
Abstract
We evaluated Klick, a nurse-led, digitally enabled model of HIV outpatient care, launched in 2020. Klick's smartphone app offers online booking, remote nurse-led consultations, and results. An audit of Klick nurse-led consultations was conducted against BHIVA monitoring guidelines, and nurses were interviewed about their experience. Of 40 Klick patients audited, 4 of 5 BHIVA standards were met: 100% had documented co-medications, smoking history, blood pressure, and viral load data, and 89% received a cardiovascular risk calculation (Targets 97%-90%-90%-90%-90%). Compared to national BHIVA audit findings, Klick performed better across 22 of 24 comparable measures. Nurses safely managed a cohort comprising some complexity (eg, co-morbidities, polypharmacy); no cases were escalated off the pathway, and all were virologically suppressed. Using a digitally supported model, nurses effectively provided safe care to HIV-positive patients with predominantly stable health, enabling consultants to focus on more complex caseloads. Care was comprehensive and person-centered and obtained better outcomes compared to previous national audits.
Introduction
HIV is now a manageable long-term condition for many individuals due to the availability of effective treatment. 1 In light of this, the Joint United Nations Programme on HIV/AIDS proposed 95-95-95 Fast-Track targets: 95% of people living with HIV (PLWH) will know their status, 95% of those will be on antiretroviral therapy (ART), and 95% on ART will be virologically suppressed by 2030. 2 Although targets have not been met globally (86-89-93, 2022), England has achieved them (95-99-98) 3 and since then the Department of Health and Social care has published an ambitious HIV Action Plan, to reach zero HIV transmissions by 2030.4,5 Moreover, 2 of its 4 core themes include: improved access to treatment and retention in care through galvanizing innovations in care models and improvements in the quality of life of PLWH with the delivery of person-centered medicine to support better health outcomes.
Two national audits of HIV outpatient care (2015 and 2018) conducted against the British HIV Association (BHIVA) annual monitoring guidance provide a measure of whether national services deliver effective, comprehensive, and holistic HIV care.6–8 Both audits identified deficiencies in the recording of data and provision of tailored, holistic interventions to PLWH and recommended the use of proformas and other adaptations within healthcare systems/models to drive improvements in care delivery.
Our HIV outpatient service at Chelsea and Westminster Hospitals NHS Foundation Trust (CWFT), London faced local challenges providing further rationale for implementing change and adapting our outpatient model. From an operational and staffing perspective most patients were seen face-to-face, by a consultant physician, with short appointments (20 minutes). Patients scheduled appointments via a call center or while attending clinic, and consultant waiting times were lengthy (up to 6 months). Specialist/senior nurses (Band 7 or 8, Agenda for Change) can conduct routine and complex HIV consultations; however, a minority of consultations in our service were seen by this level of nursing. 9 Junior (Band 6) nurses at CWFT had a lesser defined role, with none delivering routine consultations, and had limited opportunity or structure for training and development. From a governance perspective, our local BHIVA audit findings were similar to national findings. Clinic staff encountered difficulties in securely and remotely communicating with patients which meant results were relayed using inconsistent methods, which at times, risked delays to actioning/managing abnormal results.
Harnessing developments in digital technology and alternative models of care have the potential to address the national and local challenges stated above. A nurse-led, digitally supported model of care, called Klick, was therefore developed and implemented at CWFT Kobler and Dean Street HIV outpatient clinics. Klick was co-designed by patients and clinicians to support PLWH to manage their healthcare, navigate access to the clinic, and communicate with their multidisciplinary team, while also ensuring the service provides comprehensive and holistic care, in keeping with BHIVA guidelines. The model incorporated a structured training framework, to enable Band 6 nurses to remotely deliver care, which included an “annual review,” for patients with stable health. The technology underpinning Klick included a patient app and clinician-facing portal, HealthMachine™ (Avegen).
The aim of this report is to evaluate the nurse-led, digitally supported pathway of care by reviewing the clinical care outcomes, nursing staff perspectives, and operational service changes after Klick's implementation.
Methods
Klick was conceptually created in 2017 during a HIV innovation sprint, funded by ViiV Healthcare. A short proof-of-concept pilot was conducted in 2018 at Kobler clinic, involving 92 patients, and demonstrated feasibility and acceptability, good care outcomes, and service efficiencies. 10 Pilot learnings led to the model being adapted and enhanced, before Klick was re-introduced and made available to all PLWH who accessed Kobler clinic in August 2020 and Dean Street in July 2021, which represent 2 of the largest HIV clinics in Europe.
A mixed-methods, qualitative, and quantitative analysis was conducted to evaluate Klick after its full implementation. This involved an audit of care among PLWH who had experienced nurse-led consultations via Klick (2022) with comparison to the national audit, one-to-one interviews with the Klick nursing team to gain acceptability insights (2023), and a descriptive comparison of pre- and postimplementation service operational metrics. The ASSESS tool (https://publichealth.nyu.edu/w/isee/tools/assess-tool) was utilized to report evaluation findings.
The Klick Model
The Klick app allows PLWH to:
Book, reschedule, and cancel appointments (blood tests, nurse HIV review consultations, and ART injectable treatment/consultations). Scheduling was supported by appointment reminders or notifications to prompt the booking of a future appointment. By accessing nurse-review appointments, patients receive a comprehensive virtual annual review. These are available to PLWH self-selecting as having stable health. Those who are acutely unwell, have complex health needs, or are virologically detectable are encouraged to book a senior doctor appointment via the call center. Complete and submit previsit questionnaires (PVQ) ≤ 10 days before an upcoming nurse-review appointment. PLWH use the PVQ to influence discussion points during the consultation, state their preferred mode of consultation (in-person or telephone), and provide the information required for annual review (eg, smoking status). View results for all routine blood tests and accompanying clinical advice. Receive verifiable care notifications from the clinic. Request emergency oral medication prescription. Review the PVQ while preparing for clinic—to triage, anticipate, or address care needs. Document the consultation on a medical proforma that aligns with BHIVA HIV monitoring guidelines (Figure 1).
