1015Men and Boys Are Not Hard to Reach, They Are Hardly Reached: Adolescent Boys and Young Men's Preferences for Integrated PrEP Delivery and Uptake in Unconventional Spaces in Tshwane, South Africa
Ndumiso Madubela (presenting)
1
1NACOSA, Cape Town, South Africa
Introduction: Adolescent Boys and young men (ABYM) are not actively pursued for HIV prevention and treatment in South Africa. Consequently, they remain at high risk of HIV acquisition and transmission. This has negative implications for the vulnerability of adolescent and young people (AYP) to HIV and AIDS. In order to develop and integrate HIV prevention programs, better aligned HTS screening and PrEP delivery for Adolescent boys and Young men is needed.
Description: NACOSA is implementing an HIV Prevention programme (My Journey) that provides behavioural, biomedical and structural tailored-services that are human rights-based and evidence-informed. The program provides AYP aged 15–24 years, specifically ABYM gender-responsive service delivery options. Interventions such as the ABYM dialogues in unconventional spaces (sport grounds, transport hubs, taverns etc) through this the program is able to enrol at risk ABYM in spaces they frequent, offer tailored services to this neglected population.
Lessons Learned: Overall, in Tshwane region 1, n = 5 261 ABYM enrolled Between April 2022 -February 2023; 7661 ABYM received an HIV screening and know their results. 1370 beneficiaries were initiated on PrEP, and 36 were already using PrEP; 86 of these ABYM were under 15 years. Most (2 464) were between the ages of 15–19 years. What we learnt was that the lack of knowledge among vulnerable ABYM and the health system's inadequacy at providing targeted services results in the poor uptake of Sexual and Reproductive Health (SRH) services, mainly testing on HIV and sexually transmitted infections (STI).
Recommendations: Best-aligned PrEP delivery for Adolescent boys and Young men include peer group adherence support and male positive/friendly health spaces. To ensure that delivery models influence positive demand for HTS and PrEP, HIV prevention programs should focus on differentiated, gender-responsive service delivery options. Men and Boys favor accessing SRHS services from mobile clinics situated in taverns, social hubs and sports fields, all spaces that these populations frequently navigate.
1025Chemsex in PrEP Users of a Community-Based Center PrEP
Point Plus (PPP)
Sandro Mattioli (presenting)1, Lorenzo Badia2
1PLUS aps, Bologna, Italy
2Azienda Unità Sanitaria Locale di Imola, Bologna, Italy
Background: Chemsex, a phenomenon that concerns MSM in particular, is on the rise in Bologna, too. Based on the current narrative, there could be a correlation between the use of PrEP, the increase in chemsex and the increase in STIs.
Method: The analysis was performed on risk exposure, substance use and frequency, on the basis of online questionnaires completed by PPP users every 3 months, and from the results of STIs tests performed at the PPP. All users were enrolled in the observational study “Sexcheck” in 2021–2022. 99% of the sample are MSM in PrEP who live in central-northern Italy, median age is 39 years, some are chem users.
Results: In 2021, we had 46 chem users out of 150 prep users (30.7%) who rose to 165 2022, of which 63 (38%) chem users. In 2022, the no. of sexual partners among chem users increased from 38.5% to 47.5%. Risky sexual practices have also grown: group sex, fisting, UAI, no condoms use (see table).
The most used substances are mephedrone – used in various ways (see table) and GHB. On STIs in the chem user group (see table), in 2022 we observe 38.6% of NG and 36.4% of CT both stationaries compared to 2021; syphilis at 25% in 2022, was at 22.2% in 2021. The median age of users who received at least 1 of this diagnosis was 36 in 2022, 41 in 2021. In the group of PrEP users who do not use chem, in 2022 we observe 31% of NG (it was 40% in 2021), 50.8% of CT (it was 40% in 2021), 18% of syphilis (it was 19.2% in 2021)
Conclusion: We observe a decline in the use of mephedrone and GHB. STIs are stable. Exposure to risk remains high: number of sexual partners, UAI and group sex are growing. Demand for PrEP's growing. Data confirms the importance of these users being tested for STIs.
1034Four Years of PrEP Use; Results on Sexual Behaviour and STIs from the AMPrEP Demonstration Project Among MSM in Amsterdam, Netherlands
Mark A.M. van den Elshout (presenting)1, Eline Wijstma2, Vita Jongen2, Liza Coyer2, Anders Boyd2, Udi Davidovich2, Henry J.C. de Vries3, Maria Prins2, Maarten Schim van de Loeff2, Elske Hoornenborg2
1Public Health Service of the Utrecht Region, Utrecht, Netherlands
2Public Health Service of Amsterdam, Amsterdam, Netherlands
3University of Amsterdam, Amsterdam, Netherlands
Background: An increasing number of countries are currently implementing or scaling-up PrEP care. With the introduction of PrEP, there was apprehension about possible risk compensation. To inform sexual health prevention counseling and STI screening within PrEP programmes, we aimed to study long-term trends in sexual behavior and STIs among PrEP-using MSM and transgender women.
Method: The Amsterdam PrEP (AMPrEP) demonstration project provided oral daily (dPrEP) and event-driven (edPrEP) PrEP to MSM and transgender women in 2015–2020. Participants could choose their PrEP regimen, and switch at each three-month study visit. STI testing occurred at – and if needed in between – study visits. We assessed changes in the number of sex partners and condomless anal sex acts with casual partners (CAS) using negative binomial regression. We assessed changes in incidence rates (IR) of any STI (ie, chlamydia, gonorrhea, or infectious syphilis) over four years since PrEP initiation using Poisson regression. Incident cases of HIV are described.
Results: 367 participants (365 MSM) started PrEP and contributed 1249 person-years (PY). Adjusted rate ratio (aRR) of number of sex partners was 0.89/year (95% CI 0.86–0.92), aRR of CAS acts with casual partners was 0.98/year (95% CI 0.94–1.01) (Figure 1). IR of any STI was 87/100 PY (95% CI 82–93). IR of any STI did not change over time for both dPrEP and edPrEP users (Figure 2). However, IRs of chlamydia and gonorrhea decreased slightly in dPrEP users. Two HIV cases were diagnosed during the first year on PrEP.
Figure 1. Sexual behaviour during the first four years on PrEP, AMPrEP, The Netherlands, 2015-2020.
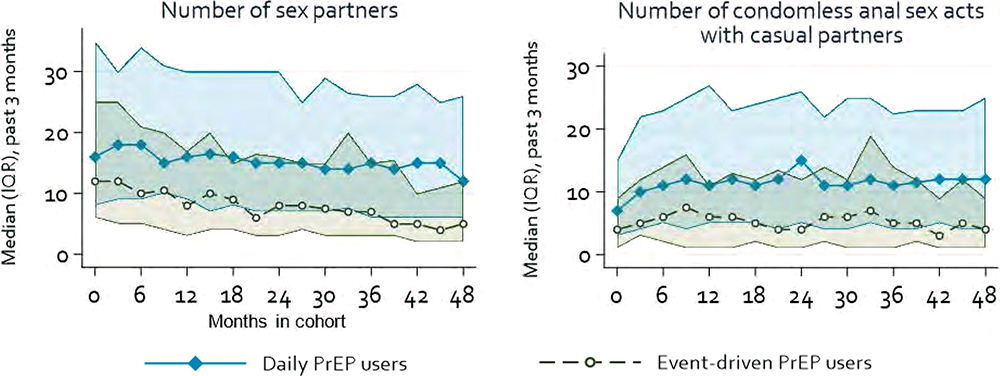
AMPrEP: Amsterdam PrEP demonstration project; IQR: interquatile range; PrEP: pre-exposure prophylaxis

1036Innovative Practices in Community Partnerships: A HOPWA Intervention
Keristen Mazyck (presenting)1, Tawana Philpott Brown1
1Roper St. Francis Healthcare, Charleston, SC, USA
Introduction: Public health services (GGD) in The Netherlands are committed to serve communities who experience barriers in accessing regular healthcare. Some notable barriers are lack of information about available services, lack of confidence in the facilities and staff, and sociocultural constraints related to gender, age, beliefs, and cultural preferences. Additionally, obstacles such as accessibility of the nearest health facility also pose significant challenges.
The GGD's Centre for Sexual Health (CSH) focuses on populations who have higher incidences of sexually transmitted infections (STIs) or who are more vulnerable to poorer sexual health outcomes. However, some of these populations remain underrepresented among people seeking care at the CSH. Therefore, we aim to apply additional strategies to better reach underserved communities.
Description: Strategies to reach underserved communities currently mostly focus on triage, meaning the thresholds to access services are lowered for people with specific characteristics. A limitation of this passive strategy is that it merely selects at the gate and does not directly influence who reaches that gate. Other – more active – strategies, summarized as outreach, focus on reaching these communities in a way and a place that is convenient for these communities. This may familiarize communities and the network of organizations surrounding them with the CSH's staff and services on offer and can facilitate peer-driven uptake.
Lessons Learned: To overcome the defined barriers, it is essential to educate staff in recognizing and respecting (cultural) diversity within target communities to ensure services are tailored to relevant norms, beliefs, and practices. This promotes a sense of inclusivity, increases trust in healthcare providers, and encourages greater utilization of CSH and regular healthcare services.
Recommendations: Involving service users in CSH programme evaluation improves service relevance and effectiveness. Institutions should plan for extended timeframes and allocate sufficient resources for successful programme implementation. Including underserved groups in health research promotes equitable service delivery. Diverse population representation leads to a better understanding of health needs and preferences.
1040The Use of a Community Panel to Design PrEP Awareness Campaigns That Engage Black, Asian, and Minority Ethnic Groups
Yvonne Richards (presenting)1, Joseph Tanzer
1BHA for Equality, Manchester, England, United Kingdom
Background: BHA for Equality, a charity working across the North of England, supported and developed a community panel to inform our PrEP awareness campaign made of local community members from Black, Asian, and minority ethnic communities. This ongoing community panel designed HIV prevention campaigns and tailored outreach methods and messaging. Several of the members have since volunteered with BHA and took part in the outreach campaigns.
Method: BHA for Equality recruited local people from Black, Asian, and Ethnic minoritized communities including people from local businesses, influencers, activists and social workers living across Greater Manchester to develop a PrEP community panel. The community panel was developed to raise awareness of PrEP among underserved communities. The panel met to discuss the barriers faced by Black and minoritized communities in accessing PrEP and designed tailored messaging and outreach methods to counteract these barriers.
Results: Awareness and take-up of PrEP among Black and minoritized communities is low. There is also a lack of trust in PrEP due to historical racism and exclusion within healthcare and clinical trials. Communities are therefore more likely to trust health information that comes from people within their own communities whom they respect. Also, due to HIV stigma, communities are more likely to engage in outreach activities and prevention messages if they are delivered in a more holistic method. HIV prevention campaigns need to be designed by the communities they wish to reach, and coproduction needs to happen at every level of design.
1049ART Adherence Experiences of People Living with HIV Receiving a Point-of-Care Adherence Assay Versus Standard of Care: A Qualitative Data from Cape Town, South Africa
Abenathi Mcinziba (presenting)1, Dillon Wademan1, Lario Viljoen1, Hanlie Myburgh1, Eric Decloedt1, Catherine Orrell2, Lauren Jennings2, Gert van Zyl1, Monica Gandhi3, Marije van Schalkwyk1, Graeme Hoddinott1, Graeme Hoddinott1
1Stellenbosch University, Cape Town, South Africa
2Desmond Tutu HIV Foundation, Cape Town, South Africa
3University of California-San Francisco, San Francisco, CA, USA
Background: A newly developed Urine Tenofovir Rapid Assay (UTRA) assesses and tests tenofovir in urine at point-of-care and immediately responds to adherence levels of people living with HIV (PLHIV). A qualitative evaluation nested in a pilot randomized controlled trial investigating the acceptability of UTRA, compares the adherence experiences of PLHIV receiving this point-of-care adherence intervention versus standard of care.
Method: We completed three series of longitudinal in-depth qualitative interviews with 25 PLHIV (a total of 75 interviews) at a primary health facility, Gugulethu, Cape Town, South Africa. Participants at risk of virologic failure and receiving a tenofovir-based antiretroviral therapy (ART) regimen were purposively sub-sampled by arm (1:1 intervention vs control) from the parent trial, for diversity in age and gender, and rich-case sampling. Data collection started in May 2022 and completed in May 2023. Data analysis involves descriptive summaries of key emergent themes with illustrative case examples.
Results: Participants from both arms reported that obstacles to ART adherence were food insecurity, side effects of ART medication, alcohol consumption, stress of daily life challenges, and lack of adequate adherence support. Participants in the intervention arm reported that being tested and informed about their adherence performance in real-time served as a motivation for accountability to take treatment consistently and created a platform for adherence discussions with health workers on how to overcome adherence barriers. Participants in the control arm reported that they rely on relatives for adherence support and accountability because there is limited time to have adherence discussions with health workers in their busy clinic.
Conclusion: Overall, PLHIV in the intervention arm, through immediate results from the assay and education from counselling, managed to find ways to overcome some of the barriers to adherence compared to those in the control arm.
1050Bacterial Sexually Transmitted Infections Are Concentrated in Subpopulations of MSM Using HIV Pre-Exposure Prophylaxis in Amsterdam, the Netherlands: An Analysis of Longitudinal Trajectories
Vita Jongen (presenting)1, Maarten Schim van de Loeff1, Mark A.M. van den Elshout2, Eline Wijstma1, Liza Coyer1, Udi Davidovich1, Henry J.C. de Vries3, Maria Prins1, Elske Hoornenborg1
1Public Health Service Amsterdam, Amsterdam, Netherlands
2Public Health Service of the Utrecht Region, Utrecht, Netherlands
3University of Amsterdam, Amsterdam, Netherlands
Background: Earlier studies have shown varying trends in incidence of sexually transmitted infections (STI) among individuals using HIV pre-exposure prophylaxis (PrEP). However, little is known on the individual trajectories of STI incidence. We assessed trajectories of STI incidence to inform PrEP monitoring policy and guidelines.
Method: We screened participants from the AMPrEP demonstration project (2015–2020) for urogenital, anal, and pharyngeal chlamydia and gonorrhea, and syphilis every 3 months. Participants could attend additional STI screening if needed. We used group-based trajectory modelling to identify trajectories of STI incidence within individuals over time and determinants of belonging to a trajectory group. We calculated cumulative proportions of STIs within STI trajectory groups.
Results: We included 366 participants (median follow-up time = 3.7 years [IQR 3.5–3.7]). 99% of participants identified as male and median age at baseline was 40 years [IQR 32–48]. We identified three distinct trajectories of STI incidence: (1) participants who had a mean of approximately 0.1 STIs per 3-months (“low overall”, 52% of the population), (2) participants with a mean 0.4 STI per 3-months (“medium overall”, 43%), and (3) participants with high and fluctuating (between 0.3–1 STIs per 3-months) STI incidence (“high and fluctuating”, 5%). Participants in the “low overall” trajectory were significantly older and reported less chemsex and condomless anal sex with casual partners than participants in the other trajectories. Participants in the “high and fluctuating” and “medium overall” groups accounted for respectively 23% and 64% of all STIs observed during follow-up.
Conclusion: We showed that STI incidence was concentrated in subpopulations of PrEP users who were younger, had more chemsex and condomless anal sex. Screening frequency for STIs could be reduced for subpopulations with low risk for incident STIs.
1052Assessing the HIV Care Continuum Among Transgender Women in the Netherlands: Does HIV Care Retention Differ from Men Who Have Sex with Men?
Vita Jongen (presenting)1, Ceranza Daans1, Ard van Sighem2, Maarten Schim van de Loeff1, Kris Hage1, Camiel Welling1, Alex von Vaupel-Klein1, Martin den Heijer3, Edgar Peters3, Marc van der Valk3, Peter Reiss3, Maria Prins1, Elske Hoornenborg1
1Public Health Service Amsterdam, Amsterdam, Netherlands
2Stichting HIV Monitoring, Amsterdam, Netherlands
3Amsterdam UMC, Amsterdam, Netherlands
Background: Transgender women are at increased risk of acquiring HIV. Earlier studies reported lower rates of retention in HIV care, antiretroviral therapy uptake, adherence and viral suppression. We compared the stages of the HIV care continuum of transgender women with those of men who have sex with men (MSM) in the Netherlands. In addition, we assessed new HIV diagnoses and late presentation between 2011 and 2021, as well as loss-to-care.
Method: Using data from the Dutch national ATHENA cohort, we assessed linkage to and retention in care, ART use, and viral suppression among transgender women and MSM for each year between 2011 and 2021. We assessed trends in new HIV diagnoses between 2011 and 2021, in addition to late presentation (CD4 count of <350 cells/µl and/or AIDS at HIV diagnosis). Difference in loss-to-care over time between transgender women and MSM was assessed using Poisson regression.
