
Abstract
Background
COVID-19 pandemic disrupted organized HIV screening efforts, HIV testing and management worldwide, and the impact of these disruptions from private HIV care clinics have not been examined in Myanmar. PSI/Myanmar had adapted through partner clinics, Sun Quality Health Clinics (SQH) and Lan Pya Kyel clinics (LPK), with measures like online booking, staff scheduling and awareness campaigns. The purpose of this paper was to describe whether HIV-related services changed before, during, and after the COVID-19 pandemic in Myanmar. This study aimed to identify factors influencing ART retention and VL testing.
Methodology
Data from 43 healthcare facilities across 8 regions (2018-2022) was analyzed for HIV indicators, including HIV tests, positive cases, ART retention, viral load (VL) testing, and suppression rates in two channels during different phases.
Results
During the COVID-19 pandemic, both Channel 1 (SQH) and Channel 2 (LPK) showed fluctuations in HIV testing and new positive cases. Channel 1 had 28.2% decrease in testing (37 735 fewer tests) while Channel 2 had 8.1% increase (81 596 tests). However, testing numbers continued to decline. ART retention declined over 12 months compared to 6 months for both channels. Channel 1 had a slight drop in 6-month retention during the crisis (89.3-88.1%) but an increase in 12-month retention after. Channel 2 maintained high 6-month retention rates (>90%) but varied in 12-month rates (from 80.1% to 92.9%). Unsuccessful outcomes were more common at 12 months in both channels (4.7-21.8% in Channel 1; 7.1-19.9% in Channel 2). VL testing at 12 months significantly decreased during the crisis, notably in Channel 2 (81.9-1.3%). However, high rates of VL suppression (>91%) were consistently seen in those tested in both channels before, during, and after COVID-19. Univariable and multivariable cox proportional hazards models were used to identify factors influencing ART retention. Univariable and multivariable logistic regression analyses were done for VL testing. Factors such as residence location, the period of COVID-19, use of second-line ART, and patient demographics (such as age and key population type) influenced both. Specifically, individuals seeking care from Mandalay [aHR = 1.37, P value < 0.01], and enrolled for ART during or after COVID-19 [aHR = 3.31, P value < 0.01], were more likely to be retained at 12 months. VL testing was positively associated with having no TB [aOR = 1.35, P value < 0.01], being MSM [aOR = 1.69, P value < 0.01], PWIDs [aOR = 2.51, P value < 0.01], and seeking care at Channel 2[aOR = 1.76, P value < 0.01].
Conclusion
The study highlighted interruption in ART retention and VL testing because of the COVID-19 pandemic, emphasizing the need to maintain essential HIV services and address gaps based on patient demographics, clinic type, ART enrollment period, and location. Certain factors played a role in influencing these outcomes, providing insights into potential areas for improvement in HIV care and treatment during similar crisis situations to ensure consistent and effective HIV care.
Plain Language Summary
Why Was the Study Done?
The COVID-19 pandemic disrupted HIV testing and treatment services worldwide. However, the impact on private HIV clinics in Myanmar has not been well studied. This study identified the extent to which HIV-related services had been affected by the COVID-19 pandemic in Myanmar and how we could overcome these challenges.
What Did the Researchers Do?
The clinics adapted by implementing measures like online booking, staff scheduling changes, and awareness campaigns. The study looked at HIV program data from 43 healthcare facilities across 7 regions from 2018 to 2022, and the following HIV indicators: number of HIV tests done, positive HIV cases identified, ART retention, viral load (VL) testing, HIV viral suppression, were explored. The data was divided into two channels and different COVID-19 periods to see how these HIV services changed.
What Did the Researchers Find?
It addressed a gap in existing studies by providing quantitative evidence from private clinics in Myanmar, shedding light on the impact of the pandemic on HIV-related care. The number of HIV tests done, and new HIV cases found fluctuated during the COVID-19 pandemic in both channels. ART retention declined at 12 months compared to 6 months in both channels. Unsuccessful treatment outcomes were more common at 12 months, while viral load (VL) testing significantly decreased during the crisis, especially in Channel 2. However, VL suppression rates remained high (>91%) in both channels. Factors influencing ART retention and VL testing included seeking care from Mandalay, initiating ART during or post-COVID-19, using second-line ART, and demographic variables such as age and belonging to key populations (MSM, PWID).
What Do the Findings Mean?
Despite declines in viral load monitoring and treatment retention, it highlighted opportunities for improvement: multi-month medication supply, online counseling, and booking systems. The findings advocated for improvement in HIV care and treatment during similar crisis situations in the future.
Introduction
Myanmar is one of the countries in the WHO South-East Asia Region with a high burden of HIV. In 2022, over 270 000 people were living with HIV in Myanmar, including 8900 children under the age of 15. 1 HIV prevalence was particularly high among key populations including people who inject drugs (PWIDs), female sex workers (FSWs), and men who have sex with men (MSMs). In the same year, 210 000 people received antiretroviral therapy (ART) and estimated 11 000 new HIV infections and 6400 HIV-related deaths occurred. 2
The rapid global spread of COVID-19 since late 2019, declared a pandemic on March 12, 2020, has created significant challenges for maintaining HIV care. 3 The pandemic has disrupted healthcare systems worldwide, leading to a substantial decline in HIV testing and ART adherence. 4 Comorbidities significantly influence COVID-19 outcomes in immunodeficient patients by exacerbating the severity of the disease and complicating treatment. 5 Global public health priorities shifted toward COVID-19 control, many healthcare providers were reassigned, resulting in critical interruptions to HIV services. This crisis has impacted the continuity of care for people living with HIV (PLHIV), limiting access to testing, treatment, and follow-up services even in well-resourced countries. 6 Furthermore, many individuals faced challenges such as loss of access to ART, with 27% unable to receive their medication, which directly correlates with increased risks of viral transmission and complications associated with untreated HIV. 5 Moreover, the COVID-19 pandemic exacerbated existing mental health issues among PLWH, with rising rates of anxiety, depression, and substance abuse. These psychological challenges compounded the difficulties in maintaining treatment adherence and navigating healthcare services. 5
There were many challenges in implementing appropriate HIV services, especially concerning healthcare provision and ensuring continuous care for individuals with HIV/AIDS. 7 People who were retained in care demonstrated higher adherence to ART and experienced improved health outcomes and reduced HIV transmission rates. 8 Missed medical appointments are independently associated with an increased risk of AIDS and death.8,9 Traditionally, retention in care has relied on the ability of people living with HIV to meet regularly with their HIV medical team, 10 which in many places has been difficult to do during the COVID-19 pandemic. The delivery of HIV treatment and prevention services has been significantly disrupted as a consequence.11-13
The first case of COVID-19 in Myanmar was detected in March 2020, followed by a gradual rise of cases which constituted the first wave until May 2020. 14 Since early January of the same year, the government swiftly implemented various public health measures to control the spread of the virus and mitigate its impact on the healthcare system and economy. 15 Subsequent waves of COVID-19 hit Myanmar, with the second wave starting in mid-August 2020 and the third wave being caused by the Delta variant in June 2021. 16 As of December 20, 2023, Myanmar had reported 641 393 confirmed COVID-19 cases and 19 494 deaths. 17 The public health facilities faced overcrowding due to COVID-19, with specialists reassigned to cope. Hospitals became hotspots, risking outpatients with chronic diseases, and staff faced challenges due to reassignment and quarantine. Many health facilities that provided HIV prevention, treatment, and care services had to change their schedules and operation to cope with the challenges imposed by COVID-19 and the prevention and control measures (social distancing, travel restrictions, stay-at-home orders, etc.) were taken to control its spread. As a result, routine, non-urgent, or elective health care visits and procedures were canceled or postponed. Additionally, supportive services, like face-to-face counseling, housing services, and outreach services, were temporarily suspended. 15 The patients avoided accessing health care, even for urgent concerns, due to fear of COVID-19 exposure.
Despite progress made over the years, due to COVID-19 and other contextual issues, Myanmar started experiencing challenges in ensuring continuity of HIV services. The COVID-19 disrupted HIV programs, affecting both mortality rates and new infections, with access to healthcare services declining since March 2020. This had posed challenges for PLHIV in receiving timely diagnosis and treatment, impacting the continuity of HIV services in the country. 18 During these challenging times, Population Services International (PSI) Myanmar collaborated with Sun Quality Health Clinics (SQH) and Lan Pya Kyel Clinics (LPK) to ensure access to HIV services, including an uninterrupted supply of essential health commodities. Their efforts extended HIV/AIDS prevention, care, and treatment services across 8 regions in Myanmar, benefiting approximately 8700 individuals from key populations with high risk, such as MSMs, FSWs, PWIDs, and transgender people (TGW). Additionally, PSI offered ongoing technical assistance to its partners (SQHC and LPK) in implementing HIV services in alignment with global guidelines, aiming for favorable health outcomes for those infected with HIV.