8
This includes tools to guide nurses-in-training on what to assess, links to medical risk calculators, and prompts to offer interventions where appropriate. Dispatch general practitioner (GP) letters, automatically generated from the medical proforma. Export documentation to CWFT's electronic patient record system (EPR). Review and release routine test results using a red-amber-green rating to the app, with canned text contextualizing results and providing additional advice/recommendations (Figure 2). Klick nurses manage the blood tests performed for all Klick-registered PLWH, not just those who are medically stable. Send push notifications to the app either individually (personalized care message) or en masse (circulating service updates).
The Klick clinician portal allows staff to:
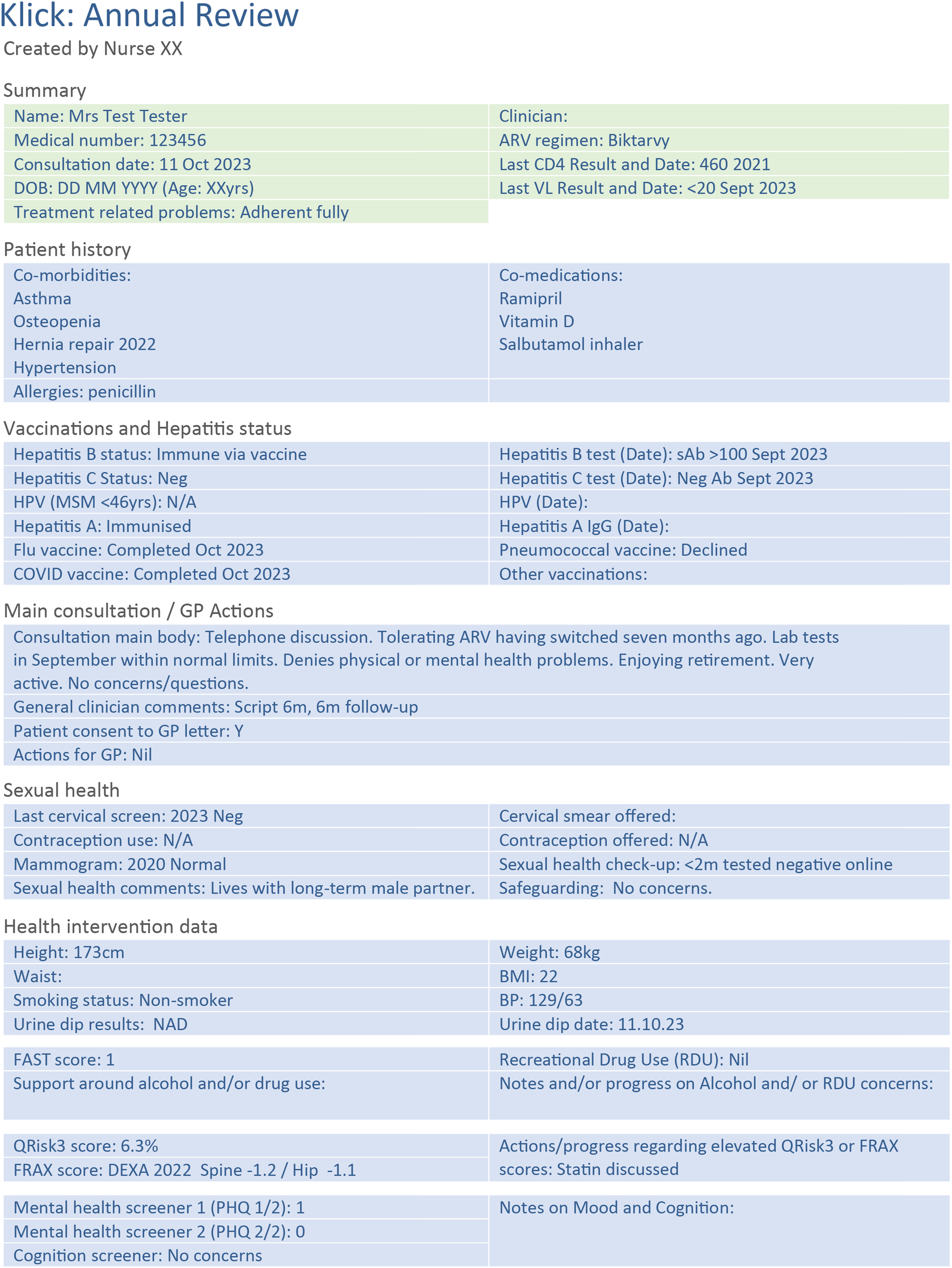
Example of the medical proforma output following a nurse-led consultation.