Results: 15,685 individuals attended at least one HIV clinical visit: 237 (2%) transgender women and 15,448 (98%) MSM. Every year, a higher proportion of transgender women than MSM was not virally suppressed. In 2021, 186 of 215 (87%) transgender women were virally suppressed, compared to 12,761 of 13,669 (93%) MSM (p < 0.001). The number of new HIV diagnoses decreased between 2011 and 2021 for both transgender women (ptrend < 0.001) and MSM (ptrend = 0.018). While late presentation was common and increased over time for MSM (ptrend = 0.011), no increase was seen for transgender women (ptrend = 0.396). Transgender women were 1.89 (95%CI = 1.28–2.79) more likely to be lost-to-care (See figure.).

Conclusion: Between 2011 and 2021, the HIV care continuum across all stages was less successful for transgender women than for MSM. Late presentation was common but did not increase over time for transgender women. Identifying remaining barriers to HIV care and retention for transgender women will be crucial to further optimize their HIV care continuum.
1061Impact of Hepatitis C Virus (HCV) Screening in an Emergency Department: Implementation of the FOCUS Program in Almería, Spain
Diogo Medina (presenting)1, Anny Camelo-Castillo2, Teresa Jordán Madrid2, Antonio Duarte Carazo2, Manuel Rodríguez Marezca2, Teresa Cabezas Fernandez2, Alba Carrodeguas1, Jose Vega Saenz2, Marta Casado Martin2
1Gilead Sciences, Madrid, Spain
2Hospital Universitario Torrecárdenas, Almería, Spain
Background: A 2017–2018 serosurvey by the Spanish Ministry of Health estimated a 0.22% hepatitis C virus (HCV) active infection prevalence among the general population, with 29.4% unknown infections. Emergency Departments (ED) often act as safety nets due to health equity issues for key populations affected by viral hepatitis, as they often lack optimal links with their primary care providers. We aimed to evaluate HCV screening efficacy in the ED of Torrecárdenas University Hospital, in Almería, Spain.
Method: We implemented opportunistic HCV screening in the ED using existing infrastructure and staff. Patients aged 18 to 69 were eligible for testing if they did not have a known diagnosis or test performed in the previous year and required blood tests at the current ED visit. We used the LIAISON®X- Diasorin assay for HCV antibodies (anti-HCV) and the Roche Cobas® 6800 for viral RNA (HCV RNA) in the same specimen. Appropriate follow-up or discharge was given regardless of test results. We contacted positive patients to ensure linkage to care.
Results: We screened 12,651 patients from August 2021 to April 2023, finding 213 (1.68%) anti-HCV positive patients (average age of 56, 76% male) and 45 (0.35%) HCV RNA positive patients (79% male). We identified risk exposures in 49% of viremic patients’ records: injection or inhaled drug use (44%), history of incarceration (13%), origin from countries with medium or high HCV prevalence (9%), and HIV or HBV co-infection (2%). 75% of viremic patients had previously visited ED, and as of reporting, 20 patients have started antiviral treatment.
Conclusion: Undocumented HCV infection among our population is almost twice that estimated in the Spanish population. Hepatitis C screening in EDs is an effective strategy and should be considered in more hospitals.
1069Multilingual Action Week Against Hepatitis C: Enhancing Immigrant Health Access in Germany
Alaa Edin Abdin (presenting)1, Adriane Skaletz-Rorowski (presenting)1
1WIR – Walk In Ruhr, Bochum, Germany
Introduction: Hepatitis C poses a public health concern in Germany, with an estimated 189.000 individuals living with chronic infection [1], often unaware of their status. Immigrants and individuals with a history of drug use are particularly vulnerable to Hep-C due to unsafe medical practices, sharing contaminated needles, or through sexual contact. Recognizing this, the WIR- Center in Bochum, a Fast-Track-City in Germany, organized a multilingual action week addressing barriers to immigrant healthcare access.
[1] Lancet Gastroenterol Hepatol 2022; 7(5):396–415
Description: Over 70 immigrants participated, seeking competent advice and undergoing Hep-C testing. Serdar Yüksel, a member of the State Parliament in Bochum, provided patronage and collaborative support was received from various stakeholders namely -St. Elisabeth Hospital, Public Health-Dep. of Bochum, Municipal Integration Centre, Middle East Humanitarian Solidarity Association, AWO Ruhr-Mitte, Ethno-Medical Centre e. V., and the bio-pharmaceutical company AbbVie Germany, a partner within the framework of the PLUS-health-initiative. The interpreters played a crucial role in facilitating effective communication, and a safe environment was created for women at WIR.
Lessons Learned: The multilingual action week successfully addressed language and cultural barriers by offering free consultations, tests, and language support. Anonymity, along with the involvement of interpreters and the provision of a women-friendly environment, played a crucial role in facilitating effective communication.
Recommendations: To eliminate Hep-C, especially among immigrants without health insurance, comprehensive strategies are necessary. These should include targeted outreach, accessible free testing, integration of diverse communities, ensuring anonymity, creating women-friendly environments, and providing personalized support among with expanding similar initiatives throughout Germany by collaborating with local healthcare-providers, organizations, and policymakers. This collaborative approach will raise awareness, improve accessible Healthcare, and eliminate stigma, ultimately enabling early detection and treatment of Hep-C.
1077Applying Lessons from Injectable Contraceptive Service Delivery in Sub-Saharan Africa for the New Generation of HIV Prevention Injectables
Anita Dam (presenting)1, Adaobi Lisa Olisa2, Temahlungwane Mkhonta3, Kevin Li1, Baker Maggwa1, Maggie Chase4
1USAID, Alexandria, VA, USA
2FHI 360 Nigeria, Lagos, Nigeria
3FHI 360 Eswatini, Lobamba, Eswatini
4USAID, Washington, DC, USA
Introduction: The introduction and scale-up of injectable contraception sets a precedent for future sexual and reproductive health prevention technologies. In various sub-Saharan African (SSA) countries, injectable contraception is associated with high rates of adoption and longer-term persistence, which can indicate promising signals for introducing injectable pre-exposure prophylaxis (PrEP).
Description: Demand and supply lessons from the implementation of injectable contraception should be considered when planning for injectable PrEP roll out, especially considering the programmatic necessity to address the overlap of high HIV incidence and unwanted pregnancy in geographies like SSA and among populations like adolescent girls and young women (AGYW).
Lessons Learned: From the demand side, promotion and advocacy towards injectable contraceptive use has been geared towards young people, providing them with a discreet, flexible contraceptive option. Demand generation efforts have involved social marketing and receiving support from national stakeholders and community leaders. A significant obstacle to demand has been the slow integration of family planning and HIV prevention services in SSA, and the lack of use of evidence-based strategies such as human-centered design.
From the supply side, injectable contraceptives are provided in the context of voluntarism and informed choice. Operationalizing these principles has faced supply chain obstacles, which do not ensure consistent access to products. Injectable contraceptives have also evolved in the service delivery space, with further demedicalized delivery once a self-injectable contraceptive was made available. Non-traditional service delivery should be explored for injectable PrEP roll out to increase access for populations that face increased social stigma for accessing oral PrEP.
Recommendations: Introduction and scale up efforts by both donors and implementers for injectable PrEP should consider lessons from injectable contraceptive programming with a focus on increasing demand and access for AGYW. To lessen the burden for users, it is important to pursue holistic, user-centered integration between contraception and HIV prevention, and further implementation science research is needed to operationalize integration of services.
1083People Living with HIV Stigma Index 2.0: Stigma and Discrimination Experienced by People Living with HIV in Portugal
Ana Luísa Duarte (presenting)1, João Brito2, Joana Bettencourt3, Ana Subtil4, Sonia Dias4
1Ser+, Cascais, Cascais, Portugal
2GAT, Lisbon, Portugal
3Directorate-General of Health, Lisbon, Portugal
4NOVA National School of Public Health, Lisbon, Portugal
Background: People Living with HIV Stigma Index is an international project implemented in Portugal in 2013 and 2021. It allowed measuring stigma and discrimination (S&D) experienced by people living with HIV (PLHIV) in this country, and assessing the evolutionary trend of these phenomena, to advocate for the defence and promotion of PLHIV rights
Method: Stigma Index questionnaire was conducted through structured interviews applied by trained peers. Data collection occurred between October 2021 and March 2022, in hospitals and community organizations. 1095 questionnaires were applied to PLHIV diagnosed for at least one year, over 18 years/age and living in Portugal, with quotas established by region
Results: 62% of respondents were men, 49% over 50 years/age, 60% diagnosed with HIV more than 10 years. 73% belong to key population(s).
38% experienced social discrimination, with people belonging to key populations being particularly affected. 90.5% reported manifestations of internalized stigma, and 30% self-discrimination (in last 12 m), more frequently in migrants, sex workers (SW), transgender people, and women.
33% avoided treatment for reasons related to S&D; 22% experienced discrimination by healthcare professionals (in last 12 m), most frequently in non-HIV-related health services (16%) and by SW, people who use drugs (PWUD), and women.
15% reported situations of rights violation for living with HIV, more frequently in SW, PWUD, men who have sex with men (MSM), and women. 19% took some action to seek justice.
Transgender people, PWUD, and MSM are the most likely to report S&D for non-HIV-related reasons (88%, 77%, and 65%, respectively).
Conclusion: Comparing with 2013 results, there seems to be a favourable evolution in terms of S&D suffered by PLHIV in various contexts. However, this remains a relevant issue in Portugal, especially in health services, affecting more frequently people belonging to key populations
1091An Open Door for Care – Implementing a Walk-in Sexual Health Clinic in Downtown Sao Paulo, Brazil
Fernanda Rick (presenting)1, Ederson Renan Silva1, Wilson César Ribeiro Campos2, Fabio Sato1, Carlos Eduardo de Oliveira1, Sheila Wudrev1, Marcia dos Anjos1, Ana Caroline Ferreira1, Hugo Ishioka1, Vivian Avelino-Silva2, Beto de Jesus1
1AIDS Healthcare Foundation, São Paulo, Brazil
2Universidade de São Paulo, São Paulo, Brazil
Introduction: Impoverished and socially excluded individuals are highly vulnerable to sexual health issues, including sexually transmitted infections, and discriminatory barriers in health services may further aggravate their susceptibility. The availability of easily accessible, comprehensive sexual health services could facilitate prevention and care, reducing complications and interrupting chains of transmission. Such services could also benefit individuals in less disadvantaged conditions who search for non-discriminatory services.
Description: We present the experience of implementation of a walk-in sexual health clinic offering combination prevention to vulnerable populations in Sao Paulo, Brazil.
Lessons Learned: Downtown Sao Paulo concentrates a large population of individuals confronting barriers to access healthcare, including people facing homelessness, drug addiction, migration, and forced prostitution. This region was selected by Aids Healthcare Foundation based on prior assessment of needs and availability of health services for the implementation of a walk-in clinic dedicated to providing sexual health services to vulnerable populations. Before inaugurating the facility, a transdisciplinary team joined efforts to 1. identify specific needs of potential clients by mapping the area and interviewing target populations; 2. plan medical services, supplies, and benchmarks; 3. develop quality care tools and inclusive communication strategies; 4. provide training to healthcare workers for non-discriminatory care; 5. identify potential barriers and facilitators.
Challenges included delays due to the COVID-19 pandemic; safety aspects; bureaucratic hurdles; and negotiations to establish collaborations for patient referral.
Aspects contributing to the successful establishment of the clinic included its strategic location; the transdisciplinary approach to training, management, and monitoring; the availability of services on-demand and beyond working hours; the efficient, problem-solving process; and the client-centered, humanized approach. (See figure.)

Recommendations: Implementation is a continuum process that must be developed collectively and strategically. Providing care for clients in extreme vulnerability can be challenging. Health facilities and clients benefit from investments in quality, process, and organization.
1092HIV Self-Testing Uptake Among Adolescent Men Who Have Sex with Men and Transgender Women in Brazil Before and During the COVID-19 Pandemic: A Cross-Sectional Study
Laio Magno (presenting)1, Dulce Ferraz2, Eliana Miura Zucchi3, Jony Arrais Pinto-Junior4, Fabiane Soares5, Alexandre Grangeiro6, Dirceu Greco7
1Universidade do Estado da Bahia, Salvador, Bahia, Brazil
2Escola FIOCRUZ de Governo, Fundação Oswaldo Cruz, Brasília, Brazil
3Programa de Pós-Graduação em Saúde Coletiva, São Paulo, Brazil
4Departamento de Estatística, Universidade Federal Fluminense, Rio de Janeiro, Brazil
5Universidade Federal da Bahia, Salvador, Brazil
6Universidade de São Paulo, São Paulo, Brazil
7Universidade Federal de Minas Gerais, Salvador, Brazil
Background: This study aimed to identify factors associated with HIVST uptake among adolescent men who have sex with men (MSM) and transgender women (TGW) before and during the COVID-19 pandemic.
Method: A cross-sectional HIVST uptake study was conducted, nested within the PrEP1519 study, a cohort study of daily oral PrEP among MSM and TGW aged 15–19 in Salvador, São Paulo, and Belo Horizonte/Brazil. HIVST provision by peer educators and health professionals (February 21/2019 to March 31/2021). The primary outcome was HIVST uptake before and during the pandemic.
Results: A total of 491 participants received an HIVST kit at least once. The uptake was 229/510 (44.9%) and 382/1075 (35.5%) before and during the pandemic. During the pre-pandemic, HIVST uptake was higher in participants who reported receptive anal sex with a steady or casual partner in the previous 3 months (aOR: 1.53, 95% CI: 1.02–2.29), whereas during the pandemic period, uptake was lower in participants with a steady sexual partner (aOR: 0.57, 95% CI: 0.39–0.82), and higher in those who had frequent oral sex with a steady partner in the previous 3 months (aOR: 2.84, 95% CI: 1.08–8.85). Before and during the pandemic, HIVST uptake was lower in TGW (aOR: 0.86, 95% CI: 0.46–1.59; aOR: 0.66, 95% CI: 0.34–1.23, respectively), and higher in those aged 18–19 years (aOR: 0.99, 95% CI: 0.61–1.60; aOR: 1.81, 95% CI: 1.10–3.05, respectively) and in participants who lived alone (aOR: 3.36, 95% CI: 1.50–8.29; aOR: 2.35, 95% CI: 1.01–5.78, respectively).
Conclusion: This study showed a high HIVST uptake before the pandemic. However, uptake decreased during the pandemic. Sexual behavioral factors associated with HIVST uptake changed during the COVID-19 pandemic, showing the complex dynamics of the sexuality of MSM and TGW adolescents.
1094Evaluating the Implementation of Home-Based Sexual Health Care Among Men Who Have Sex with Men Using the RE-AIM Framework; Limburg4Zero
Cornelia JD (Hanneke) Goense (presenting)1, Ymke J Evers1, Jonas Manait2, Christian JPA Hoebe1, Inge HM van Loo2, Dirk Posthouwer2, Robin Ackens2, Roland van Hooren3, Rocxanne Theuerzeit3, Rik Crutzen2, Nicole HTM Dukers-Muijrers3
1Maastricht University, Maastricht, Netherlands
2Maastricht University Medical Centre, Maastricht, Netherlands
3Living Lab Public Health, South Limburg, Netherlands
Background: Testing and subsequent treatment is an important strategy to improve clinical outcomes and reduce sexually transmitted infections (STI) and HIV transmission in at-risk groups, such as men who have sex with men (MSM). Home-based sexual health care can reduce barriers to testing and reach MSM who do not (regularly) test, including younger MSM and MSM living in less urban areas. This study aimed to systematically evaluate the implementation process of home-based sexual health care among MSM in the South-eastern part of the Netherlands.
Method: Recently the Centre of Sexual Health implemented home-based sexual health care, including self-sampling STI/HIV tests for MSM not using pre-exposure prophylaxis (PrEP). Via a mixed methods study which included a cross-sectional survey with MSM who received a test kit (n = 362) and in-depth interviews with 10 care providers, we assessed (R) reached population, (E) effectiveness, (A) adoption of the innovation by care providers, (I) implementation fidelity, and (M) maintenance (REAIM).
Results: As of December 2022, 362 participants were reached with sexual health information and received a self-sampling testkit. Of participants (median age 30), 44% had never tested for HIV and 38% reported not testing every 6 months. Subgroups more represented than clinic visiting MSM included MSM living in less urban areas (52% vs 47%) and younger MSM (27% vs 18%) (effectiveness). Adoption by care provider was highly acceptable when involved and due to the expected extended reach of MSM. Key elements were implemented as intended (fidelity), with co-created adjustments. Infrastructural boundaries were mentioned as a hurdle to maintenance of the implementation.
