
Abstract
Background
Launched in the United States (US) in 2016, the ‘undetectable equals untransmittable’ (U = U) message has revolutionized human immunodeficiency virus (HIV) management by affirming that individuals on antiretroviral therapy (ART) with undetectable viral loads (VL) cannot sexually transmit the virus. This study aimed to assess the knowledge and understanding of U = U and factors associated with the lack of understanding among people living with HIV (PLHIV) in the US.
Methods
A cross-sectional, online survey was fielded from February to June 2022 in the US to PLHIV aged ≥18 years who were currently taking ART. Data on sociodemographic variables, HIV-related and general health characteristics were collected. The study assessed the knowledge and understanding of U = U and sources of U = U information. Multivariable analyses were used to identify the factors associated with the lack of U = U understanding among PLHIV.
Results
A total of 781 PLHIV completed the study and were included in the analysis. Most participants were <50 years old (67.0%), cisgender males (56.2%), and majority having at least some college education (80.5%). More than half (54.5%) of the participants did not know the meaning of the U = U. Sources of learning about the meaning of ‘undetectable’ included a healthcare provider (HCP) alone (50.4%), the U = U campaign alone (7.6%), both an HCP and the U = U campaign (14.7%), and sources other than HCPs or the U = U campaign (32.2%); 3.1% of participants reported having never heard the term before. About 12.0% of the participants were unaware of their VL status. After adjusting for covariates, PLHIV who lacked an understanding of U = U were more likely to have a college degree or higher education (OR: 0.6, 95% CI: 0.41-0.86, P = 0.006), recent HIV diagnosis (6 months to <12 months) (OR: 2.06, 95% CI: 1.14-3.77, P = 0.018), suboptimal ART adherence (OR: 2.74, 95% CI: 1.88-4.01, P < 0.001), and lack HCP communication about the importance of an undetectable VL compared to those who understood U = U.
Conclusion
The study highlights substantial gaps in understanding U = U among PLHIV and in HCP-patient communication. These findings underscore the need for targeted education for both PLHIV and HCPs, emphasizing the clinical implications and benefits of U = U in relation to HIV prevention.
Plain Language Summary
The U = U message means that people living with HIV who are on treatment and have undetectable levels of the virus in their blood cannot pass the virus to others through sex. The study shows that many people living with HIV and healthcare providers do not fully understand the U = U message. It highlights the importance of educating both these groups about how U = U can help prevent HIV transmission and improve patient care.
Keywords
Introduction
Human immunodeficiency virus (HIV) remains a public health challenge. In the United States (US), there were approximately 1.2 million people living with HIV (PLHIV), with around 31,800 new infections in 2022.1,2 The National HIV/AIDS Strategy 2022–2025 for the US has outlined four critical objectives to combat the HIV epidemic within the nation, including i) the prevention of new HIV infections, with a target to achieve a 90% decrease in new HIV infections by 2030; ii) the enhancement of HIV-related health outcomes among PLHIV; iii) the reduction of HIV-related disparities; and iv) the achievement of integrated and coordinated action among all stakeholders. 3
Antiretroviral therapy (ART) has substantially reduced mortality, 4 increased life expectancy,5-7 and improved quality of life8,9 over the past two decades. Importantly, ART has been instrumental in reducing the risk of sexual transmission of HIV by achieving viral suppression.10-16 Viral load (VL) that is too low to be detected by standard tests, is classified as an ‘undetectable viral load’. The risk of sexual transmission is zero when PLHIV maintain an undetectable VL or a viral load less than 200 copies/mL,17,18 and there is almost zero or negligible risk of transmission when the VL is from 200 to 1000 copies/mL. 19
The clinical concept of ‘Treatment as Prevention (TasP)’,18,20-22 clarified and adapted by the community into the ‘Undetectable equals Untransmittable (U = U)’ message, indicates that the best way to prevent transmission of HIV is through achieving and maintaining an undetectable viral load through adherence to ART.18,23 The U = U campaign was launched in 2016 by the Prevention Access Campaign (PAC) to build scientific consensus, raise awareness, and promote the knowledge about U = U with the mission to end the HIV epidemic and HIV-related stigma. 24 PAC worked with civil society organizations, HIV advocacy groups, and PLWH networks worldwide to endorse and promote the U = U message. Education about U = U is especially needed in the US, where viral suppression is low, with just 65% of diagnosed PLHIV in 2022 having viral suppression at their most recent VL test. 25
Awareness of U = U has been shown to reduce anxiety and stigma, promote timely HIV testing, enhance treatment adherence, and improve viral suppression among PLHIV.26-29 It may support safer family planning in serodiscordant couples.30,31 Moreover, PLHIV who discussed the U = U concept with their healthcare providers (HCPs) have demonstrated an increased level of comfort in sharing their HIV status and discussing their related concerns with HCPs. 26 Therefore, awareness and understanding of U = U among PLHIV is imperative, considering its overarching benefits not just for PLHIV but also from the broader public health perspectives.