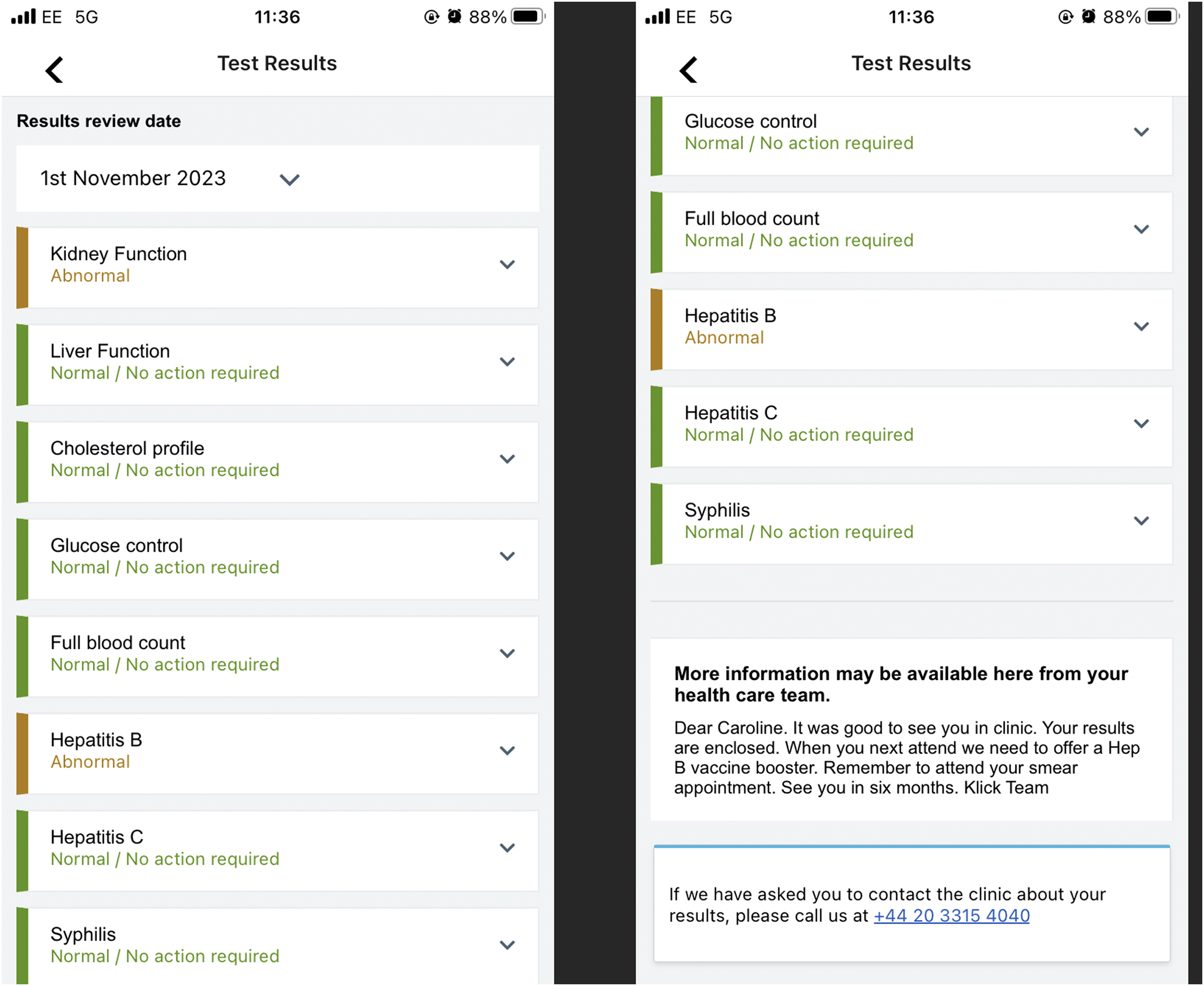
Example of laboratory results view in the patient portal application.
Nurse-Delivered Care
Each Klick nurse is allocated a consultant supervisor, with whom they discuss their clinic list at pre and postclinic meetings to agree on a management plan and obtain prescriptions. Nurses conduct their clinics alongside a consultant-led team. If required (eg, patient is acutely unwell) cases can be discussed with, or escalated to be seen by, the consultant in charge on the day. Nurses aim to obtain accredited (National HIV Nursing Association) NHIVNA/STI Foundation competencies and certifications during their clinical practice, supported by the virtual learning environment provided within the national program.11,12
Onboarding to register and use the Klick app is voluntary so patients have the option to use the Klick pathway or access the outpatient service via the historic (mainstream) processes outlined above. Thus, they can use either pathway exclusively or a blend of both pathways according to their preference and self-perceived needs.
Evaluation Methodology
Clinical Audit
Using the clinician portal and CWFT EPR, the records of 40 Kobler patients who received care via Klick nurse-review clinics between 25 July 2022 and 8 August 2022 were reviewed, by a consultant physician. Audit standards included documentation within the previous 15 months of routine blood tests, vital signs, co-morbidities, co-medications, adherence to ART, sexual and reproductive health history, mental health and cognitive status, cardiovascular disease (CVD) and bone fracture risk profiles, vaccine uptake, and last HIV viral load measurements performed within 9 months. Results were compared with BHIVA HIV monitoring targets and the 2018 BHIVA national audit outcomes that involved 40 PLWH aged ≥50 years. 6
BHIVA's key auditable targets were: 97% on ART should have all current co-medications recorded ≤15 months, 90% PLWH have HIV viral load measured ≤9 months, 90% individuals aged ≥40 years have a 10-year CVD risk calculated ≤3 years, 90% PLWH have a smoking history documented ≤2 years, and 90% have had their blood pressure recorded ≤15 months.
Nurse Interviews
Semistructured, in-depth video interviews were conducted with Klick nurses from both clinics to provide qualitative insights about the acceptability but also the effectiveness and impact of Klick. Interviews were 45 minutes duration, held between October 2022 and June 2023 and conducted by 2 consultants from an independent innovations consultancy (TCC Health). Analysis followed thematic synthesis. Using a theoretical framework of acceptability, themes comprised: affective attitude, ethicality, opportunity costs, perceived effectiveness, and self-efficacy. 13 Analyses were reviewed for intercoder consistency, aligned through discussion and common outcomes extracted. Outcomes are described according to nurse acceptability of Klick, perspectives on core Klick features, and perspectives on patient access.
