. The inadequacy of technical and emotional preparation during undergraduate education, the lack of systematic approaches to sexuality, and the need for continuing education to deal with sensitive and complex issues were highlighted factors.
The training and capacity building offered to professionals focus on the clinical management of HIV cases: I have taken several courses on, for example, reception, rapid testing of Clinical Protocol of Therapeutic Guidelines (PCDT- in Portuguese) training, which is the clinical protocol. So, we must complete a certain number of training hours per year and provide proof of this. (HP04, 54, Nurse)
Thus, the guidelines provided to WLHIVs refer to preventive issues and treatment adherence: I asked about the woman's health itself. (…) whether she is taking proper precautions during sexual intercourse because she could contract other STIs, and whether I see that she is emotionally distressed. (…). (HP01, 46, Nurse) We advise them, even though it is not transmissible, to always use protection, condoms for STIs, not just for HIV. (HP02, 40, Nurse) She said this … Whenever you go out with someone, use a condom. Because you will protect your partner, and you will protect yourself because you run the risk of getting other infections. (W11, 46 years old) …they said, You don't need to worry about food; these things don't pass, but if you're going to have sex with your partner, you find a partner; you have to sit down and explain it to him if you want to come here to talk to us…. (W09, 27 years old)
Or even more broadly focused on aspects of self-care and sexual experience: From telling them about care, the importance of skin. Informing them that undetectable patients cannot transmit the virus. That they can have a sexual experience. Assessing issues of self-image. Because of depression and anxiety as well. (HP06, 35, Nurse) Women's rules, prevention, physical activity, diet, water intake, support network, work, and leisure, which they must agree on. Whenever the person is open to it, I advise them to seek therapy and refer them to a psychologist. I think that's it. Attend appointments and take your medication. I always explain to them what HIV is and what it means for their lives. (HP07, 42, Doctor)
Sexuality is sometimes not recognized as a dimension of care: […] I didn't think at any point about sexuality. I thought, like, oh, is this a problem for her? You know? I didn't relate HIV to being a problem. (HP05, 43, Nurse) Most women speak up when they have a need. So, if you’re feeling something—pain, pain, something—you notice something different, women speak up. (HP06, 35, Nurse) I believe that no one mentions it. Only if it's a gynecologist. I think that's the only one, or a psychologist. Especially if that woman has trauma related to sexuality. (HP01, 46, Nurse)
When asked about their preparation for providing sexual health care to PLHIV, professionals pointed to gaps in the training process. They highlighted the difficulty of addressing sexual health comprehensively due to a lack of technical and emotional preparation: It wasn't discussed. I'm not sure if it's because I graduated many years ago. Still, I don't remember having just the basics, contraceptive methods, STIs, but getting into the issue of sexuality itself … No, no. (HP01, 46, Nurse) I've been in the medical field for about 15 years now. We are not taught to talk about it. These are neglected. (HP07, 42, Doctor) …I don't know if I feel prepared to ask the right questions. (HP05, 43, Nurse) I'm not prepared, not at all. Often, even the healthcare professional who is treating the patient doesn't have enough experience or knowledge of the subject to be able to pass it on to someone else or address it. (HP07, 42, Doctor) I think there is a certain protection on my part, a shyness, and a lack of preparation. (HP01, 46, Nurse)
WLHIV highlights the lack of discussion on the subject as a gap in care: Practically all my consultations, there was never any point in talking about anything other than viral load and medication … I lost trust in the health professionals, you know. Occasionally, I know more than he because I know myself, and he treats his patients as if they were all robots with the same form. (W05, 43 years old) There was no more guidance, because they see that we are already a couple there. You know? So, they don't talk. (W03, 41 years old)
This perception of unpreparedness sometimes culminates in not addressing the issue of routine care: …when we're not prepared, we avoid bringing up the subject, because you don't know how to handle it. (HP04, 54, Nurse)
When approached, it is mediated by bonds established between the professional and the patient. Because I think you need to have a bond for them to tell the truth. As they have more freedom, patients open. (HP09, 49, Doctor) Since I know I'll have other opportunities every 15 days, I don't feel anxious about approaching them right away. I let things flow naturally. (HP04, 54, Nurse)