Conclusion: Implementing home-based sexual health care has reached at-risk MSM who have never been tested before. Care providers assess a co-created home-based sexual health care acceptable for implementation. Therefore, home-based sexual health care should be considered a necessary addition to regular clinic-based sexual health care.
1116Assessment of Linkage Gaps for People with Advanced HIV Disease (AHD) in Pilot Implementation of Cryptococcal Meningitis (CM) Care Package in Delhi, India
Arushi Dixit (presenting)1, Anuradha Subramaniam (presenting)2, Arushi Dixit1, Yashika Bansal1, Sachin Kataria3, Arvinder Walia1, Dinesh Rathakrishnan4, Ana Moore4, Alaina Altamura4, James Conroy4, Carolyn Amole4, Umesh Chawla1, Arnab Pal1
1William J. Clinton Foundation, New Delhi, India
2Maulana Azad Medical College, New Delhi, India
3Lok Nayak Hospital, ART Center, New Delhi, India
4Clinton Health Access Initiative, New Delhi, India
Background: AHD refers to people living with HIV (PLHIV) with CD4 < 200 cells/mm3, WHO HIV Stage 3/4, or age below 5 years. ∼40% of PLHIV enter care with CD4 < 200 cells/mm3 under the National AIDS Control Program and are more vulnerable to opportunistic infections like CM. As AHD care packages included in national guidelines (2021) are yet to be adopted at treatment centers, the CM-AHD package was piloted at a Centre of Excellence in Delhi (2022) to inform national implementation and assess coverage.
Method: Adults with CD4 < 200 cells/mm3 were tested using Cryptococcal antigen lateral flow assay (CrAg) and linked to CM prophylaxis / treatment. Operational protocols and distinguishable AHD records were created. Within eight months, 2763 PLHIV underwent CD4 testing, of whom 215(8%) had CD4 < 200 cells/mm3. 100(47%) of them received the same-month CrAg screening.
Results: High Median turnaround time (MTAT) between CrAg and CD4 test (26 days) resulted from a 1-day TAT for CD4 results, lack of quicker revisitations and difficulty in tracking pending tests. Hence, tracking lists and follow-up calls were systemized (which didn’t reduce MTAT), and remnant samples with CD4 < 200 cells/mm3 were reflexively tested using Plasma CrAg to avoid revisitation, which led to ∼100% coverage via same-day testing. (See table.)
Conclusion: Preliminary data suggests that reflex testing improves linkage to CrAg screening, whereas systemized tracking may require improvements. Hence, CD4 TAT reduction and optimized client-tracking should accompany the national scaleup of the AHD package. 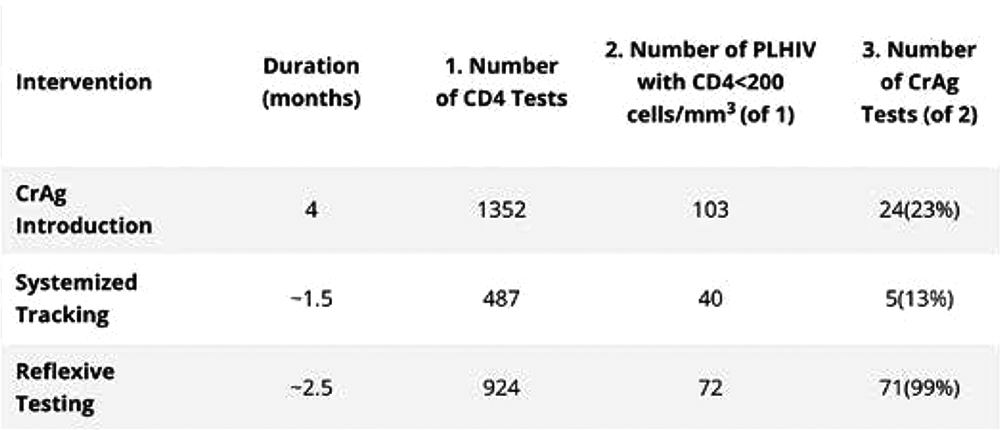
1121Impact of Improvements in the HIV Care Continuum in Miami, FL, USA: A Modeling Study
Dan Escudero (presenting)1, Noé Maldonado Rueda2, Saman Seifi2
1Vanderbilt University Medical Center, Nashville, TN, USA
2Harvard T.H. Chan School of Public Health, Boston, MA, USA
Background: Miami, a fast-track city, has had the highest rate of new HIV diagnosis in the United States for decades. Miami has also experienced numerous successes, particularly in improvements to the care continuum. We sought to estimate the impact these improvements had on the rate of HIV diagnosis and total incident infections during the period of 2014–2021.
Method: We constructed an agent-based model of the Miami population, incorporating many important local factors: demographics, sexual risk behavior, HIV treatment and disease progression, pre-exposure prophylaxis (PrEP), condom use, among others.
We used HIV care continuum data obtained from the Florida Department of Health to estimate annual levels of linkage-to-care within 30 days of diagnosis, total patients in care, and viral suppression from 2014 to 2021. We used these data to infer rates of HIV treatment enrollment, loss-to-follow-up (LTFU), and return-to-care (RTC) by race/ethnicity for the total population. We calculated the HIV diagnosis rate and new infections for two scenarios: a “baseline” based on empirical data from 2014–2021, and a scenario in which “no improvement” was made from 2014 estimates of treatment enrollment, LTFU, and RTC.
Results: Results from a weighted average of 20 calibrated simulations indicated that about 468 new infections among males and 150 among females were averted due to improvements in the care continuum in Miami from 2014–2021. The largest annual reduction in HIV diagnosis rate by 2021 was among Black residents, who had 34.1 fewer cases per 100,000 (59.9 vs 94.0), though all observed subpopulations experienced a marked reduction in HIV diagnosis rate. (See figure.)

Conclusion: Improvements in the care continuum in Miami since 2014 appear to have reduced new HIV infections and diagnoses in all simulated subpopulations. Further work is needed to understand phenomena not completely captured in this model, including potential differences in HIV mortality and care between certain subpopulations.
1122Internet Use Enhances Retention While Depression and Mistrust Exacerbate Drop-Out from a Sexual Health App Intervention Study for Men Who Have Sex with Men
Noah Mancuso (presenting)1, Gordon Mansergh2, Rob Stephenson3, Sabina Hirshfield4, Patrick Sullivan1
1Emory University, Atlanta, GA, USA
2Centers for Disease Control and Prevention, Atlanta, GA, USA
3University of Michigan School of Nursing, Ann Arbor, MI, USA
4SUNY Downstate Health Sciences University, Brooklyn, NY, USA
Background: The United States has seen increases in STIs and HIV diagnoses among all men who have sex with men (MSM) aged 25–34 and Hispanic/Latino MSM overall. mHealth interventions can offer access to multiple primary prevention and intervention services; however, challenges exist in translating mHealth research into practice. The objective of this analysis was to understand the use of a sexual health promotion app among MSM.
Method: Data was used from MSM in the M-Cubed app trial from January 2018 to October 2019 in Atlanta, Detroit, and New York City. The e-commerce acceptance model (EAM) – which includes components of trust, perceived risk, perceived usefulness, and perceived ease of use – was used to assess persistence of app use. Corresponding variables (medical mistrust, perceived risk of HIV acquisition/transmission, perceived protection by HIV/STI testing, and internet use) were mapped to the four EAM domains. Interactions with depression and drug use were considered. Multivariate Cox regression models were used to assess associations with time to study drop-out, defined as the latest date of survey completion, app interaction, or self-test kit ordering.
Results: A total of 611 MSM were included. In bivariate analyses, men with >=4 h of daily internet use at baseline had a 29% lower hazard of drop-out. In the final model, men without depression had a 30% lower hazard of drop-out. The association between internet use and drop-out differed significantly by depression status [not depressed: aHR = 0.43 (0.25–0.72); depressed: aHR = 0.72 (0.38–1.34)]. Depression also modified an association between increased medical mistrust and drop-out [not depressed: aHR = 0.31 (0.09–1.02); depressed: aHR = 0.53 (0.18–1.54)].
Conclusion: Implementation science frameworks, such as the EAM, can help researchers understand how users interact with mHealth interventions to bridge gaps in sexual health access and address mental health concerns. To improve uptake of mHealth, researchers should focus on improving usability and building trust among vulnerable populations.
1123Lesson Learned in Implementing HIV and Tuberculosis Prevention and Treatment Programs Among Key Population in the Megacity of Karachi
Syed Sharaf Ali Shah (presenting)
1
1Bridge Consultants Foundation, Karachi, Pakistan
Introduction: Karachi is among the megacities of the world. It is the largest city in Pakistan, with an estimated population of 20 million persons.
Majority of people living with HIV in Pakistan are concentrated in three major cities including Karachi, Lahore and Islamabad.
Description: We engaged community-based organizations (CBOs) working with key population (KPs) in Karachi and other major cities in Sindh province to provide education, counseling, and screening for HIV and TB to transgender women and male sex workers. The process involved verbal screening, followed by X pert MTB/RIF and HIV testing with informed consent.
Lessons Learned: Challenges
Gaining trust and confidence of transgender women and male sex workers proved challenging, necessitating the involvement of their peers and leaders.
They had limited access to healthcare services and faced deep-seated stigma and discrimination by healthcare providers.
Poverty, unemployment, poor education, malnutrition, unhygienic living conditions and risky behaviours increased their vulnerability.
Recommendations:
Involving peers and community leaders was crucial to establish trust and accessing these populations.
Engaging peers as treatment supporters for TB treatment and ART led to better outcomes.
Counseling and awareness-raising sessions improved their health care seeking behaviors. Addressed low condom use eg, negotiating condom use.
Training of health care providers resulted in user-friendly services.
Access to treatment services improved by establishing treatment centers at convenient places.
It is prudent that there is timely progress on the MOU signed between UNAIDS and the City Government, which will strengthen the HIV response in a mega city like Karachi.
Motorbikes were the most practical means of reaching these populations living in remote peri urban slums.
1128Trends of Testing for HIV and Syphilis in Community-Based Voluntary Counselling and Testing (CBVCT) Services in the Period 2019–2022: Are There People More at Risk?
Daniele Calzavara (presenting)1, Alessandro Soria1, Roberto Rossotti2, Lella Cosmaro3, Roberto Repossi1, Alessandro Tavelli1, Simona Bossolasco4, Anna De Bona5, Alessandra Bianchi1, Donatello Zagato6, Nicoletta Frattini1, Pietro Vinti1, Antonella d'Arminio Monforte7, Massimo Cernuschi1
1Milano Check Point, Milan, Italy
2ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy
3Fondazione di partecipazione LILA Milano ONLUS, Milan, Italy
4San Raffaele Scientific Institute IRCCS, Milan, Italy
5ASST Santi Paolo e Carlo, Milan, Italy
6ASA Onlus, Milan, Italy
7University of Milan, Milan, Italy
Background: HIV screening in informal contexts is a cornerstone of preventive strategies to reduce transmission. Community Based Voluntary Counselling and Testing (CBVCT) might play an essential role.
Method: HIV and syphilis capillary tests in informal contexts (indoor in the association site, outdoor during public events, amusement venues) have been offered between 2019 and 2022 to at-risk populations, along with an anonymous questionnaire investigating attitudes and sexual risks. Data was collected through a web platform (cobatest.org) and analyzed with descriptive statistics.
Results: In the 2019–2022 period, 9353 questionnaires have been administered by volunteers of three associations (6% ASA Milano, 28% LILA, 66% Milano Checkpoint, MCP). Clients were predominantly men (72%); women and transgender women were 27% and 1%. The median (IQR) age was 32 (26–41): 27 (23–35), 29 (24–37) years for men, women, transgender women, respectively. In a 4-year period, there were 62 HIV positive out of 8952 tests (0.69%), and 194 syphilis positive out of 6518 tests (2.98%). The HIV positivity rate dropped during COVID pandemic (2020–2021), but rose again in 2022, while the syphilis positivity increased significantly in the same time span (p = 0.001, Figure 1). HIV prevalence was higher in transgender women (5.08%) and in people reporting unprotected sex (1.06% vs 0.57%), subjects with concomitant syphilis infection (5.91% vs 0.43%), foreigners (1.59% vs 0.50%), subjects reporting previous sexually transmitted infections (1.76% vs 0.54%), sex workers (3.11% vs 0.61%), being MSM (0.97% vs 0.40%) (Table 1). In a multivariable regression analysis, the only factors independently associated with a positive HIV test were being MSM, foreigner and with a concurrent positive syphilis test (Table 2).
Conclusion: CBVCT confirms a role in unveiling new HIV infections. Moreover, it is possible that the context of informal testing and outreach activities could catch even “the hardest to reach”, in particular foreign MSM, thus favoring linkage to care of submerged.
1132Temporal Trends of Incidence of HIV, HCV, and Bacterial Sexually Transmitted Infections Among PrEP Users of a Community-Based PrEP Service in Milan: Data of Milano Checkpoint
Alessandro Tavelli (presenting)1, Roberto Rossotti2, Daniele Calzavara3, Alessandro Soria3, Enrico Caruso3, Roberto Repossi3, Nicoletta Frattini3, Pietro Vinti3, Camilla Muccini4, Daniele Tesoro5, Giovanni Mulè5, Davide Moschese6, Antonella Foschi2, Lorenzo Biasioli5, Simona Bossolasco7, Anna De Bona5, Antonella d'Arminio Monforte8, Massimo Cernuschi7
1Icona Foundation, Milan, Italy
2ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy
3Milano Check Point, Milan, Italy
4IRCCS San Raffaele Scientific Institute, Milan, Italy
5ASST Santi Paolo e Carlo, Milan, Italy
6ASST Fatebenefratelli Sacco, Milan, Italy
7San Raffaele Scientific Institute IRCCS, Milan, Italy
8University of Milan, Milan, Italy
Background: PrEP prevents HIV acquisition but is ineffective against other sexual STIs. Few data are available on trends of STIs in recent years in PrEP users Italy. We describe the incidence of HIV, HCV and bacterial STIs in PrEP users of a community-based service in 2019–2022.
Method: Analysis on PrEP users attending Milano Checkpoint (MCP) from 2019 to 2022. At each PrEP visit, POCTs for HIV, HCV and syphilis and NAATs for C. trachomatis (Ct), N. gonorrhoeae (Ng) was performed.
Repeated tests after first-visit were counted to calculate incidence rates (IR) over time. Incidence rate ratios (IRRs) to estimated changes per calendar year calculated using Poisson regression models, adjusted for age and nation of birth.
Results: 878 PrEP users of MCP included: 97.7% male, 96.4% MSM, median age 36 (31–44), 79.3% born in Italy.
1 HIV (IR 0.99 x1000 PYFU) and 4 HCV seroconversions (IR 4.00 x1000 PYFU).
83 syphilis diagnosed: prevalence 8.2%, IR low during the study period [Table 1A, Figure 1], no differences by year [Table 2A].
329 Ct positive tests, prevalence 26.6% and IR 27.0 x100 PYFU [Table 1B, Figure 1], no significant difference by year [Table 2B].
318 Ng positive tests, prevalence 25.8% and IR 25.5 x100 PYFU. IR raised from 17.4 to 34.4 x100 PYFU [Table 1C, Figure 1]. The year 2022 was associated with a 2-fold higher incidence of Ng [Table 2C]. Non-Italians and users <30 years had a higher incidence increase in 2022 [Fig. 2A-B].
