
Abstract
Background
This study assessed the acceptability, among caregivers, of a mental health chatbot designed for adolescents living with HIV aged 10 to 19 years.
Methods
Fifteen caregivers interacted with the mental health chatbot. Pre–post assessments and semistructured interviews evaluated acceptability. Data were analyzed using a Framework Analysis approach.
Results
Caregivers aged 31 to 70 years found the chatbot acceptable on individual, interpersonal, and environmental levels. They appreciated the educational content and self-help tools, feeling the chatbot would benefit them personally. Caregivers also saw potential in the chatbot to improve communication with their children, particularly during critical periods like HIV diagnosis. Despite concerns about data costs or internet access, most viewed the chatbot as an accessible supplement to traditional mental health services.
Conclusion
This study suggests that a mental health chatbot for Peruvian adolescents living with HIV was acceptable to their caregivers, potentially benefiting caregivers’ mental health, enhancing caregiver–adolescent interactions, and fostering better communication.
Introduction
Mental health conditions, especially depression and anxiety, are a significant concern among adolescents living with HIV (ALWH), who already face unique psychosocial stressors stemming from HIV-associated stigma, the complexities of lifelong treatment adherence, fears of HIV disclosure, and the emotional burden of navigating social relationships while managing their health. 1 In low- and middle-income countries (LMICs) like Peru, these challenges are exacerbated by the limited access to mental health services, making it even more difficult for ALWH to receive the support they need to maintain their well-being and adhere to their HIV treatment regimens.2,3
Given these challenges, caregivers play a critical role in supporting ALWH, significantly influencing their children's mental health outcomes through emotional and practical care. 4 In environments where stigma and limited healthcare infrastructure hinder access to care, caregivers often act as gatekeepers to health resources. 5 Notably, many caregivers also live with HIV, providing them with unique, first-hand insights into managing the disease. 6 However, this dual role often introduces additional challenges, such as managing their own health, that must be factored into caregiving strategies. 7 Therefore, it is important to consider the needs and perspectives of caregivers when developing mental health interventions for ALWH, as their acceptance and support can significantly influence the success and sustainability of these interventions. 8
Digital health tools such as chatbots have emerged as promising solutions to provide scalable and accessible mental health support. 9 However, despite the growing use of these interventions, research has largely focused on the direct users—adolescents—while overlooking the critical role that caregivers play in the overall effectiveness of such tools. 10 Little is known about how caregivers perceive digital mental health interventions, especially in terms of their usability, emotional impact, and perceived effectiveness. Understanding how caregivers perceive these digital interventions is crucial for ensuring that these tools are successfully adopted and utilized by ALWH.
This study aimed to address this gap by providing a qualitative exploration of caregivers’ perceptions of a mental health chatbot designed for adolescents. Specifically, the primary objective of this study was to explore the acceptability of the chatbot among caregivers of ALWH, focusing on its potential for use with their adolescents. This aim was addressed through surveys and interviews evaluating 6 dimensions of acceptability: affective attitude (caregivers’ emotional responses to the chatbot), ethics (perceived fairness and respectfulness of the tool), barriers (practical or situational challenges to use), adoption (willingness to engage with the chatbot), perceived effectiveness (belief in the tool's ability to provide support), and self-efficacy (confidence in their ability to use the chatbot effectively). By addressing this objective, this study provides a comprehensive understanding of how caregivers perceive a digital mental health intervention and its potential to support their ALWH.
Methods
Participants and Procedures
This was a qualitative study nested within another study examining the acceptability of a mental health chatbot named E.V.A. (Educación, Vinculación, y Autoayuda) among adolescents with HIV in Lima, Peru, detailed elsewhere. 11 E.V.A. consisted of 3 modules—education, self-help skills, and linkage to care—with language, images, and content tailored specifically for adolescents (Figure 1). Educational content focused on mental health conditions prevalent in adolescents, such as depression, anxiety, and eating disorders. Self-help skills focused on managing emotions, breathing exercises, and a game to unlearn common misconceptions about mental health and HIV. Linkage to care included contact with a mental health professional and an emergency contact list. The present study assessed the acceptability of E.V.A. among caregivers of adolescents with HIV.

Images from an interaction with E.V.A., a chatbot designed to provide mental health education, self-help, and linkage to care for adolescents living with HIV in Peru. Images show the introductory page for E.V.A. and a few of the content options EVA offers related to mental health.