Service Metrics
Appointment attendance rates (during the auditable period) were calculated at Kobler clinic: Klick-booked junior nurse-review appointments were compared to doctor/senior nurse appointments booked using the mainstream/historic processes. The waiting times for the first available consultant appointments booked via mainstream processes were collected also.
Ethical Approval and Informed Consent
Ethics approval was deemed not to be required by the CWFT research department because the audit, interviews, and service metrics captured were conducted only for service evaluation and not for research purposes. Informed consent was obtained verbally for interview participation to evaluate the Klick service. The consent was provided in the presence of an independent witness.
Results
Between August 2020 and April 2024, 5859 patients had registered to use Klick and 2509 (43%) actively used the app in April 2024, representing >57% of the combined Kobler and Dean Street clinic cohorts. At the time of the audit period August 2022, 1629 Kobler clinic patients had registered for Klick, and 571 had used the app during that month.
Clinical Audit
Of 40 audited patients, the median age was 52 years (range, 29-85), 10% (4 of 40) were female, all were virologically suppressed (HIV-1 RNA <20 copies/mL), and the median CD4+ count was 740 cells/mm3 (range, 175-1274).
All patients (40 of 40) had documented co-medications, smoking history, blood pressure, and viral load data recorded, meeting the BHIVA monitoring targets (97%, 90%, 90%, and 90%, respectively; Figure 3A). Thirty-two patients were aged ≥40 years, and 4 had preexisting CVD; 25 of 28 (89%) of the remaining patients had a CVD risk calculated, falling just below the 90% BHIVA target. Overall, 4 of 5 key BHIVA targets were met.
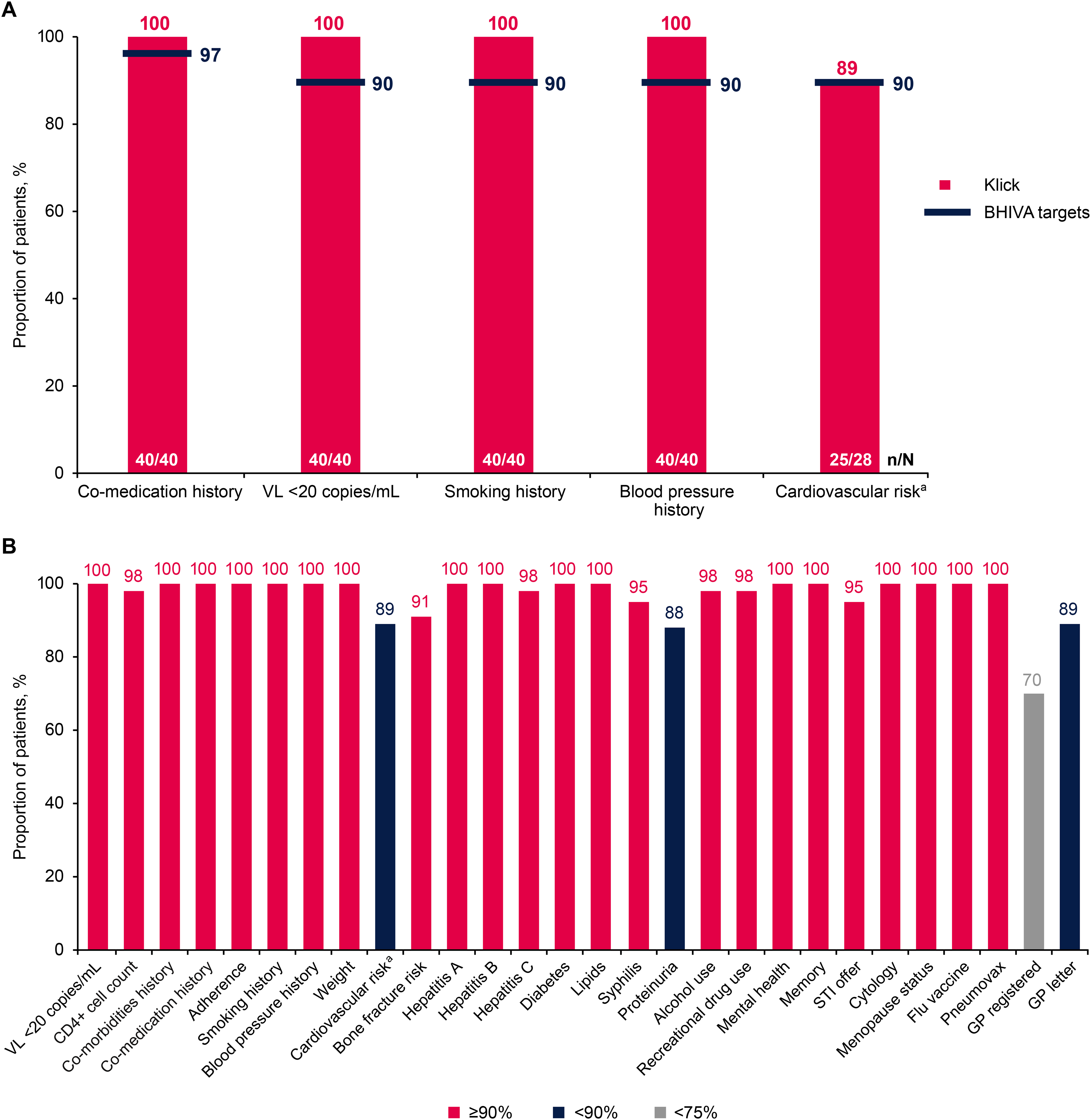
Klick clinical audit results for (A) the 5 key BHIVA HIV monitoring targets and (B) all metrics assessed. BHIVA, British HIV Association; GP, general practitioner; STI, sexually transmitted infection; VL, viral load. aCVD risk was assessed in patients aged ≥40 years without preexisting CVD. 8
Co-morbidities, metabolic parameters, hepatitis status, ART adherence, CD4+ count, vaccine status, sexual and reproductive health, substance and alcohol misuse, bone health, cognition, and mental health measures captured are shown in Figure 3B. All metrics were recorded for >90% of patients, except for documentation of proteinuria (88%), registration with a GP (70%), and the proportion of GP-registered PLWH having a letter dispatched (89%).
