
Abstract
Objective
This mixed-method cross-sectional study identified different barriers faced by key population in accessing HIV services hindering epidemic control on National Aligned HIV/AIDS Initiative (NAHI) in Nigeria.
Methodology
Data were collected from 1932 participants (≥18 years) in 12 NAHI states using structured surveys and analyzed with SPSS. Focus Group Discussion and Key Informant Interview were conducted among 312 KPs and 12 health workers respectively and thematically analyzed using NVivo.
Results
From 1932 respondents, 40% were Female Sex Workers (FSW), 37% Men who have Sex with Men (MSM) and 24% People who inject drugs (PWID). About 82% self-reported receiving HIV testing, 67% accessed prevention services and 63% currently receiving ART treatment among participants. Major barriers faced by KP included distance to facilities (57%), financial constraints (30%) and stigma (24%). Socioeconomic status significantly predicted risky behaviors (R = 0.201, p < 0.001). Qualitative findings highlighted abuse and violence, attitude of health workers, mental health, homelessness and drug stock-outs, as barriers.
Conclusion
Structural, biomedical, and behavioral barriers hinder HIV epidemic control among KPs in Nigeria. Multilevel interventions addressing commodity supply, socioeconomic support, abuse and stigma reduction are critical to improve HIV outcomes in Nigeria.
Introduction
Key populations (KP), including transgender people, female sex workers, men who have sex with men, people who inject drugs and prison inmates, are more vulnerable and contribute to new HIV infections than the general population (GP). HIV prevalence among MSM is 11 times higher than that of GP, four times higher among FSW, seven times higher among PWID and 14 times higher among TG compared with adults in GP between 15 and 49 years in 2022. These populations and their sexual partners account for 70% new HIV infection despite being <5% of the global population. 1 A global estimate in 2022 showed that men who have sex with men (MSM) have 28 times the risk of HIV infection relative to heterosexual (HET) adult men, female sex workers (FSW) have 30 times the risk relative to other adult women, and people who inject drugs (PWID) have 35 times the risk compared to those who do not inject drugs. 2
In Nigeria, the current Key population size (KPSE) was estimated at 600,000 for MSM; 740,000 for FSW; 441,500 for PWID, and for Transgender, about 94,000. 3 Despite making up a small proportion of the overall Nigerian population, they account for 74,000 new infections and face discrimination, stigma and criminalization. 4 Young people from key populations are highly vulnerable and struggle in terms of safety and health in contexts marked by stigma, discrimination and harassment, punitive laws and social taboos. 5
Globally, a remarkable effort has been made toward ending AIDS, yet work on the HIV burdens and barriers to services for key populations is limited in several settings, despite improvements in data sources and studies on KP in a particular context. 6
In South Africa and Zambia, KP face behavioral and structural challenges in receiving HIV prevention and treatment services, along with other relevant primary care routine services, due to stigma and discrimination, violence, service rejection and verbal and physical abuse from health providers. 7 Additionally, discrimination towards people living with HIV remain alarming in all regions, and stigma is hindering people from seeking HIV prevention services, testing for HIV and retention on HIV treatment in low and middle income countries. 8
Recent implementation of anti-LGBT laws, such as the Same-Sex Marriage Prohibition Act, demonstrates that these obstacles worsen difficulties for MSM and transgender groups in getting HIV services. Some countries have restricted the scope of or removed laws criminalizing HIV transmission, exposure or non-disclosure and drug use. Furthermore, unfavourable contacts between police and important populations, particularly MSM, transgender, sex worker and PWID communities, are a result of the stigmatization and criminalization of substance use, sex work and same-sex activities. 9
Consequently, in Nigeria, studies have shown that KPs face significant barriers to HIV prevention and treatment services, including stigma, discrimination and criminalization.10,11 For example, a study conducted in Lagos found that female sex workers faced significant barriers to HIV testing and treatment due to stigma and discrimination. 12 Another study conducted in Abuja found that men who have sex with men faced significant barriers to HIV prevention services due to criminalization and stigma. 13
Achieving HIV epidemic control means that the total number of new HIV infections falls below the total number of deaths from all causes among HIV-infected individuals 14 ; hence, all barriers hindering this achievement will need to be tackled for Nigeria to achieve epidemic control of HIV. These populations are particularly vulnerable to HIV acquisition, with high prevalence and incidence rates across Africa.Understanding these barriers is crucial given the high prevalence and incidence rates among KPs in the world. 15 The integration of HIV intervention programs with other life-saving services to promote health-seeking and reduce risky behaviours will increase access to prevention and treatment services for key populations. Minimum Prevention Packages Interventions (MPPI) such as HIV testing, harm reduction, condom and lubricant programming, gender affirmation, STI management, sexual and reproductive health services, sexual and gender-based violence prevention, mental health and psychosocial support services, must therefore be tailored and expanded. 16 This study aims to identify barriers to HIV prevention, care and treatment services hindering epidemic control among the Key Population on the National Aligned HIV/AIDS Initiatives grant in Nigeria.
Rationale for Using the NAHI Grant Context for the Study
The National Aligned HIV/AIDS Initiatives (NAHI) is a joint alignment of all HIV programming stakeholders in Nigeria. The NAHI grant cycle six HIV program was initiated in 2021 to reduce HIV burden among Key populations in Nigeria. The prime recipient, oversaw the project's technical and programmatic direction in all the states with sub-recipients, monitoring program implementation and implementing partners in respective states. The NAHI project adopted a differentiated service delivery and fixed model strategies through a One Stop Shop (OSS) and community model of care to expand access to HIV prevention, treatment, care and support targeting key and vulnerable populations. The One Stop Shop was overseen by the respective sub-recipients with qualified health care workers and a data officer, while the community model was handled by the implementing partners from different KP community-based organizations.