In response to the pandemic, a contingency plan, incorporating online booking, awareness campaigns, alternative staffing, and scheduling, was implemented. Teleconsultations and social media engagement were adopted to address communication challenges and actively follow-up with clients for HIV testing, adherence to ART, counseling, and medical care connections. Additionally, efforts such as setting up emergency response core group, staff training, scheduled assignments, and commodity supply, including home delivery, were also being done to ensure continuity of HIV services.
Several studies have shown that COVID-19 pandemic had posed various challenges to maintaining HIV care. 19 Despite the high burden of COVID-19 in low- and middle-income countries, little is known about COVID-19's contribution to the interruption of healthcare for PLHIV from Myanmar. To improve healthcare delivery and provide sustainable quality care to PLHIV during the COVID-19 pandemic and future pandemics, we need to better understand the nature, scope, and factors associated with interruptions in HIV treatment services.
This study aimed to understand areas and types of services affected by COVID-19 in private clinics. This study examined trends in HIV testing, positivity, ART retention, and viral load testing rates, aiming to identify factors influencing ART retention and viral load testing among PLHIV before and during the COVID-19 pandemic. The results of this study will allow operation team and healthcare providers to understand and find solutions to reduce HIV care interruptions to PLHIV. In addition, it informs policymakers about planning and allocating resources for PLHIV in low- and middle-income countries and it can help to prepare for future public health emergencies.
Methodology
Study Design
This cross-sectional quantitative study utilized individual HIV program data from 43 healthcare facilities collected between January 2018 and December 2022 from PSI Myanmar and partner organizations such as Lan Pya Kyel (LPK) Association and Sun Community Health (SCH). The study included individual HIV cascade data from seven states and regions—Ayeyarwady, Bago, Kachin, Mandalay, Sagaing, Shan (North) and Yangon. This study aimed to examine HIV care services, including testing, positive cases, yield, ART initiation interval, retention, viral load testing, and suppression, across different COVID-19 phases to understand healthcare delivery for HIV patients during the pandemic.
Study Population and Setting
This study included PLHIV enrolled in care at 43 private facilities affiliated with PSI Myanmar and partner organizations such as Lan Pya Kyel (LPK) Association and Sun Community Health (SCH) from January 2018 to December 2022 with no age restrictions. These 43 private facilities were selected because they were affiliated with PSI Myanmar and partner organizations, such as the Lan Pya Kyel (LPK) Association and Sun Community Health (SCH) and played a crucial role in providing free ART and other HIV-related services across the country. These facilities are strategically located to ensure that individuals living with HIV have access to essential healthcare services, especially in underserved areas. By collaborating with local organizations (LPK and SCH), PSI Myanmar enhances the reach and effectiveness of HIV programs, ensuring that vulnerable populations receive comprehensive care. This network not only facilitates access to ART but also includes support services such as counseling and testing, which are vital for managing HIV effectively. In addition to providing medical services, these facilities contribute to broader public health goals by implementing innovative approaches to HIV prevention and treatment, like community-based outreach programs, online platforms that engage key populations at higher risk of HIV, thereby fostering a supportive environment for those affected by HIV. ART and other HIV-related services are provided free of charge at all these clinics, and they remained open during the COVID-19 lockdown in Myanmar. Before and throughout the lockdown, there were no reports of ART stockouts in the study clinics, and public health messaging highlighted the importance of ART for all PLHIV. 20
The SCH affiliated SQH GP clinics (Channel 1) offered an essential package of integrated HIV services within general health services to improve access for other vulnerable populations (OVPs). Hidden key populations uncomfortable with visiting KPSC were referred to SQHs through community referrals and peer health workers from partner organizations. Community-referred HIV testing involved volunteers providing health education sessions and referring individuals to SQH clinics for counseling and testing. Linkage to care was managed by SQH clinic doctors.
The LPK (Channel 2) provided HIV prevention services to key populations, including MSMs, FSWs, transgender women (TGW), and other vulnerable populations (OVPs) through the key population service center (KPSC), community-based HIV screening (CBS), index testing, and mobile activities. Linkage to care and treatment was facilitated at KPSC.
Data Collection
Quantitative data was extracted from the HIV cascade database of routinely collected PSI Myanmar's HIV program data server and client cascade data from SCH and LPK's clinics from the period of January 2018 and December 2022. Data retrieval was done by PSI/Myanmar in-house research team with support from PSI/MM MIS team, PMD team, operation side (SCH and LPK).
Data Sources were from 2 types: HIV testing data, ART enrollment and cascade data. Client's demographics, provider information, HIV records related to testing and treatment, and relevant diagnostic and treatment information, outcome status were also extracted.
Data Management and Analysis
The extracted anonymized patient-level program data were entered directly into Stata 14© (StataCorp, College Station, TX) for cleaning and analysis. Descriptive statistics, including counts and percentages, were used to summarize demographic and clinical data and present crude summaries of outcomes before and after the pandemic. Differences in testing services and treatment services were compared before COVID-19 and during and after COVID-19 phases. Included PLHIV received a separate study code before data were extracted into Stata to create the study database. The key to link study codes with program codes was password protected, only accessible to the first author. In case of discrepancies in the program database, clarification was done with respective operation team of SCH and LPK and data management team of PSI Myanmar, and corrections made. Data cleaning and verification were mainly conducted by the first author.
As for the testing services, the number of HIV tests was defined as the number of individuals who received HIV Testing Services (HTS) and received their test results within the covered period. HIV yield/positivity rate was calculated as the percentage of HIV-positive case among tested individuals within the covered period. Testing services were compared across different COVID-19 phases in each channel (Channel 1 vs Channel 2). The percentage reduction/increase was calculated as a simple proportion taking the difference as the numerator and the overall count per each interval as the denominator, along with the 95% confidence interval (CI) calculated.
As for the treatment services, the ART initiation interval was calculated as the interval between HIV positive and ART initiation. The ART retention (clients who were still on ART) was calculated from the date of treatment initiation until completion of 6 months and 12 months.
For ART retention in this study, the time interval in Kaplan–Meier curves was defined as the time from the start of therapy until the event of interest, the discontinuation of ART or loss to follow-up. The start point was defined as time zero when each patient started ART that was the baseline for measuring retention. For the time to event (retention or non-retention), the Kaplan–Meier curve tracked each patient over time, measuring the duration until an event occurred. The event could be a patient discontinuing therapy, being lost to follow-up, or reaching a defined follow-up period (eg, 6 or 12 months).
Censoring, patients who were still on ART at the last follow-up time were “censored” at that point, meaning they did not experience the event (non-retention). Censoring could also occur if the patient was lost to follow-up for reasons other than stopping ART, such as moving away or dying from unrelated causes.
The observed intervals were continuous in Kaplan–Meier analysis, meaning the curve plots the proportion of patients still retained in ART over the entire follow-up period. This was shown over years (0.5 year for 6 months, 1 year for 12 months, 1.5 years for 18 months, and 2 years for 24 months), continuously tracking survival (retention) from the start of therapy until the event or censoring.
If the Kaplan–Meier curve showed a sharp drop after a certain time (eg, 12 months), it meant that more patients stopped therapy or were lost to follow-up after that point. The steepness of the curve indicated the rate at which patients were leaving therapy (discontinued), and flat segments indicated periods when most patients were retained.
Twelve months VL testing was defined as ART clients who had at least one VL tested after 12 months. Viral load suppression was calculated as the percentage of ART patients with suppressed viral load (VL) result (<1000 copies/ml).
Univariable and multivariable Cox-regression analyses were conducted to identify factors associated with ART retention. Hazard ratios (HR) and 95% confidence intervals (CI) were presented. The univariable and multivariable logistic regression were applied for VL testing. Age and sex were retained in the multivariable model, as well as variables with p-values ≤0.05. Odds ratios (OR) and 95% confidence intervals (CI) were presented.
Findings
Table 1 presented the characteristics of HIV clients, including enrollment for ART across different time periods, demographic profiles, key population categories, ART treatment durations, regimens taken, TB status and anti-TB treatment. A total of 10 338 HIV clients were enrolled across different phases: 46.6% before the COVID-19 crisis (Jan 2018-Mar 2020), 4.9% during the first wave (Apr 2020-July 2020), 9.2% during the second wave (Aug 2020-Apr 2021), 13.4% during the third wave (May 2021-Dec 2021), 6.1% during the fourth wave (Jan 2022-April 2022), and 19.9% in the post-COVID-19 crisis (May 2022-Dec 2022).
Characteristics of People Receiving ART Through Different Health Service Channels.