Compared to the 2018 UK national audit results (Figure 4), of the 24 comparable metrics assessed, Klick performed better for all metrics except for GP registration (70% vs 97%) and GP letter dispatched (89% vs 90%). Klick performed particularly well for bone fracture risk assessment (91% vs 45%), memory or cognition assessment (100% vs 28%), and CVD risk calculation (89% vs 67%) but also in relation to vaccinations and sexual/reproductive health interventions.
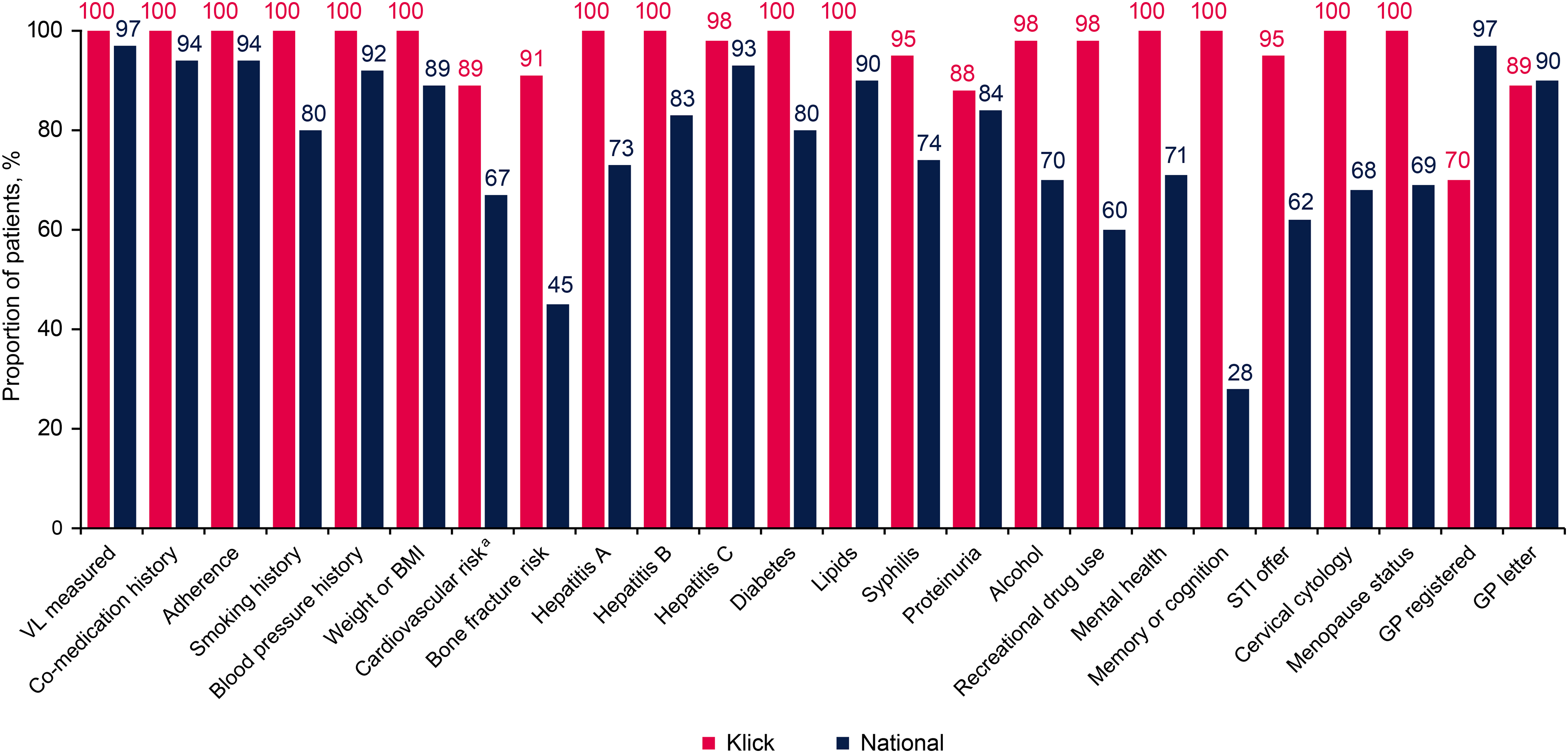
Results from the Klick audit compared with a national audit conducted in 2018. BMI, body mass index; GP, general practitioner; STI, sexually transmitted infection; VL, viral load. aCVD risk was assessed in patients aged ≥40 years without preexisting CVD. 8
Eighty-five percent (34 of 40) of PLWH had ≥1 co-morbidities and 71% had ≥2 (24 of 34). These included hypertension, hyperlipidemia, diabetes, chronic kidney disease, CVD, anxiety/depression, osteoporosis, and obesity. Moreover, 68% (27 of 40) of patients reported polypharmacy (≥2 non-ART medications). No patients were virologically detectable or required escalation to see a consultant. Eight (20%) patients had treatment-switch discussions, with 6 (15%) switching and 2 (5%) declining to switch. Furthermore, 15 of 40 drug–drug interactions (DDIs) were suspected: 11 had been previously documented and actioned; 2 new DDIs were identified and actioned appropriately by the nurse; 2 DDIs were noted by the auditor but were not documented—these were minor and needed no action.