This study, as part of the NAHI program implementation to evaluate the performance of the developed and tested differentiated model adopted in reducing HIV burden, access to comprehensive HIV services and barriers to these services among the key population in Nigeria. This is suitable for implementation science study because it aims to solve the implementation problems of the proven interventions (differentiated model of care) hindering HIV epidemic control among KP.
Methodology
Study Settings and Participant Recruitment
This study conducted in 12 states of Nigeria, accounting for one-third of the overall states in Nigeria across the South-West, South-East and Northern Nigeria. The NAHI was implemented in 13 states of Nigeria with the exemption of Taraba state in the study due to logistics issues. These states include Abia, Anambra, Ebonyi, Edo, Enugu, Gombe, Imo, Kaduna, Kano, Kwara, Oyo and Plateau. Participants were recruited from members of key population typologies: Female Sex Workers (FSW), Men who have Sex with Men (MSM) and People Who Use/ Inject Drugs (PWUD/PWID), except Persons in Correction Centre (PICC) due to ethical reasons. The recruitment of participants was at different KP hotspots in the states, which include One Stop Shop, brothels, Community Based Organization secretariat, MSM hangout spots and bunks for comfort and privacy in a confidential manner. Transgender people belong to the MSM community, and in this study, there would be no distinction between MSM and TG as they form a single community and are identified only as males during the study.
Study Design and Population
A cross-sectional design using stratified sampling for the quantitative method and purposive sampling for the qualitative method was used to recruit participants. The stratified sampling method was adopted for equal participation of FSW, MSM and PWID typologies across different age groups, gender and socioeconomic factors who are 18 years and above at the time of data collection and receiving treatment and support on the program.
All participants provided written informed consent prior to data collection on the use and publication of data for research purposes and program improvement. Selected KP members also participated in the Focus Group Discussion (FGD) and Key Informant Interviews for health workers who offered services to the key population on the project.
The study was exempted for ethical approval as it was considered a part of program evaluation and therefore not a research.
Data Collection and Instruments
This study was conducted for three months between October 2023 and December 2023 with survey data collected synchronically for 3 weeks across 12 states with respective typologies. Structured questionnaire was adapted from the program toolkit (NAHI KP Register, 2021) and validated with interview guides for FGD and KII newly developed and pilot tested before the commencement of the study.
The sample size for the survey was determined using the 2018 KP size estimate and proportion of clients currently on treatment per facility which varies from state to state. The Cochrane formula was used to determine the minimum sample size for the study in each state of the NAHI implementation.
n = (Z2×p × q)/ E2 where Z is 95% and E is 5%.
The sample size used for each state was as follows: Edo 253, Imo 252, Enugu 232, Anambra 180, Ebonyi 177, Kaduna 162, Gombe 150, Kano 131, Abia 118, Plateau 125, Kwara 68 and 83 for Oyo state. This reporting of this section followed the STROBE principle for intervention studies (Duncan E, O'Cathain A, Rousseau N, Croot L, Sworn K, Turner KM, Yardley L, Hoddinott P. Guidance for reporting intervention development studies in health research (GUIDED): an evidence-based consensus study. BMJ Open. 2020 Apr 8;10(4):e033516. Updated November 19, 2021. https://www.equator-network.org/reporting-guidelines/guidance-for-reporting-intervention-development-studies-in-health-research-guided/).
Qualitative data were also received from KP participants through open-ended interviews during focus group discussion (FGD) on barriers to HIV prevention and treatment services and key informant interviews (KII) from at least one health worker on barriers to HIV services, efficient strategies adopted in reducing barriers and recommendations to improve further program implementation. Each focus group discussion consists of 8–10 participants across all typologies. This number of participants and reporting principles for qualitative study followed the SRQR principle by (O'Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. Updated January 19,2023. https://www.equator-network.org/reporting-guidelines/srqr/).
Quantitative data were collected using a survey through the Open Data Kit (ODK) application and Kobo toolbox with sections on demographics, Access/Uptake of prevention services, Access/ Uptake of treatment services, and barriers affecting prevention and treatment services which includes biomedical, behavioral and structural barriers among 1932 participants from 12 states of the NAHI project.
Method of Statistical Analysis
Data were first downloaded into Microsoft Excel 2019 and were scanned for missing and incomplete data, and thereafter cleaned for entry completeness. Data were transferred to and analysed using Statistical Package for the Social Sciences (SPSS) Version 23. Descriptive statistical analysis was utilized for quantitative data, which were summarized in mean and standard deviation and presented in frequency tables. Furthermore, the hypothesis was tested using regression analysis.
Method of Thematic Analysis
Qualitative data were translated to English from local languages, transcribed from audio to text including field notes in a Word document and analysed using thematic analysis on Nvivo. Transcripts were coded independently by two researchers, with inter-coder reliability checked (κ > 0.8). Thematic analysis followed Braun and Clarke's 17 framework, involving familiarization, code generation, theme searching, review and definition.
Data Management and Security
All de-identified data were transferred to a secure encrypted database with access to authorized staff only. The informed consent obtained from this study were scanned and also kept in an encrypted file securely saved on NAHI folder on the database.