The World Health Organization (WHO) underscores the importance of clinicians educating PLHIV that maintaining an undetectable VL carries zero risk of sexual HIV transmission, provided adherence to ART. 17 A cross-sectional survey conducted in 25 countries reported that on average, two-thirds of PLHIV had discussed U = U with their HCPs; though this varied by country, from 38% in South Korea to 87% in Switzerland). 26
Factors such as racial identity, 32 social marginalization, 33 low income, 32 and heterosexuality 34 have been identified as barriers to understanding and awareness of U = U. Additionally, HCP-specific barriers such as limited information, inconsistent acceptance of U = U, and hesitancy to discuss the concept,27,35 may further impact HCP-patient communication about U = U. A lack of appropriate resources tailored to a diverse population can also influence communication of U = U. 35
Previous studies in the US have also reported varying proportions of awareness27,36,37 (ranging from 69% to 95%) and low level of trust in the U = U concept (<43%)36,38 among PLHIV and/or individuals who are HIV-negative. However, they were either limited to specific regions within the US or focused on minority populations, not fully exploring factors that influence patients understanding of U = U in detail.29,34,36-38
The aim of this study was to assess the knowledge and understanding of U = U and identify factors associated with a lack of understanding of U = U in a broader population of PLHIV across the US.
Methods
This non-interventional, cross-sectional, online survey of people living with HIV in the US was conducted from February 22, 2022, through June 2, 2022. The study participants were PLHIV who were members of the opt-in general-purpose (ie, not health care specific) web-based Kantar Profiles consumer panel or a member of one of Kantar Profiles’ panel partners. Email invitations were sent to potential respondents in optimized batches, such that not all eligible respondents received an invitation on the same day. Participants were recruited from across the US. Initially, a natural fallout method (ie, no quotas were put on the participants entering the survey) was used to administer the survey. However, quota recruitment at the end of March 2022 was conducted owing to the underrepresentation of younger (<25 years old) and older (65 + years old) participants. Therefore, during the quota recruitment period, only those <25 years or >65 years of age were permitted to complete the survey.
Prior to the quantitative data collection, qualitative pretests were conducted with a convenience sample of PLHIV (n = 15) to assess if the questionnaire accurately measured the intended design. Feedback from the pretests was used to edit and refine survey questions and formatting to ensure that all questions, language, and format were clear.
The study protocol was reviewed by an Institutional Review Board (Pearl IRB, Indianapolis, IN) (IRB #21-KANT-269) and received an exemption under FDA 21 CFR 56.104 and DHHS 45 CFR 46.104 regulations. All participants provided written informed consent electronically prior to assessing the survey. Methods to minimize bias included using quotas to recruit a demographically diverse sample of PLHIV to reduce selection bias, sending survey reminders to help reduce non-response bias, informing participants of the privacy of their responses to reduce social desirability or other response biases, and randomizing the order or response options and statements rated on the same scale to reduce order bias.
The reporting of this study conforms to the STROBE cross sectional reporting guidelines (Supplemental Material: STROBE checklist). 39
Study Sample
Participants were considered eligible if they were aged ≥18 years, diagnosed with HIV, were receiving ART, and received the HIV treatment for ≥6 months at time of survey administration, could read and write in English, and provided informed consent. Participants who did not provide informed consent or did not complete the survey were excluded from analyses. A total of 781 PLHIV participated in the study.
Study Measures
A list of survey questions and measures is included in Supplemental Table 1. Data on sociodemographic including age, sex at birth, gender identity, sexual orientation, race/ethnicity, education, employment status, insurance type, US census region, and location of residence were collected. Data on general health characteristics such as body mass index (BMI), smoking status, burden of non-HIV comorbidities including self-reported medical conditions and sexually transmitted infections (STIs), and social determinants of health (SDOH) including housing instability [ratings of somewhat to extremely worried about stable housing] and food insecurity [ratings of sometimes to always worried food would run out before having the chance to buy more] were collected.
HIV-related characteristics including duration of infection (6 months to <1 year, 1 to <5 years, 5 to <10 years, ≥ 10 years), ever been undetectable or virally suppressed, VL status at time of survey completion, and length of time of being undetectable or virally suppressed (<6 months, 6 to <12 months, 1 to <5 years, ≥ 5 years, don’t remember) were assessed. VL status was defined as undetectable (self-reported undetectable or reported the actual VL <200 copies/mL), detectable (≥200 copies/mL), or unaware of VL status. Polypharmacy was assessed by asking PLHIV if they were taking ≥5 pills/day or currently taking medicines for ≥5 conditions. Number of HIV treatment switches was also collected. Adherence to HIV medication was captured by using a survey question asking the frequency (‘never to rarely’, ‘sometimes’, ‘often to always’) of intentionally or purposefully skipping doses of any of the medications at the time of the survey; suboptimal adherence was defined as ratings of sometimes, often, or always. In addition, participants rated their satisfaction with their current HIV treatment.