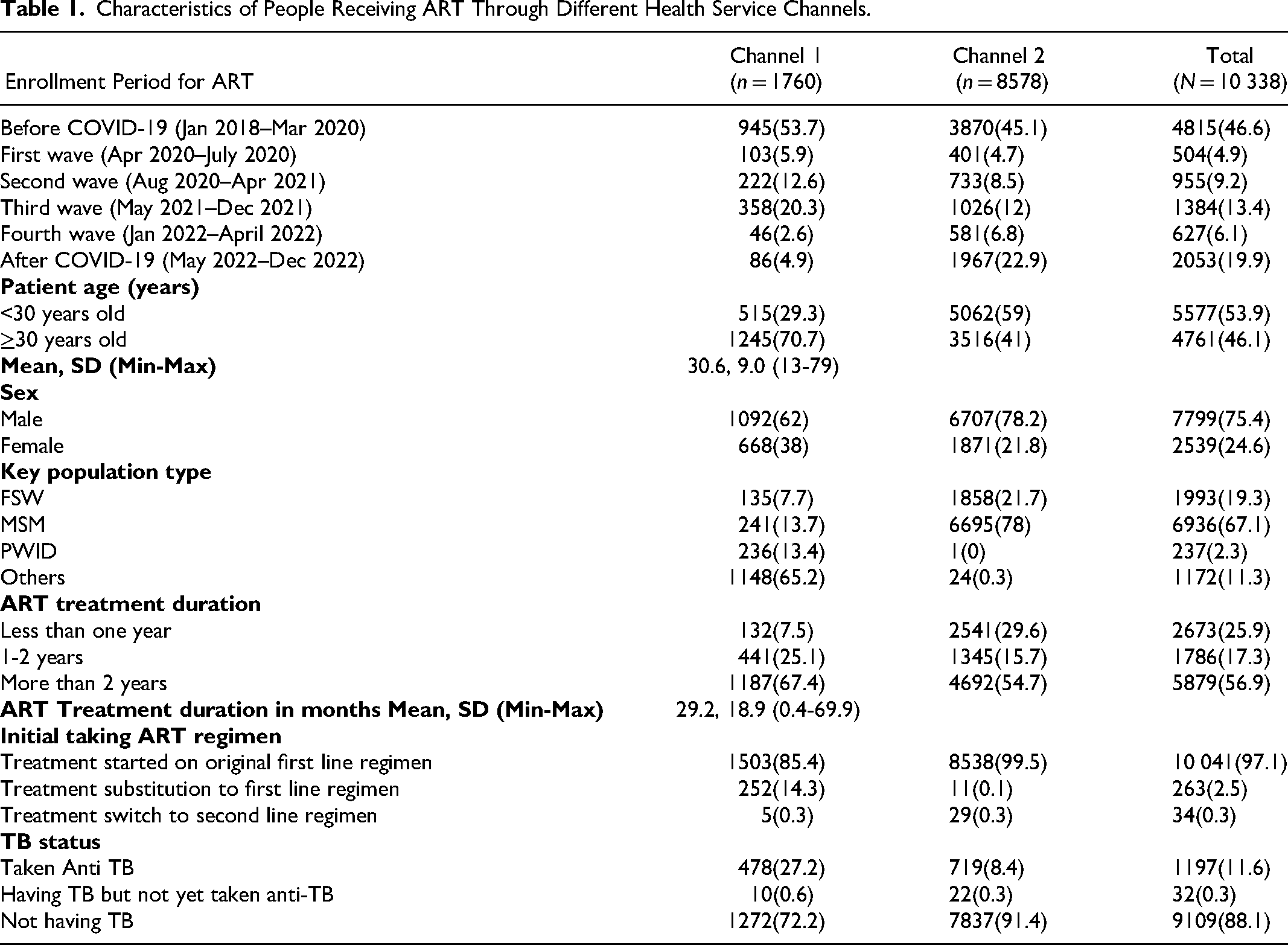
Sun Quality Health (Channel 1) enrolled 17.0% of all HIV clients, whereas Lan Pya Kyel (Channel 2) enrolled 83.0% of them. Half of the HIV clients (46.1%) were aged 30 and above. The majority were men (75.4%) with women making up 24.6%. Among different key population groups, 19.3% were FSWs, 67.1% were MSMs, 2.3% were PWIDs, and 11.3% were from the general population. ART treatment duration was categorized as follows: 25.9% for less than 1 year, 17.3% for 1-2 years, and 56.9% for more than 2 years. In terms of the initial ART regimen, 97.1% started with the original first line regimen, 2.5% underwent treatment substitution to the first line regimen, and 0.3% switched to the second line regimen. Regarding TB status, 11.6% were on anti-TB, while the majority (88.1%) were not having TB nor on anti-TB.
HIV Testing Services
Figure 1 illustrated a decrease in the percentage of positive HIV tests over time, despite fluctuating total test numbers. Channel 2 consistently had a higher positive yield than Channel 1, and although there was a slight increase in 2022, both channels displayed decreasing trends. The total number of HIV tests varied yearly, with Channel 2 having the highest count in 2022 and Channel 1 in 2019. This indicated regular testing in both channels, but a decrease in positive yield (Figure 1).
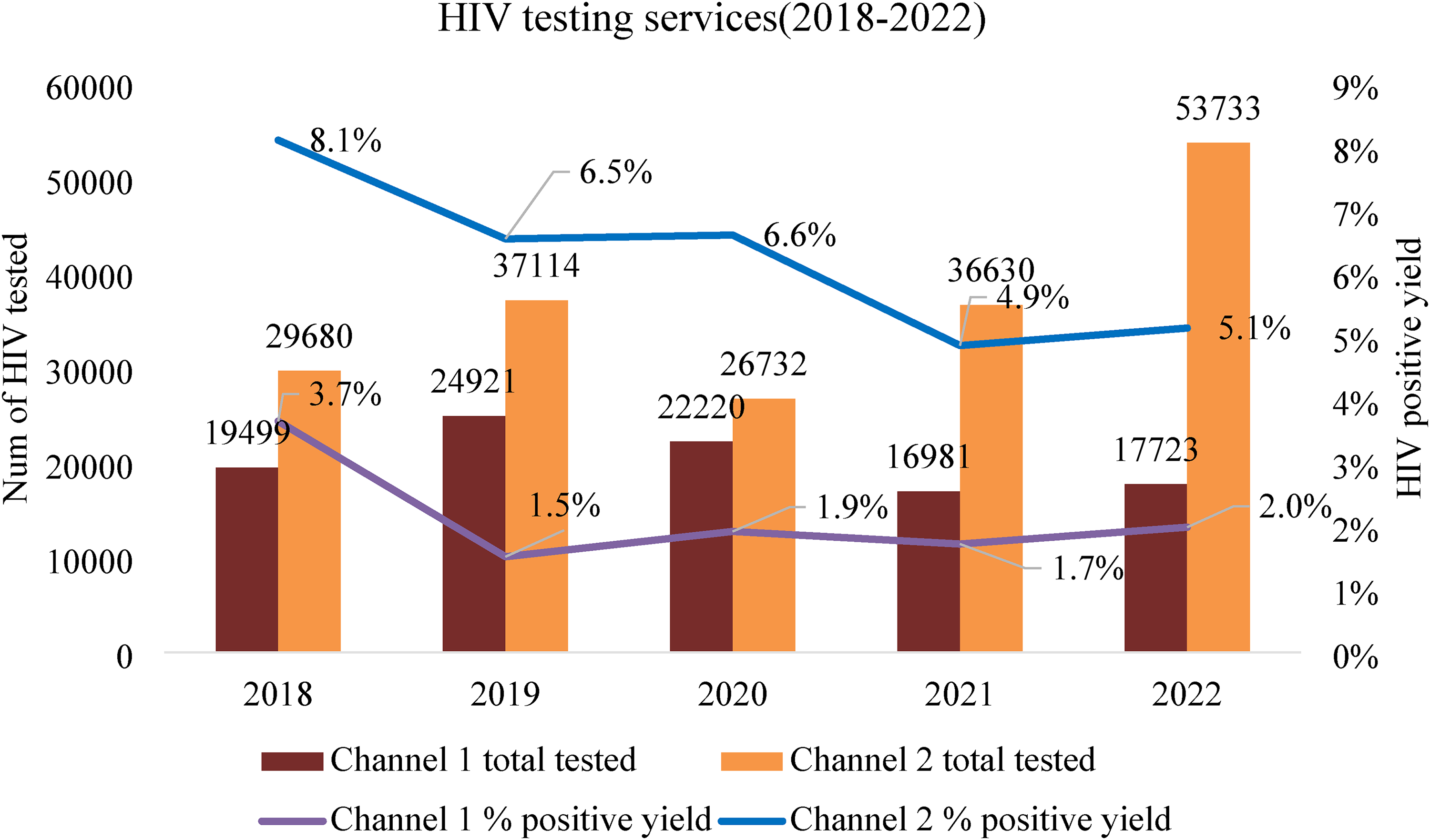
HIV testing services by year between different channels.
The HIV testing trends during COVID-19 phases were similar to the HIV testing from the observed period between 2018 and 2022.
Figure 2 showed HIV positive yield and total HIV tests at Channels 1 and 2 before and during the crisis. Before the crisis, Channel 2 had a 7.2% yield, and Channel 1 had 2.4%. During the crisis, yields decreased, varying across phases. In the first wave, Channel 2 decreased to 6.9%, and Channel 1 remained at 2.4%. The lowest yield was in the second wave, with a slight increase after the third wave. Channel 2's yield during the second wave was 4.8%, and Channel 1's was 1.7%, with more tests at Channel 2. In the third wave, Channel 1 had a 1.7% yield, with increased yield at Channel 2. Overall, COVID-19 impacted HIV testing rates and positive yield in both channels, showing a decrease in most periods, though regular testing continued during and after the crisis.