Caregivers were eligible for study participation if they were a parent, family member, or other legal guardian aged 18 years or older providing care to an ALWH aged 10 to 19 years. All participants were recruited directly, in person or by phone, from the sample of caregivers whose adolescents participated in the larger study. 11
Prior to face-to-face and virtual interviews, participants were informed about the study's purpose and asked to provide written informed consent. Interviews were conducted in Spanish by NR, a U.S.-based male medical student. DV, a Peruvian male psychologist and study professional, was present to assist in the interview. NR began the interviews by administering the sociodemographic survey, which collected data on age, sex, level of education, occupation, and route of HIV transmission for the ALWH.
Next, the adolescent depression knowledge questionnaire (ADKQ) was administered to caregivers. The ADKQ, originally developed to assess depression literacy among adolescents, was selected for this study due to its straightforward language, making it accessible to adults with varying educational backgrounds. Although this study does not compare scores between adolescents and caregivers due to sample size limitations, using the same instrument as the main chatbot study provided a shared framework for evaluating depression knowledge across different user groups. 11 The ADKQ has demonstrated acceptable internal consistency in adolescent populations, and it has been shown to effectively measure changes in depression knowledge following educational interventions.12,13 While its psychometric properties have been primarily validated in adolescent populations, its use with caregivers in this study was exploratory, aiming to assess their baseline understanding of depression and the potential educational impact of the chatbot.
Participants were then given 20 min to interact with the introductory educational parts of E.V.A. on their own. After 20 min, participants explored the 3 key modules of E.V.A.—education, self-help, and linkage to care—with guided assistance from NR (Image 1). Once the 3 modules were explored, NR administered the ADKQ again. Finally, using a semistructured interview guide (Table 1) informed by a theoretical framework of healthcare intervention acceptability,14–16 the interviews commenced covering 6 core domains of chatbot acceptability: affective attitude, ethics, barriers, adoption, perceived effectiveness, and self-efficacy (Figure 2). The psychologist present provided emotional support at necessary times of the interview if participants were in emotional distress, and participants were provided with information about local mental health resources to ensure ongoing support if desired. All interviews were digitally recorded for later analysis. Overall time for participation in the study was between 2 and 3 hr, conducted as a single session. Recruitment of participants began in April of 2024 and interviews were completed by June of 2024.

Social-ecological model of the acceptability of a mental health chatbot among caregivers of adolescents living with HIV.
Semistructured Interview Guide for Interviews with Caregivers of Adolescents Living With HIV to Assess the Acceptability of a Mental Health Chatbot.
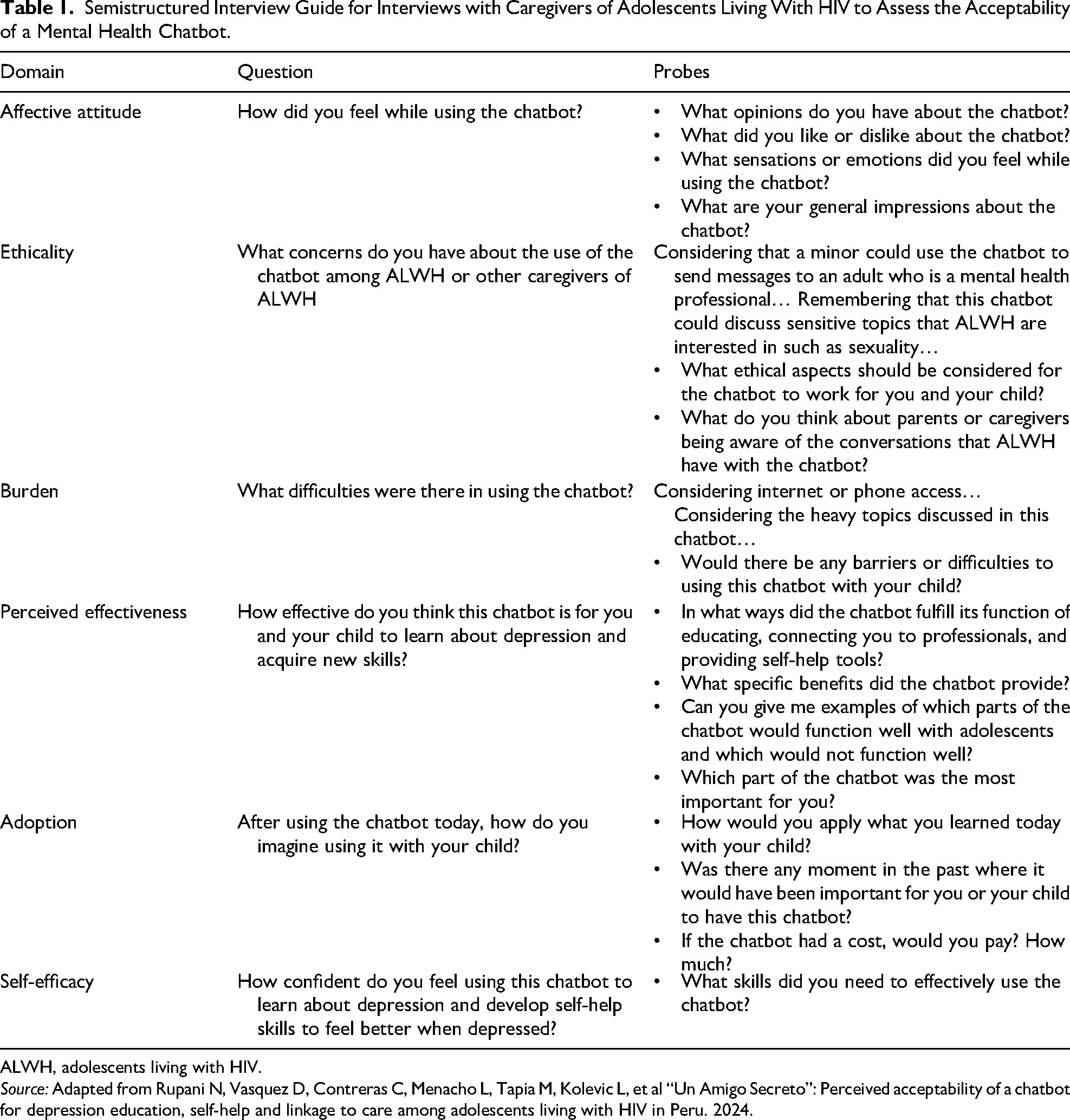
ALWH, adolescents living with HIV.
Source: Adapted from Rupani N, Vasquez D, Contreras C, Menacho L, Tapia M, Kolevic L, et al “Un Amigo Secreto”: Perceived acceptability of a chatbot for depression education, self-help and linkage to care among adolescents living with HIV in Peru. 2024.
Data Analysis