However, bonding is often hindered by a lack of time and excessive focus on biomedical aspects of care, as identified in the following statements: And when there is no bond, we cannot address these issues. There is no time, and it becomes more difficult. (HP06, 35, Nurse) But I don't have that intimacy, sometimes I don't feel comfortable talking about sexuality because I see that they are not looking for that information. So, I end up not bringing up the subject. (HP05, 43, Nurse) Health, medication in that sense … Oh, have you had any illnesses? That's the question I ask almost every time. Have you lost weight quickly? … the rest of their health is not their problem. (W05, 43 years old)
They also emphasize that the approach must be sensitive and respectful of boundaries to prioritize effective communication. … improving my communication technique, welcoming that individual, sensing how receptive they are to talking that day, and if I see that it's not going to happen that day, I’ll try again the next day. So, I just see how it goes. When I see that the person is receptive, I start talking. If I see that they’re not, I try to ask more lightly. (HP07, 42, Doctor)
Other elements identified as barriers to talking about sexual health were cultural taboos and shame: I think it's also the taboo, the shame, the culture of professionals. Because I think the professional will be a little uncomfortable bringing up the subject. (HP01, 46, Nurse) They are ashamed, there is also a bit of denial, they are afraid of being judged, there are also many patients who are afraid to talk about their sexual orientation for fear of being judged. (HP09, 49, Doctor)
In addition, the preconception that older women are afraid to discuss sexuality due to cultural and generational contexts was mentioned: A woman of 50, 60 years old, she came from a world where women did not study, where women did not work, where women could not enjoy themselves, let alone talk about sex, they couldn't, where women had to be submissive, accept everything that men wanted. Men called the shots. So, it's tough for them to talk. (HP07, 42, Doctor) …let's suppose that if it were a young woman, for you to talk to, maybe for her, it would be something more … How can I say … Natural. Now a 60-year-old person can talk about it (sexuality). (HP01, 46, Nurse)
Participants emphasized that when it does occur, it is at the woman's request: We see the patient. It's what she wants to talk about. If she doesn't bring up sexual issues, I don't ask either. (…) As she brings things up, we talk about them, including sexual health. (HP03, 71, Psychologist) It's usually more physical care than … And they don't pay much attention to their bodies, or their pleasure. They even avoid touching on the subject. (HP08, 42, Psychologist)
The cultural, social, and training challenges in addressing the sexual health of WLHIV as a care demand are compounded by structural and organizational limitations in the work process itself.
Discussion
The care needs related to promoting sexuality among WLHIV encompass challenges shaped by HIV-related stigma, difficulties in experiencing sexuality, and persistent gaps in how health professionals address this issue. Bronfenbrenner's ecological model 11 provides a useful lens to understand how these challenges emerge across multiple levels of influence.
Participants’ narratives highlighted the interplay between moral prejudice at the macrosystem level, emotional barriers within interpersonal contexts at the microsystem level, and healthcare practices, still centered on biomedical model outcomes at the exosystem and chronosystem levels. Together, these factors negatively affect WLHIV's ability to experience sexuality safely and fully, underscoring the difficulty of integrating comprehensive care within HIV services.
Evidence of good practice exist for the integration of HIV care with sexual and reproductive health services, demonstrating improvements in patient satisfaction, access to counseling, and overall quality of care—particularly in systems with strong primary care foundations.21,22 Such evidence can inform service redesign through standardized protocols for sexual-health assessment, interdisciplinary consultations, internal referral pathways, and educational strategies grounded in sexual and reproductive rights.23,24
Approaching sexual health as a core component of comprehensive care requires recognizing its complexity and ensuring that services address individual needs in a safe, satisfying, and nondiscriminatory manner. 5
Yet HIV remains distinct from other chronic conditions because it carries moral, historical, and cultural burdens that shape experiences of stigma. Sexual transmission is particularly stigmatized, reinforcing moral narratives about “deviant” behavior and restricting both disclosure and full participation in sexual life. 25 Participants emphasized that HIV exposes them to social and moral vulnerabilities not encountered in other chronic illnesses, contributing to concealment of diagnosis and negatively affecting mental health, treatment adherence, and opportunities for health promotion. 26 Recognizing the role of stigma is therefore essential for planning care and creating inclusive environments that transform experiences of exclusion into opportunities for autonomy.