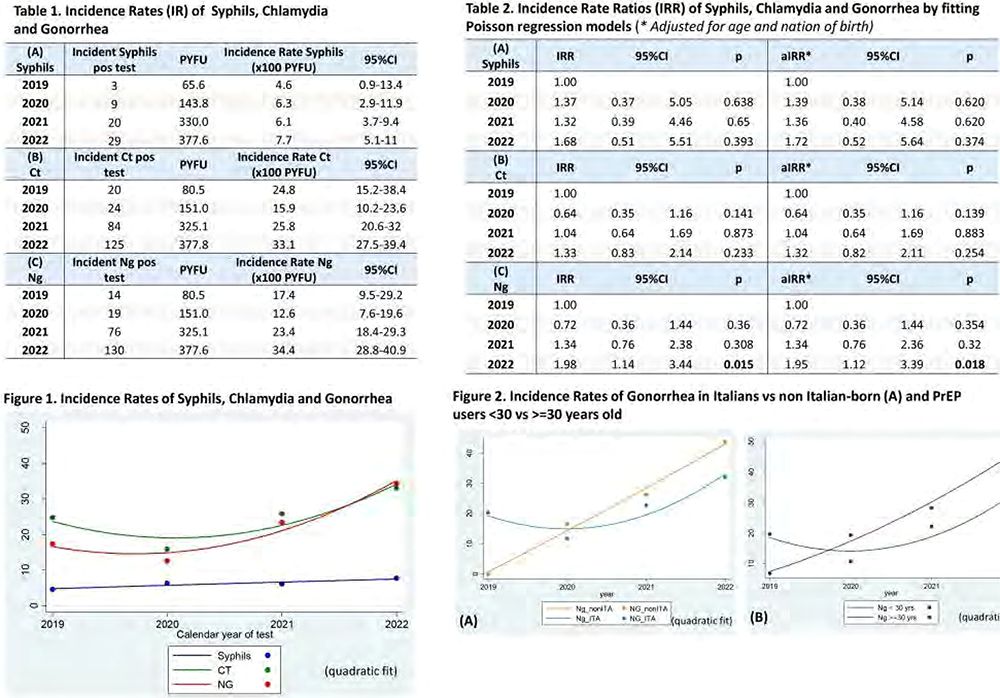
Conclusion: Ct and Ng incidence among MCP PrEP users were high: in 2022 a significant increase in Ng, especially among non-Italians and youngers. Monitoring sexual behaviours and STIs diagnosis in this Ng “outbreak” is an essential task of PrEP services given the high contagiousness and the reports of resistance.
1143Community-Based Organization's Role in Reengaging Out-of-Care People Living with HIV in Portugal
Diogo Medina (presenting)1, Mariana Vicente (presenting)2, Miguel Rocha (presenting)3, Willian Gomes2, Alba Carrodeguas1
1Gilead Sciences, Madrid, Spain
2GAT, Lisbon, Portugal
3Grupo de Ativistas em Tratamentos, Lisbon, Portugal
Introduction: GAT, a patient-led non-governmental organization, advocates for the rights of people living with or affected by HIV (PLHIV) and related co-infections in Portugal. GAT employs a “one test, three paths” approach to diagnose PLHIV who are newly infected, previously diagnosed and out-of-care, or people who test negative and are eligible for comprehensive prevention services. Experts estimate approximately 1000 PLHIV were linked to care in Portugal in 2022. Herein, we describe our contribution to reengaging previously diagnosed out-of-care PLHIV.
Description: In 2022, GAT conducted 31,189 screening sessions and 30,281 HIV tests at six testing centers and two mobile units in the Lisbon area. PLHIV were also offered navigation into care, addressing documentation required to access the national health service, promoting health literacy, and providing social support.
Lessons Learned: In 2022, GAT referred 664 PLHIV to care: 261 (39%) were newly infected, 403 (61%) were previously diagnosed out-of-care. Of these, 276 (68%) were engaged through GAT-Intendente, a center tailored to the needs of transgender people, sex workers, migrants, and people experiencing homelessness; 119 (30%) were engaged through GAT-CheckpointLX, a center tailored to the needs of men who have sex with men; and 8 (2%) were engaged through other GAT services. GAT's success can be attributed to several factors: service tailoring to key populations in an informal, low-threshold environment; integration of peers across services and management; skilled social workers on staff to overcome barriers in accessing care; language familiarity for most Brazilian migrant population; and word of mouth in the community.
Recommendations: GAT's services accounted for most of PLHIV linked or relinked to care in Portugal in 2022, with men who have sex with men and migrants from Brazil representing the largest volume.
1145Community-Based Organization's Best Practices for HIV Comprehensive Prevention Services
Diogo Medina (presenting)1, Gema Garrido (presenting)2, Jorge Garrido (presenting) 2, Juan Francisco Cabrera Solano (presenting) 2, Alba Carrodeguas1, Lucio J García-Fraile Fraile2
1Gilead Sciences, Madrid, Spain
2Apoyo Positivo, Torremolinos, Spain
Introduction: In its Political Declaration on HIV and AIDS, UNAIDS challenged countries to commit to increasing the proportion of HIV services delivered by communities, ensuring that, by 2025, community-led organizations deliver 30 per cent of testing and treatment services, with a focus on HIV testing, linkage to treatment, adherence and retention support, and treatment literacy. Herein we address the innovative methods applied by Apoyo Positivo (A+), a community-based organization in Spain, focusing on a center in Torremolinos.
Description: Founded in 1993, A + operates 6 community centers (CASA) in Spain to offer sexual health services, psychosocial care, and social entrepreneurship initiatives. A unique aspect is the centers’ holistic approach to create a sense of home and connection, to ensure people feel comfortable seeking services. The Torremolinos center, established in 2019 with assistance from the FOCUS Program, is an example of this comprehensive approach.
Lessons Learned: Over four years, the Torremolinos center tested nearly 2000 individuals for HIV, Hepatitis B and C, resulting in 45 diagnoses, primarily HIV. It delivered nearly 3000 sexual health counseling sessions and drug use harm reduction sessions, with a significant focus on Chemsex harm reduction. It linked 80% of eligible persons to biomedical HIV prevention, aided by a proprietary smartphone app, “PrEParadxs”. Challenges included addressing the rise in Chemsex, increasing reach to women, trans, and migrant populations, refining relationships with formal healthcare services, and securing governmental funding.
Recommendations: A+'s holistic approach to HIV prevention has proved successful. Recommendations include collaboration with community-based organizations and championing their approach to maximize utilization of prevention tools and continue efforts to end the HIV epidemic. There's a need to adapt and accommodate changing demographics, behaviors, and systemic barriers, emphasizing the importance of continued funding and collaboration with healthcare entities.
1146Artificial Intelligence-Assisted Identification and Retrieval of Chronic Hepatitis C Patients Lost to Follow-Up in the Health Area of Pontevedra and O Salnés, Spain
Diogo Medina (presenting)1, Pablo Parada Vázquez (presenting)2, Santiago Pérez Cachafeiro3, María Belén Castiñeira Domínguez2, Nuria Vázquez Temprano2, Indhira Miosotis Pérez Medrano2, Yolanda Falagan Cachafeiro2, Raquel Souto Rodríguez2, José Manuel Mera Calviño2, Matilde Trigo Daporta2, Julio Diz Aren2, Juan Turnes2
1Gilead Sciences, Madrid, Spain
2Complejo Hospitalario Universitario de Pontevedra, Pontevedra, Spain
3CS Virxen Peregrina Área Sanitaria Pontevedra e O Salnés, Cambados, Spain
Introduction: Hepatitis C Virus (HCV) is a significant global health issue. The World Health Organization aims to eliminate HCV by 2030, but undiagnosed or untreated cases pose a challenge. Our study focused on identifying and retrieving HCV patients lost to follow-up within the health area of Pontevedra and O Salnés, Spain, using retrospective search and patient data analysis.
Description: Between 2007 and 2019, we identified 1832 HCV-positive patients, narrowed down to 99 who were untreated and lost to medical follow-up. This group was majority male with a mean age of 55, and a significant percentage had a history of drug abuse. These patients were contacted and offered renewed consultation.
Lessons Learned: We were able to retrieve 53.5% of the lost patients, who then began antiviral treatment. A significant proportion had never been referred to a specialist, while others dropped out during consultation due to fear of treatment, mobility impediments, lack of disease perception, or confusion about treatment. A quarter of the retrieved patients were at an advanced stage of liver fibrosis, highlighting the importance of early diagnosis and treatment.
Recommendations: Active search efforts, combined with education about HCV and its treatment, are critical for retrieving lost patients and reducing HCV spread. Improving referral protocols and maintaining persistent follow-up can address the issue of undiagnosed and untreated HCV. Future research should investigate the impact of COVID-19 on HCV elimination efforts and the effectiveness of retrieval strategies in different regions.
1153Our Healthbox: Implementation and Evaluation of Interactive Dispensing System for Low-Barrier Access to HIV Self-Testing and Harm Reduction Supplies for Marginalized People in Canada
Kristin McBain (presenting)1, Darshanand Maraj (presenting)2, Jason M. Lo Hog Tian3, Maarij Hannan Ulah2, Brian Fung2, Jordon Bell2, Richard Galli4, Kristin McBain1, Sean B. Rourke2
1MAP Centre Urban Health Solutions, Toronto, ON, Canada
2Unity Health Toronto, Toronto, ON, Canada
3University of Toronto, ON, Canada
4CIHR Centre for REACH, Toronto, ON, Canada
Background: In Canada, there are an estimated 6500 persons currently living with HIV who remain undiagnosed, many of whom also have complex health and social circumstances and housing instability. Our Healthbox (Notre Boîtesanté) program is centered around a network of ‘smart’, interactive dispensing machines hosted by community-based organizations that provide low-barrier anonymous access to HIV self-testing (HIVST) kits, harm reduction materials (eg, naloxone kits, safe injecting and inhalation supplies), sexual health supplies (eg, condoms, lube), and personal health items (eg, tampons, toothbrushes). It also provides health information and a directory for people to find healthcare and social services they may need in their community. Our Healthbox launched in January 2023 in four New Brunswick (Canada) communities: Moncton, Sackville, Richibucto and Woodstock First Nation (large urban, small urban, small rural, and Indigenous rural communities, respectively).
Method: Evaluation of the program's reach included describing participant demographics, supplies dispensed and reason for accessing items using data collected from the optional sign-up, dispensing and post-access survey questions between January 23 to May 23, 2023.
Results: During this period the four Health boxes served 649 persons of which the majority were female (63%, except Woodstock where 77% were female), under 40 years (70%), identified as heterosexual (49%), educated (high school or further, 61%), had difficulty paying for basic needs (61%), and were under-housed (58%). Participants dispensed >1200 safe injecting and >750 inhalation supplies and approximately 200 HIVST kits (for themselves or to share with a social connection, eg, partner, friend). Overall, > 50% of those accessing HIVSTs were first-time testers with the smaller communities generally reporting much higher proportions.
Conclusion: The program is reaching underserved people where they are in both large urban and small rural areas. By the end of 2023 we aim to implement 25 machines in communities across Canada and scale-up to 100 communities over the 3-year program.
1154Clients Lost to Follow-Up (LTFU) and Re-Engagement in HIV Care in Lagos, Nigeria (2020–2021)
Helen Omowumi Olowofeso (presenting)1, Oladipupo Fisher2, Rotimi Agbolagorite3, Monsurat Adeleke4, Olusegun Ogboye5, Sindhu Ravishankar6, José M. Zuniga7
1IAPAC, Lagos, Nigeria
2Lagos State Aids Control Agency, Lagos Island, Nigeria
3Lagos State Ministry of Health, Lagos, Nigeria
4Lagos State AIDS Control Agency Nigeria, Lagos, Nigeria
5Lagos State Ministry of Health, Lagos, Nigeria
6Fast-Track Cities Institute, Lagos, Nigeria
7IAPAC, Washington, DC, USA
Background: Patient Loss to Follow Up (LTFU) is a barrier in attaining the third 95 viral suppression target. In Lagos, extended ART coverage led to increased treatment program outcomes, but LTFU remains a major challenge to retention in care and viral suppression.
Method: A retrospective analysis of routine data (2020 and 2021) collected by the Lagos State Ministry of Health (LSMOH) and reported using the NHMIS database was conducted. Data collection and reporting was done by. Enrollment, retention, and LTFU data (defined as 90 days absence from date of last appointment) were analyzed.
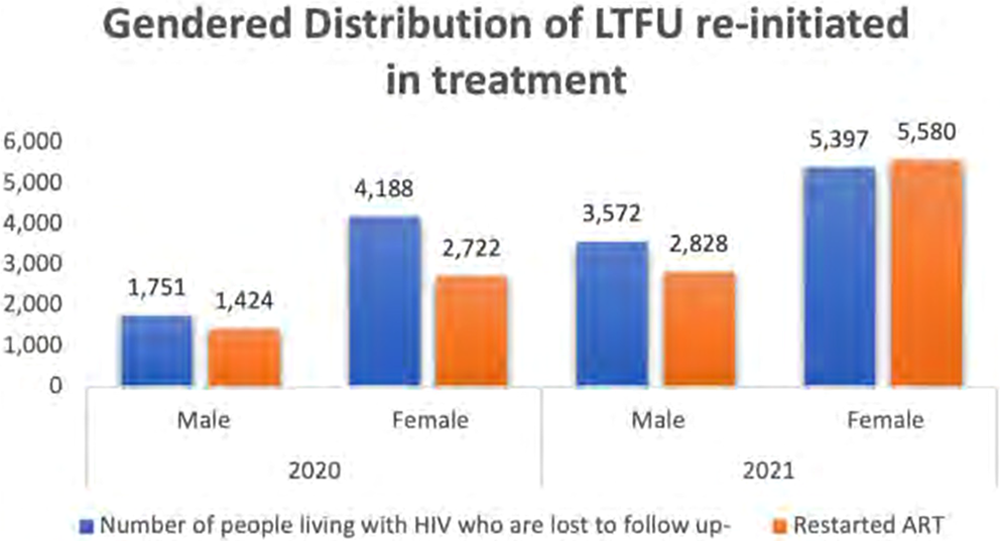
Results: From 2020 to 2021, PLHIV enrolled and retained in treatment over 12 months increased by 7% in Lagos. These clients represented 8% of those initiated on treatment across the country in 2021. The LTFU rate in Lagos was 5% in 2020 and increased to 7% in 2021, compared to a national rate of 6% in 2021. The increase in the number of clients traced in 2021 versus 2020 was 2622 (27%). Women and girls made up to 55% of those needing to re-initiate on treatment. In 2021, 9% of clients LTFU in Nigeria were reported in Lagos. 70% of clients LTFU in Lagos in 2020% and 94% in 2021, were re-enrolled in treatment (66% female). In 2020, 62,990 PLHIV attained viral suppression (69% female) while in 2021 the number increased to 82,557 (70% female). (See figure.)
Conclusion: Despite an increase in the loss to follow up between 2020 and 2021, there was an improvement in the proportion of LTFU re-engaged between 2020 and 2021. Addressing interruption of HIV treatment and continuing to strengthen efforts to re-engage those LTFU has the potential to improve third 95 outcomes in Lagos. There is also an opportunity to examine the educational, economic and socio-cultural ramifications which make women disproportionately affected as seen in the data.
1158Utilizing Existing HIV/STI Outreach to Reduce Disparities in Mpox Vaccination
Cherise Rohr-Allegrini (presenting)1, Stephanie Young (presenting)1, Gabriel Medina1
1San Antonio AIDS Foundation, San Antonio, TX, USA
Introduction: Communities disproportionately affected by HIV are also more susceptible to Mpox infection. As Mpox cases increased in Bexar County, the San Antonio AIDS Foundation (SAAF) began incorporating Mpox vaccination into existing HIV/STI outreach events. SAAF's strategy focused on fighting stigma and addressing the challenges of individuals who face barriers to accessing Mpox vaccination.
Description: Data from the 2022 outbreak indicated that men who have sex with men (MSM), communities of color, and individuals experiencing homelessness are disproportionately affected by Mpox. However, only 15% of at-risk Texans received at least one dose of the vaccine. The first-come first-served model originally implemented favor individuals with resources, such as transportation and the ability to make appointments during work hours, which contributes to disparities in vaccination rates.
Because SAAF already provides HIV/STI testing in these communities, ensuring privacy and judgement-free care for all, we have established trust. To increase equity in access to Mpox prevention, SAAF initiated Mpox vaccination during HIV testing outreach events, providing dual services from our mobile testing van with private testing rooms. Events were held at homeless shelters, recovery residencies, and LGBTQ spaces.
Lessons Learned: SAAF hosted 13 events, administering 157 Mpox doses. Of these, 52.87% are experiencing homelessness, 54.8% are Hispanic, 21% Black, and 17.2% identify as MSM. SAAF found higher success administering second doses when returning to the same location after 28 days. Clients were given cards with info about the mobile unit's return, and details about SAAF's clinic so they can make an appointment if they prefer.
Recommendations: Mobile clinics from a trusted source increase equity with the delivery of Mpox vaccines to vulnerable populations. This strategy is well received by the community, and is an impactful way to maximize vaccine uptake, improving community health.