Nursing Interviews
All Klick nurses were invited to interview. Seven verbally consented and were interviewed: 4 of 5 from Kobler clinic and 3 of 3 from Dean Street.
Klick Acceptability
Nurses expressed positivity to Klick-enabled care across the 5 domains of acceptability suggesting that Klick is a well-adopted solution. Table 1 provides domain definition and substantiating quotes. Nurses consistently expressed high satisfaction for the role within Klick and confidence to perform the role. They expressed appreciation for: the opportunity to structure patient care; responsibility for their own patient case load; autonomy to co-ordinate patient support and their ability to provide holistic care. Nurses generally felt that time allocated to the Klick role was sufficient and did not negatively impact other responsibilities within clinic, though managing postconsultation actions for complex cases could be challenging. Nurses described high levels of support from multidisciplinary colleagues.
Domain Descriptions for Acceptability and Nurse Quotes.
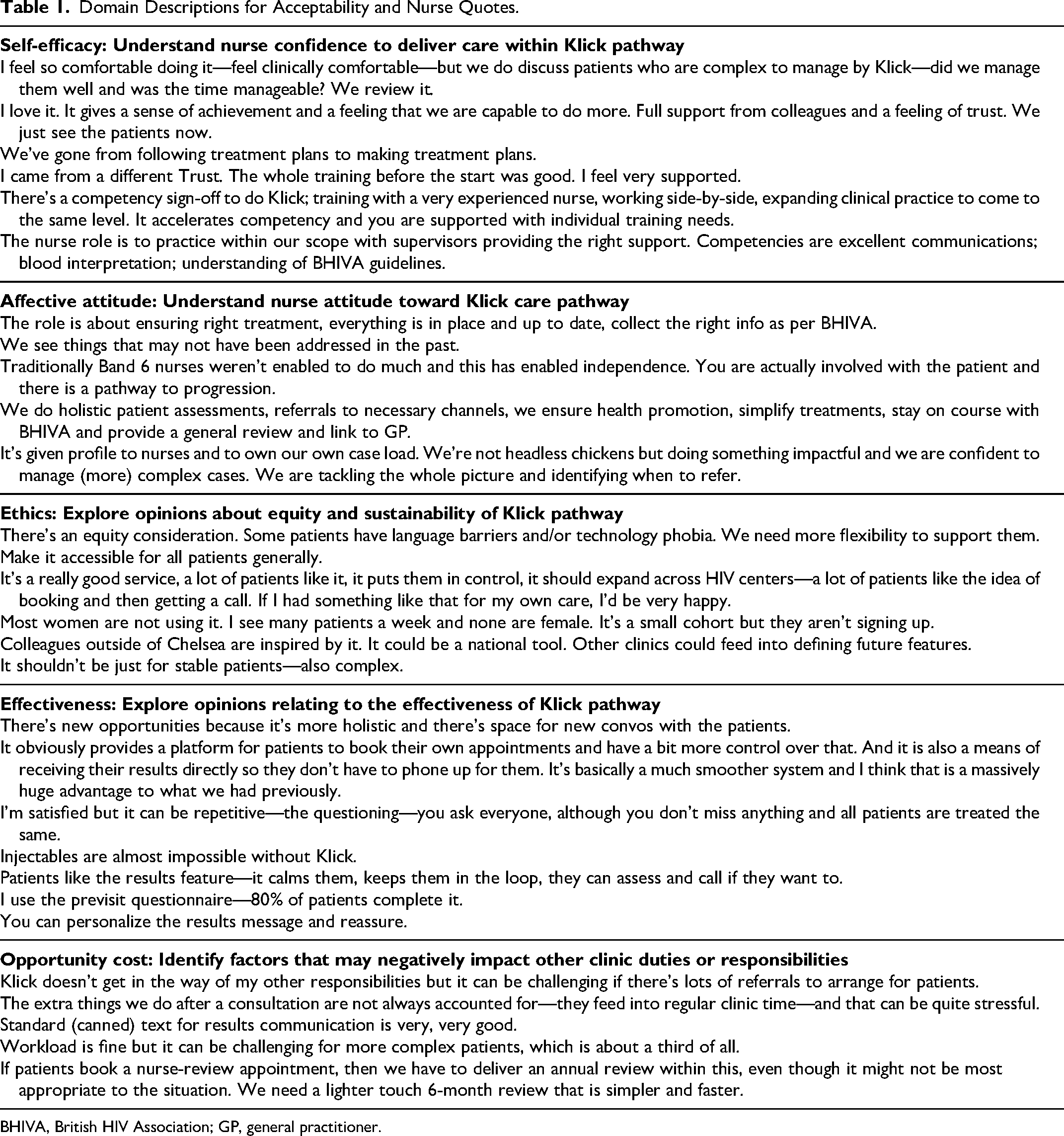
BHIVA, British HIV Association; GP, general practitioner.
Core Klick Features
Nurses were largely positive about all Klick pathway features and found them effective. They reported most patients complete the PVQ and responses were useful for clinic preparation. The digital communication tools helped reduce outgoing calls or letter dictation. Nurses expressed high satisfaction with the results feature and reported the functionality to be user-friendly. To optimize efficiencies and patient experience nurses suggested integrating the medical proforma and PVQ, adapting both documents to increase personalization, improved automation of results, and provision of more appointment types to respond to the diversity of patient needs.
Patient Access
Nurses reported that most patients find Klick beneficial but some may use Klick as a de facto way of engaging with the service, rather than for accessing the specific/intended services offered by Klick. They felt that the Klick service was appropriate for all patient types and identified a need for intervention/activities to encourage uptake in patient populations who may typically avoid digitally enabled services and/or interact with the clinical team with lower frequency than the population as a whole. Nurses felt the onboarding process was structured.