Other measures included in this study were poor self-rated overall health (yes = ratings of “poor” or “fair”), trust in information received from their clinician (yes = ratings of “somewhat agree” or “strongly agree”), difficulty verbalizing health concerns in each of four areas: general wellness concerns, non-HIV-related illness concerns, sexual health concerns, and HIV health concerns (yes = ratings of somewhat or extremely difficult), overall difficulty verbalizing health concerns (yes = ratings of somewhat or extremely difficult in ≥1 area(s)), and satisfaction with primary clinician who manages HIV. Furthermore, the Patient Activation Measure® (PAM®) was used to assess respondent's knowledge, skills, and confidence in managing their own health and healthcare. It consists of 13 items, with a score ranging from 0 to 100; higher score represents a greater patient activation. Based on the PAM scores, respondents were categorized into four levels of activation including “disengaged and overwhelmed” (level 1, range: 0 = 47.0), “becoming aware but still struggling” (level 2, range: 47.1 = 55.1), “taking action and gaining control” (level 3, range: 55.2 = 72.4), and “maintaining behaviors and pushing further” (level 4, range: 72.5 = 100). 40
Study Outcomes
The lack of knowledge about U = U was defined as ‘no knowledge of U = U at all, or never heard about this term’. The understanding of U = U was assessed based on the survey question, ‘What does the phrase undetectable mean to you related to HIV?’ Participants selecting at least one of ‘I cannot transmit the virus sexually’ and ‘I can’t pass HIV onto others’ with or without also selecting ‘I am virally suppressed’ and without selecting any other responses were considered to have an understanding of U = U. Any other selection (≥1 of the following: I am cured, I can have carefree sex, I can still pass HIV onto others, I was misdiagnosed with HIV and never had it to begin with, my immune system fought the disease, and I no longer have HIV, or not sure) was defined as lack of understanding of U = U.
Participants were also asked to specify their source of information about U = U in context of HIV and were able to select all that apply. These data were collapsed into the following categories: ‘HCP but not U = U campaign’, ‘U = U campaign but not HCP’, ‘both HCP and U = U campaign’, ‘other source’, and ‘never heard that term before’. Participants who reported hearing about U = U from an HCP were asked to share the details of their communication with the HCP (Supplemental Table 1).
Statistical Analyses
Study variables were summarized and presented as means and standard deviations or counts and percentages. As missing data were by design (ie, some questions were asked only to a subset of respondents based on an earlier survey response – eg, number of treatment switches was only asked of those who had a switch in treatment), no efforts were made to impute missing values. Instead, when there was missing data due to survey skip logic, either the number of participants answering the question was reported (eg, length of time virally suppressed in Table 1) or the data were recoded such that all participants had a response (eg, number of treatment switches was recoded to include a “none” category, which included the number of participants who selected “no” in response to the question, “Have you ever switched from one HIV prescription medication to another?”).
Sociodemographic and Health Characteristics of the Study Participants.

Excludes 1 respondent who reported being insured but did not know which type of insurance.
Respondents did not select any comorbidity listed in the survey, but could have another condition that was not listed.
Abbreviations: BMI, body mass index; HIV, human immunodeficiency virus; HPV, human papillomavirus; max, maximum; min, minimum; STIs, sexually transmitted infections.
Bivariate analyses were conducted to identify the factors associated with the lack of understanding of U = U, using independent samples t-tests to compare continuous variables and chi-square test to compare categorical variables. Power analysis using a t-test for mean differences in independent samples, a significance level of 0.05, 80% power, and achieved sample sizes for the lack of understanding of U = U measure (yes: n = 426; no: n = 355) was used to understand the detectable effect sizes. There was sufficient sample to detect a small effect size with our current samples (Cohen's d = 0.21).
In multivariable analyses, a logistic regression model was used to assess the factors associated with the lack of understanding of U = U. Covariates were selected based on clinical importance and statistical significant differences in the bivariate analysis that include age, gender identity, sexual orientation, race/ethnicity, education, duration of HIV, VL status at the time of survey completion, suboptimal ART adherence, difficulty of verbalizing health concerns, PAM® score, HCPs’ lack of communication about undetectable VL with their patients, and depression. Odds ratios (OR) and 95% confidence intervals (CI) were generated and P-values of <0.05 (two-tailed) were considered statistically significant. All statistical analyses were conducted using R version 4.3.1 and IBM® SPSS Statistics version 28.
Results
Sociodemographic and Health Characteristics
A total of 2081 participants accessed the study survey online. Among these 1943 were screened for eligibility, where 781 participants met the criteria and completed the study (Figure 1). Most participants were aged <50 years (67.0%), cisgender male (56.2%), and about half (51.5%) were non-Hispanic White followed by non-Hispanic Black or African American (24.5%) (Table 1). About 46% of the participants self-identified as heterosexual and 36.1% as gay, lesbian, or same-gender loving. Approximately two-thirds of male participants (67.1%) were men who have sex with men (MSM). Most participants had some college level education (some college or associate degree: 41.7%, college degree or higher: 38.8%) and were employed (69.1%). At the time of the survey, 93.0% of the participants were insured under government (50.2%) or commercial/private (42.8%). About one-third of participants each were ‘very to extremely worried about stable housing’ (33.9%) and ‘often or always worried about food running out before they had the chance to buy more’ (32.8%) (Table 1).

Flow Chart Showing the Construction of the Study Sample.
Clinical and Treatment Characteristics
About 55.0% of the participants had HIV for ≥5 years and the majority (90.8%) ever had undetectable VL or were virally suppressed. At the time of survey completion, 85.5% of participants had an undetectable VL, of which 38.8% reported being undetectable or virally suppressed for ≥5 years. The majority (58.6%) reported more than two comorbidities and 40.2% reported polypharmacy. About 42.0% of participants reported sometimes, often, or always intentionally or purposefully skipping ART doses, indicating suboptimal adherence to HIV medications (Table 2).