Interview recordings, supplemented by note-taking, were transcribed verbatim and loaded into Dedoose qualitative analysis software for coding and analysis. 17 Initial transcriptions were performed using Happy Scribe software 18 ; all transcripts were checked for accuracy by DV before analysis. Using an initial codebook populated with a priori codes based on the 6 acceptability domains, NR and DV coded the interviews in Spanish using the Framework Analysis approach 19 guided by an adapted version of Sekhon's theoretical framework of healthcare intervention acceptability,14,15 and de novo codes were added as needed (Figure 2). All transcripts were independently and iteratively coded, and NR and DV met to resolve discrepancies and discuss data saturation. After all transcripts were initially coded, tables were created, which compiled all text segments for each code, and a second analysis was conducted to detect the overarching themes within each acceptability domain. The themes were then integrated within a socioecological model, allowing for an examination of caregivers’ perceptions of chatbot acceptability across individual, interpersonal, and environmental levels. Finally, the overarching themes were reported using illustrative quotes that were translated to English by NR and verified by a bilingual, native Spanish speaker DV. To ensure the rigor of the data and enhance the clarity of reporting, the Consolidated Criteria for Reporting Qualitative Research checklist was completed (Supplemental Material S1).
Statistical Analysis
For comparisons of ADKQ scores before and after using the chatbot, Wilcoxon signed-rank test was planned for nonparametric data.
Results
Twenty-eight caregivers were approached for an interview, and fifteen caregivers agreed to participate in an interview. Six caregivers were taking care of ALWH between 10 and 14 years of age, and 9 caregivers were taking care of ALWH between 15 and 19 years of age; see Table 2. All participants completed the ADKQ before and after using the chatbot. Twelve interviews were conducted in person, and 3 interviews were conducted virtually. The median total score increased from 7 out of 14 to 9 out of 14 on the ADKQ; however, due to the small sample size, tests for significance were not possible.
Characteristics of Caregivers Participating in In-Depth Interviews (N = 15).

ALWH, adolescents living with HIV.
The top themes from the qualitative analysis are mapped on a social-ecological model with 3 levels: individual, interpersonal, and environmental (Figure 2). Themes for each level are presented below with illustrative quotes. Quote attributes present caregiver relationship to ALWH, age of caregiver, age of adolescent, and route of HIV acquisition (perinatal, ie, during birth or breastfeeding; blood transfusion; or sexual) for the adolescent under care. Interviews lasted 14 to 30 min in duration.
Individual Level
Affective Attitude: Caregivers Felt a Range of Positive and Negative Emotions While Using E.V.A
Many caregivers expressed positive feelings while using E.V.A. and highlighted E.V.A.'s ability to provide comfort and a sense of security. (E.V.A.) had precision in addressing the doubts I had about (depression), and then (E.V.A. gave) recommendations. So, you feel secure, like someone is paying attention to you, listening to you, and guiding you. (Mother, 47; Adolescent [19], perinatal)
This sentiment of reassurance was echoed by another participant who felt understood and supported by E.V.A.'s insights, stating, “(E.V.A.) informs us about anxiety, which made me feel like someone else understood me (…) and if I had had that kind of psychological support, it would have been easier for me” (Mother, 48; Adolescent [14], perinatal).