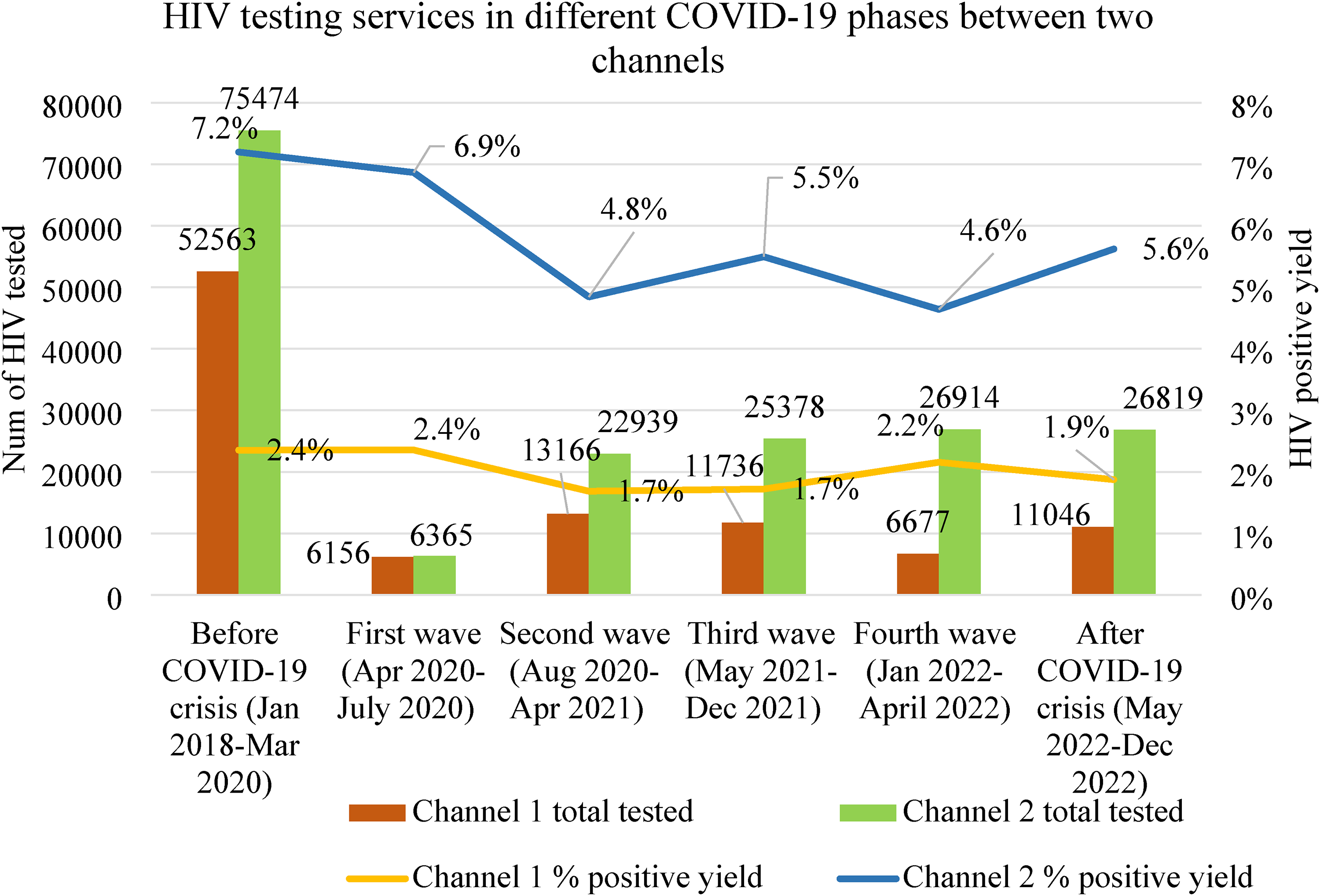
HIV testing services in different COVID-19 phases between two channels.
Table 2 provided HIV testing and new positive cases across COVID-19 phases for Channels 1 and 2. Before COVID-19 (Jan 2018-Mar 2020), Channel 1 conducted 52 563 tests, and Channel 2 conducted 75 474 tests. After COVID-19 (May 2022-Dec 2022), testing further decreased, with Channel 1 conducting 11 046 tests, and Channel 2 conducting 26 819 tests.
Impact of COVID-19 Pandemic on the HIV Testing for People Living with HIV and new HIV Positive Yield in HIV Testing.
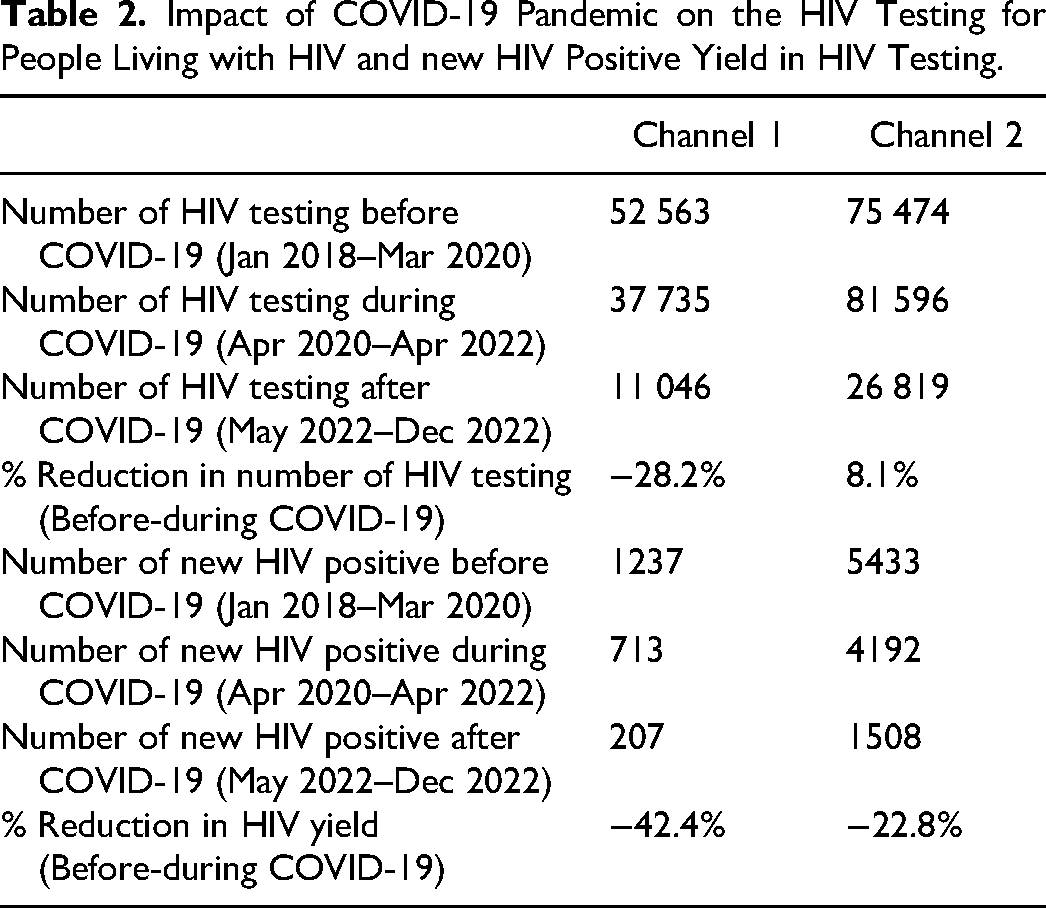
New HIV positive cases decreased substantially in each channel during the crisis. Before the crisis, Channel 2 identified 5433 new cases, and Channel 1 did 1237. During the crisis, Channel 2 identified 4192 new cases (22.8% reduction), and Channel 1 did 713 new cases (42.4% reduction). In the post-COVID-19 period, new cases continued to decrease for both channels, with Channel 2 identifying 1508 new cases and Channel 1: 207 new cases.
Linkage to Care-Treatment Services
Antiretroviral Therapy (ART) Initiation
To calculate ART initiation intervals, 6.3% of HIV clients had no recorded information on their first HIV confirmed date. Among the 9691 clients with their first HIV tested date, 88.5% were from Channel 2, and 11.5% were from Channel 1.
Figure 3 presented the ART initiation intervals in two channels before, during, and after COVID-19 pandemic. In Channel 1, the percentage of clients initiating ART within 7 days increased from 5.6% before COVID-19 to 6.2% during and further rose to 11.6% after the crisis. Channel 2 showed a substantial increase in the percentage of clients initiating ART within 7 days during the crisis (from 75.0% to 95.6%), but this declined to 70.6% after the crisis.