Clinical and Treatment Characteristics.
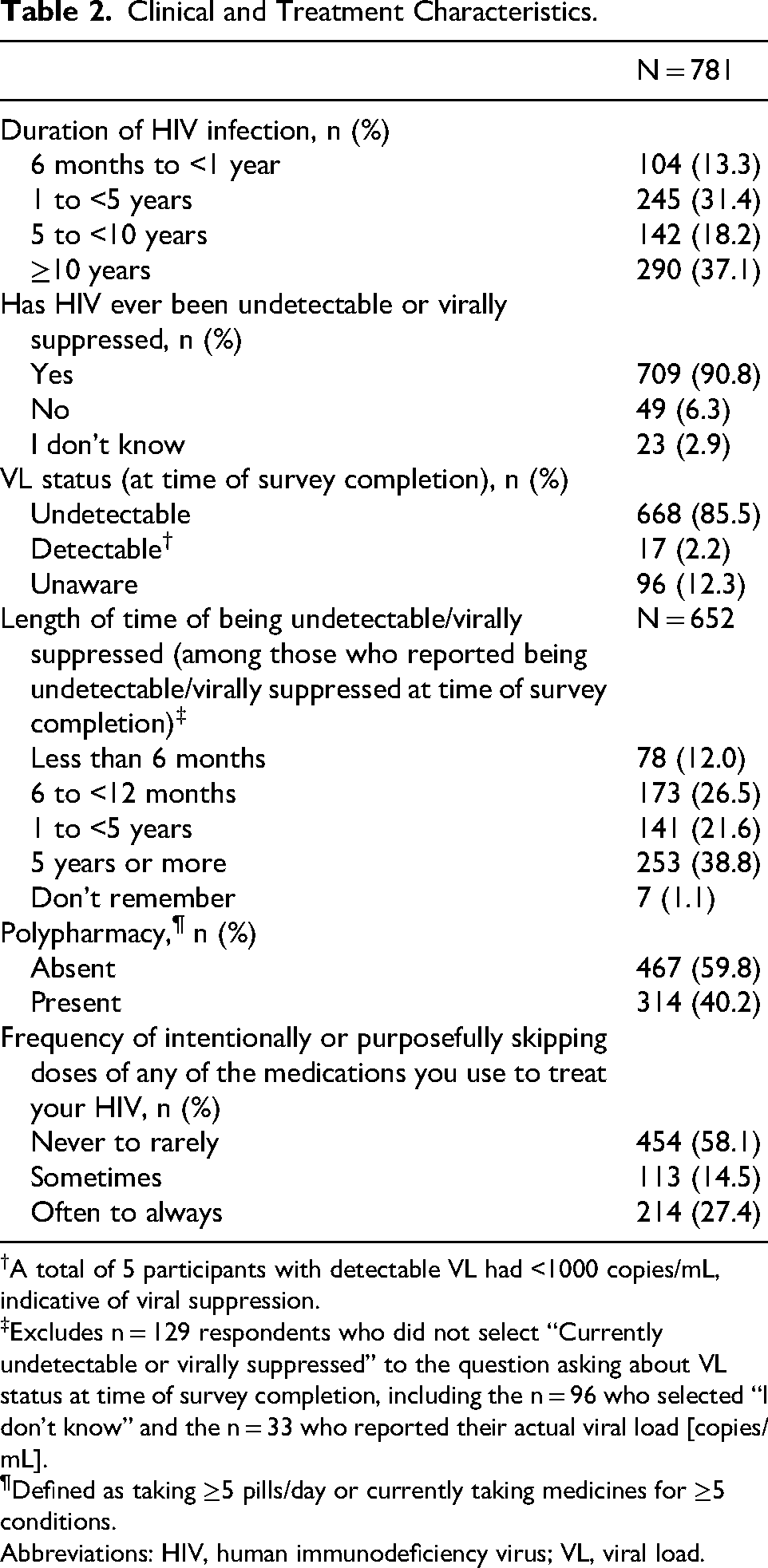
A total of 5 participants with detectable VL had <1000 copies/mL, indicative of viral suppression.
‡Excludes n = 129 respondents who did not select “Currently undetectable or virally suppressed” to the question asking about VL status at time of survey completion, including the n = 96 who selected “I don’t know” and the n = 33 who reported their actual viral load [copies/mL].
Defined as taking ≥5 pills/day or currently taking medicines for ≥5 conditions.
Abbreviations: HIV, human immunodeficiency virus; VL, viral load.
Knowledge and Understanding of U = U
Over half (54.5%) of participants had a lack of understanding of U = U, and 24 participants (3.1%) had never heard about the term U = U. For 50.4% of the participants, HCPs were the sole source of information regarding U = U, whereas 24.2% heard the message from sources other than HCPs or the U = U campaign. Over one-third of respondents (34.8%) did not learn about the meaning of ‘undetectable’ from a clinician, or other HCP. Among respondents who heard about the term ‘undetectable’, 27.9% reported that their HCP never informed them that they were undetectable, and 26.5% reported that their HCP never discussed what undetectable means to them. About 12.0% of respondents were unaware whether their VL was undetectable or suppressed (Table 3).