1159From the Margins to the Center: Tackling Stigma and Poor Mental Well-Being as the Key Global Barriers to Living Well with HIV, a Multinational and Multi-Community Position
Dazon Dixon Diallo (presenting)1, Stephan Vernhes2, Susan Cole-Haley3, Jorge Garrido4, Ntombenhle Mkhize5, Victoria Ortega6, ZongTai YoYo Wu7, Michael Bogart8, Connie Kim8, Mario Casco9
1SisterLove, Inc., Atlanta, GA, USA
2AIDES, Les Lilas, France
34 M Network, London, England, United Kingdom
4Apoyo Positivo, Madrid, Spain
5AIDS Foundation of South Africa, Durban, South Africa
6FLUX, Los Angeles, CA, USA
7Taiwan HIV Story Association, Taipei City, Taiwan
8Gilead Sciences, Inc, Toronto, ON, Canada
9European AIDS Treatment Group, Brussels, Belgium
Introduction: The global HIV Community Council (HCC), a group of ten leaders of diverse, under-represented groups of people with HIV, prioritized stigma, and poor mental wellbeing as critical barriers to successfully living well with HIV. The HCC has developed a set of recommendations to address these critical barriers.
Description: The HCC achieved consensus on six global recommendations through offline and online meetings, a comprehensive literature review, and the sharing of examples of successful practical solutions to address stigma and poor mental wellbeing. The HCC selected the two recommendations that, based on their experience, would have the greatest impact, and provided guidance on their implementation.
Lessons Learned: To address HIV-related stigma, the HCC recommended harnessing the ‘power of one's own story’ using incubator programs, that provide access to mentorship and collaboration opportunities, to disseminate engaging, culturally appropriate, and relatable stories that challenge stigma across various settings, including social media. Supported by talent scouts to identify potential partners, build relationships, and facilitate collaborations between influencers and brands or organizations, these programs provide influencers with the resources and support to create and share accurate and culturally competent information about HIV across community-appropriate platforms. To address mental wellbeing, the HCC recommends partnering with expert organizations to equip leaders of peer-support groups with Mental Health First Aid training to enable staff of community organizations to identify and screen for mental health needs such as anxiety and depression and connect individuals with mental health services in crisis and non-crisis situations.
Recommendations: The HCC calls for action to implement community-endorsed, culturally appropriate, and practical solutions to tackle stigma and mental wellbeing and improve HIV care in a way that reflects the unique local lens of each community.
1161Utilization of Conversation Map in eThekwini
Kalvin Pugh (presenting)
1
1IAPAC, Kansas City, KS, USA
Introduction: In eThekwini, there are an estimated 672,437 people living with HIV (PLHIV). However, lack of awareness of the science and campaign around “Undetectable = Untransmittable” (U = U), internalized and community level HIV-related stigma are contributing to sub-optimal HIV outcomes. IAPAC's Conversation Map (CM) on “Staying in Care for U = U” is being implemented to raise awareness of U = U and illustrate the continuum of care.
Description: The objective of the CM is to provide illustrated steps through the HIV continuum from diagnosis, understanding HIV, finding support, falling out of care and reengagement. PLHIV lead trainings, workshops, and mentorship on key issues. Trainers present local epidemiology, best practices, and M&E. Trainers teach both community-based groups, including Ward AIDS Committee (WAC) training sessions, support group leaders and members. The workshops deliver key messages of stigma reduction and achieving epidemic control. Participants interact with trainers on issues raised and potential CM uses/plans. Participants are asked to evaluate the usage of the CM following the trainings.
Lessons Learned: CM training/use is ongoing with promising results. To date, 284 individuals have been trained on the CM including: 27 Support group facilitators, 82 participants, 18 adherence officers, 200 WAC members and 15 children's sector leaders. 72 trainees overwhelmingly agreed/strongly agreed: the CM is easy to understand and use, and topics are relevant. 99% indicated it would be useful in their ward. Of 67 PLHIV surveyed post-exposure, 91% “had a better understanding and were willing to achieve U = U,” and 97% were “extremely likely” to recommend the program.
Recommendations: The CM provides an important tool in illustrating the journey from diagnosis to U = U and is well received by trainers and community members alike. Increasing awareness around U = U and reducing HIV-related stigma are crucial to ending AIDS as a public health threat by 2030. Scaling of the CM is recommended.
1163A PrEP Decentralization Project – Almada on the Fast-Track to End the AIDS Epidemic
Daniela Lages (presenting)1, Joelsy Pacheco2, Inês Correia2, Cátia Pires2, Fátima Gomes2, Mariana Vicente2, Bruno Pinto2, Joeli Sousa2, Paula Brito1, Alexandre Tomás3, Rita Cunha4, Nuno Silva Marques1
1Hospital Garcia de Orta, Almada, Portugal
2GAT, Lisbon, Portugal
3ACES Almada-Seixal, Almada, Portugal
4Câmara Municipal de Almada, Almada, Portugal
Background: Hospital Garcia de Orta (HGO) is a Portuguese public central Hospital, located in the city of Almada, at the metropolitan area of Lisbon, with a direct catchment area of 350.000 inhabitants.
The infectious diseases service implemented on 15th September 2021, a decentralized PrEP HIV clinic service delivery in the community at CIRSS Almada (Center for Integrated Social and Health Responses), in a partnership project with Almada City Council, the local primary healthcare centers group and the NGO GAT (treatment activist group). This project aims to bring the service closer to the population at risk, in order to achieve a greater response in the prevention of HIV infection.
Method: We conducted a retrospective data analysis from 15th September 2021 until 31st May 2023.
Results: In total, 1170 medical appointments were performed, 329 first visits and 841 subsequent. In this period, 157 people were followed, mainly males (94,9%; n = 149), MSM (134) and migrants (100, of which 67 from Brazil). The mean age was 33 y/o [19–57].
Regarding specific HIV acquisition risk factors with indication to start PrEP, 13 (8,3%) had an HIV infected partner, 13 (8,3%) were sex workers and 12 (7,6%) had chemsex practices on a regular basis. Previous PrEP use was reported in 36 (22,9%) cases, of which 4 without medical prescription and history of PPE HIV treatment was mentioned by 19 (12,1%) people. The majority (57,3%, n = 90) were previously diagnosed with STI, not HIV.
Daily PrEP was the most suitable regimen for the majority (65%, n = 102).
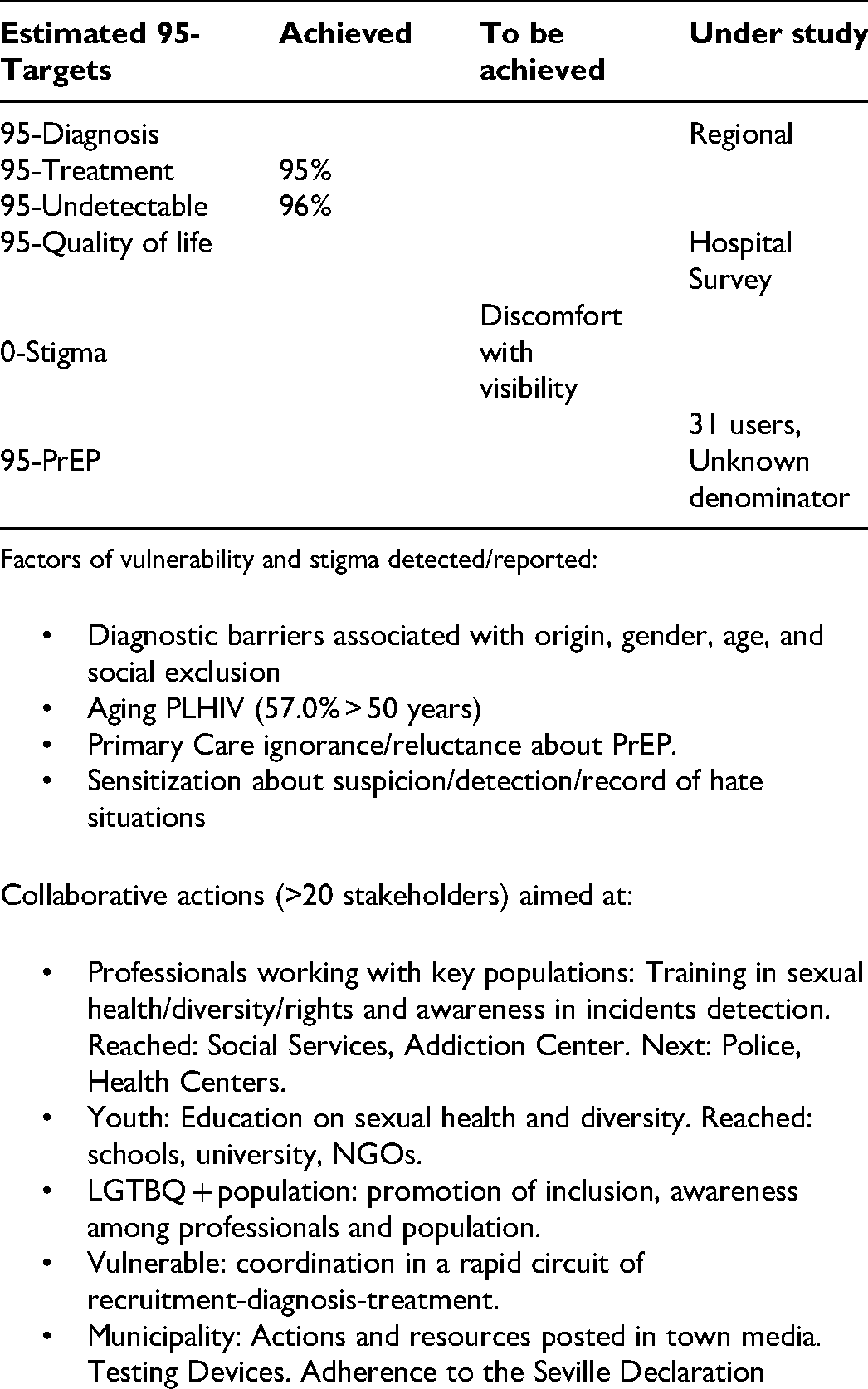
Conclusion: This PrEP decentralization project contributes to the dissemination strategy to scale up PrEP delivery in a national healthcare service with scarce health responses in proximity to the community and populations at higher risk for HIV acquisition.
1169Perceived Quality of Life, Experiences of (Healthcare) Stigma, and Viral Load Differences Among People Living with HIV in German Cities and States: A Community Perspective Based on the Positive Voices 2.0 Survey
Kai Jonas (presenting)1, Franziska Hartung2, Matthias Kuske3, Clemens Lindner4, Marie Piening5, Janine Dieckmann2
1Maastricht University, Maastricht, Netherlands
2Institute for Democracy and Civil Society, Jena, Germany
3Stiftung Akademie Waldschlösschen, Gleichen, Germany
4Friedrich Schiller University, Jena, Germany
5Goethe University, Frankfurt, Germany
Background: Usually, HIV cascade indicators are provided by national registries and do not include data on psycho-social indicators provided by the community. Furthermore, it is important to map out regional and urban/rural differences especially in countries like Germany characterized by larger recent political changes (eg, the reunification in 1991) and known socio-economic divides. By including both community perspectives and broader sets of (psycho-social) indicators into the comprehensive assessment of the state of the HIV epidemic can help to reduce new HIV infections.
Method: Among 935 male and female individuals living with HIV, we assessed viral load status, but also individual level determinants, such as experienced (healthcare) stigma, acceptance of the infection, and general self-evaluation, as well as identification and representation with(in) the HIV community as community level determinants. Data was gathered via the Positive Voices 2.0 survey in Germany in 2021/2022 and analyzed with ANOVAs.
Results: No East-West German states divide appeared but an urban versus non-urban difference was found with significantly more individuals with a detectable viral load living in smaller urban or non-urban settings (less than 100 k inhabitants). Perceived stigma, guilt and general self-evaluation was found to be worse in both East and West German states compared to the city state of Berlin. Experiences of healthcare discrimination and healthcare access problems were reported most frequently in states with large surface areas and few urban areas.
Conclusion: To improve quality of life and to achieve higher percentages of viral suppression it seems indicated to scale up HIV care, to reduce experiences of stigma and guilt, and to increase positive self-evaluations outside of Berlin and in rural areas. Achieving such outcomes can impact positively on the HIV epidemic in Germany.
1183Stigmatization Towards People Living with HIV/AIDS in the Era of Test and Treat Policy in Kampala-Uganda
Edward Mawejje (presenting)
1
1USAID Uganda Health Activity-Uganda, Kampala, Uganda
Background: In 2015, WHO introduced test and treat policy, all PLHIV started on antiretroviral therapy (ART) same day of a positive status confirmed regardless of CD4 counts. only 20.9/37 million people living with HIV globally were registered to be in HIV care by the end of 2018. However, even post guideline roll out of the test and treat policy, the problem continues to persist. This study aimed at determining Stigmatization prevalence it has associated among PLHIV enrolled under the test and treat policy in three health facilities in Kampala district.
Method: A cross-sectional study among eligible PLHIV enrolled into HIV care during the test and treat period 2016–2020, from three ART Health facilities in Kampala, simple random sampling, applied Berger questionnaire for data collection for overall prevalence, four subscales of HIV stigmatization. Modified Poisson method for variate analysis to determine the risk factors associated with HIV stigmatization. Data was analyzed using STATA and the level of significance was determined at p value 200), and a confidence interval of (95% CI).
Results: Overall, 85% of the respondents experienced at least one subscale of stigmatization in the last three months prior to the survey, predominantly personalized at 98.6%, least public attitude at 83.7%. At adjusted analysis, the prevalence of HIV stigmatization was 1.2 times (95% CI: 1.05–1.88) higher among the males, those with a baseline CD4 count above 200, 9.2 times (95% CI: 5.7–23.4) and those with comorbidities like hypertension 8.2 times (95% CI: 4.21–15.4) and diabetes 5.3 times (95% CI: 3.11–9.31).
Conclusion: HIV related stigma in this population was very high and was most prominent among men, individuals with higher CD4 counts (>200), and those with comorbidities.
Findings indicate need to further enhance facility and community level stigma reduction interventions, especially among the men, comorbidities and higher CD4 counts
1185Comfort Corner: Bridging the Gap of Love and ART Adherence Among Youth Living with HIV in Blantyre City
Madalitso Juwayeyi (presenting)
1
1Forum for AIDS Counseling and Training (FACT Malawi), Blantyre, Malawi
Introduction: Young People Living with HIV(YPLHIV) in Blantyre City express the distressing struggle to find love while maintaining their health and adhering to Antiretroviral Therapy (ART). This challenge has made many YPLHIV resort to lying about their HIV status which often leads to secret medication intake and subsequent poor adherence to HIV medication. In response to this critical concern, FACT Malawi- a youth-led organization pioneered an innovative solution called” Comfort Corner” (COMFCO). This initiative aims to combat stigma, facilitate ART adherence, and foster meaningful connections and networks among YPLHIV. COMFCO also serves as a place where YPLHIV form relationships and find love.
Description: “Comfort Corner” works as a platform where FACT Malawi engages with over 5000 YPLHIV from Blantyre city and has successfully expanded its reach to other districts. COMFCO offers a sense of belonging, helps alleviate loneliness, and creates a supportive community where YPLHIV freely discuss their experiences, challenges, and successes. By facilitating connection, COMFCO provides a family for those who feel isolated or misunderstood. COMFCO also facilitates a meaningful connection between YPLHIV who are willing to openly share their HIV status and their peers who are HIV negative.
Lessons Learned: The implementation of COMFCO has yielded profound outcomes for YPLHIV and has successfully tackled the prevalent issues of lying about HIV status. By providing a space for honest and compassionate engagement, COMFCO has effectively reduced stigma and encouraged ART adherence. YPLHIV in COMFCO have reported feeling less lonely, more connected and motivated to prioritize their health.
Recommendations: Based on the resounding success of COMFCO, it is crucial to scale this initiative national wide and foster collaboration with local healthcare providers, NGOs, and government agencies. The inclusion of comprehensive counselling services, educational HIV prevention campaigns, and ongoing mental health support can further enhance the initiative's impact.
1188High HIV Incidence Follows High Testing Rates in the Rotterdam Area, the Netherlands: A Cross-Sectional Population-Based Study
Denise Twisk (presenting)1, Abraham Meima1, Jan Hendrik Richardus1, Ard van Sighem2, Casper Rokx3, Jan den Hollander4, Hannelore Götz1
1Municipal Public Health Service Rotterdam-Rijnmond, Rotterdam, Netherlands
2Stichting HIV Monitoring, Amsterdam,Netherlands
3Erasmus University Medical Center, Rotterdam, Netherlands
4Maasstad Hospital, Rotterdam, Netherlands
Background: Appropriate access to HIV testing is crucial for detection, linkage to treatment, and prevention. HIV testing is probably more reliant on general practitioners (GPs) in less urban areas since sexual health centers (SHCs) are typically located in urban areas. In this cross-sectional study, we aim (1) to assess and compare HIV testing at GP and SHC, and (2) to assess population- and provider-specific HIV incidence.