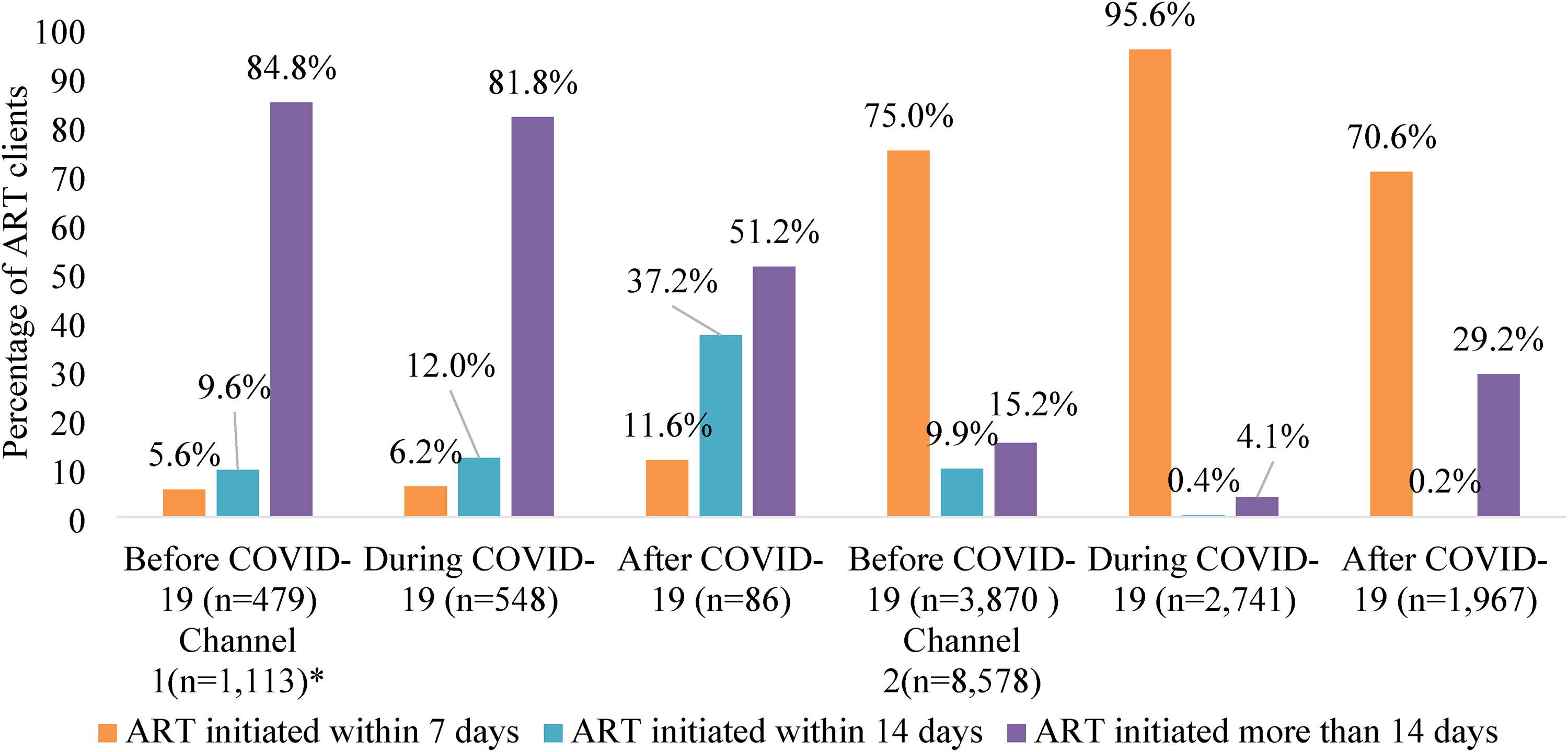
ART initiation interval between two channels. *For only those who have first HIV-positive records.
Both channels showed variations in the percentage of clients initiating ART within 14 days. In Channel 1, the percentage increased from 9.6% before COVID-19 to 12.0% during COVID-19 and further rose to 37.2% after COVID-19. In contrast, Channel 2 experienced a sharp decrease in the percentage of clients initiating ART within 14 days, from 9.9% before COVID-19 to 0.4% during the crisis, and further down to 0.2% after the crisis.
A notable shift was observed in the percentage of clients initiating ART more than 14 days after their first HIV test. In Channel 1, this percentage decreased from 84.8% before COVID-19 to 51.2% after the crisis. In Channel 2, there was a drastic decrease from 15.2% before COVID-19 to 4.1% during the crisis, followed by a substantial increase to 29.2% after the COVID-19 pandemic.
ART Retention and Other Outcomes
Figure 4A shows the Kaplan–Meier survival estimate for ART retention among PLHIV enrolled in the ART program across two channels. There were significant differences in retention in care between Channel 1 and Channel 2 (Log Rank = 146.61, p < 0.001). Figure 4B shows the Kaplan–Meier survival curves for ART retention in channel 1, by COVID-19 timeline while Figure 4C similarly shows the Kaplan–Meier survival curves for ART retention in Channel 2 by COVID-19 timeline.
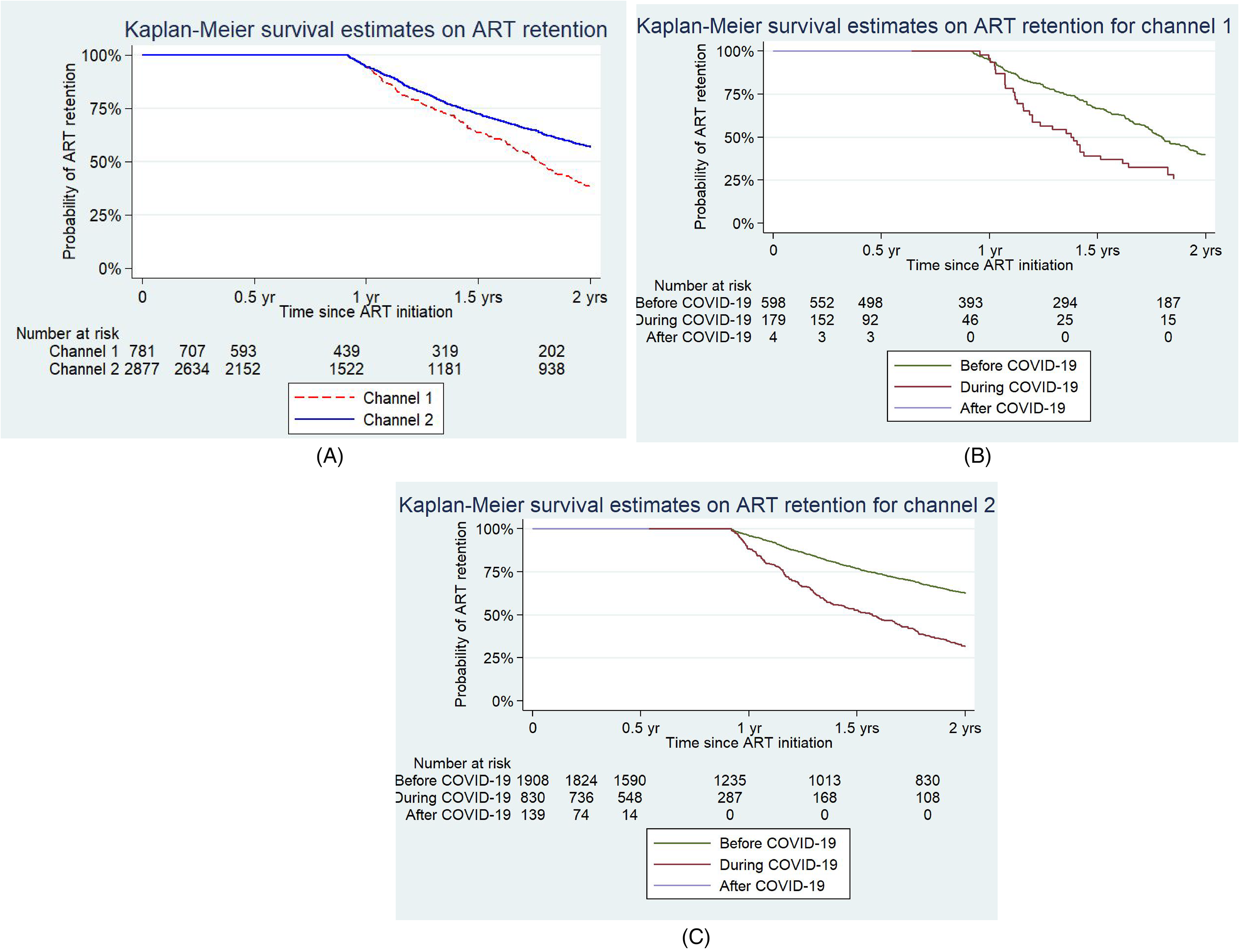
(A–C) Kaplan–Meier survival estimates on ART retention.