Understanding of U = U among PLHIV.

Selected any “wrong” response: ≥ 1 of the following: I am cured, I can have carefree sex, I can still pass HIV onto others, I was misdiagnosed with HIV and never had it to begin with, My immune system fought the disease and I no longer have HIV, or Not sure.
Selected I cannot transmit the virus sexually, I can’t pass HIV onto others, and/or I am virally suppressed without selecting any other categories.
Excludes n = 272 respondents who did not hear about ‘undetectable’ from a doctor, clinician, or HCP.
Abbreviations: HCP, healthcare provider; HIV, human immunodeficiency virus; PLHIV, people living with HIV; U = U, undetectable equals untransmittable.
Factors Associated with Lack of Understanding of U = U
In the bivariate analysis, PLHIV who lacked an understanding of U = U were less likely to report having switched their antiretroviral (ARV) regimens three or more times, and trust the information they received from their HCP compared to those with an understanding of U = U. Participants with lack of understanding of U = U were more likely to demonstrate suboptimal ART adherence, difficulty in verbalizing health concerns to an HCP and had heard about U = U from other sources (neither HCP nor U = U campaign) compared to those who had an understanding of U = U (Table 4). Of the participants lacking an understanding of U = U, 45.3% never heard about U = U from an HCP (Figure 2, Table 4) and 58.5% had suboptimal ART adherence (Figure 3, Table 4). About 69.0% of participants with detectable VL or who were unaware of their VL lacked understanding of U = U. Participants lacking knowledge and understanding of U = U compared to those having knowledge and understanding of U = U were less likely to be categorized as PAM level 4 (29.6% vs 37.7%) (Table 4). In other words, those lacking knowledge and understanding of U = U relative to those having knowledge and understanding of U = U tended to have lower PAM levels (70.4% vs 62.3% for levels 1 = 3).

Patient Source of Information About the Meaning of ‘Undetectable’.
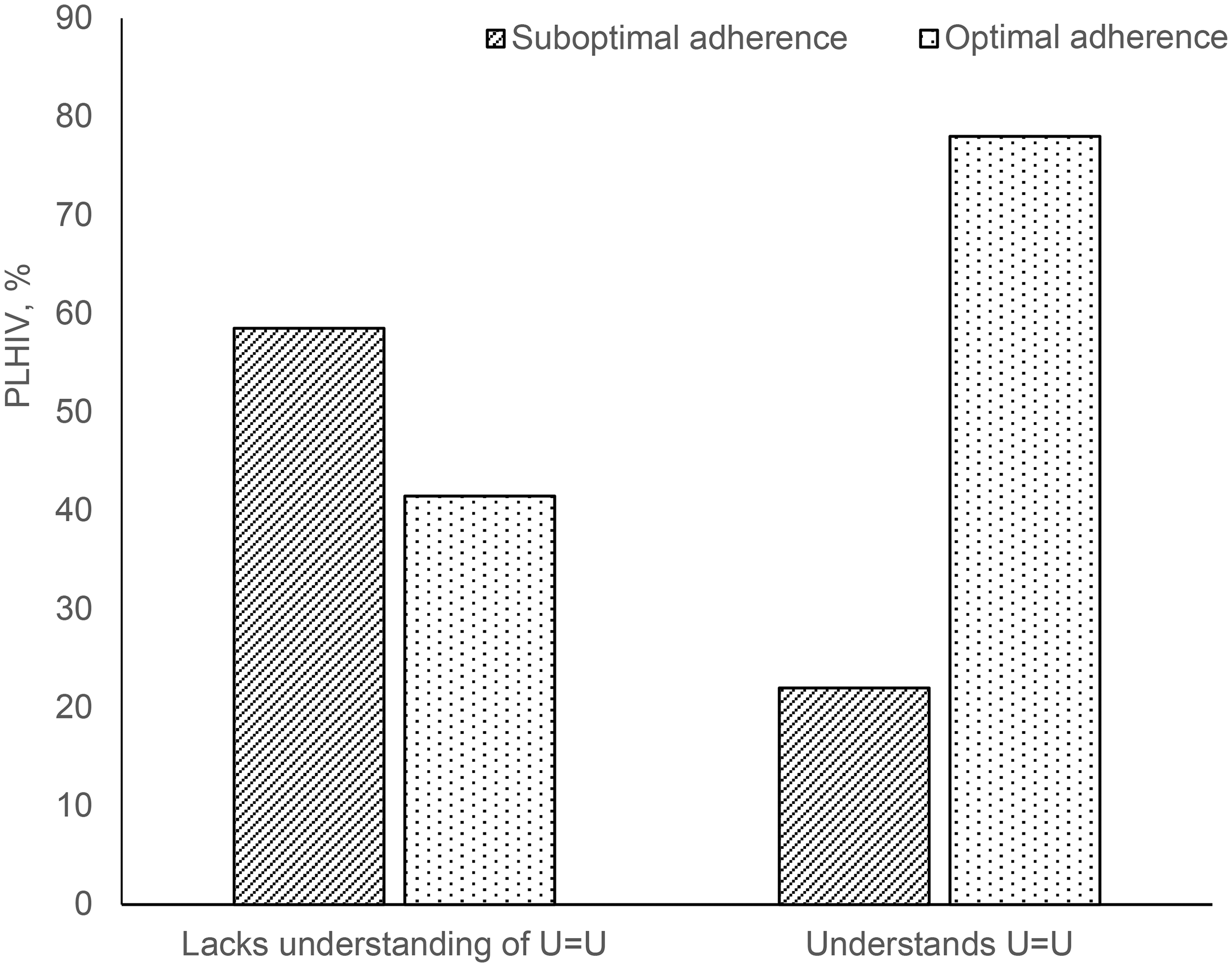
HIV Medication Adherence and Understanding of U = U.