In contrast, some caregivers experienced mixed emotions, with E.V.A. prompting reflections on past challenges and mistakes, leading to feelings of sadness or guilt. One mother described this duality: Well, for a moment (while using E.V.A.), I was fine (…) learning how to manage to treat my daughters. But there were some moments when I also felt a bit sad because it's not always about scolding my daughters, like (E.V.A.) mentioned (…) I did feel a bit, on one hand, sad, on the other hand, happy because I was informing myself more. (Mother, 41; Adolescent [12], perinatal)
This theme of mixed emotions was recurrent, as other caregivers also highlighted discomfort stemming from reflecting on unresolved issues or traumatic experiences. For instance, some noted that engaging with the chatbot brought memories of past emotional struggles to the surface, which they had not fully processed. Additionally, a few caregivers reported discomfort when discussing emotions with E.V.A. (This chatbot) is something new for me (…) sometimes the questions cause you a bit of sadness, a bit of panic or fear about answering. Sometimes you think: ‘Should I be honest or pretend to be okay?’ (…) Sometimes (I felt) discomfort (…) because not all of us react the same way when it comes to saying what we have or what we feel. Sometimes, we don't know how to express it. (Grandmother, 62; Adolescent [13], blood)
Perceived Effectiveness: Caregivers’ Belief That E.V.A. Would Be Useful for Themselves
Many caregivers believed E.V.A. would be useful for themselves, citing its educational value and ease of use. Yes, (E.V.A.) helps me a lot. For example, if I had been taught or had something like this (when I was an adolescent), it would have been easier. Now, with things like E.V.A., it helps, it informs you a lot, and it's very easy to understand (…) There are videos, drawings, it explains very well, it asks you questions, and helps us understand better. (Mother, 48; Adolescent [14], perinatal)
E.V.A.'s guided breathing exercises were especially perceived as effective, with caregivers finding them calming and helpful in managing emotions: The breathing exercise to control emotions is also a good tool. Sometimes we feel bad, and doing that exercise helps us a lot to calm down a bit (…) to release everything we have inside, which could be sorrow, sadness, or worry, I don't know, or just the need to scream sometimes, and doing the breathing exercise made me feel calmer. (Mother, 47; Adolescent [19], perinatal)
Some caregivers mentioned that E.V.A. would have been effective for themselves at various points in their lives. When I was in my adolescence, (this chatbot) would have been very helpful, or when my daughter was 4 years old, or when I was alone as well. Because after the death of my son's mother, I was attacked by depression. (Father, 42; Adolescent [14], perinatal)
Self-efficacy: Caregivers Expressed Both Confidence and Doubt in Their Abilities to Use E.V.A.
When asked about their confidence in using E.V.A., most caregivers expressed that they felt they would be able to use E.V.A. on their own. (E.V.A.) is quite clear, and even though, because of my age, I'm not as tech-savvy as children, I found it to be quite explicit, and I didn't need to ask for explanations. (Mother, 37; Adolescent [14], blood)
After interacting with E.V.A., a few caregivers expressed doubt about their technological skills or expressed difficulty in using E.V.A. on their own. One caregiver gave a specific example: Well, for me, it's typing [to E.V.A.] that's a bit difficult for me. (Mother, 44; Adolescent [19], perinatal)
Similarly, other participants mentioned that navigation within the chatbot was not intuitive for those unfamiliar with smartphones, highlighting a potential accessibility gap for less tech-savvy users.