Method: Individual HIV testing data of GP and SHC were linked to population register data (aged ≥ 15 years, Rotterdam area, 2015–2019). We reported the proportion of HIV tested and compared GP and SHC testing rates with negative binomial generalized additive models. Data on new HIV diagnoses (2015–2019) from the Dutch HIV Monitoring Foundation relative to the population were used to assess HIV incidence.
Results: In total 1.14% of all residents were tested for HIV (range 0.41% for ≥40-year-olds to 4.70% for Antilleans). GPs had a higher testing rate than the SHC (overall rate ratio (RR) of 1.61; 95% CI: 1.56–1.65), except for 15–24-year-olds (RR: 0.81, 95% CI: 0.74–0.88). Large differences in HIV testing rate (1.36 to 39.47 per 1000 residents) and GP-SHC ratio (RR: 0.23 to 7.24) by geographical area were observed. Groups that were relatively often tested also had the highest incidence of HIV (eg, men, non-western). The overall incidence was 10.55 per 100,000 residents, but varied by demographic and area characteristics, ranging from 3.09 to 24.04 per 100,000 residents.
Conclusion: GPs play a significant role in HIV testing in less urban areas further away from the SHC, and among certain population groups. For most population groups, a high incidence corresponds with high testing rates. Opportunities to improve HIV testing have been found for some subpopulations. Also, additional testing via SHC branch locations and outreach activities seems promising in areas distant from the SHC.
1194Tailored HIV Support Services for African Men Living with HIV in Greater Manchester
Jeff Ukiri (presenting)
1
1George House Trust, Manchester, England, United Kingdom
Introduction: The African Men's Engagement Project, a service provided by George House Trust, is specifically tailored to support African men living with HIV. The project employs an African Men's Engagement Worker to offer person-centered and individualized one to one support and facilitate group activities.
Description: The project focuses on achieving the following key outcomes:
Improved social engagement and connectivity
Reduced social isolation
Improved mental well-being
Increased involvement in volunteering activities
Lessons Learned: Impact and Evaluation:
An external evaluation of the project demonstrated its significant positive impact on the participants. The project has empowered African men living with HIV to take control of their health and well-being, leading to tangible life improvements. The evaluation revealed that engagement with the project has greatly increased participants’ confidence in managing HIV, with 88.8% reporting a notable increase in their ability to do so. Moreover, 85% of participants expressed high levels of confidence in living with HIV.
Additional positive outcomes reported by participants include:
Benefitting from engaging with other African men living with HIV (80%)
Improved social engagement and connectivity (78.8%)
Reduced social isolation (76.2%)
Improved mental well-being (72.6%)
Increased involvement in volunteering activities (58.8%)
Since project inception
205 unique individuals have engaged with the project
111 unique individuals have accessed the project for one-to-one support
87 unique individuals have accessed group spaces
31 Group Sessions have been completed
An average of 20 individuals have attended groups
Recommendations: Based on the clear success of this project, other HIV organizations should consider establishing person-centered services that are tailored to the needs of African men living with HIV in order to address their unique circumstances and improve their wellbeing.
1201Implementation of Differentiated Models of Care in a Paediatric Cohort in eThekwini Municipality, Durban, South Africa
Yukteshwar Sookrajh (presenting)1, Lara Lewis2, Thokozani Khubone1, Johan van der Molen2, Riona Govender3, Nigel Garrett2, Phelelani Sosibo1, Munthra Maraj1, Andy Gray2, Jienchi Dorward4
1eThekweni Municipality, Durban, South Africa
2Centre for the AIDS Programme of Research in South Africa (CAPRISA), Durban, South Africa
3South African National Department of Health Moherndran Archary, Durban, South Africa
4University of Oxford, Oxford, England, United Kingdom
Background: eThekwini Municipality has one of the largest populations of people living with HIV globally, with a large number of children and adolescents with HIV (CAWH) receiving antiretroviral therapy (ART). We aimed to evaluate the implementation and impact of Central Chronic Medicine Dispensing and Distribution programme (CCMDD), which has enabled rapid ART provision at community pick-up points since mid-2020.
Method: We analyzed routinely collected, de-identified data from 59 eThekwini Municipality Health Unit primary care clinics. We describe enrolment of CAHW into CCMDD between June-Dec 2020 and assessed 12-month retention-in-care and viral load suppression (<50 copies/ml).
Results: During the study period, 951/6985 (13.6%) of all CAHW on ART were referred to CCMDD. Of these, 194 were enrolled into CCMDD before December 2020. The median age of this cohort was 16 (IQR 13–18 years) and 60.3% were female. 59.3% of these CAHW received a 6-month CCMDD prescription, and 40.7% received a 12-month prescription. There were 10 treatment regimens prescribed, with the majority for TDF/XTC/EFV (39.7%) and TDF/XTC/DTG (32.5%). After 12-months, 178/194 (91.7%) CAWH were retained-in-care. 148/178 (83.1%) had a 12-month viral load, of whom 123/148 (83.1%) were suppressed.
Conclusion: While CCMDD uptake has been low, retention-in-care and viral suppression were high in those enrolled. This suggests that CCMDD is an effective strategy as a differentiated model of care for this population. The majority of prescriptions were fixed dose combinations, which also facilitates the rollout of CCMDD among CAWH. Further work is needed to evaluate barriers to uptake among younger CAWH in CCMDD, and the impact of the rollout of simplified dolutegravir-based regimens in this population.
1203Sustaining Person-Centered Care Beyond COVID-19: Leveraging the Private Sector for Home-Based HIV Treatment in Jakarta, Indonesia
Jessie Olivia Yunus (presenting)1, Verry Adrian (presenting)2, Rahmat Aji Pramono2, Erika Indrajaya1, Dimas Kurnia1, Riska Apriliyanti1, Stefano Giovani1
1FHI 360 Indonesia, Jakarta, Indonesia
2Jakarta Provincial Health Office, Jakarta, Indonesia
Introduction: To ensure uninterrupted care for people living with HIV (PLHIV) during the COVID-19 crisis, the Provincial Health Office (PHO) in Jakarta, Indonesia pioneered home-based delivery of antiretroviral therapy (ART), assisting 9413 PLHIV to safely receive life-supporting medications at home between April 2020 and May 2022. As COVID-19 emergency provisions are coming to an end, the PHO and USAID/EpiC project have brokered a partnership with a private sector telemedicine platform, Good Doctor Technology Indonesia (GDTI), to extend and sustain this critical patient-centered service.
Description: Jak Anter, the home-based ART service introduced by the PHO and USAID/EpiC, utilized ride-based apps to make 23,620 drug deliveries to PLHIV in Jakarta during the COVID-19 pandemic. To sustain this service post-COVID, the PHO and USAID/EpiC approached GDTI, a telemedicine platform that provides over 10,000 teleconsultations a day in Indonesia. In collaboration with 12 targeted primary health facilities and five district health offices, the PHO and GDTI established a pilot partnership whereby eligible PLHIV can request home-based ART services directly through the GDTI interface. After a short online teleconsultation with a GDTI doctor, the platform will send an electronic message to the participating facility and activate the Good Doctor courier system, which will be dispatched to collect the medication and deliver it to the PLHIV client.
Lessons Learned: Integration of technology-enabled solutions into the existing healthcare infrastructure requires Government approvals for service flow, data security, patient communications, and confidentiality.
Recommendations: The collaborative efforts of the PHO, USAID/EpiC and GDTI offer a promising avenue for extending person-centered care to PLHIV beyond the immediate COVID-19 crisis. By harnessing the potential of these partnerships, the healthcare ecosystem can ensure continuity, accessibility, and quality in HIV care delivery while embracing the advancements brought forth by digital health solutions.
1214Co-Developing a Novel Campaign for Amsterdam's MSM at Risk of Late Diagnosis of HIV
Muhammad Sharjeel (presenting)1, Arjan van Bijnen2, Nina Schat3, John de Wit4, Udi Davidovich5, Godelieve de Bree6
1Amsterdam Institute of Global Health, Amsterdam, Netherlands
2SOA AIDS Nederland, Amsterdam, Netherlands
3H-TEAM / Amsterdam Institute for Global Health and Development, Amsterdam, Netherlands
4Utrecht University, Utrecht, Netherlands
5Public Health Service of Amsterdam, Amsterdam, Netherlands
6Academical Medical Centre Amsterdam, Amsterdam, Netherlands
Introduction: According to monitoring data from the Netherlands, MSM comprises the largest group of at risk of late diagnosis of HIV in Amsterdam, many of whom have diverse cultural backgrounds as shown in Table 1. This project aims to co-develop an innovative intervention with the MSM community that enhances HIV testing while addressing the challenges faced by a small yet culturally diverse group. (See table.)

Description: We identified three key determinants of delayed testing: low-risk perception, high perceived severity of HIV, and negative experiences of the AIDS epidemic through formative literature research and interviews of late presenter MSM. This project drew on the Behavior Change Wheel (BCW) to co-develop intervention with community MSM addressing key determinants of HIV testing among not recently tested MSM. The BCW approach proceeds through three stages: Understanding behavior using data and community insights identifying intervention options, and identifying behavior change strategies, content, and implementation options.
Lessons Learned: In collaboration with a community group of MSM, profiles of late presenters were translated into four distinct MSM personas (ie, combinations of personal characteristics and behavioral determinants). Through co-creation, we identified three matching behavior change strategies considered feasible, acceptable, and potentially effective: persuasive health communication, role modeling, and enablement. In the third stage, intervention options were translated into an online campaign applying a narrative-based approach. Furthermore, stories were developed for an online campaign: short films, key messages, and referral links to testing sites. The transformative journey, as depicted in the campaign, is expected to change the perceptions of HIV testing. Furthermore, a facility to obtain free self-tests at home was integrated into the campaign design to enable testing. (Short Film 1, Short Film 2)
Recommendations: The combination of BCW and community co-creation is promising for translating scientific knowledge and community insights into interventions with a promise of impact.
1218Prevention, Diagnosis, Treatment, and Monitoring of the Hepatitis C Virus in the Mobile Screening Unit “Saúde + Perto”
Gonçalo Bento (presenting)1, Maria Eugénia Saraiva (presenting)
1
, Sofia Melo Refoios1
1Liga Portuguesa Contra a Sida, Lisbon, Portugal
Background: Liga Portuguesa Contra a SIDA (LPCS) was founded in 1990 and since then provides care and support to People Living with HIV, Hepatitis and/or other Sexually Transmitted Infection (STI). LPCS main project regarding Prevention, Diagnosis, and Treatment of these infections is Mobile Screening Unit (MSU) “Saúde + Perto”. MSU aims to provide easy access to testing, counselling, diagnosis, care and treatment among key populations (MSM, Drug Users, Homeless people, Sex Workers and their clients, and Immigrants).
Method: This mobile unit goes through the councils of Lisboa, Loures, and Odivelas performing health screenings for HIV, Hepatitis B and C and other Sexually Transmitted Infections (STI). These screenings are all free of charge, confidential, and anonymous. The MSU has a multidisciplinary team composed by a doctor, a psychologist, a technical of screening analyses, and mediator.
Results: From 1/10/2014 to 31/03/2023, 10587 patients performed a screening session at the MSU: 5938 (56%) men, 4628 (43.7%) women and 21 (0.2%) transgenders, with an average age of 41.3 years (SD = 16.0), with 87% accepting an HCV screening session. Of 9183 HCV screening sessions, 524 patients had reactive results (88% accepted referral, 89% of these had an appointment, 374 patients confirmed diagnosis; 13% had antibody due to previous infection. Of 93% patients who started treatment (n = 212), 13% abandoned therapy. Of 242 patients who completed treatment, 206 are cured. (See table.)

Conclusion: Considering the synergy between STIs, co-infections between HCV and other STI were analysed. 96 patients had reactive screening for HCV and at least one other STI (18% reactive HCV). Of these 82 people, 45% live with this STI and HIV. More than 50% of these HCV infections belong to patients from key populations: 31,9% are Drug Users, 19,7% are Homeless People.
1239Health Coverage and Integrated Systems Are Important for Achieving HIV Viral Undetectability Efficiently After Rapid Treatment Start Among Migrant Populations
Anish Arora (presenting)1, Bertrand Lebouché (presenting)1, Kim Engler1, Serge Vicente1, David Lessard1, Edmundo Huerta1, Joel Ishak1, Nadine Kronfli1, Jean-Pierre Routy1, Joseph Cox1, Giada Sebastiani1, Benoît Lemire1, Lina del Balso1, Marina Klein1, Alexandra de Pokomandy1, Isabelle Vedel1, Amélie Quesnel-Vallée1
1McGill University, Montréal, QC, Canada
Background: There is limited data exploring the feasibility of rapid treatment initiation among migrants living with HIV (MLWH), who often experience numerous barriers to HIV care and treatment engagement. We sought to examine time-to-treatment and time-to-undetectability for MLWH enrolled in a program with free, on-site, and rapid treatment dispensation.
Method: In January 2020, we initiated a 96-week prospective cohort study at a hospital-based clinic in Canada. All patients received bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) for free and as soon as possible following care linkage. Median time to B/F/TAF initiation and viral undetectability from care linkage were calculated and compared between sub-groups via survival analysis (Kaplein-Meier and Cox regression with stratified bootstrapping).
Results: As of May 2023, data for 31/40 enrolled MLWH were available. Many participants were men who have sex with men (n = 16, 52%); from Africa (n = 14, 45%); and <39 years of age (n = 17, 55%). Ten participants (32%) had insufficient health coverage (ie, no coverage for HIV care and/or treatment). The median number of days to ART initiation was 0 (range: 0–42). The median number of days to viral undetectability was 60.5 (range: 0–379). Those with insufficient health coverage took a median of 30.5 days longer to reach undetectability (p = 0.002).
Conclusion: Lack of health coverage significantly delayed time to undetectability. Those without coverage were unable to receive free blood tests at our clinic. Instead, they attended other public health facilities that provide free tests. This potentially delayed time for conducting tests and receiving results, ultimately hindering efficient management in our clinic. Ensuring all people have HIV-related health coverage and that HIV-related services are well integrated seems critical to efficiently achieving HIV viral undetectability among MLWH.
1241Data Cleaning for a Large HIV Dataset: Experience from Dar es Salaam City, Tanzania
Lameck Machumi (presenting)1, Angelica Rugarabamu1, Moses Kehengu1, Fikiri Chisonjela1, Emmanuel Philipo1
1Management and Development for Health, Dar es Salaam, Tanzania
Introduction: While HIV programs in Sub Saharan Africa generate data from millions of patient visits, the quality of data is questionable since it is not always cleaned to meet operational research standards. We describe the process used to clean data for a large HIV care and treatment program in Dar es Salaam city, Tanzania.
Description: Tanzania uses a standard database (CTC-2) to manage HIV care and treatment services. Traditionally, data are recorded at the paper-based CTC-2 card by clinicians, then transferred to an electronic format by data clerks. Common sources for data errors include missing, out of range and illogical data. Dar es Salaam has more than 465,000 PLHIV registered, more than 180,000 active on ART and more than 11.5 million clinical visits. A standard operating procedure was developed to guide the data cleaning team. An online monitoring tool was developed to facilitate tracking of cleaning progress. Furthermore, a two-day training course involving theory and practical sessions was provided for data clerks. Data cleaning activity started in August 2022.
Lessons Learned: A total of 3,031,050 data errors were identified in the dataset. Among these 86.1% were due to missing data, 10% illogical data 3.5% were out of range data and 0.4% were wrong data. By the end of March 2023, 2,634,203 errors were cleaned which is equivalent to 87% of errors. We observed that most data errors resulted from lack of knowledge among clinicians and data clerks to identify and address data challenges on a daily basis.
Recommendations: For successful operational research, clean data is as important as the findings it represents. From this observation, we recommend training/mentoring data clerks, clinicians and enforcing mandatory daily cleaning of data in CTC-2 database.
1242Impact of COVID-19 on Biomedical and Non-Biomedical HIV Services Among Key Populations in Rwanda
Kabanyana Nooliet (presenting)1, Andrew Gasozi Ntwali2, Rwibasira Gallican3, Ayingoma Jean Pierre1
1Rwanda NGOs Forum on HIV/AIDS and Health Promotion, Kigali, Rwanda
2UNAIDS, City of Kigali, Kigali, Rwanda
3Rwanda Biomedical Center, Kigali, Rwanda
Background: At the advent of COVID19, stringent prevention measures were imposed by the Government of Rwanda. Prior to COVID19, Rwanda had made good progress in HIV response to reach epidemic control and close the gaps by 2020, where 76% of all HIV-positive adults (80% HIV-positive women) had achieved viral load suppression, a widely used measure of effective HIV treatment.
This paper discusses findings from an assessment aimed at identifying the impact of COVID19 on biomedical and non-biomedical HIV services among key populations (KPs).