Factors Associated with Lack of Understanding of U = U among PLHIV, N = 781.

Defined as: No = Knows that U = U (selected I cannot transmit the virus sexually, I cannot pass HIV onto others, and/or I am virally suppressed without selecting any other categories, excluding those who only selected “I am virally suppressed” (n = 327); Yes = Lack of understanding of U = U (selected at least one of the following: I am cured, I can have carefree sex, I can still pass HIV onto others, I was misdiagnosed with HIV and never had it to begin with, My immune system fought the disease and I no longer have HIV, or Not sure)†Defined as one or more non-HIV comorbidities.
No = rating of extremely easy, somewhat easy or neutral to all four of the health concern areas (general wellness, non-HIV-related illness, sexual health, and HIV health); Yes = rating of extremely difficult or somewhat difficult to at least one of the health concerns areas.
Excludes n = 272 respondents who did not hear about ‘undetectable’ from a doctor, clinician, or HCP (n = 79 who do not lack understanding of U = U and n = 193 who have lack of understanding of U = U).
No = excellent, very good, good (n = 535); Yes = fair or poor (n = 246).
Chi-square tests are used for calculating P-values for categorical variables and t-tests used for calculating P-values with continuous variables.
*Indicates statistical significance at P < 0.05.
Abbreviations: HCP, healthcare provider; HIV, human immunodeficiency virus; PAM, Patient Activation Measure; PLHIV, people living with HIV; SD, standard deviation; U = U, Undetectable equals Untransmittable.
In the adjusted analysis, factors associated with a lack of understanding of U = U among participants were sexual orientation (OR: 0.65, 95% CI: 0.43-0.97, P = 0.035), having a college degree or higher education (OR: 0.6, 95% CI: 0.41-0.86, P = 0.006), some college or associate degree versus college degree or higher), shorter HIV duration (OR: 2.06, 95% CI: 1.14-3.77, P = 0.018), suboptimal medication adherence (OR: 2.74, 95% CI: 1.88-4.01, P < 0.001), and lack of HCP to patient communication about the meaning and importance of achieving an undetectable VL (Figure 4). Specifically, the odds of lacking understanding of U = U were 1.54 times higher for participants who identified as heterosexual compared to those who identified as homosexual and 1.67 times greater among participants who had a college degree or higher compared to those with some college or an associate degree. The odds of lacking an understanding of U = U among participants with a relatively recent HIV diagnosis, between 6 and <12 months, were twice as those of participants diagnosed >5 years ago. Participants with suboptimal ART adherence were nearly three times (OR: 2.74, 95% CI: 1.88-4.01) more likely to lack an understanding of U = U than those with optimal adherence (Figure 4).

Multivariable Analysis Showing Factors Associated with a Lack of Understanding of U = U among PLHIV.
Discussion
Knowledge and understanding of U = U has critical importance for PLHIV, their sexual partners, and the public health community at large in the effort to eliminate sexual transmission of HIV. Particularly, understanding U = U plays a critical role in the prevention of sexual transmission of HIV to partners by encouraging PLHIV to achieve and maintain undetectable VL. Moreover, for PLHIV, understanding of U = U may empower them in achieving and maintaining optimal adherence to ART and destigmatize the treatment for HIV. This study assessed the knowledge and understanding of U = U and potential factors associated with lack of understanding of the U = U concept among PLHIV in the US.