Interpersonal Level
Adoption: Caregivers Described Situational Usage of E.V.A. and Applying Knowledge From E.V.A. With ALWH
Caregivers described various scenarios where E.V.A. could be instrumental, with many particularly mentioning the critical period of their child's HIV diagnosis. When the diagnosis was revealed, (E.V.A.) would have helped a lot. I believe that for all adolescents, this tool would be very helpful in the revelation of the diagnosis. I think professional help is definitely important, to prepare the child to receive the diagnosis and to take away that fear and anxiety they have. Even now, some kids still experience this. (Mother, 47; Adolescent [19], perinatal)
Additionally, several caregivers expressed a desire to use E.V.A. alongside their children, turning it into a shared activity. Well, actually, I would like both him and me to participate in the (chatbot), perhaps using it on the days when he is free after school, in the afternoons, and together, we could engage in an activity using the application. (Mother, 31; Adolescent [15], sexual)
Caregivers also discussed how they would incorporate the insights gained from E.V.A. into their daily interactions with their children. Interviewer: How would you apply what you learned today from this application with your daughter? Participant: From what I've seen (in E.V.A.), I need to have a bit more patience, talk with (my children), and be more tolerant. A lot of changes (…) It's like I've been in a whirlwind, but I also have to learn from this to calm down a bit. (Mother, 41; Adolescent [12], perinatal)
Another father planned to integrate physical activities suggested by E.V.A. into their routine: Sometimes we can't understand or (pay attention to our kids) properly. So, I'm interested because now I'm also going to use my phone and look at (E.V.A.). Because I saw in the module that one cure (for depression) can be physical activity … so I'll go running with (my kids). We'll do sports together, I tell them. (Father, 45; Adolescent [15], perinatal)
Perceived Effectiveness: Caregivers’ Beliefs That E.V.A. Would Be Useful for Their ALWH
Caregivers affirmed E.V.A.'s effectiveness, particularly its educational, self-help, and linkage-to-care features tailored for ALWH. They appreciated E.V.A.'s ability to facilitate communication with professionals, providing a trusted space for their children to ask questions and express concerns. The part where they can talk to a professional is excellent because they often hold back from asking us, the parents, or at the hospital many things. So, perhaps with the application on their phone, they feel more comfortable through the screen, there's more trust, and they would feel more at ease to vent and ask deeper questions that they might not ask us, the parents. (Mother, 37; Adolescent [14], blood)
The guided breathing exercises were highlighted as a particularly valuable feature, with one mother stating, “That breathing exercise (…) it would be great if this were always available because it's really helpful for people who suffer from depression and anxiety” (Mother, 52; Adolescent [19], perinatal).
Barriers: Caregivers’ Social Challenges to Using E.V.A. With ALWH
When exploring potential difficulties in using E.V.A. with their children, some caregivers highlighted challenges stemming from their relationship dynamics and the sensitive nature of the topics discussed. Yes, there could be (challenges) for a teenager. Sometimes they don't communicate well with their dad (…) it has happened to me with my son (…)” (Mother, 52; Adolescent [19], perinatal)
A few others explained that generational gaps or cultural norms discouraged open conversations about mental health within families. Most caregivers felt there were no significant social barriers and expressed confidence in their ability to engage with their children and E.V.A. openly: Interviewer: What difficulties would there be for you to use E.V.A. with your son? Participant: None, really (…) I would be with him, helping him (with E.V.A.), supporting him, explaining that it's okay. Later on, if he's with me and wants to see (parts of E.V.A.) like (content on) anxiety, behavior. I'll help him with that. Because informing him about these things will help him. (Mother, 48; Adolescent [14], perinatal)
Ethicality: Caregivers’ Concerns About Topics Discussed in E.V.A., Parental Supervision, and Privacy for ALWH
Caregivers were also asked about the potential inclusion of sexual education content in E.V.A. Some caregivers described the need for sensitive framing of such topics to avoid causing distress. Other caregivers specifically expressed concerns about sexual health content being a trigger of past traumatic events to ALWH. Well, if teenagers who have been victims of rape are told about sexuality, they might sink into deeper depression if they haven’t finished their psychological treatment. For example, in the case of my nieces and daughter, when I try to talk to them, I tell them (about) avoiding sexual infections, avoiding unwanted pregnancies. I talk to them, but they feel uncomfortable because of the trauma they have experienced. (Aunt, 32; Adolescent [16], sexual)
On the other hand, many caregivers recognized the critical role of sexual education for ALWH. I think that all information about sexuality is of utmost importance for teenagers. I believe it's very important that talking about sexuality is not bad nowadays. It's good to educate them for their self-care and to care for others. (Mother, 47; Adolescent [19], perinatal)
Concerns about adolescents using E.V.A. without supervision were also prevalent. Some caregivers worried that ALWH might misinterpret the information without guidance. Sometimes teenagers cannot quickly grasp when they have (HIV). Sometimes, they also cannot understand what (HIV) means. And that is why a guardian should be by their side to explain what those things mean. (Father, 42; Adolescent [14], perinatal)
Some parents also had concerns about the privacy of information in E.V.A., and who the interactions would be shared with. I have always been aware of what she writes or who she is chatting with. I have always been concerned … Let's say that now she enters this chatbot and talks to a specialist like you, that's fine. But if (the chatbot has) an adult whom I don't know and who doesn't inform me who they are, then I have no reason to let her enter and talk to that person. (Grandmother, 62; Adolescent [13], blood)
Conversely, some caregivers trusted their children to use E.V.A. independently. Honestly, it doesn't give me any distrust or anxiety because if (my daughter) sees something that is out of place, she will tell me because she is a very sharp girl. It is a very instructive application … she won't be talking to strangers or people who are not qualified, and it also comes from the hospital. It is not just any application where she will be talking to unknown people or those who will instruct her in bad things. (Mother, 37; Adolescent [14], blood)
Self-Efficacy: Caregivers’ Confidence in ALWH's Ability to Use E.V.A. on Their Own
Many caregivers expressed confidence in their children's ability to use E.V.A. on their own. A caregiver noted, “There are many kids who use (things like E.V.A. on their own) more than we do” (Uncle, 70; Adolescent [16], perinatal). This sentiment was echoed by several caregivers who felt that their children's familiarity with technology would facilitate their use of E.V.A.