In the present study, participants highlight the fact that living with HIV is a condition that exposes them to social and moral vulnerabilities when compared to other chronic diseases, such as hypertension or diabetes, which are treated more naturally. This differentiation reinforces the emotional weight of an HIV diagnosis, which is often hidden to avoid judgment and discrimination, affecting not only mental health but also adherence to treatment, social relationships, and opportunities for health promotion. 25 Given this, health services must consider the impact of stigma in care planning and create a welcoming and sensitive environment to transform these experiences marked by exclusion into experiences of care, autonomy, and dignity.
Stigma also constrains communication about sexuality. Silence surround diagnosis, fear of rejection, and limitations in intimate relationships reflect not only individual responses but also health-system practices that prioritize biomedical outcomes over subjective and relational dimensions of care. These dynamics are reinforced by gender norms, moral discourses, and institutional cultures that restrict discussion of pleasure, intimacy, and sexual rights.27,28
Difficulties were especially evident among women whose infection occurred in contexts of infidelity or breached trust, contributing to internalized stigma, shame, and withdrawal, sometimes resulting in cessation of sexual activity. 29 Macrosystem gender inequities further constrain autonomy, sexual desire, and negotiation within partnerships. 9 Similar patterns have been documented in Sub-Saharan Africa and Southeast Asia, indicating that global health systems face common challenges in integrating sexuality into HIV care.21,22
Despite these barriers, some participants described opportunities to reframe sexual experiences over time when supported by emotional counseling, accurate information, multiprofessional follow-up, and peer networks. Rights-based sexual education, discussions of pleasure, and guidance on preexposure prophylaxis, condom use, and self-care were identified as facilitators for rebuilding confidence and resuming sexual life safely. 30
Strengthening provider capacity is essential for implementing this type of support. Training that focuses largely on sexually transmitted infections and contraception does not equip professionals to address the emotional and cultural dimensions of sexuality. 31 These gaps reflect institutional structures—including limited consultation time, heavy workloads, absence of protocols, and persistent gender taboos—rather than individual provider shortcomings.32–34 Clinical hierarchies also restrict dialogue, as sexuality is often framed as a risk rather than a right.
The findings of this study have direct implications for nonjudgmental and humanized nursing practice. Providers must acknowledge sexuality as a legitimate component of care and integrate it systematically into consultations. This includes the use of inclusive language, structured open-ended questions about sexuality, confidentiality measures, interdisciplinary training, and peer-support groups. Within Brazil's Unified Health System, primary care teams can incorporate sexual-health counseling into HIV care through standardized protocols, telehealth services, referral pathways, and community education initiatives.
Overall, the findings underscore the need for multilevel strategies that incorporate sexuality as an inseparable part of comprehensive HIV care. Addressing these challenges requires coordinated actions at clinical, institutional, community, and policy levels, with sustained commitment to promoting dignity, autonomy, and quality of life for WLHIV.
Limitations
This study has several limitations that should be considered when interpreting the findings. Data were collected in 2 specialized services located in the Central-West region of Brazil, a context characterized by specific sociocultural, demographic, and organizational features. Although the results contribute to understanding the sexual experiences of WLHIV, their transferability to other regional contexts should be interpreted with caution, particularly in settings with different care structures and cultural dynamics.
The possibility of self-selection bias must also be acknowledged. Women who felt more comfortable discussing aspects of their sexuality—or who had already begun processes of reframing their experiences—may have been more likely to participate. As a result, experiences marked by greater withdrawal or silence may be underrepresented. Additionally, the presence of a female researcher may have facilitated the disclosure of intimate experiences, yet it may also have shaped how certain narratives were constructed and shared—an issue considered in the reflexive component of the analysis.