Results
Sociodemographic Characteristics of Respondents
A total of 1932 respondents participated in the quantitative study across twelve states: Edo, Imo, Enugu, Anambra, Ebonyi, Kaduna, Gombe, Kano, Abia, Plateau, Kwara and Oyo of Nigeria, where the NAHI project was implemented, amounting to a 100% response rate. As presented in Table 1, most respondents (13%) resided in Edo state, followed by Imo (13%) and Enugu (12%), with the least from Kwara (4%) and Oyo (4%). There were more males (54%) than females (46%) respondents. The mean age of respondents was 31 years (±9.32), with the young adults having the highest proportion of respondents (70%), while the older adults made up the least proportion of respondents (2%). A slight majority (40%) were FSWs, 37% were in the MSM category, while the PWIDs (24%) made up the least number of respondents. Nearly half of the respondents (50%) completed secondary education, and the majority (70%) were single. On religion, over three-quarters of the respondents (78%) were Christians. Regarding employment status, almost half of the respondents (49%) were self-employed and almost half (46%) earned below minimum wage. Summarily, there were more males (54%) than females (46%) respondents overall, reflecting the inclusion of MSM (all males) and PWID (majority males). However, by typology, FSW (all females) comprised the largest group (40%), followed by MSM (37%) and PWID (24%).
Respondents’ Sociodemographic Characteristics (N = 1932).

NGN = Nigerian Naira; PWID = people who inject drugs; MSM = men who have sex with men; FSW = female sex workers.
Access to Comprehensive HIV Services: Prevention, Testing and Treatment
Minimum Prevention Packages (Testing and Prevention)
Of all the respondents (1652), as shown in Figure 1, 82% had access to HIV testing, 67% to prevention services (condom, lubricants, STI management and PrEP), while 63% had access to treatment services. Condom is the most utilized prevention package (94%), followed by lubricants (85%), then PrEP (61%), while 54% had utilized STI management services, as seen in Figure 2. Only 3% were not utilizing any of the prevention packages.

Percentage of KP with access to HIV services.

Percentage uptake of MPPI among KP typologies.
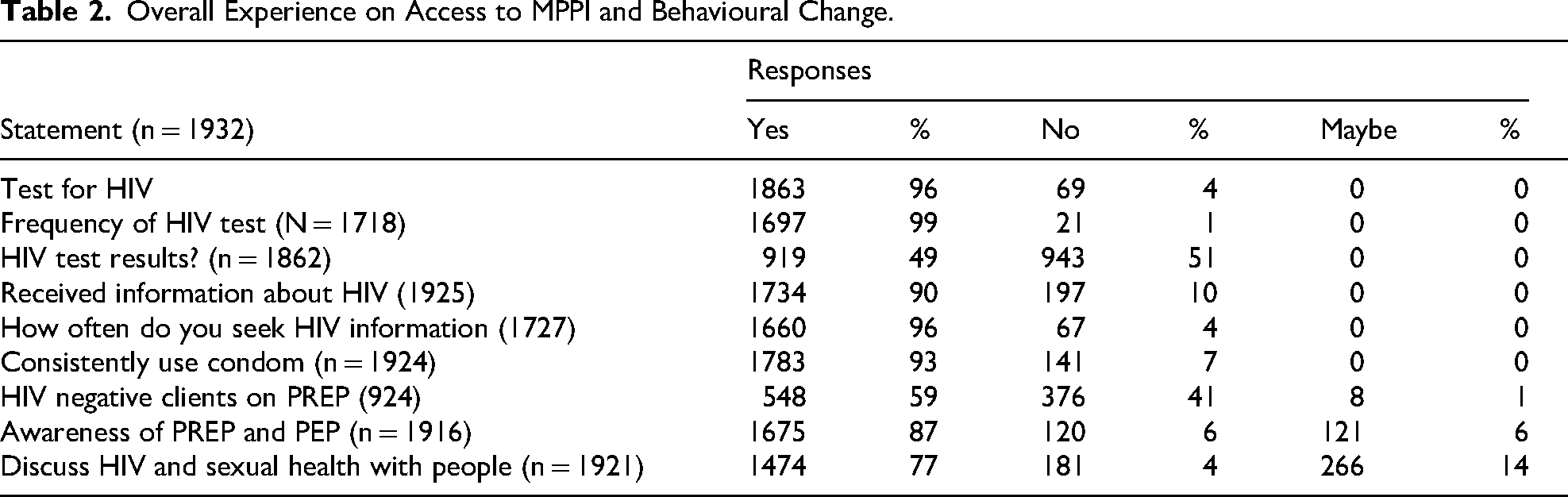
Table 2 presents an understanding of the overall experience and uptake of HIV testing services and behavioural change. Most respondents (96%) had an HIV test, and slightly less than half (49%) were positive. For those who received HIV testing, 99% continue to have HIV testing regularly (every 3–6 months). The majority (90%) sought HIV-related information, and 96% continue to seek HIV information. Also, most respondents felt comfortable discussing sexually related health matters with their partners (77%).
Overall Experience on Access to MPPI and Behavioural Change.
KP Access to Treatment Services
The majority of HIV positive KP are receiving ART treatment at our OSS (90%), which is a designated NAHI site, as presented in Table 3.
KP's Access/Enrolment on ART.

Barriers to Uptake/Access to MPPI Hindering HIV Epidemic Control Among KP
Biomedical Barriers
Fear of the test result was a major barrier among 47% of the respondents, from the 4% who have not received HIV testing, as shown in Table 4. From the rest, 27% reported not at risk of HIV, while 9% reported distance to facility as a barrier preventing them from receiving an HIV test.
Biomedical Barriers to Uptake of MPPI (HIV Testing Services).