Additionally, some caregivers highlighted their willingness to learn from their children and rely on their assistance when using E.V.A. (I would be confident) if (my granddaughter) teaches me and then I start to learn (E.V.A.) … that's how we did it at home … because I don't know how to handle it on my own.” (Grandmother, 61; Adolescent [15], perinatal)
Environmental Level
Adoption: Monetary Value Caregivers Placed on E.V.A.
To obtain an estimate of the economic value of E.V.A., caregivers were asked if and how much they would pay for it. Most caregivers indicated they would be willing to pay for E.V.A., with suggested one-time amounts ranging from 20 to 300 Peruvian soles (USD 5-80). A caregiver at a shelter stated, “I’m being very honest, 200 Soles, between 200 (USD 53) and 300 Soles (USD 80)” (Caregiver at shelter, 65; Adolescent [15], unknown). Another mentioned, “Maybe 20, 30 Soles (USD 5, USD 8)” (Uncle, 70; Adolescent [16], perinatal).
Barriers: Material Barriers Caregivers Perceived to Accessing E.V.A.
Some caregivers discussed material barriers, such as access to a phone and internet, as potential difficulties for ALWH using E.V.A. Most people don't have cell phones, so there's no way (to use E.V.A.). (Mother, 51; Adolescent [18], perinatal) Well, the internet is expensive. So, the problem is that some families don't have it. They would like to have (E.V.A.), but if you don't have internet … (you can’t). (Uncle, 70; Adolescent [16], perinatal)
Other caregivers felt there were no significant material barriers and suggested that E.V.A. could even reduce barriers to care. It could be useful for many teenagers and young people because, to seek a psychologist, economic resources are needed. And (E.V.A.) could be (more) manageable for those teenagers who can access it. (Mother, 31; Adolescent [15], sexual)
Discussion
Our study revealed that caregivers of ALWH found the E.V.A. chatbot designed to improve depression education, self-help, and linkage to care for ALWH to be acceptable across various domains and levels. This acceptability spanned individual benefits, interpersonal dynamics with their ALWH, and material considerations, indicating a broad potential for the chatbot's application in improving mental health for not only ALWH but also their caregivers.
At the individual level, caregivers found E.V.A. beneficial for learning about depression and their own emotional processing. E.V.A. provided a sense of security and support, particularly through features like guided breathing exercises and educational content. These features helped caregivers learn about managing their emotions and feel reassured, comforted, and heard. Caregivers also provided examples of what they learned from E.V.A. after one use, suggesting preliminary evidence that the education function of E.V.A. may have been effective for caregivers. Many also expressed that they would have benefited from such a tool during their adolescence and even in their current lives, reflecting on challenging times. Interestingly, the fact that caregivers voluntarily shared these challenges without being directly asked about their own mental health highlights the significance of this issue. Understanding caregivers’ mental health, including their help-seeking behaviors and prior access to support, warrants further exploration in future studies. A study by Webster et al (2019) showed that impaired caregiver mental health adversely affects their child's quality of life, a deficit that is exacerbated in children with HIV. 20 Conversely, positive caregiver mental health can improve adolescent quality of life by enhancing caregiver engagement in shared activities, responsiveness to their children's needs, and effective emotional regulation within the family. 4 Therefore, supporting the mental health of ALWH necessitates supporting the mental health of their caregivers. Other studies support the use of chatbots by caregivers by showing that digital mental health interventions can be used to improve caregiver emotional understanding, coping, and regulation. 21
Caregivers also found E.V.A. acceptable for use by and with their ALWH. Caregivers expressed a desire to use E.V.A. alongside their children, creating shared moments that enhance communication through which the caregiver and their ALWH can learn from each other, and they both can learn from E.V.A. They mentioned they would integrate insights from E.V.A., such as increased patience and tolerance, into daily interactions with their ALWH, serving as a model for their children. The use of E.V.A. by caregivers alongside their ALWH is supported by studies showing that caregiver participation in their child's mental health treatment leads to improvements in the child's emotional processing and mental health symptoms. 22 At the same time, caregivers were also confident in their children's ability to use E.V.A. independently due to their familiarity with technology. They noted E.V.A.'s effectiveness in facilitating communication with professionals, its ease of understanding, and the trusted space it provides for children to ask questions. This finding is consistent with the perceived effectiveness of E.V.A. prior to its design and studies showing that digital interventions are acceptable for adolescents, catering to their preferences and level of understanding.15,23,24
Importantly, many caregivers noted that E.V.A. would have been particularly beneficial during the critical period of their child's HIV diagnosis, providing professional help to alleviate their child's fear and anxiety. This showed that caregivers could envision scenarios in which E.V.A. would be useful for their adolescents, highlighting its potential adoption. Moreover, this supports further testing of digital interventions at the point of care to improve linkage to mental health support when adolescents are initially diagnosed. 25 This aligns with the broader movement to integrate mental health services into healthcare platforms, including HIV care, to enhance access to mental health support for ALWH.26,27