Table 3 illustrats that both channels experienced fluctuations in retention rates during the COVID-19 pandemic. Channel 1 showed a slight decrease in its 6-month retention rate during the crisis, from 89.3% before the crisis to 88.1% during the crisis. However, the 12-month retention rate increased after the crisis. In contrast, Channel 2 maintained high 6-month retention rates (89.6-93.7%) across all time periods, but its 12-month retention rates fluctuated (80.1-92.9%). The unsuccessful outcomes were higher at 12 months compared to 6 months, ranging from 4.7% to 21.8% at Channel 1 and 7.1% to 19.9% at Channel 2. Notably, retention rates were generally lower during the crisis but showed improvement after the crisis, both at the 6-month and 12-month ART retention in Channel 2.
Patient Outcome Disaggregated by COVID-19 Phases and Different Channels.
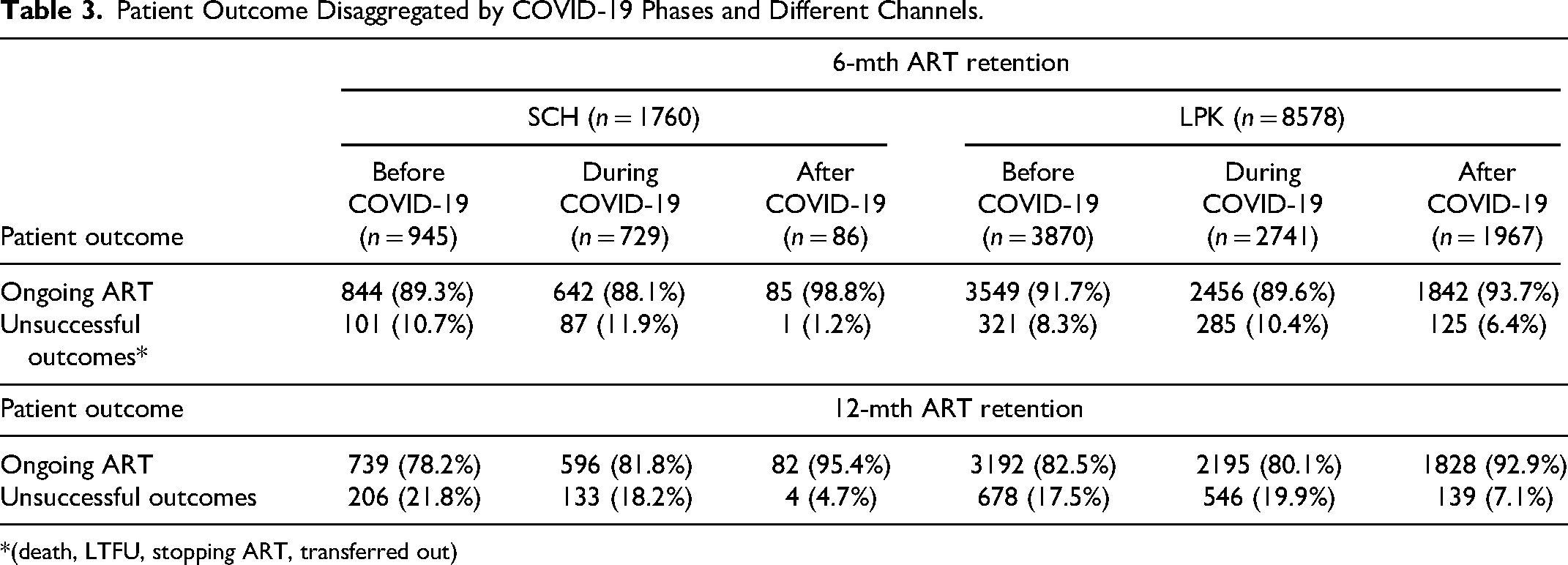
*(death, LTFU, stopping ART, transferred out)
Table 4 shows a comprehensive overview of VL testing status and VL suppression status among HIV clients, by health service channels and the COVID-19 phases. Within 12 months after ART initiation, 62.2% of HIV clients underwent viral load (VL) testing, while 37.8% did not. Variations in VL testing rates across Channel 1 and Channel 2, with a substantial decline in VL testing rate after COVID-19, particularly in Channel 2. Among those who received testing for VL from both channels showed consistently high rates of VL suppression (>90%) across different phases of COVID-19.
VL Testing and VL status Disaggregated by COVID-19 Phases and Channels.

*Clients who had VL result, and currently on ART at the end of Dec 2022.
Predictors of ART Retention
Table 5 presents the results of the univariable and multivariable Cox-regression analyses for predictors of ART retention. In the univariable analysis for 6-month ART retention, being female (hazard ratios (HR) 1.42; 95% confidence interval [CI] 1.31-1.54; P < 0.001), seeking care from Mandalay (HR-1.23; 95% CI 1.09-1.38; P < 0.001), enrolling for ART during/after COVID-19 (HR-2.93; 95% CI 2.67-3.23; P < 0.001) were positively associated with retention, while seeking care from Yangon (HR 0.66; 95% CI 0.60-0.72; P < 0.001), being a man who has sex with men (MSM) (HR 0.67; 95% CI 0.61-0.74; P < 0.001), seeking care at Channel 2 (HR 0.67; 95% CI 0.61-0.74; P < 0.001), were negatively associated.
Results from Cox Regression Model, Hazard Ratios (HR) and Adjusted Hazard Ratios (aHR) for 6-Months, 12-Months Retention on Antiretroviral Therapy (ART).
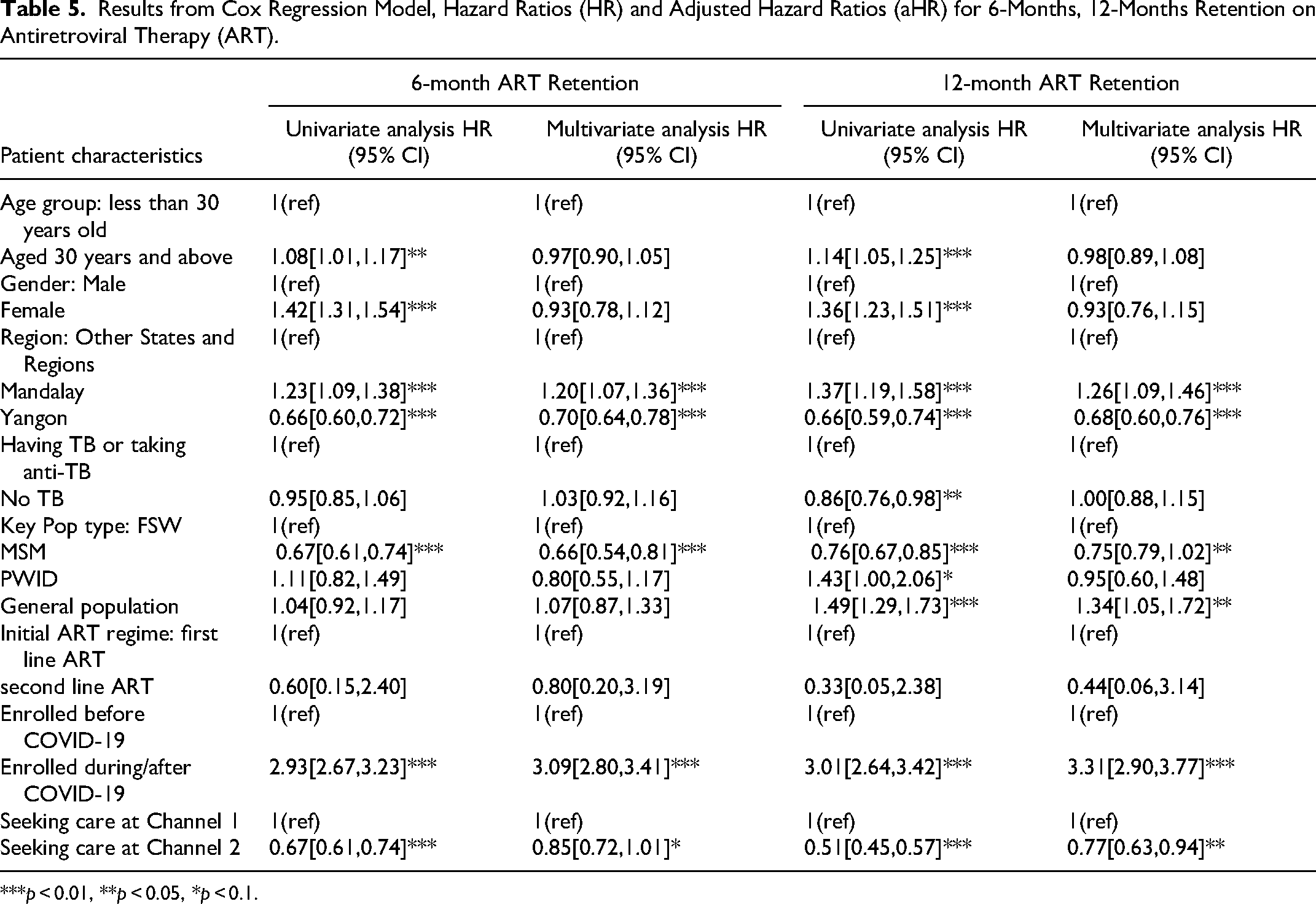
***p < 0.01, **p < 0.05, *p < 0.1.
In the multivariable analysis, being MSM (HR 0.66, 95% CI 0.54-0.81), and seeking care from Yangon (HR 0.70, 95% CI 0.64-0.78), were negatively associated with the 6-month ART retention, while seeking care from Mandalay (HR 1.20, 95% CI 1.07-1.36), and enrolling during or after the COVID-19 period (HR 3.09, 95% CI 2.80-3.41) were positively associated.