Behavioural Barriers
Findings showed that participants with a low perceived risk of HIV accounted for 46% of the population, with 30% medium risk of HIV, as seen in Table 4. More than half (59%) of HIV negative clients are on PrEP, while 41% are not but use condoms consistently during sexual intercourse (94%) as presented in Figure 2. The majority (93%) reported consistent use of condoms during sexual intercourse, as seen in Table 3. Owing to the NAHI project's intervention, almost three-quarters of the respondents (69%) did not engage in substance-induced risky sexual behaviours, and almost half (46%) had a low perceived risk of contracting HIV. Most respondents reported a minimal influence of peers on their sexual choices (32%), and 26% reported that their peers do not influence their sexual behaviours or HIV prevention choices; most (53%) had injecting partners, and less than half (43%) had multiple injecting partners. Almost half of the respondents (49%) had multiple sexual partners. Sex with multiple partners or sharing needles and having injecting partners continue to pose a barrier to HIV prevention and transmission (Table 5).
Behavioural Barriers to Access/Uptake of MPPI.

** Multiple responses allowed, and percentages do not amount to 100%.
Barriers to Antiretroviral Treatment (ART) Hindering HIV Epidemic Control
From the few respondents who missed their medications (36%), the majority (83%) forgot their medication dates, 10% had no food to eat with 18% struggled with taking pills continuously, as seen in Table 6. Among those who did not have access to PCT services, more than half of the respondents (57%) were limited by the distance to the facility, 30% reported financial issues, 13% reported appointment wait time, and 19% struggled with taking pills every day for continuity, while 5% are still in denial of their HIV status. We could imply that forgetfulness could be associated with being newly initiated on ART and busy schedules, as the majority are young key populations who need to fend for themselves due to self-employment, as seen in Table 1 on sociodemographic characteristics of KP respondents. Also, the thought of taking pills for life could be very scary to young single people, who consume alcohol with fear of kidney failure due to alcohol consumption and ART/Prep medication.
Biomedical Barriers to ART Treatment.

**Multiple responses allowed, and percentages do not amount to 100%.
Structural and Social Justice Barriers to HIV Prevention and Treatment
Results from the survey found 24% self-reported experience of stigma and discrimination, where 48% reported perpetrators are mostly from community members and 11% by health workers. It is evident from Table 7, as shown that stigma and discrimination were not the main reasons people were not getting tested, but fear of HIV HIV-positive result, as seen in Table 4. Moreover, all forms of violence or abuse are imminent, with verbal abuse being the most pervasive (63%), with about 15% reported sexual abuse. However, 64% of the respondents reported that they got HIV-related support from the community.
Structural Barriers to HIV Prevention and Treatment.

** Multiple responses allowed, and percentages do not amount to 100%.
Socioeconomic variables (marital status, educational level, employment status, income level and religion) collectively predict HIV risky behaviour among key populations (R = .201) as shown in Table 8. However, the overall model explains only 4% of the variance in HIV risky behaviour among key populations. Nevertheless, the model remains statistically significant. This proved that even though socioeconomic factors are predictors of HIV risk behaviours, HIV risk behaviours among key populations had significantly reduced, leaving multiple sexual/injecting partners and violence or abuse as major behavioural barriers to achieving epidemic control.
Multiple Regression of Socioeconomic Variables and HIV Risky Behaviour.

**R = .201; R2 = 040; adjusted R2 = .037; SE = 2.143.
Further analysis via regression ANOVA revealed a marginal joint linear association of the predictor variables on HIV risky behaviour among key populations (F(5,1703) = 14.297, p = .000). The adjusted R-square value of .037, with shrinkage from the unadjusted R-Square of .040, suggests the model's potential generalizability to the population (SE = 2.14).
These findings suggest that when all predictor variables (marital status, educational level, employment status, income level and religion) are collectively considered, HIV risky behaviour decreases. Consequently, we can conclude that socioeconomic variables significantly predict HIV risky behaviour among key populations.
Further analysis was conducted to assess the individual contribution of each predictor variable to HIV risky behaviour. Among the five socioeconomic variables studied, educational level (β = .130, t = 5.106, p = .000), employment status (β = .077, t = 2.842, p = .005), income level (β = .141, t = 5.261, p = .000) and religion (β = .082, t = 3.378, p = .001) emerged as significant predictors. This indicates that respondents’ educational level, employment status, income level and religion significantly influence HIV risky behaviour among key populations (KPs), with 13%, 7.7%, 14.1% and 8.2% of the variance in HIV risky behaviour among KPs attributed to these factors.
Respondents with no formal education demonstrated a higher likelihood of engaging in HIV risky behaviour, whereas KPs with tertiary education are less likely to be involved in such behaviour, as illustrated in Figure 3. Similarly, Figure 3 illustrates that KPs in paid employment demonstrate a lower likelihood of engaging in HIV risky behaviour, whereas unemployed KPs are more likely to be involved in such behaviour.

Educational level and HIV risky behaviours.
Nevertheless, marital status (β = .006, t = .250, p > .05) did not emerge as a significant predictor, as seen in Figure 4. This suggests that when marital status is examined independently, it does not exert a significant influence on HIV risky behaviour. Additionally, our findings, as depicted in Figure 5, indicate that although there was no significant influence detected, married KPs exhibited a lower level of HIV risky behaviour, while separated KPs showed a higher likelihood of engaging in such behaviour.