Method: Qualitative methods with desk were used, examining the results obtained from the interviews conducted in selected communities of KPs including 63 FSWs, 42 MSM, 8 Transgender people, 14 PWUDS/PWIDs, CSOs for KPs and 10 healthcare providers. The sample size was drawn based on the proportion to the size of KPs per hotspot.
Results: HIV services that were affected include limited access to biomedical and structural prevention approaches, many KPs reported practice of unsafe sex due disruption of supply and distribution channels for health commodities. Clinic-based testing continued but restrictions of movement and gatherings hindered access to health facilities, limited access to self-testing tools. Clients who tested positive from self-tests were not immediately initiated to treatment, KPs who were on treatment abruptly and involuntarily discontinued treatement due to stockout of their medical supplies, lack of food and attendance for CD4 and routine VL testing was discontinued.
Conclusion: Results from the study demonstrate the need to assess further the preparedness of the public health system and the need for investment in readiness for response to future pandemics.
1244Revolutionizing HIV Testing and Care for Men Who Have Sex with Men in Nairobi, Kenya: A Tailored Approach to Overcoming Stigma
Joseph Omwamba (presenting)1, Shillah Mwavua2, Peter Memiah3
1Ishtar MSM, Nairobi, Kenya
2Nairobi County Government, Nairobi, Kenya
3University of Maryland, Baltimore, MD, USA
Introduction: In areas where homosexuality is stigmatized or criminalized, it is crucial to provide client-centered service delivery approaches to enable MSM to know their HIV status. Traditional community- and self-based HIV testing methods may not be fully observed, making personalized approaches all the more essential for effective HIV prevention and control efforts.
Description: Ishtar MSM is working in partnership with the Global Fund through KRCS to provide various outreach strategies for MSM in Nairobi County to access HIV testing, prevention, care, treatment, The organization has employed personalized approaches that utilize volunteer peer educators to promote HIV testing among MSM. Additionally, the organization has adopted social media approach strategies that involve online outreach workers, community social influencers, targeted campaign messaging, and dedicated dating sites. These platforms provide MSM with the opportunity to self-assess their risk behaviors towards exposure to HIV, hence leading them to seek testing services at MSM-friendly wellness centers.
Lessons Learned: Between April 2019 to May 2022, a total of 7308 MSM were tested. 378 were identified as HIV-positive and enrolled in care and treatment services. The implementation of personalized approaches resulted in a 13% increase in average quarterly case-finding rates. Through these efforts, there has been an improvement in HIV prevention, care, treatment, and support services over the course of the years.
Recommendations: Services provided for individuals at high risk of HIV infection are inadequate to meet their needs and keep them healthy, it may not be possible to end the AIDS epidemic in the community. To increase coverage of HIV programming among MSM, particularly in areas where they face discrimination, implementing various mobilization strategies proves helpful.
1248Sustaining HIV Care and Treatment Services During Disease Outbreaks: Lessons from Kagera
Lameck Machumi (presenting)1, Aidat Mugula1, Kuduishe Kisowile1, Aaron Nkini1, Emmanuel Sarakikya1
1Management and Development for Health, Dar es Salaam, Tanzania
Introduction: The outbreak of Marburg Viral Disease (MVD) in Kagera, Tanzania was confirmed by the Ministry of Health on 21st March 2023. As part of epidemiological measures to contain the disease, the MoH closed six health facilities providing HIV care and treatment services to more than 1345 clients, heightening the risk of interruption in treatment (IIT). IIT leads to negative HIV treatment outcomes such as increased risk of transmission due to viral load rebound, increased risk of loss to follow up, increased risk of virologic failure due to drug resistance and HIV disease progression. We describe interventions applied to sustain HIV care and treatment services and lessons learnt.
Description: We worked with Regional and Council Health Management Teams (R/CHMT) to implement alternative service delivery models to ensure continuity of treatment. These included relocating clients to alternative facilities, community ART delivery, using HIV self-test kits, and public awareness through posters to educate clients about the dangers of Marburg and available alternative services. As a result of these interventions, 96% of clients scheduled for clinic appointments before the outbreak were reached and provided with lifesaving ART.
Lessons Learned: Coordination with the Government at all levels for a successful response to outbreaks proved to be crucial. During this period, we noted the significance of community engagement and education to counter false rumors, misinformation, mistrust of healthcare providers as a strategy to gain confidence from the community. The outbreak also underscored the need for preparedness through training, planning and regular drills.
Recommendations: Emerging infectious diseases continue to threaten health systems globally, and particularly the gains made against long standing outbreaks such as HIV/AIDS and Tuberculosis. Carrying the lessons learnt through the MVD outbreak in Kagera is as crucial as strengthening health systems to withstand potential future outbreaks.
1253Tackling TB Among PLHIV: A Success Story in Screening and Prevention
Thitisant Palakawong Na Ayuthaya (presenting)1, Chantapat Brukesawan1, Sauwakon Pattharasikarin1, Nattinee Isarankura1
1Bangkok Metropolitan Administration, Bangkok, Thailand
Introduction: Public Health Center 28th, a primary care unit (PCU) under Bangkok Metropolitan Administration, has been providing free services for Tuberculosis (TB) and HIV patients since 2017. We are the first PCU in Bangkok to initiate antiretroviral therapy (ART) for people living with HIV (PLHIV). As of June 2023, we currently provide care for 4398 PLHIV.
Description: TB remains the leading cause of mortality among PLHIV. Therefore, we have implemented a comprehensive TB screening package for PLHIV. Our screening methods include TB symptom questionnaires, assessing contact history with TB patients, chest x-rays (CXRs), molecular techniques for sputum examination (GeneXpert), and TB culture tests at the initial visit. TB-negative PLHIV have undergone tuberculin skin testing or interferon-gamma release assays (IGRA) to screen for latent TB infection (LTBI). LTBI-positive individuals receive tuberculosis preventive therapy (TPT). Notably, no cases of active TB were detected among PLHIV after initiating ART at our PCU. However, three PLHIV referred to our PCU for continued ART subsequently developed active TB. We also employ TB symptom questionnaires during each visit and perform annual CXRs.
Lessons Learned: Between October 2017 and September 2022, we provided care for 3627 PLHIV, out of which 246 (6.8%) had TB/HIV co-infection. All 246 individuals successfully completed their TB treatment. Additionally, 671 (18.5%) PLHIV were diagnosed with LTBI, and all of them received TPT.
Recommendations: Implementing a systematic and comprehensive TB screening and prevention package for all PLHIV, including using TB symptom questionnaires during each visit, assessing contact history with TB patients, performing annual CXRs, utilizing molecular techniques for sputum examination, and culture tests. TB-negative PLHIV should undergo screening for LTBI and receive TPT if diagnosed with LTBI. These measures are crucial for managing TB among PLHIV and reducing TB-related morbidity and mortality.
1254Optimizing Primary Health Services for Integrated, Person-Centered Care in Jakarta, Indonesia
Jessie Olivia Yunus (presenting)1, Rahmat Aji Pramono (presenting)2, Aulia Human1, Erlian Rista Aditya1, Agus Aribowo1, Caroline Francis1
1FHI 360 Indonesia, Jakarta, Indonesia
2Jakarta Provincial Health Office, Jakarta, Indonesia
Introduction: In Jakarta, Indonesia, one third of people living with HIV (PLHIV) rely on primary health care facilities, known as “puskesmas,” for their HIV care. The Provincial Health Office (PHO), in collaboration with the USAID/EpiC project, is dedicated to improving the capacity of these facilities as they transition from isolated approaches to integrated, patient-centered care.
Description: This initiative employs a collaborative quality improvement approach that actively seeks client feedback and establishes community-facility partnerships to facilitate service access, uptake, and retention. To ensure an uninterrupted supply of essential HIV prevention and treatment commodities, decentralized supply chain mechanisms have been established. Site-level technical assistance is further tailored to address policy, capacity, logistics, and reporting barriers that hinder the effective implementation of HIV programmatic minimum standards.
By March 2023, 42 puskesmas in Jakarta enrolled at least 95% of newly diagnosed PLHIV, provided same day antiretroviral therapy (ART) to 70% of newly diagnosed PLHIV, initiated 97.5% of new-on-ART PLHIV on Tenofovir, Lamivudine, and Dolutegravir (TLD), and facilitated viral load (VL) testing for 100% of eligible PLHIV, with 96% achieving VL suppression. Eleven established private-public partnerships to extend home-based ART services, 12 facilities are providing PrEP, and 15 are distributing HIV self-test kits to index testing.
Lessons Learned: As puskesmas consistently achieve and maintain optimal performance across HIV programming standards, it becomes increasingly feasible to focus on service differentiation and integration. This includes offering multi-month dispensing and providing integrated service packages that address the specific needs of PLHIV.
Recommendations: To enhance access and coverage of high-quality care in Indonesia's health care system, it is essential to expand integrated, person-centered primary health care services offered at Jakarta puskesmas. This approach will contribute to the ongoing transformation of HIV care, ultimately improving the overall health outcomes and well-being of PLHIV in Jakarta and beyond.
1257Impact of the COVID-19 Pandemic on 95-95-95 Targets in 10 Fast-Track Cities
Sindhu Ravishankar (presenting)1, Helen Omowumi Olowofeso2, José M. Zuniga1
1IAPAC, Washington, DC, USA
2IAPAC, Lagos, Nigeria
Background: Fast-Track Cities are committed to attaining the Joint United Nations Programme on HIV/AIDS (UNAIDS) programmatic 95-95-95 targets by 2025. Disruptions in access to HIV services during the COVID-19 pandemic could have had an impact on progress against the 95-95-95 targets.
Method: 95-95-95 data from 10 Fast-Track Cities in North America (4); Europe (4); Asia Pacific (2) were analyzed using the following parameters: 1) Reported all three 95 targets from 2017–2021 inclusive; and 2) COVID-19 was first detected in the country between Jan-Mar 2020. The percent increase of the 95 targets was calculated for the period between 2017–2019 and the period between 2019–2021 to assess if the COVID-19 had an effect on the rate of progress against the 95-95-95 targets.
Results: 3 of the 10 cities indicated a greater or equal percent increase in the first 95 (diagnosis) target in 2019–2021 compared to 2017–2019. The average percent increase across the cities from 2017 to 2019 was 6.07% compared to 2.27% increase from 2019–2021. 3 of the 10 cities indicated a greater or equal percent increase against the second 95 (treatment) target in 2019–2021 compared to 2017–2019. The average % increase across the cities from 2017 to 2019 was 8.63% compared to a 4.99% increase from 2019–2021. 5 of the 10 cities indicated a greater or equal percent increase against the second 95 (treatment) target in 2019–2021 compared to 2017–2019. The average % increase across the cities from 2017 to 2019 was 7.01% compared to 1.48% increase from 2019–2021. (See Table.)
Conclusion: Overall cities made progress against the 95-95-95 targets during both the pre-pandemic and pandemic time periods; but at a slower rate during 2019–2021 pandemic period.
1260Applying Incidence-Prevalence Ratio to Define HIV Epidemic Control in 6 U.S. Fast-Track Cities
Sindhu Ravishankar (presenting)1, Helen Omowumi Olowofeso2, José M. Zuniga1
1IAPAC, Washington, DC, USA
2IAPAC, Lagos, Nigeria
Background: SDG 3.3 calls for ending the AIDS epidemic by 2030, which involves a reduction in incidence. Targets including the 95-95-95 treatment targets have garnered global consensus in working towards reducing HIV incidence and mortality; yet there lacks specific consensus on an incidence-focused goal though several metrics have been proposed. The Incidence-Prevalence Ratio (IPR) is one such proposed metric for defining epidemic control.
Method: The incidence prevalence ratio (Incidence/Prevalence) was calculated for 6 US Fast-Track Cities. Fast-Track Cities in the US were included based on availability of incidence and prevalence data on or after 2020. The threshold for having reached epidemic control was defined as 0.03, based on a meeting convened by the UNAIDS Science Panel. This threshold assumes average survival following HIV acquisition as 33 years. The threshold 1/33 (0.03) indicates the epidemic is controlled and in a state of decline; and above this indicates growth of the epidemic over time. The IPR data were considered proportion of PLHIV virally suppressed, which also would trigger a reduction in incidence.
Results: 3 of the 6 cities (Charleston, Denver, San Francisco) have achieved epidemic control based on IPR < .03. However, these cities were not necessarily the same cities with the highest proportion of PLHIV virally suppressed, which were San Francisco (70%), San Antonio (67%), and Denver (65%). Further, cities with the same IPR in some instances varied greatly in terms of proportion of PLHIV virally suppressed. For example, Austin and Houston both have an IPR of .04 but have 56% and 39% of PLHIV virally suppressed, respectively. (See Table.)
Conclusion: The incidence-prevalence ratio is a useful metric in considering the epidemic control but must be leveraged alongside other metrics, such as viral load suppression, which can also inform a cities’ success in incidence reduction towards zero new HIV infections.
1266Screening for Hepatitis B, Hepatitis C, and Human Immunodeficiency Virus Among Migrants Visiting the Center for Sexual Health and the Travel Vaccination Center of the Public Health Service of Amsterdam, the Netherlands
Ellen Generaal (presenting)1, Yara Bachour1, Annemarie Meiberg2, Nora Hamdiui2, Evelien Siedenburg1, Sara Klijzing1, Titia Heijman1, Akke Cornelissen1, Roel Toering1, Elske Hoornenborg1, Maria Prins1
1Pubic Health Service Amsterdam, Amsterdam, Netherlands
2National Institute for Public Health and the Environment, Amsterdam, Netherlands
Background: We evaluated the uptake and diagnostic outcomes of hepatitis B (HBV), hepatitis C (HCV) and human immunodeficiency virus (HIV) screening among visitors of the Center for Sexual Health (CSH) and the Travel Vaccination Center (TVC) of the Public Health Service of Amsterdam, who were born in endemic countries for these infections (‘migrants’).
Method: From June 2021-June 2022, 1172 visitors of the CSH born in an HCV-endemic country were offered testing for anti-HCV and HCV-RNA (HBV and HIV testing was previously implemented at CSH). From July 2022-April 2023, 385 visitors of the TVC born in an endemic country for one of these infections were invited for anti-HBc and HbsAg (HBV), anti-HCV and HCV-RNA (HCV), and HIV Ab/Ag testing.
Results: Participation rate among eligible visitors was high at both centers (n = 1051/90% at CSH; n = 289/75% at TVC). Visitors were mainly born in Suriname (30%) or Africa (15%) at CSH, and in Ghana (20%) and Suriname (15%) at TVC. At the CSH, we identified 6/1051 (0.6%) anti-HCV positive individuals, of whom 1/1051 (0.1%) had a new HCV-RNA positive infection and was successfully referred to care. At the TVC, we identified 6/289 (2.1%) new cases with a HbsAg-positive test result, and no new cases for HCV and HIV. Screening at both centers was easily implemented: ICT preparations were limited, and staff were trained to conduct counselling, testing, and patient referral to care.
Conclusion: Implementation of HBV, HCV, and HIV testing for migrants visiting the Public Health Service of Amsterdam is feasible. However, national implementation of this project is limited by financial costs and registration/privacy issues. Also, we only reached migrants who may have a positive attitude towards testing and prevention. Routine screening of HBV, HCV, and HIV within existing health care facilities is recommended for this key population, besides other efforts such as outreach activities.
1279Implementation of Virtual Outreach Services for HIV Prevention Among “at Risk” Population in Mumbai, India
Vijaykumar Karanjkar (presenting)1, Ramakant Biradar (presenting)1, Smita Chougule1, Shrikala Acharya1, Anil Shinde1, Amol Palkar1
1Mumbai Districts AIDS Control Society, Mumbai, India
Introduction: India has experienced massive growth in smartphone users especially among the youth. Community consultation revealed high use of dating apps among key population to find sexual partners. It is important to reach out to these ‘at risk’ individuals for HIV prevention services. Virtual Targeted Intervention was planned and implemented to cater to these individuals who seek sexual partners via virtual mode in Mumbai.
Description: Virtual Outreach workers (VORW) created profiles in the respective dating apps and social media platforms. VORW reached out to prospective clients with information on HIV, STI services along with behavior change communication and motivated the clients to access the services. VORW referred and navigated the ‘at risk’ clients to the nearest Integrated Counselling and Testing Centre for HIV/STI counselling and testing services. The clients found reactive were provided treatment at these clinics.
Lessons Learned: VORW reached out to virtual clients through 7 different dating applications. During the last two years, introductory messages were sent to 84385 clients; 13537 (16%) responded. 4232 clients took appointments, 1166 (27.6%) agreed for HIV & Syphilis testing, 617 (52.9%) tested for HIV & 30 (4.9%) clients were diagnosed with HIV. 313 (26.8%) clients were screened for syphilis & 53 (16.9%) clients were found to have syphilis. The clients were predominantly males in the age group of 18–34 years (93%).