In this study, more than half of the participants did not understand the meaning of the U = U message, and about 12% were not aware of their VL status, meaning that they did not know whether their VL was undetectable or virally suppressed. A survey of MSM conducted in Vancouver, Canada from 2012 through 2014 found that over two-thirds (69%) of participants living with HIV reported being aware of TasP. However, only 14% of these participants provided ‘complete’ TasP knowledge, identifying all three aspects of TasP, including use of ART, viral suppression, and prevention of HIV transmission).27,28 Moreover, prior cross-sectional surveys from the US reported that 70.0–96.0% of participants were aware of the U = U concept36-38; of which, less than 43% reported it as completely accurate 37 or trusted/believed it.36-38 The discrepancy in findings between studies could be attributed to differences in characteristics of study population (HIV status and sexual orientation) or the assessment methods used. Taken together, such data are suggestive of a high level of awareness but a suboptimal level of understanding of the U = U message in the US, which may also be attributable to the relatively recent adoption of the U = U message and campaign in the US relative to other countries and calls for initiatives to improve the overall understanding of U = U among PLHIV. This finding is particularly relevant in highlighting the role of U = U awareness, as a recent CDC study reported a decline in viral suppression in the US from 66% in 2021% to 65% in 2022.25,41
Additionally, nearly half of the participants heard about the meaning of undetectable from HCPs while one-fourth heard via sources other than HCPs or the U = U campaign. Moreover, over one-third (34.8%) of PLHIV reported that they had not heard about ‘undetectable’ from their clinicians or other HCPs. This indicates an inadequate information dissemination by HCPs and the gaps in patient-clinician communication regarding such an important element of ART initiation and maintenance. This may also be due to the knowledge gaps regarding U = U among HCPs, leading to ineffective communication or hesitancy and a low level of acceptability by HCPs, lack of appropriate resources catering to a PLHIV, or concerns related to other STIs.27,35 Moreover, HCPs acknowledged exercising caution while mentioning ‘zero risk’ to PLHIV. 35 To integrate the U = U message in clinical practice, several regional HIV societies/associations within the US have endorsed it in their public guidelines and communication. 42 For instance, recent guidance by the New York State Department of Health recommends sharing information about U = U with PLHIV regardless of their status of sexual activity, duration of the disease, and treatment journey. 43
Our results suggest a disconnect between educational attainment and comprehension or accessibility of HIV-related information. Individuals with a college degree or higher were more likely to lack an understanding of the U = U message, compared to those with some college or an associate degree, a result contrary to previous reports from the US 37 and other countries.32,33,43,44 The disparity in findings could be due to differences in population demographics such as those studied by Meanley et al which focused on younger men who have sex with men (YMSM; ages 18 = 25 years), where awareness and understanding of the U = U concept was higher. 37 Nevertheless, a multi-country study demonstrated that HCPs tend to provide information about U = U to PLHIV with lower education levels. 26 It is possible that HCPs are more proactive in sharing U = U information with individuals who have lower educational attainment, contributing to their relatively higher understanding of U = U noted in this study. Thus, educational strategies to increase awareness of U = U should not be overlooked among populations with higher education. It is possible that the messaging around U = U may not be reaching or resonating with individuals with higher education, or these individuals might not perceive the information as pertinent or reliable. There is a need for more focused, accessible, and clear dissemination strategies that resonate with specific educational backgrounds.
In the present study, we also found that PLHIV who identified as heterosexual had higher odds of lack of understanding of U = U compared to those identifying as gay, lesbian, or same gender loving. Although not directly comparable, this finding is in line with the Positive Perspectives study where awareness that HIV medications prevent HIV transmission was highest among men who have sex with men. 26
In the current study, a recent HIV diagnosis (6 months to <5 years vs >5 years) was associated with higher odds of lacking an understanding of the U = U message. This finding is particularly important because PLHIV who were recently diagnosed with HIV may need to be educated about the benefits of initiating ART and maintaining optimal ART adherence to achieve an undetectable VL and thus understand the benefit of U = U. Also, for PLHIV in the early years of HIV diagnosis, understanding of U = U may help them with destigmatization and improve retention in HIV care.
Moreover, PLHIV with lack of understanding of U = U were more likely to have suboptimal adherence. The relationship between understanding U = U and suboptimal adherence, however, can be bidirectional. Several previous studies have addressed the issues of suboptimal ART adherence in PLHIV. For instance, HIV-related stigma, commonly prevalent in PLHIV, is one of the contributing factors to low ART adherence. 43 In a few recent studies, enhancing the understanding of U = U has been demonstrated to mitigate HIV-related stigma,26,27 and therefore, can also effectively improve ART adherence among PLHIV. Our findings underscore the need to educate PLHIV who are recently diagnosed and those who have suboptimal ART adherence on the benefits of U = U and maintaining the undetectable VL throughout the course of treatment.
This study also noted a gap in patient-provider communication related to the HIV treatment goal of viral suppression and, ultimately, an undetectable VL. In our analysis, lack of HCP communication about the meaning of undetectable with PLHIV under their care was associated with a greater likelihood of lacking an understanding of U = U among PLHIV. In a survey from Canada, HCPs expressed that they may deprioritize these conversations and initiate them on a case-by-case basis. 35 In the positive perspectives study, more favorable health outcomes were reported by PLHIV who were informed about the U = U by their HCPs (vs those not informed by their HCPs). 26 Considering a higher receptiveness/level of trust shown by patients, 26 these observations underscore the crucial role of HCPs in disseminating information and proactively discussing the importance of achieving an undetectable VL with PLHIV.
Overall, our findings highlight the need for ongoing, targeted educational and interventional strategies that address barriers to understanding of U = U, particularly among PLHIV with different educational level and at varying stages of their HIV journey. Suboptimal HCP engagement around U = U translates into a missed opportunity to destigmatize HIV for PLHIV and their sexual partner(s), promote ART adherence to achieve an undetectable VL, and leverage the therapeutic and preventative benefits that ART can confer when taken as prescribed by an HCP.