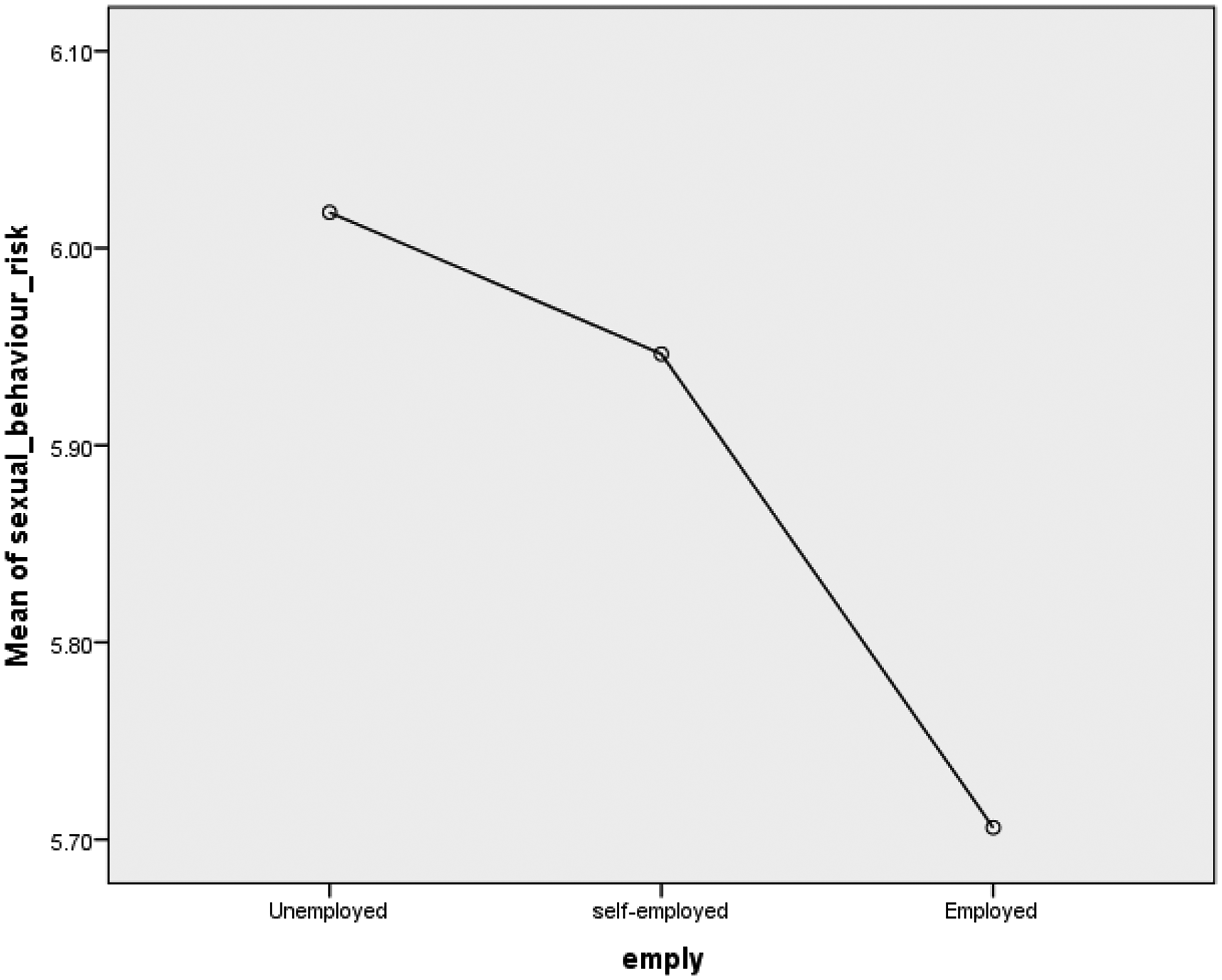
Employment status and HIV risky behaviours.

Marital status and HIV risky behaviour.
Qualitative Results
Focus Group Discussion on Biomedical Barriers to HIV Prevention and Treatment Services
Based on thematic qualitative results of FGD among KP participants, the following are biomedical barriers preventing KP from accessing and uptake of HIV prevention and treatment services.
Pill burden due to non-stop ingestion of ART Adverse drug reaction to ART Unavailability of ART refills and Adherence support in the community, except at the OSS
Focus Group Discussion on Behavioural Barriers to HIV Prevention and Treatment Services
Multiple sexual/injecting partners
Unprotected sex due to unplanned sex
Restricted access to condoms and lubricants in the community
Focus Group Discussion on Structural Barriers to HIV Prevention Services
Distance to OSS for care and support
Financial problems due to unemployment/business capital affecting nutrition
Hike in transportation due to fuel prices
Violence/abuse
Stigma and discrimination from health workers
Parental neglect
Homelessness
Quotes From Respondents on Barriers and Recommendations to Improve Access to HIV Services
“I have a concern. Someone outside the OSS learned about my HIV status, and this makes me doubt the health workers’ confidentiality at the OSS and the community”.
“Sometimes when we come to the OSS for condoms and lubricants, it is unavailable. “We wish they could always make it available as much as possible”.
“Through digital platforms, one can continue to have access to information and knowledge of HIV and adherence counselling without having to go to the OSS to minimize the cost of transport.
“How would we think of safe sex when we do not have a home to rest. Our home is our bunk, and we do not have interest in sex, but when it happens, it is not planned.”
“I think if someone is busy doing a business or learning a skill, it will reduce commercial sex work and frequent hanging out at KP hotspots, which influence unprotected sex and HIV transmission.”