This study did not include participant transcript review or feedback on findings, which may limit opportunities for participant validation; however, analytic rigor was supported through double coding and peer debriefing.
Despite these limitations, the findings provide valuable insights for the development of public policies and clinical practices that position sexuality as a fundamental component of comprehensive HIV care, in alignment with the multilevel perspective proposed by the ecological model.
Final Considerations
For WLHIV, the experience of sexuality continues to be shaped by fear, insecurity, and apprehension about judgment—elements deeply intertwined with historically constructed stigma and taboos. These factors directly affect the microsystem, influencing self-esteem, affective relationships, partnership dynamics, and interactions with healthcare professionals. At the mesosystem level, these experiences intersect with other significant environments—family, health services, and social support networks—often reinforcing silence and limiting access to comprehensive care.
From the perspective of healthcare professionals, sexuality remains insufficiently addressed in clinical practice, revealing gaps in training and challenges in approaching the topic. This invisibility reflects exosystem influences, such as inadequate professional curricula, lack of specific protocols, and institutional constraints. At the macrosystem level, sociocultural values that sustain moral judgments, prejudice, and gender inequalities create a context in which the sexuality of WLHIV is frequently stigmatized or treated as secondary.
The findings of this study reaffirm sexuality as a central care priority for WLHIV and highlight the need for approaches that simultaneously address women's subjective experiences and the challenges encountered by providers. Structural changes in healthcare settings are essential, including the implementation of public policies that integrate sexual health across services and investment in continuous team training to ensure humanized, nonjudgmental, and gender-sensitive care.
By strengthening welcoming environments and promoting practices that acknowledge the multiple layers shaping sexual experience—from intimate relationships to cultural and institutional determinants—it becomes possible to challenge stigma, enhance women's autonomy, and contribute to improved health and well-being.
Future research should include the partners of WLHIV to deepen understanding of affective–sexual negotiations and shared care dynamics. Including managers and service coordinators is also recommended to examine how organizational structures support or hinder the integration of sexuality into HIV care.
Supplemental Material
sj-pdf-1-jia-10.1177_23259582261426238 - Supplemental material for The Sexuality of Women Living With HIV: Care Demands and Implications for Practice
Supplemental material, sj-pdf-1-jia-10.1177_23259582261426238 for The Sexuality of Women Living With HIV: Care Demands and Implications for Practice by Tailma Silva Lino de Souza, Ana Paula de Assis Sales, Thaís Gianini Dias, Elis Regina Souza and Luciana de Alcântara Nogueira, Maria Neto da Cruz Leitão, Gareth Wiltshire, Elen Ferraz Teston in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582261426238 - Supplemental material for The Sexuality of Women Living With HIV: Care Demands and Implications for Practice
Supplemental material, sj-docx-2-jia-10.1177_23259582261426238 for The Sexuality of Women Living With HIV: Care Demands and Implications for Practice by Tailma Silva Lino de Souza, Ana Paula de Assis Sales, Thaís Gianini Dias, Elis Regina Souza and Luciana de Alcântara Nogueira, Maria Neto da Cruz Leitão, Gareth Wiltshire, Elen Ferraz Teston in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
ORCID iDs
Author Contributions
Tailma Silva Lino de Souza: Study conception, data collection, data analysis and interpretation, discussion of the results, writing and/or critical revision of the content, review and final approval of the final version. Ana Paula de Assis Sales: Study conception, discussion of the results, writing and/or critical revision of the content, review and final approval of the final version. Thaís Gianini Dias: Writing and/or critical revision of the content, review and final approval of the final version. Elis Regina Souza: Writing and/or critical revision of the content, review and final approval of the final version. Luciana de Alcântara Nogueira: Writing and/or critical revision of the content, review and final approval of the final version. Maria Neto da Cruz Leitão: Writing and/or critical revision of the content, review and final approval of the final version. Gareth Wiltshire: Writing and/or critical revision of the content, review and final approval of the final version. Elen Ferraz Teston: Study conception, data collection, data analysis and interpretation, discussion of the results, writing and/or critical revision of the content, review and final approval of the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Grant No. 001).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.