Caregivers identified communication barriers and the sensitivity of topics as challenges in using E.V.A. with their ALWH. Discussing mental health with children can bring up feelings such as guilt or shame for caregivers that are uncomfortable to deal with in the presence of their children. 28 Despite these concerns, most felt confident in communicating with their ALWH while using E.V.A., believing it would foster open discussions and provide valuable support. Ethical concerns about sexual education content and privacy were also raised, reflecting worries about triggering trauma and misinterpretation of information. These findings are consistent with literature highlighting the need for careful content curation and safety of digital interventions for vulnerable populations.29,30 At the same time, many caregivers acknowledged the critical role of sexual education for ALWH, emphasizing its importance for self-care and prevention, which is supported by research advocating comprehensive sexual education for ALWH. 31 To incorporate these sensitive educational topics safely, a chatbot should include warnings for potentially triggering information and allow users to customize what information they would like to see early on during their interactions with the chatbot. 32 Caregivers could play a crucial role in screening or preapproving content, ensuring that the chatbot provides information appropriate to the adolescent's age and specific circumstances. Customization should not only be based on user preferences but also consider demographic factors such as age and route of transmission to tailor the content effectively.
Given the critical role of caregivers in adolescent mental health, interventions like E.V.A. should actively integrate caregiver-focused components. This includes clear tutorials at the beginning of digital interventions to improve caregivers’ technological proficiency and their confidence in using digital tools to support their adolescents’ mental health. For example, digital parenting interventions delivered through accessible platforms like WhatsApp have successfully improved caregiver engagement and responsiveness in low-resource settings. 33 Structured modules focusing on building communication skills and addressing sensitive topics, such as emotional health and sexuality, could further empower caregivers to foster open and supportive discussions within families, which is a key determinant of adolescent well-being. 34 Policy frameworks can add initiatives for caregiver-inclusive digital health programs to ensure the scalability and sustainability of these interventions in low-resource settings, as caregiver mental health is synergistic with that of their adolescents.
While E.V.A. did not directly include artificial intelligence (AI), the use of AI in chatbots and specifically for mental health is rapidly emerging, bringing with it both opportunities and risks. Generative AI may assist in mental health interventions by providing a more personalized experience for users. 35 Additionally, chatbots can use AI to detect signs of self-harm, suicidal ideation, patterns of depression, or other crises, prompting immediate connections to human counselors or crisis services when necessary. 36 These measures would align with “doing no harm” and move the chatbot toward providing more supportive and secure interactions for all users. 37 However, there are risks to using generative AI in mental health interventions, such as AI systems inadvertently perpetuating biases present in their training data and the inability of AI to provide human empathy and understanding during crises.38,39 These risks can be mitigated by clearly setting boundaries for what generative AI can do in a mental health intervention, ensuring users understand the limits of generative AI, and keeping human interactions as an option.40,41 A future version of E.V.A. may benefit from incorporating AI to screen for high-risk users and create more personalized dialog.
Most caregivers indicated they would be willing to pay for E.V.A., suggesting that it has tangible value to those from a spectrum of financial backgrounds. The willingness to pay ranged significantly, with some caregivers insisting repeatedly and surprisingly that they would pay amounts as high as $80 USD due to their personal need for support after trauma. However, material barriers such as access to phones and the internet were noted as potential challenges for ALWH. Reviews have highlighted access and costs of materials for digital mental health interventions as potential barriers. 42 However, reports show that up to 96% of households in metropolitan Lima and 76.6% of households in rural Peru have internet access. 43 This is supported by caregivers in the study who believed E.V.A. could reduce barriers to care by providing an affordable alternative to traditional mental health services, consistent with literature stating that digital solutions can bridge gaps in healthcare access even in low-resource settings.44,45
Limitations
This study was designed as a qualitative exploration rather than a formal pilot feasibility study, with data collection concluding upon reaching thematic saturation. While this approach ensures rich and in-depth insights, it does not include feasibility metrics such as educational efficacy, module completion rates or dropout rates. Future research could evaluate these metrics to complement the qualitative findings. Additionally, our study had a small sample size as it was based on convenience and not a predetermined calculation for sample size. Still, we provide the foundation for future quantitative and longitudinal studies to assess feasibility and effectiveness.