“I learnt fashion designingI. If I can get access to funds to improve my business, it will improve my adherence to ART and encourage other PLHIV not enrolled in care or lost to follow-up to seek treatment.”
“I have noticed few health workers, especially during refills, have this judgmental undertone. I feel like the staff are unprofessional and don’t do their work properly. I hate to see judgment on their faces; I want them to do their job without any bias.”
FGD on Suggestions for Improving Access to HIV Services From KP Participants
Vocational and digital training to reduce idleness and increase employment opportunities.
Access to business start-up capital to reduce commercial sex work.
Free HIV prevention vaccine to replace PrEP/ ART daily ingestion.
Digital tools to assess and manage adherence counselling and MHPSS reducing long wait times at OSS and anonymity for confidential purposes.
Professional training on handling confidentiality among health workers
Key Informant Interview With Health Workers on Barriers Hindering PCT Services
At least one health worker (Nurse, Data officers, Pharmacist, Case managers) from each of the 12 states participated in the key informant interview to identify barriers hindering the implementation of HIV prevention, care and treatment services.
Stock out of commodities such as condoms and lubricants. Distance of OSS to some local government areas in the state for MPPI distribution. Low staff strength, which sometimes leads to burnout and job turnover. Long waiting hours when there is a surge of clients for HIV retesting, adherence counselling and MHPSS. Hike in transportation due to fuel subsidy. A low number of clients are participating in support groups due to limited funds available for support. Poor documentation of MPPI kits by the staff of KP Community Based Organisation. No weekend services when some clients are only available for medication refills, HIV retesting and other supports.
Adopted Strategies in Reducing Previous Barriers to HIV Services
Use of the Community ART team for community HIV testing and treatment
Monthly Advocacy visits to faraway communities for HIV education, testing and prevention
Creation of synergy between OSS case managers and community case managers, both selected from the KP community, to reduce stigma and discrimination and monitor tracking of clients.
Creation of drop-in-centres in each local government to supplement OSS duties.
Monthly support group sessions for different typologies with assisted funds for transport.
Joint supportive supervisory visits for Stakeholders’ alignment.
Quarterly data quality assurance, weekly data reporting and daily stand-up meetings for discussion on program activities.
Suggestions in Improving Barriers to HIV Services for Epidemic Control
Increased staff strength at the OSS and the community.
Provide job security through program sustainability by institutionalizing KP-friendly clinics.
Emotional and well-being support for clinical staff to manage workload and burnout.
Use of digital tools in assessing and managing adherence and MHPSS supports to reduce wait time at the clinic and improve work–life balance.
Vocational and digital skills training for members of KP.
Access to business start-up capital for members of key populations to reduce commercial sex work.
Reduce commodities stockouts with adequate testing kits, condoms and lubricants.
Discussion
The study identified all form of barriers faced by clients and health providers on the NAHI grant which includes medical, behavioral and structural barriers and suggested strategies to further reduce these barriers in contribution to reaching HIV epidemic control in Nigeria by 20230.
Findings from the study supported the Key population size estimates by NASCP, 3 where the number of FSW was higher (about 740,000) than any other typologies across Nigeria.
From the overall participation, there were more male participants than females due to participation of MSM (all males) and PWID (majority male), but based on typology, FSW have higher participation reflecting the population of FSW in the NAHI program. It is noteworthy to mention that typology is the classification method used to distinguish different key population categories based on their vulnerability to HIV, and this is quite different from gender identity (males, females and transgender) and sexual orientation (heterosexuality, homosexuality and bisexuality). In this study, participants identified themselves as either males or females and belonging to either FSW, MSM and PWID whereas transgender population are also members of the MSM community.
Additionally, majority of respondents are young people which aligns with the findings from Baggaley R. et al in 2015 “young key population are highly vulnerable and struggle to stay healthy due to discrimination.”
From the study, access to prevention services such as condoms and lubricants have contributed to reduced perception of HIV risk and promoting health-seeking behaviours. These support the findings of 16 that “integration of condom and lubricants, harm reduction and other prevention packages promote health seeking and reduce HIV risk sexual behaviours among KP.”
The high proportion of KP who reported positive during the study is inline with the country's estimation of HIV new infection rate among KP according to Reference 4. The country HIV response team inline with guidance from World Health Organization recommended regular testing for KP every 3 months because of their vulnerability and at high risk of HIV, hence the high testing rate among key populations on the NAHI project.
Before the NAHI project, criminalization and unfavourable contacts between police and KP members exist contributing to stigma and discrimination which was addressed by the NAHI strategic action of providing HIV awareness and KP-friendly training to law enforcement officers, drug response team, health providers and others for improved service adoption. This training reduced bunk rading of PWID and harassment f FSW but same sex marriage is still prohibited in Nigeria according to the constitution but not preventing MSM from accessing routine healthcare services. As it is, stigma and discrimination though still relatively high agrees with the statements from by Jin H. et al.10,13 However, from the survey, perpetrators of stigma and discrimination were rather family members, health providers and community members but not law enforcement officers (police).
All forms of abuse are still relatively high as evident from the study which agrees with the statement by Sabathy et al. 8 Interviews from the focus group discussion revealed few respondents mentioned judgmental attitudes from health workers in a few states contributed to the barriers in accessing PCT services. This study, based on the Nigerian context, is not far from the findings 9 who reported that stigma and discrimination, verbal, and emotional abuse are from health providers.