In the univariable analysis for 12-month ART retention, seeking care from Yangon was negatively associated with ART retention (HR 0.66, 95% CI 0.59-0.74), while seeking care from Mandalay was positively associated (HR 1.37, 95% CI 1.19-1.58). Being a man who has sex with men (MSM) was negatively associated (HR 0.76, 95% CI 0.67-0.85), while being female (HR 1.36, 95% CI 1.23-1.51) or being from the general population was positively associated (HR 1.49, 95% CI 1.29-1.73). Being aged 30 years and above (HR 1.14, 95% CI 1.05-1.25), enrolling during or after the COVID-19 period (HR 3.01, 95% CI 2.64-3.42), and seeking care at Channel 2 (HR 0.51, 95% CI 0.45-0.57) were other statistically significant factors.
In the multivariable analysis, seeking care from Yangon (HR 1.26, 95% CI 1.09-1.46), enrolling during or after the COVID-19 period (HR 3.31, 95% CI 2.90-3.77) were associated with a higher likelihood of ART treatment retention, while seeking care from Yangon (HR 0.68, 95% CI 0.60-0.76) was associated with a lower likelihood of ART care retention. Table 6 shows the univariable and multivariable logistic regression analysis for 12-month VL testing. In the univariable analysis, being female (OR 0.62; 95% CI 0.57-0.68; P < 0.001), seeking care from Mandalay (OR 0.56; 95% CI 0.5-0.62; P < 0.001), receiving second line ART (OR 0.19; 95% CI 0.08-0.47; P < 0.001), enrolling during or after COVID-19 (OR 0.27; 95% CI 0.25-0.29; P < 0.001), were negatively associated with viral load testing. Conversely, being a MSM (OR 1.68; 95% CI 1.52-1.85; P < 0.001), seeking care at Channel 2 (OR 1.77; 95% CI 1.59-1.96; P < 0.001), having no TB (OR 1.28; 95% CI 1.14-1.44; P < 0.001) and seeking care from Yangon (OR 1.15; 95% CI 1.04-1.26; P < 0.001) were positively associated with viral load testing.
Results from Univariate and Multivariate Logistic Regression Analysis for 12 Months Viral Load Testing.
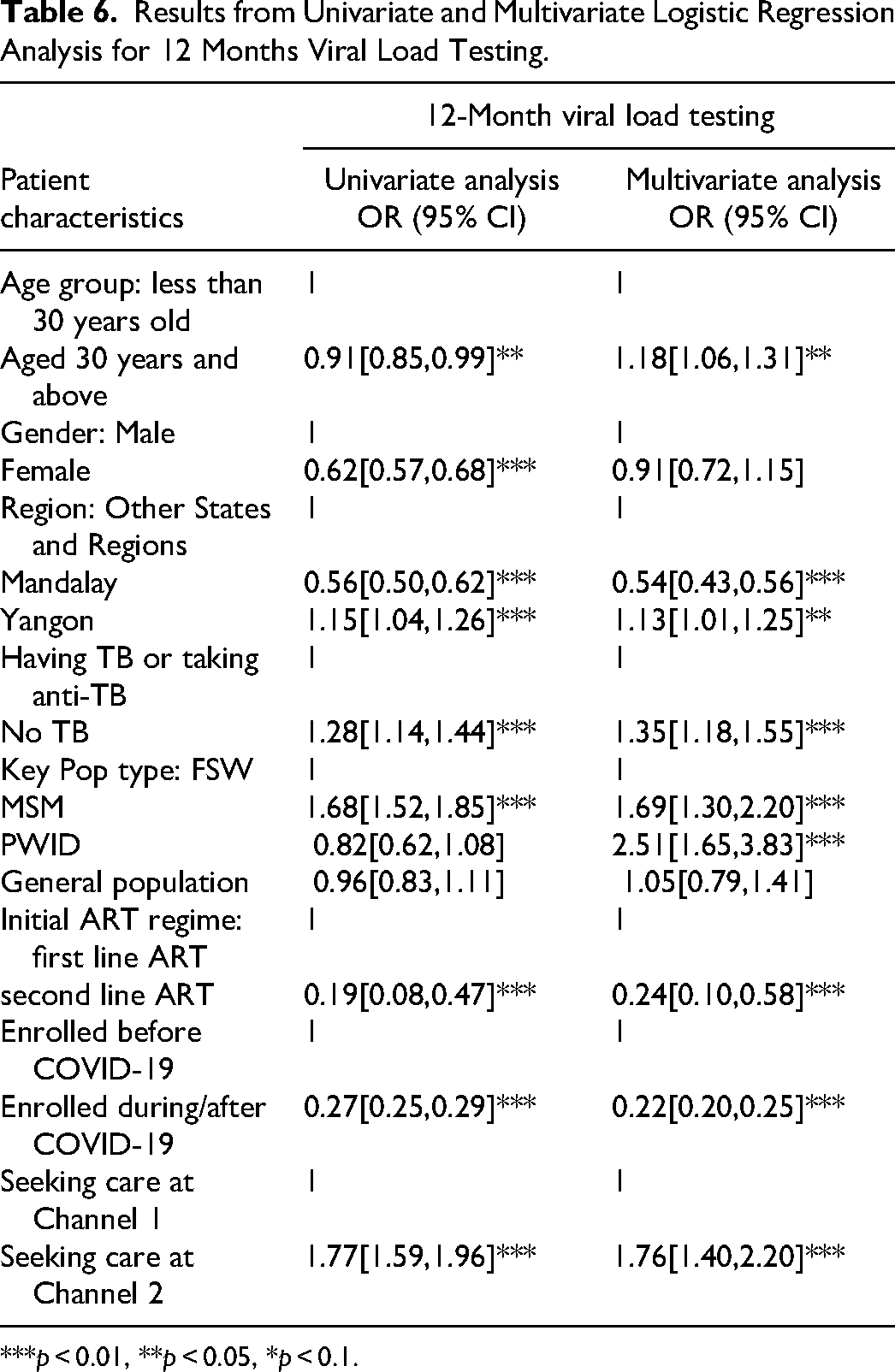
***p < 0.01, **p < 0.05, *p < 0.1.
Multivariable logistic regression analysis was conducted and factors positively associated with viral load test uptake included having no TB (OR 1.35; 95% CI 1.18-1.55; P < 0.001), being an MSM (OR 1.69; 95% CI 1.30-2.20; P < 0.001), or a PWID (OR 2.51; 95% CI 1.65-3.83; P < 0.001), and seeking care at Channel 2 (OR 1.76; 95% CI 1.40-2.20; P < 0.001). Conversely, being a resident of Mandalay (OR 0.54; 95% CI 0.43-0.56; P < 0.001), enrolling during or after COVID-19 (OR 0.22; CI 0.20-0.25; P < 0.001) were negatively associated.
Discussion
This study was the first one to investigate the effects of the COVID-19 pandemic on HIV services in private sector facilities in Myanmar, while the study done in 2021, reviewed the implementation of the HIV Contingency Plan after 4 months of implementation during the first wave of COVID-19 in Myanmar which began in March 2020. 20 The study found that despite efforts to mitigate the impact, there were significant disruptions in HIV services due to the COVID-19 pandemic, indicating notable declines in HIV testing, positive test rates, ART retention, and viral load testing. Although the number of PLHIV on ART remained stable from April to September 2020 according to UNAIDS, our findings were consistent with their reports of reduced HIV testing and ART initiation globally during the same period. 21 This could be due to lockdowns to prevent the spread of COVID-19, and it had a wide-range impact on healthcare delivery along with widespread fears of contracting the virus, which resulted in a significant drop in HIV testing.