They reported managing some complex patients but feeling confident and supported to do so. Nurse-reported findings between Kobler clinic and Dean Street clinics were broadly similar with some variation attributable to underlining service characteristics, that is, more junior nurse-led clinics at Kobler, whereas Dean Street focused on efficiency of appointment utilization.
Operational Metrics
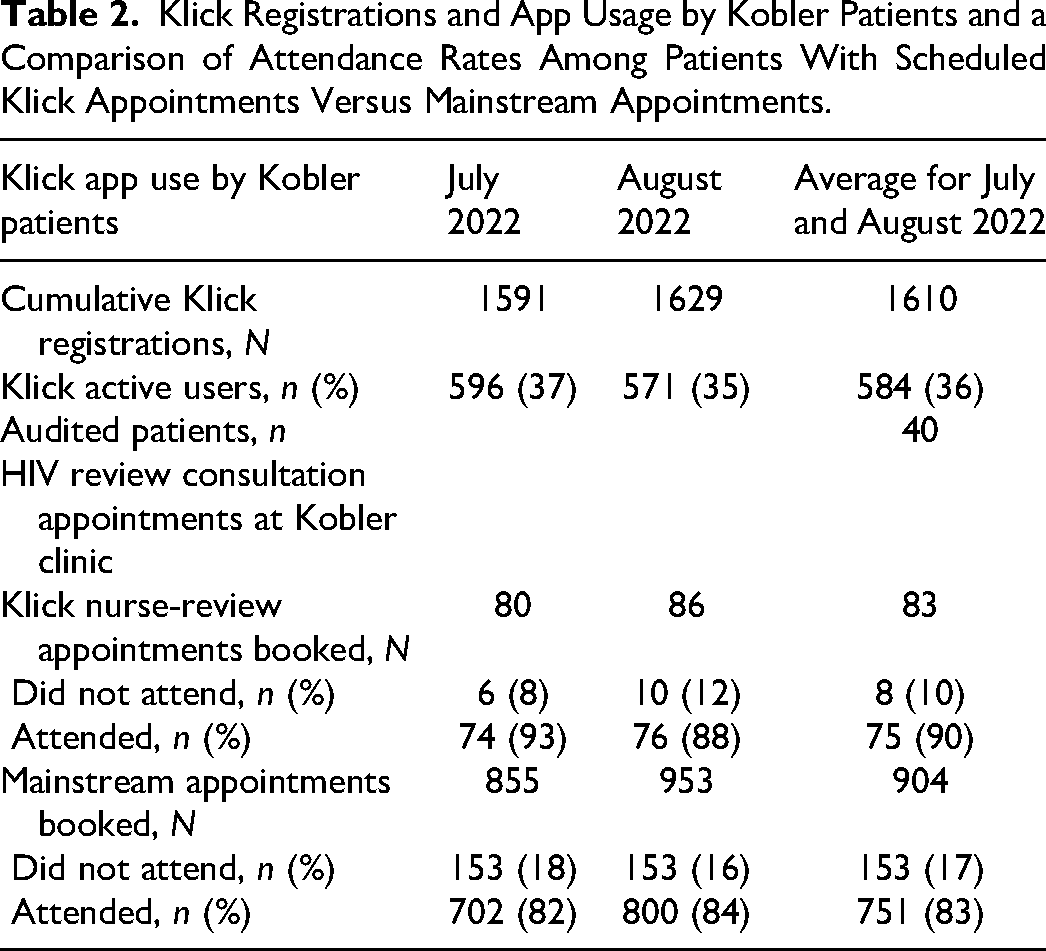
Eight nurses have received Klick training at the Kobler clinic to date, and during August 2022, 5 Band 6 nurses were conducting 7 to 8 clinics/week. The mean waiting time to see a Kobler consultant was 18 weeks pre-Klick in 2019 to 8 weeks post-Klick in August 2022 and these appointments had also extended from 20 to 30 minutes/patient, respectively. During the audited period, 10% (8 of 83) of Klick patients did not attend or respond to telephone contact (DNA) at their scheduled nurse-review appointed time. This compares with 17% (153 of 904) who had booked their appointment with a doctor/senior nurse via mainstream methods, equating to a 41% reduction in DNA rates among the Klick pathway (Table 2).
Klick Registrations and App Usage by Kobler Patients and a Comparison of Attendance Rates Among Patients With Scheduled Klick Appointments Versus Mainstream Appointments.
Discussion
UK HIV services face several challenges. The growing and aging HIV-positive population incurs increased care costs due to co-morbidities, polypharmacy, and higher proportions taking ART. 14 Nationally the sector has also experienced disruption due to major healthcare reforms and commissioning rearrangements for sexual health and HIV care and prevention services (Health and Social Care Act 2012). Moving to separately commissioned pathways that involve regular tendering of contracts by local authorities has been associated with disruption and fragmentation of some HIV services, particularly those that were previously co-located within sexual health services. 15 Retention and recruitment of the HIV workforce have been negatively impacted by these changes and exacerbated further by changes to the genitourinary medicine and HIV specialty curriculum (dual accreditation).16,17 Compared to other countries, the UK already faces strikingly low levels of doctors and is heavily reliant on foreign-trained staff. 18
Effective and novel strategies are required to ensure that cost-efficient HIV care provided by a suitably skilled workforce can be sustained in this climate. Utilizing nursing professionals or other multidisciplinary team members represents one potential solution. Both BHIVA standards of care and the Select Commons Committee report on HIV/AIDS in the UK have endorsed and recommended the adoption of more nurse-led clinics.19,20 In many low-income countries, shifting tasks from physicians to nurses and nurse-led services has addressed physician shortages, increased capacity within heavily burdened services, and improved access to HIV care and ART.21–24 In the UK, the contribution of nursing to HIV care has been reported and led to high patient retention rates and sustained viral suppression, comparable to rates seen with physician-led care.25,26 However, there is substantial variability in specialist nursing roles and some roles are underdeveloped within their service.26,27 Furthermore, of UK HIV clinics that participated in a 2016 survey, 0 of 75 (0%) were nurse-led only and 25 of 75 (33%) provided a combination of being doctor- and nurse-led. 28
The Klick outpatient model aimed to amplify the role and contribution made by the HIV nursing team. This report showed they provided comprehensive clinical care during their consultations, achieving 4 of 5 BHIVA targets and demonstrated excellent performance compared to the standard-of-care provided by doctors and nurses in outpatient HIV services nationally.