Furthermore, KP with low education, self-employment and unemployment exhibited higher HIV risk behaviours. We could infer that low educational attainment, unemployment and low or no income earning predispose KP to unsafe sexual practices such as transactional sex and multiple sexual partners. Though marital status did not show much significance on its own; however, collectively with other socioeconomic factors, it poses a risk of HIV as well. Previous studies haven’t discussed these concepts as barriers but pose serious threat to achieving HIV epidemic control in Nigeria on NAHI project. Because KP engage in transactional sex, they have multiple sexual partners and/or injecting partners, access to condoms and lubricants from the OSS and community is still restricted due to stcockout as gathered from health workers.
While previous studies only focused on structural barriers from the clients perspectives, this study emphasized biomedical, behavioural and structural barriers from clients and health providers with insights for future interventions and health policies. Digital skills training for clients and staff, with use of digital tools to manage adherence and MHPSS was notably mentioned by clients and staff at NAHI sites.
Limitations of the Study
This study has several limitations that should be considered when interpreting the findings. The reliance on self-reported data introduces potential social desirability bias, as KP participants may have underreported risky behaviours or overreported service uptake due to stigma or fear of judgment. The cross-sectional design precludes establishing causality between socioeconomic factors and HIV risky behaviours, limiting our ability to assess temporal relationships.
Additionally, transgender participants were categorized as part of the MSM community based on sexual orientation and not gender identity which may limit the generalizability of findings to this subgroup.
Finally, the regression model explained only 4% of the variance in HIV risky behaviours (adjusted R2 = 0.037), suggesting unmeasured factors (eg, psychological or cultural influences) may play a significant role. Future longitudinal studies with broader representation and objective measures could address these limitations.
Recommendations
To expand HIV prevention, care, and treatment (PCT) services and achieve epidemic control among key populations (KPs) in Nigeria under the National Aligned HIV/AIDS Initiative (NAHI), we proffer the following prioritized recommendations based on study findings.
Short-term (0-12 months):
Eliminate immediate barriers to PCT access via improved commodity availability and service delivery. Supply condoms and lubricants with routine supply, as stock-outs were very frequently reported in FGDs and key informant interviews (KIIs). Increase staffing at OSS to reduce waiting time and workload among health workers. Implement professional training for health workers to boost confidentiality and reduce judgmental attitudes. Provide emotional and mental well-being support for clinical staff.
Medium-term (1-3 years):
Promote economic empowerment to decrease financial barriers and HIV risky behaviours that are linked to low income and unemployment. Provide vocational and digital skills-building training programs to decrease reliance on transactional sex among FSW and MSM. Expand digital health platforms, including virtual adherence counseling, to increase access and decrease transportation costs.
Long-term (3-5 years):
Advocate for structural and legal reforms to address systemic barriers, including stigma and abuse. Strengthen community-based interventions and engage policymakers to reduce criminalization of KP behaviours, building on NAHI's sensitization efforts with law enforcement. Integrate mental health and psychosocial support services into HIV programming to enhance adherence and viral suppression.
Conclusion
Though the program reached its goal of reducing HIV burden and increases access to prevention and testing servives through the differentiated model of care, barriers hindering epidemic control among KP persists as seen in this study. This study proved that socioeconomic factors could increase vulnerability to HIV risky behaviors and that stock-out of commodities, attitude of health workers, pill burden, mental health, financial constraints and multiple sex/drug use partner contribute hinder epidemic control among KP in Nigeria.
Since socioeconomic factors contribute to HIV sexual risk behaviours and access to prevention and treatment, introducing digital and vocational empowerment programs to improve retention, income and means of livelihood will increase the chances of achieving HIV epidemic control among key populations in Nigeria before 2030. Furthermore, strengthening mental health and psychosocial support services through telehealth will improve medication adherence, ART suppression and reduce wait time at the facilities. Since abuse and violence are prevalent among KPLHIV, an approach to managing KP- or HIV-related abuse and violence should be introduced into HIV programming to enhance treatment retention and viral suppression. When priorities are given to both staff and clients, access to prevention, treatment and care are not just possible but capacities are also built economically, socially and mentally. This will reinforce informed decisions towards KP sexual health and enhance staff strength and motivation to provide comprehensive services with non-judgmental attitudes.