The management of HIV infection in low- and middle-income countries (LMICs) was significantly impacted by the COVID-19 pandemic, particularly in health service delivery. Numerous studies have documented the detrimental effects of COVID-19 on the treatment of PLHIV, revealing significant challenges in both HIV-specific and general health care.4,22,23 For instance, the study involving ten Asian countries reported that 35.9% of PLHIV and 57.5% of key populations experienced reduced hospital visits during the pandemic, with notable declines in HIV RNA viral load testing (21.9% for PLHIV and 47.3% for key populations) and interruptions in ART affecting 22.3% of PLHIV. 24 In countries like the Philippines and India, healthcare providers reported higher rates of rescheduled or delayed appointments due to clinic closures, highlighting significant disparities in service access. Moreover, health care providers perceived interferences in delivery of healthcare to the HIV community, with decreased patient load, HIV-related testing, as well as ART refills. These observations were also reflected in Africa, 25 China, 26 Europe, 27 and the USA, 28 with reports of decreased viral load monitoring, interferences in ART adherence. Common barriers included travel restrictions (40.6%), financial difficulties (28.9%), and challenges in obtaining prescription refills (26.9%). Although 85% of healthcare providers adopted telemedicine to deliver HIV care, a substantial portion of PLHIV (56.4%-64.1%) did not utilize these services, indicating a gap in access to digital health solutions. Despite these challenges, there are signs of recovery in service utilization in the post-pandemic period, indicating some resilience within healthcare systems. The study done in South Africa had found that while some regions adapted quickly to the disruptions, others lagged significantly, highlighting disparities in healthcare responses that required additional support. 22 Overall, while initial declines in HIV services were substantial, ongoing efforts were essential to build resilience within healthcare systems and ensure equitable access to HIV care.4,22,23
These findings in our study suggested that residential area, key population type, timing of enrollment, and healthcare channel were influential factors for ART retention at different time points. Furthermore, the COVID-19 crisis led to decreased positivity rates among key and vulnerable populations, along with reduced ART retention and viral load testing. These declines could also be attributed to lockdowns, travel restrictions, strains on health facilities, and disruptions to community-based health programs. Private GP clinics, which were vital for health services, faced limitations in operations due to provider health conditions and medical supply shortages during the crisis. Key populations were aware of COVID-19 risks, and hesitated to visit clinics, resulting in decreased new HIV testing and yield. The routine VL test and other diagnostic tests for PLHIV that were crucial for managing immunity and ART side effects, were disrupted, impacting their health and HIV transmission risks. Travel restrictions and lockdowns prevented timely ART follow-up visits, leading to patients becoming lost to follow-up, and some immunosuppressed patients succumbed to COVID-19 infections. 29
Service providers prioritized their focus to the continuity of ART for existing patients during COVID-19 period, rather than prioritizing outreach activities and new case findings. Providers also used telephone follow-ups, multi-months dispensing (6-8 months) of ART supply, and implementing appointment systems (online or phone) to minimize physical contact. Clinics adapted to COVID-19 prevention settings with plastic-shields/partitions, social distancing, and the provision of PPE items. By May 2020, with decreased COVID-19 rates and eased mobility restrictions, face-to-face visits increased, had implemented extended visit times and enhanced disinfection measures. However, public health sectors faced human resource limitations, impacting ART services with decreased opening hours and closures for lockdown sites. Therefore, linkage to HIV confirmation and linkage to care for ART service were also decreased after HIV positive testing at the provider clinics during the COVID-19 crisis.
The drop-in viral load testing rates post-COVID-19 in both channels could be to several factors. Limited testing centers, supply chain disruptions, and repurposed platforms for COVID-19 diagnostics all contributed to decreased testing. 30 The public sites in Mandalay and Channel 2's viral load lab were the main testing locations. ART patients could be tested viral load in Yangon and Mandalay LPK centers and public health laboratory (PHL) respectively. However, the closure of testing centers during the crisis and the prioritization of the COVID-19 response during that period and struggled with manpower shortage issue during political turmoil by PHL, led to a decrease in testing. The in-house viral load lab in Channel 2 could not operate at full capacity due to a shortage of reagents, as the manufacturer prioritized COVID-19 supplies. This reduction in testing not only affected viral load suppression but also resulted in patients failing to arrive at clinics on time for treatment and follow-up visits. In both crises, the entertainment facilities were closed and many of the key population lost their jobs. Economic struggles, particularly among FSWs, further prioritized income over healthcare. Further investigation was needed to address these barriers and ensure sustained and effective HIV patient care.
In response to the COVID-19 pandemic, Channel 2 implemented several measures to enhance access to treatment. Core group meetings were held to ensure that communication and collaboration among healthcare providers and the operation team were maintained. This allowed for efficient coordination and decision-making during a challenging time. Community-based drug distribution was also facilitated, ensuring that patients could access their medications without having to visit crowded healthcare facilities. This not only improved convenience but also reduced the risk of exposure to the virus. 31 Multi-month dispensing (MMD) was another strategy implemented by Channel 2. This involved providing patients with several months’ worth of medication in one visit, reducing the need for frequent visits to healthcare facilities. Studies had shown that MMD could lead to higher rates of viral load suppression and improved patient adherence, which are essential for successful HIV treatment 31 and data from cohort studies in Malawi 32 and Italy 33 also showed increased rates of VLS during COVID-19 due to introducing patient-centered care models.
In Channel 1, staff received training on infection control measures to protect themselves and their patients from COVID-19. Vaccination efforts were initiated to reduce the risk of infection among healthcare providers. Work-from-home schedules were implemented where possible, minimizing the number of staff present in healthcare facilities and reducing the risk of transmission. To ensure the safety of both providers and patients, essential commodities such as personal protective equipment (PPE) were supplied. This included items like surgical masks and N95 masks, which were crucial in preventing the spread of the virus. Resources like handwashing and social distancing vinyl were being distributed. Clinics were also renovated to create COVID-19 prevention settings, implementing measures like social distancing and handwashing facilities. Additionally, strategies had been devised to prioritize providers handling a high patient load during the COVID-19 situation. This was done to ensure that healthcare facilities could effectively manage the increased demand for services while minimizing the risk of transmission. In order to minimize physical contact between providers and patients, a 3-6-8 monthly ART supply was implemented. This meant that patients received a 3-month supply of medication, followed by subsequent 6-month and 8-month supplies. This reduced the need for frequent visits to healthcare facilities and helped maintain continuity of treatment for patients.
Overall, both Channel 1 and Channel 2 implemented various measures to adapt to the challenges posed by the COVID-19 pandemic. Both channels had implemented virtual appointment systems through online Facebook pages and telephone calls to simplify the appointment scheduling process, decrease waiting times, and improve access to care for patients. These measures prioritized the safety of staff and patients while ensuring uninterrupted access to HIV treatment and care.
Strength and Limitation
The study had few notable strengths and limitations. It effectively analyzed the main gaps in the continuum of HIV care across different phases of the COVID-19 pandemic. Now, we had learnt that staff scheduling, online appointment and social media support, multi-months drug dispensing services for ART medications were useful and powerful tools for HIV services continuity. The inclusion of a large sample size of 10 338 ART clients from 43 healthcare facilities across 7 States and Regions enhanced the reliability and generalizability of the findings. The study design incorporated appropriate statistical methods, which increased the credibility of the results. Longitudinal data analysis (2018-2022) provided valuable insights into trends over time and helped establish causal relationships. Comparing data across the COVID-19 crisis period allowed for the identification of specific impacts of the pandemic on HIV care disparities.
As for the limitations, this was data review without follow-up, which limited the ability to determine the consequences and effectiveness of the strategies implemented. The absence of detailed clinical information in routine data, such as missed visits, hindered the direct assessment of differences between patients who missed viral load tests during the pandemic and those who missed visits before. Missing data on HIV (+) date at the individual level for many clients could have affected the completeness of the analysis. The reduction in the number of HIV tests during the pandemic could have implications for early diagnosis and treatment.
Conclusions
This study provided valuable insights into the impact of the COVID-19 pandemic on HIV services in Myanmar's private care settings. The findings revealed a decrease in ART-retention and VL-testing rates, highlighting the need to address the identified factors influencing ART retention and VL testing. The study also emphasized the importance of implementing strategies to minimize service disruptions and ensure the continuity of essential HIV services. Continued efforts were necessary to bridge the service delivery gaps and ensure the well-being of PLHIV in the face of future challenges.
Footnotes
Acknowledgments
This paper was produced as a result of the contribution of different implementation teams and cross-department collaboration work that worked from the beginning in the strategic thinking, implementation, data analysis and finding sharing. The authors thank fieldworkers who collected study data (program data), and to the colleagues from Sun Community Health (SCH) and Lan Pya Kyel Organization (LPK) for their great contribution to maintain the needed supply.
Author Contributions
The original manuscript draft was prepared by MNTK and SHL. Overall supervision of the study was provided by MMT, HKK, ZMH. The methodology was developed by MMT and MNTK. Analyses were conducted by MNTK and NETP, and both were responsible for visualization of the data. Resources were contributed by HKK, SHL and LHA. All authors reviewed and approved the final manuscript.
Data Availability
The dataset contained programmatic and sensitive clinical, client information and thus, was not publicly available. Data can be made available from the authors upon reasonable request and with permission from the relevant organizations listed above.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study was approved by Population Services International Research Ethics Board (PSI REB), Approval-REB2522022, utilized de-identified and aggregated HIV program data for testing components and de-identified individual data with unique IDs for ART data, adhering to PSI's data protection policy and guidance. Informed consent was not required in this study as there was no direct contact with participants. As this was a retrospective analysis using secondary data, it would have been impractical to collect informed consent. No personal identifiers were used in analysis or reporting.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.