The Klick nurses managed primarily medically stable patients but also some with complex needs under the supervision of a consultant: Klick patients self-certified as “medically stable” but most had polypharmacy, several required ART switches, and 85% had ≥1 co-morbidity, a higher proportion than reported in the national audit (29%), all of which demonstrate a level of complexity. Piercy et al assessed the specific contributions of HIV care delivered by specialist nurses and our findings provide evidence that more junior nurses provided similar contributions. 27 Upskilling the junior nursing workforce to manage less complex cohorts has the potential to help address the capacity and workforce sustainability pressures facing UK services.
The digital components of Klick were perceived by nurses to be effective and impactful to patients and staff. The PVQ was used to capture annual review monitoring requirements and anticipate and/or triage care needs, minimizing the number of on-the-day escalations to the consultant. The medical proforma likely contributed to the further completeness of audit data collected and intervention offer rates. Prepopulated proforma, canned text for results provision, and autogeneration of GP letters helped minimize the clinic-associated administration burden.
The evaluation findings suggest the Band 6 nurses were able to participate in a supported, training and development pathway that led to them developing the requisite clinical skills to manage their own cohort of medically stable patients and structure how aspects of care were delivered in the clinic. This resulted in job satisfaction and a degree of professional autonomy, and they were able to work toward and complete national qualifications during their weekly clinics. They found utility in the training features incorporated within the clinician portal, reported confidence in managing their own patient cohort, and felt well supported by the consultant-led team when seeing patients with more complex needs. The team were invested to further optimize the pathway, proposing opportunities to enhance the service for patients and staff. These are all factors that help bolster morale, improve staff retention and promotion prospects, and strengthen relationships with patients and clinical colleagues, all features that have been difficult to quantify for this report.
Although cost-benefit was not a primary objective in the design of Klick, the model likely contributed to alleviating resource and capacity pressures, by delivering additional Kobler clinics and securely providing results for all blood appointments booked online. A reduction in waiting times and extension of appointment length was observed for consultant clinics in 2022, despite no growth in Kobler consultant establishment since 2020 and an increase in the cohort size of both clinics. This suggests consultants can spend longer seeing patients with more complex/urgent healthcare needs in a timelier manner. Patient engagement rates were 41% higher for Klick-booked appointments compared to mainstream booking processes, which is likely a result of allowing patients to directly book/reschedule their appointments online. Klick technology proved advantageous during the COVID-19 pandemic because Klick staff could rapidly adapt to conducting consultations and communicating with patients remotely.
The evaluation had a number of limitations. The experience and engagement of PLWH have not been reported because this has been submitted for publication separately. The clinical audit involved small numbers and was not conducted at Dean Street because the site only launched with Klick less than 12 months before the audit, and staff did not initially use the Klick medical proforma. We plan to re-audit Klick-registered versus Klick-unregistered PLWH at both sites in due course. Pre-Klick service metric data was available only for Kobler clinic because of the research carried out during the sprint design and pilot evaluation, therefore Dean Street service metrics have not been presented. Other factors that could potentially have contributed to the changes in operational metrics observed at Kobler clinic have not been reported (eg, clinics provided by other multidisciplinary team members, service adaptations during the pandemic, recommended frequency intervals of appointments/year).
This report showed that by adopting a nurse-led, digitally assisted model of care the service has demonstrated improvements in the delivery of comprehensive, holistic patient-centered care and supported the mobilization and upskilling of a junior nursing workforce to manage PLWH with stable health. Service pressures have eased since launch with consultants being able to prioritize care for patients with more complex healthcare needs. The Klick model has been rolled out at 2 further CWFT HIV outpatient sites (October 2023 and March 2024). Using similar models of care in other large HIV outpatient settings has the potential to support the UK's commitment to eliminating HIV as a public health problem and enhance the experience of both PLWH and the outpatient multidisciplinary team that serves them.
Footnotes
Acknowledgments
The authors and Klick team would like to thank the staff and patients at Kobler and 56 Dean Street clinics for their time and feedback in the design, development, and growth of Klick. They would also like to thank the technology developer Avegen and TCC Health. Assistance with manuscript submission was provided by Paula Farmer, MedThink SciCom, and funded by ViiV Healthcare. This assistance was authorized by the authors, and the authors approved all statements and declarations included in the manuscript.
Declaration of Conflicting Interests
SD, RW, YF-Y, SO-A, and CR have no conflicts of interest. AM is an employee of ViiV Healthcare and may own stock in GSK. CA received travel bursaries and conference registration fees from and participated in advisory boards for ViiV Healthcare and has appeared in peer support information videos for Gilead Sciences. DA participated in advisory boards for ViiV Healthcare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ViiV Healthcare. The funder did not have a role in the design of the study or in the analysis or interpretation of data.