Supplemental Material
sj-pdf-1-jia-10.1177_23259582261423609 - Supplemental material for Barriers to HIV Prevention and Treatment Services in Achieving Epidemic Control Among Key Population in Nigeria: An Implementation Science Study on NAHI Project
Supplemental material, sj-pdf-1-jia-10.1177_23259582261423609 for Barriers to HIV Prevention and Treatment Services in Achieving Epidemic Control Among Key Population in Nigeria: An Implementation Science Study on NAHI Project by Ganiyat O Kareem, Christiana Laniyan, Christopher Akolo, Philip Imohi, Joseph Ashivor, Emeka Anoje, James E. Uba, Ugbe Maurice-Joel Ugbe, Samson Bamidele, Uche Amalu, Oluwapelumi Aliu, Joyce Ndam, Nibretie Workneh, Uchenna Michael Ugwoke, Onyinoyi Aishatu Adegbe, Mary Morenike Oguntokun, Ofem Obeten and Leah Umeokeke in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-2-jia-10.1177_23259582261423609 - Supplemental material for Barriers to HIV Prevention and Treatment Services in Achieving Epidemic Control Among Key Population in Nigeria: An Implementation Science Study on NAHI Project
Supplemental material, sj-pdf-2-jia-10.1177_23259582261423609 for Barriers to HIV Prevention and Treatment Services in Achieving Epidemic Control Among Key Population in Nigeria: An Implementation Science Study on NAHI Project by Ganiyat O Kareem, Christiana Laniyan, Christopher Akolo, Philip Imohi, Joseph Ashivor, Emeka Anoje, James E. Uba, Ugbe Maurice-Joel Ugbe, Samson Bamidele, Uche Amalu, Oluwapelumi Aliu, Joyce Ndam, Nibretie Workneh, Uchenna Michael Ugwoke, Onyinoyi Aishatu Adegbe, Mary Morenike Oguntokun, Ofem Obeten and Leah Umeokeke in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-3-jia-10.1177_23259582261423609 - Supplemental material for Barriers to HIV Prevention and Treatment Services in Achieving Epidemic Control Among Key Population in Nigeria: An Implementation Science Study on NAHI Project
Supplemental material, sj-pdf-3-jia-10.1177_23259582261423609 for Barriers to HIV Prevention and Treatment Services in Achieving Epidemic Control Among Key Population in Nigeria: An Implementation Science Study on NAHI Project by Ganiyat O Kareem, Christiana Laniyan, Christopher Akolo, Philip Imohi, Joseph Ashivor, Emeka Anoje, James E. Uba, Ugbe Maurice-Joel Ugbe, Samson Bamidele, Uche Amalu, Oluwapelumi Aliu, Joyce Ndam, Nibretie Workneh, Uchenna Michael Ugwoke, Onyinoyi Aishatu Adegbe, Mary Morenike Oguntokun, Ofem Obeten and Leah Umeokeke in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
List of Abbreviations
Acknowledgements
The authors sincerely acknowledge the contributions of the Global Fund HIV/TB Grant team, the Federal Ministry of Health (FMOH), Nigeria, the National Agency for the Control of AIDS (NACA) and the National AIDS and STI Control Programme (NASCP) for their technical guidance and support. This study was conducted as part of the National Aligned HIV/AIDS Initiatives (NAHI) Project evaluation to identify barriers to HIV prevention and treatment services hindering epidemic control in Nigeria. Special appreciation goes to the principal recipient, FHI 360 and the sub-recipients: Society for Family Health (SFH), Achieving Health Nigeria initiative (AHNi) and Excellence Community Education Welfare Scheme (ECEWS) for their leadership, coordination and data access support. We also extend gratitude to all key population community-based organizations (CBOs) across participating states whose active collaboration, participants recruitment and field engagement were instrumental to the success of this evaluation. We thank the study participants, program team, healthcare providers, peer educators, outreach workers and implementing partners who provided valuable insights and made this research possible.
ORCID iDs
Ethical Consideration and Statement of Informed Consent
The FHI 360 Office of International Research Ethics (OIRE) reviewed the study protocol and granted an exemption from full ethical review (Protocol No. 2097844-1), determining that the evaluation did not meet the regulatory definition of research as stated under the U.S. Department of Health and Human Services Code of Federal Regulations [45 CFR Part 46.102]. The study was classified as a program/service evaluation within the framework of the Nigeria HIV and AIDS Indicator and Impact (NAHI) project, designed to assess HIV epidemic control among key populations receiving prevention and treatment services.
Although exempt from full IRB review, OIRE approved the requirement for informed consent due to human participation. The Federal Ministry of Health (FMOH) Ethics Committee provided local ethical clearance (Ref No. NHREC/01/01/2007-25/09/2023) approving the study protocol, questionnaires, interview guides and consent procedures.
All participants provided written and signed informed consent before enrolment. Research assistants read and explained the consent form to ensure comprehension, voluntary participation and the right to withdraw at any stage. Participants were fully informed of the study's purpose, procedures, potential benefits and minimal risks. Confidentiality and data protection were guaranteed throughout the process.
Focus Group Discussion (FGD) participants received modest transport reimbursement and time compensation. All interview recordings were made using encrypted devices (Samsung tablets) and stored securely in the NAHI project's restricted-access, password-protected database. Paper-based consent forms were locked in secure cabinets before being digitized and archived in encrypted folders accessible only to authorized personnel.
The study complied with the ethical principles outlined in the Declaration of Helsinki (2013 revision) and all relevant FHI 360, Federal Ministry of Health, and Global Fund HIV/TB project ethical standards for human subjects’ research and program evaluation.
Authors Contributions
Ganiyat O. Kareem developed the study protocol, co-developed data collection tools and conducted the literature review and responsible for the manuscript (start to finish) including the manuscript preparation and dissemination.
Akolo Christopher, Anoje Emeka, Joseph Ashivor, Philip Imohi and Christiana Laniyan conceptualize the title, reviewed the study protocols, provided methodological and technical guidance throughout the project and contributed to the final review of the manuscript including abstract submission.
Uba James, Bamidele Samson and Ashivor Joseph coordinated the research team, develop research memo, performed statistical analysis and oversaw submission of the study for ethical approval.
Ugbe Maurice Joel, Ndam Joyce Nana, Ugwuoke Uchenna, Aliu Oluwapelumi and Amalu Uche, co-developed the questionnaires and interview guides adapted from the Integrated Biological and Behavioural Surveillance Survey (IBBSS) and national program tools, and jointly supervised data collection activities in the field.
Workneh Nibretie provided expertise review and guidance on the full manuscript, including updated literature reviews where applicable.
Oguntokun Mary Morenike, Adegbe Aishatu Onyinoyi, Obeten Ofem and Umeokeke Leah supported with data collection, cleaning and preliminary analysis and contributed to reviewing and finalizing the manuscript. All authors read and approved the final version of the manuscript.
Funding
This study was supported by the
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.