Another limitation of our study is that we did not directly assess caregivers’ own mental health experiences, access to treatment, or beliefs about mental health prior to the interviews. While some caregivers voluntarily shared mental health challenges and a desire for support, the lack of direct inquiry limits our ability to fully understand how these factors shape their perceptions of the chatbot. Future studies should consider exploring these aspects to provide a more comprehensive understanding of caregivers’ needs and their influence on digital mental health intervention acceptability.
While digital health interventions like E.V.A. offer accessibility and scalability, they face limitations when addressing sensitive topics in culturally diverse settings. Cultural norms surrounding mental health and sexuality may create discomfort or resistance among users, while preprogrammed content often fails to address the unique needs of marginalized populations.29,30,32 Privacy concerns are another critical barrier, particularly in communities where stigma around HIV and mental health is prevalent, as users may fear unauthorized data access. 42 Furthermore, the lack of human empathy in chatbots may hinder their ability to navigate trauma or nuanced emotional needs effectively. 39 Addressing these challenges requires culturally adaptive content, robust privacy safeguards, and hybrid models combining chatbots with human support to enhance trust and engagement.
Conclusion
This study provides evidence that a mental health chatbot named E.V.A. for Peruvian adolescents living with HIV is acceptable for a broader audience that includes their caregivers. The findings suggest that E.V.A. could not only be beneficial for caregivers’ mental health and emotional processing but also has the potential to enhance their interactions with their ALWH, fostering better communication and understanding. Despite some concerns about content sensitivity and access barriers, caregivers generally viewed E.V.A. as a useful tool that could be integrated into their caretaking. Future research with larger sample sizes is necessary to confirm these findings and explore E.V.A.'s broader applicability and impact in diverse settings.
Supplemental Material
sj-docx-1-jia-10.1177_23259582251327911 - Supplemental material for “Like Someone Is Paying Attention to You, Listening to You, and Guiding You”: Acceptability of a Mental Health Chatbot Among Caregivers of Adolescents Living With HIV
Supplemental material, sj-docx-1-jia-10.1177_23259582251327911 for “Like Someone Is Paying Attention to You, Listening to You, and Guiding You”: Acceptability of a Mental Health Chatbot Among Caregivers of Adolescents Living With HIV by Neil Rupani, Diego H. Vasquez, Carmen Contreras, Luis Menacho, Lenka Kolevic, Molly F. Franke and Jerome T. Galea in Journal of the International Association of Providers of AIDS Care (JIAPAC)
Footnotes
Acknowledgments
We are grateful to the caregivers who participated in this study.
Ethical Approval
All study procedures were approved by the Comité Institucional de Bioética de VÍALIBRE (study CIPHER), which is an IRB of record for the performance site, Socios En Salud Sucursal, Peru. The Institutional Review Board (IRB) at the University of South Florida formally agreed to rely on VÍA LIBRE for the review, approval, and continuing oversight of the research project under an interagency IRB Authorization Agreement (University of South Florida IRB Study # 005124).
Informed Consent
Written informed consent was obtained for all participants for participation in the interview or focus group, recording of the interview or focus group, and publication of deidentified information. To maintain confidentiality, the consenting process and interviews were performed in a private place chosen by the participant.
Author Contributions
Conceptualization and methodology: Neil Rupani, Jerome T. Galea, Carmen Contreras, and Diego H. Vasquez; data curation: Neil Rupani, Diego H. Vasquez, and Carmen Contreras; formal analysis: Neil Rupani, Diego H. Vasquez, and Jerome T. Galea; writing—original draft preparation: Neil Rupani; writing—review and editing: Diego H. Vasquez, Carmen Contreras, Luis Menacho, Lenka Kolevic, Molly F. Franke, and Jerome T. Galea; supervision: Jerome T. Galea.
Funding
Funding for this project was made possible by a scholarly award from Research, Innovation & Scholarly Endeavors at USF Health, Morsani College of Medicine and a Collaborative Initiative for Pediatric HIV Education grant from the International AIDS Society. The views expressed in written materials or publications do not necessarily reflect the official policies of the International AIDS Society.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data will be made available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.