This study has some limitations to be considered. First, as the data were self-reported, there is potential for social desirability bias and recall bias that may affect the accuracy of the reported data, and we were unable to verify the accuracy of the data through another data source, such as electronic health records or physician-supplied clinical data. Second, self-selection bias may also influence the results, with participants comfortable discussing their HIV status overrepresented and participants who may be uncomfortable discussing their gender or unsure how to answer the question on gender underrepresented. Third, the cross-sectional design of this study limits the ability to infer causality. Another limitation of the study is the relatively small sample size given that this was fielded across the US, which could limit the ability to generalize to the entire US HIV population. However, we were sufficiently powered (1-β = 0.80) to detect a statistically significant difference (two-tailed p < 0.05) between those with lack of understanding of U = U and those with understanding of U = U when there is a small effect size (Cohen's d = 0.20). In addition, this study likely underrepresents individuals without access to or comfort using the Internet, less healthy individuals, and individuals who are institutionalized, which may limit the generalizability to the entire HIV population. Further, the study participants were found to have high patient activation levels, which also may limit the generalizability to the whole HIV population.
Conclusion
The study highlights substantial gaps in understanding of the U = U message among PLHIV and the HCP-patient communication about U = U. These findings emphasize the need for tailored educational and interventional strategies aimed at both PLHIV and HCPs, focusing on the clinical evidence and benefits of U = U in HIV prevention strategies.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251370236 - Supplemental material for Lack of Knowledge and Understanding of Undetectable Equals Untransmittable (U = U) Among People Living with HIV in the United States: Results from a Cross-Sectional Survey
Supplemental material, sj-docx-1-jia-10.1177_23259582251370236 for Lack of Knowledge and Understanding of Undetectable Equals Untransmittable (U = U) Among People Living with HIV in the United States: Results from a Cross-Sectional Survey by Bekana K Tadese, M Janelle Cambron-Mellott, Jean Marie Arduino, Bridget L Balkaran, Shakiba Eslamimehr and José M Zuniga in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-docx-2-jia-10.1177_23259582251370236 - Supplemental material for Lack of Knowledge and Understanding of Undetectable Equals Untransmittable (U = U) Among People Living with HIV in the United States: Results from a Cross-Sectional Survey
Supplemental material, sj-docx-2-jia-10.1177_23259582251370236 for Lack of Knowledge and Understanding of Undetectable Equals Untransmittable (U = U) Among People Living with HIV in the United States: Results from a Cross-Sectional Survey by Bekana K Tadese, M Janelle Cambron-Mellott, Jean Marie Arduino, Bridget L Balkaran, Shakiba Eslamimehr and José M Zuniga in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Supplemental Material
sj-pdf-3-jia-10.1177_23259582251370236 - Supplemental material for Lack of Knowledge and Understanding of Undetectable Equals Untransmittable (U = U) Among People Living with HIV in the United States: Results from a Cross-Sectional Survey
Supplemental material, sj-pdf-3-jia-10.1177_23259582251370236 for Lack of Knowledge and Understanding of Undetectable Equals Untransmittable (U = U) Among People Living with HIV in the United States: Results from a Cross-Sectional Survey by Bekana K Tadese, M Janelle Cambron-Mellott, Jean Marie Arduino, Bridget L Balkaran, Shakiba Eslamimehr and José M Zuniga in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
The authors acknowledge Bryan Ricker and Kristin Falbo, MS, formerly of Oracle Life Sciences, Oracle Corporation, USA (formerly known as Cerner Enviza, USA), for their contributions to study design, execution and project management and the medical writing support provided by Silki, PhD and Ashwini Atre, PhD, of Indegene Ltd Bangalore, India.
Ethical Approval Statement
The study protocol and amendments were reviewed by an Institutional Review Board (Pearl IRB, Indianapolis, IN) (IRB #21-KANT-269) and received an exemption under FDA 21 CFR 56.104 and DHHS 45 CFR 46.104(b)(2): (2) Tests, Surveys, Interviews regulations.
Patient Consent Statement
All patients who participated in this study provided written informed consent electronically prior to accessing the survey.
Author Contributions
JMA, MJCM, BLB, and JMZ were involved with the conception of the study, study design, and development of protocol and survey; BLB and MJCM were involved with conducting statistical analyses; JMA, BKT, MJCM, JMZ, and SE were involved in development of study protocol amendments, reviewing and interpreting study results; MJCM, SE, BKT, JMA, and JMZ were involved with either drafting of the manuscript and/or providing critical revisions to finalize the manuscript. All authors have reviewed the final manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.J. Cambron-Mellott is an employee of, and B.L. Balkaran, and S. Eslamimehr are former employees of Oracle Life Sciences, Oracle Corporation, which received funding from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., NJ, USA, to conduct and report on the study. M.J. Cambron-Mellott and B.L. Balkaran own stock in Oracle Corporation. José M. Zuniga received consulting fee from Gilead Sciences (Advisory Board) and Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA (research study). Bekana K. Tadese and Jean Marie Arduino are employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. Jean Marie Arduino owns stock in Merck & Co., Inc., Rahway, NJ, USA.
Data Availability Statement
The data presented including the methodology are the intellectual property of Oracle Life Sciences and will not be shared without reasonable request. Results of this study in part were presented at the 25th International AIDS Conference, July 2024, Munich, Germany.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.