The high detection of HIV and syphilis among ‘at risk’ clients reached through virtual outreach highlights the importance of virtual interventions. Client centric outreach, sensitization and training of facility staff are necessary for higher uptake of services. Further, VORW from the community had higher acceptance.
Recommendations: Implementing Virtual outreach strategies to deliver a comprehensive package of services along the entire HIV continuum for ‘at risk’ population is the need in the current context and needs to be scaled-up in the national HIV programme strategy.
1282Creating an Enabling Environment for Youth Living with HIV to Access Health and Well-Being: A Case Study in Four Rwandan Cities
Jean Berchmans Tugirimana (presenting)1, Deo Mutambuka1, Andrew Gasozi Ntwali2
1Rwanda National Network of People Living with HIV/AIDS (RRP+), Kigali, Rwanda
2UNAIDS, Kigali, Rwanda
Introduction: This study aimed to improve the accessibility of health services and promote the overall well-being of young people living with HIV (YLHIV) in the cities of Kigali, Musanze, Rubavu, and Muhanga in Rwanda. Specifically, the project focused on identifying the challenges faced by young female sex workers (FSWs), men having sex with men (MSM), and teen mothers (TM) in accessing HIV services.
Description: Implemented by the Rwanda Network of People Living with HIV/AIDS (RRP+), this project received technical and financial support from the German Agency for International Cooperation (GIZ). A total of 133 YLHIV participated in peer education support groups, where they shared their perceptions regarding the barriers to achieving the three 95 UNAIDS objectives. The Well-Being Index developed by the World Health Organization (WHO) was employed for a rapid assessment of the mental health of the youth. The findings and recommendations resulting from this study were discussed in community and national dialogues, bringing together rights holders and duty bearers.
Lesson Learned: Improved communication regarding the viral load, enhanced confidentiality measures in health facilities, and addressing food insecurity were identified as crucial factors for increasing testing, self-care, adherence to treatment, and reducing HIV transmission. Consequently, recommendations were formulated based on these findings.
Recommendations: To create a more youth-friendly environment and empower YLHIV to make informed decisions, future interventions should encompass research activities, adjustments in health systems, and peer-facilitated mechanisms. These efforts should aim to provide comprehensive information, mental health support, and foster youth empowerment. Furthermore, advocating for the respect of human rights is crucial. The UNAIDS – Rwanda presents an opportunity to leverage the findings of this study and continue progressing towards a more inclusive environment for all YLHIV.
1283STI Incidence and Retention in Care Among Priority Populations Participating in the National HIV Pre-Exposure Prophylaxis (PrEP) Pilot Program in Amsterdam, the Netherlands
Eline Wijstma (presenting)1, Vita Jongen1, Anders Boyd1, Henry J.C. de Vries2, Maarten Schim van de Loeff1, Maria Prins1, Elske Hoornenborg1
1Public Health Service of Amsterdam, Amsterdam, Netherlands
2Amsterdam Infection and Immunity Institute (AI&II), Amsterdam, Netherlands
Background: The Dutch national HIV pre-exposure prophylaxis (PrEP) pilot (NPP) provides subsidized PrEP care through Centers for Sexual Health (CSH). In Amsterdam, people less likely to access PrEP elsewhere received priority access to the NPP: those <25 years, transgender and gender-diverse (TGD) people, sex workers, migrants from low- and middle-income countries (LMIC) and those uninsured. We aimed to assess behavioral risk for HIV by priority criterion by comparing incidence of sexually transmitted infections (STI) and compared program retention by priority status.
Method: We used data from PrEP visits and additional STI visits among HIV-negative individuals starting PrEP at the CSH-Amsterdam (July 2019-February 2023). We compared incidence of any STI (ie, chlamydia, gonorrhea or infectious syphilis) by presence or absence of each priority criterion using incidence rate ratios (IRR), adjusting for STI testing frequency and the other priority criteria. We calculated the hazard ratio (HR) for loss-to-follow-up (ie, last PrEP visit more than 6, 7, 8 or 9 months before February 2023, in case of an agreed-upon follow-up interval of 3, 4, 5, or 6 months, respectively) between those meeting ≥1 versus zero priority criteria, adjusting for year of NPP enrolment.
Results: Among 4061 clients (n = 1991 meeting ≥1 priority criterion), STI incidence was 85.6/100 person-years. STI incidence was higher among those <25 years (n = 867, aIRR = 1.30 [95% CI = 1.15–1.46]), doing sex work (n = 388, aIRR = 1.39 [1.18–1.65]), uninsured (n = 201, aIRR = 1.24[1.03–1.50]), or born in an LMIC (n = 1198, aIRR = 1.18[1.09–1.29]), and lower among TGD clients (n = 228, aIRR = 0.62[0.49–0.79]), compared to clients not meeting the respective priority criterion. N = 1096 individuals were lost-to-follow-up (IR = 18/100 person-years). Loss-to-follow-up was more common among participants meeting ≥1 priority criterion than those meeting zero criteria (aHR = 1.63[1.40–1.89]).
Conclusion: STI incidence was higher and PrEP program retention lower among populations prioritized for program inclusion. PrEP programs with limited capacity should continue prioritizing populations vulnerable to adverse health outcomes, but interventions to improve PrEP retention among these populations are needed.
1299No Child Left Behind! eThekwini District AIDS Council Empowerment of Community Through Collaboration, Coordination, and Capacitation of Civil Society to Operationalize the Sevilla Declaration for the Benefit of Children
Chalone Savant (presenting)1, Nthabiseng Malakoane2, Roger Tevan3, Theressia Ndlovu4, Rekha Nathoo5
1IAPAC, Durban, South Africa
2eThekwini Municipality, eThekwini, South Africa
3Health Systems Trust, Westville, South Africa
4eThekwini PLHIV Sector, Durban, South Africa
5Children in Distress Network (CINDI), Pietermaritzburg, South Africa
Introduction: With only 52% of the world's children living with HIV (CLHIV) on HIV treatment, South Africa has joined other countries committing to the Global Alliance for Ending AIDS in Children by 2030. In March 2022, eThekwini had an estimated 20,047 CLHIV (under 15): 80% diagnosed, 59% on ART and 62% virally suppressed.
In 2022, eThekwini Mayor Kaunda committed to linking 3000 CLHIV to care as a Fast Track Cities initiative. The eThekwini District AIDS Council identified challenges including lack of a functional children's sector and need for coordinated collaborative multisectoral efforts to raise awareness and reach CLHIV. In January 2023, Mayor Kaunda signed the Sevilla Declaration, promising to support community capacitation and leadership of HIV responses including those for CLHIV.
Description: Numerous activities have been implemented to improve CLHIV outcomes, including dialogue around important issues (stigma, disclosure), and coordinated collaboration between stakeholders (Departments of Health, Social Development, and Education and People Living with HIV (PLHIV), Children, Women, Men, NGO, and Faith sectors).
Lesson Learned: Collaborative workshops provided platforms for sharing data, strategies and interventions. Databases were developed facilitating communication. A Children's Sector leadership election was held. Civil Society leaders began collaborating as “united sectors,” toward common goals.
These activities served as a catalyst for capacity strengthening. Children's Sector and PLHIV Sector leaders were included in a significant DOH workshop on pediatrics. IAPAC has trained children's sector and PLHIV leaders to facilitate a Conversation Map tool, sparking dialogues around CLHIV left behind.
Recommendations: Municipal AIDS Councils are key facilitators of sector development, collaboration, and coordination enabling an effective CLHIV response. Communication, mobilization, bilateral consultation and partnership between Civil Society and government, and capacity building foster mutual ownership motivating and empowering stakeholders. Such activities operationalize the Sevilla Declaration and are recommended for the CLHIV response.
1303London HIV Empowerment Programme
Steven Solasta (presenting)1, Maria Vidal-Read (presenting)1
1Healthy London Partnership, London, England, United Kingdom
Introduction: In April 2022, London Fast Track Cities launched an Empowerment Programme to tackle HIV-related stigma by supporting people living with HIV to develop resilience, confidence, and other skills to tackle self-stigma.
Description: Voluntary sector organizations were commissioned to deliver six projects over a one-year period. A variety of methods and approaches were used to address self-stigma, improving participants wellbeing while also building confidence and self-esteem, including in-person and virtual workshops, life coaching courses, women-only spaces, a co-designed magazine, collaborative podcasts, and peer-to-peer. The key outcomes for participants were to develop a support network, understand HIV, living well, internalized/self-stigma, build self-acceptance, self-esteem, and an individual's sense of power.
Lesson Learned: Independent facilitation enhanced delivery, supporting group discussions. Flexibility on duration of sessions to meet varying levels of enthusiasm to stay in discussion and keep learning. Learning around HIV treatment and U = U was best delivered conversationally, using simple language. Sufficient focus on the social consideration of living with HIV such as telling new partners about HIV status was important. There was some benefit in groups protected for certain cohorts such women's groups. However, there was value in providing more diverse groups, allowing participants to appreciate and tackle their own unconscious bias, preconceptions or stereotypes.
Recommendations: Future projects should encourage organizations to work more closely together to ensure those who are eligible are signposted to the most appropriate group. This should be supported by a shared digital library to support collaboration and learning. Consideration should be given to provision of women only spaces to enable women to talk about family planning and safety. Programmes should signpost to financial and social support services so that people can be directed to the help they need outside of the course. Supervision support is needed for facilitators, particularly for vulnerable participants experiencing trauma or suicidal ideation.
1305Interventions in the Context of a Suspected HCV Outbreak Among Men Who Have Sex with Men in Barcelona
Carles Pericas Escalé (presenting)1, David Palma2, Adrià Arconada1, Pere Simón1, Vicente Descalzo3, Eva Masdeu1, Cristina Domingo1, Isabel Moreira1, Lidia Arranz1, Cristina Rius1
1Public Health Agency of Barcelona, Barcelona, Spain
2Consorcio Centro de Investigación Biomédica en Red (CIBER), Barcelona, Spain
3Drassanes - Vall d'Hebrón, Barcelona, Spain
Introduction: Barcelona is a city with specific social and economic characteristics that materialize in very tight sexual networks. This entails high incidences of all sexually transmitted infections (STIs). A decreasing use of condoms and changes in sexual behavior, such as chemsex, have been observed among men who have sex with men (MSM). The objective is to describe the interventions carried out by the Public Health Agency of Barcelona to respond to a suspected HCV outbreak among MSM.
Description: In early 2023, different hospitals notified an increase in diagnoses of HCV among MSM (Figure 1), being all of them either PrEP users or HIV (+). The initial hypothesis of the route of transmission was the use of anal douches without disposable head in a sex club, but it was discarded after checking that only 10% of cases frequented the suspected club. The new hypothesis was a general increase in new cases among MSM who do not use barrier methods. A joint campaign with grass-roots organizations was launched in June 2023 which included posters (Figure 2) in clubs and saunas and announcements through sociosexual apps. The campaign was aimed at promoting screening, raising awareness on how HCV can be transmitted and providing information on how to get proper care if necessary.


Lesson Learned: HCV increase among MSM might be favored by sexual practices with potential blood sharing or bleeding. Testing of PrEP users and HIV (+) individuals helps with early detection. Baseline incidence for HCV might become higher in the upcoming years. Targeted interventions work well to provide information on prevention and testing resources.
Recommendations: It is essential to carry out proactive surveillance to advance in HCV eradication. Efforts need to be directed towards key populations and focused on outreach campaigns that provide non-stigmatizing information in places and events in which condomless sexual practices can take place. (See figure 1.)
1306Strengthen the 95-95-95 Cascade Focusing on Recently-Released Individuals: Program Description in Maputo Municipality
Teles Nhanombe (presenting)1, Alice Abreu1, Belia Xirinda1, Everilde Chilundo1, Vasco Nhanengue1, Yolanda Manuel2, Luis Elias3
1Maputo Council, Maputo, Mozambique
2IAPAC, Maputo, Mozambique
3Fast-Track Cities Institute, Maputo, Mozambique
Introduction: Maputo City has an estimated population of 1.2 inhabitants and, like other Mozambican provinces, faces the challenge of the widespread HIV epidemic. The city has the third highest HIV prevalence (16.2%) among adults. As part of the commitment to achieving the 95-95-95 UNAIDS HIV targets by 2030, the city has prioritized key populations, including prisoners and released from prisons, to eliminate the HIV epidemic.
Description: To retain released these KP in care, the city has developed a follow-up program for the post-release period – during their reintegration into the community – where ex-prisoners from the Preventive Penitentiary establishments in Maputo city and province are closely followed to ensure their adherence to and retention in ART. To that end, all public Health Facilities (HF) in the city were eligible to receive former inmates, and healthcare providers were trained to better approach this group. We analyzed disaggregated data from Maputo's Electronic Patient Tracking System in the HF from 2019 to 2022.
Lesson Learned:

There was an increase of more than 200% in ex-prisoners initiating ART from 2020 to 2022.
Although stigma and discrimination are common among KP, data shows an increase in ex-prisoners adhering to treatment and care after introducing the strategy.
Our target is to reach 95-95-95, in the third 95, in 2020, all patients under ART with viral load test came with viral load suppression. (See table 1.)
Recommendations: We recommend (a) building SRRH & HIV integration inside penitentiaries to better link recently released individuals to care with low costs; (b) promoting SRRH, including HIV should begin in prisons and continue after release; and (c) ensuring post-release support to former inmates so they can connect with HF, given that stigma and discrimination continue to influence their retention in care negatively.
1308Addressing Stigma and Public Trust: Lessons from the UK 2022 Mpox Outbreak
Colette Biesty (presenting)1, Charlotte Hemingway1, Miriam Taegtmeyer1
1Liverpool School of Tropical Medicine, Liverpool, England, United Kingdom
Background: In 2022 the UK experienced an Mpox outbreak, disproportionately affecting gay, bisexual, queer, and other men who have sex with men (MSM). Stigmatization and poor knowledge can worsen health outcomes and exacerbate existing health inequities during a disease outbreak. This project assessed public health messaging during the recent Mpox outbreak and how it influenced experiences of stigma and health seeking behavior in Liverpool.
Method: We used a participatory health research approach to assess and co-produce improved communication strategies for infectious disease outbreaks. Primary data consisted of nine semi-structured interviews with key stakeholders involved in the 2022 UK Mpox response, and four focus groups with priority populations of men who have sex with men (MSM) in Liverpool from: migrant communities; sex positive individuals; and university students. Purposive recruitment via community organizations and subject experts was supplemented with snowballing to obtain a wide range of relevant perceptions.
Data were analyzed using a general inductive approach. Research activities were informed by Stangl's health stigma and discrimination framework, and inductive themes emerged throughout analysis.
Results: Three major themes emerged: preference for anti-paternalism and honesty in public health communication; reduced public trust in governmental bodies; key role of community champions and the third sector in information dissemination; and the lasting impact on populations following recent COVID-19 self-isolation measures; and historical HIV communication campaigns with MSM communities. Insights were translated into a set of good practice recommendations for community-based public health communication.
Conclusion: The 2022 UK Mpox outbreak highlighted lessons learned in public health communication of emerging infectious diseases, as well as shortcomings of equitable health communications. These recommendations will support future public health communications for infectious disease outbreaks, to help guide practitioners when working with groups that already experience stigma and have the potential to be marginalized or discriminated against.
1309Local Strategy on HIV, STIs, Viral Hepatitis, Sexual Health, Sexual Diversity, Vulnerable Populations and Stigma in Alcorcón
(Madrid – Spain)
Julian Alexander Portocarrero Nuñez (presenting)1, Alexandra Jimenez Rodriguez1, Juan Emilio Losa García2, Reyes Velayos3, Mónica Morán Arribas4, Carlos Cevallos García5, Helena Martín6, Tamara de la Mora Amengual7, Claudio Domínguez1, Inés De la Fuente Hermosín8, Ángel Lizcano Álvarez9, Pablo Trapero10, Ivan Quiroga11, Maria Victoria Melendez Agudin1, Juan Azorín Serrano1, Ana Iriarte12, Jorge Beltrán13, Luis Rosales14, Carlos Iniesta Marmol15, Paulina Ramirez16, Almudena García17, Begoña Gallego18, Kierstie Watt19
1Alcorcón City Council, Alcorcón, Spain
2Alcorcón Hospital, Alcorcón, Spain
3State Coordinator for HIV/AIDS (CESIDA)
4Prevention and Early Diagnosis Program for HIV and STIs, Madrid, Spain
5Epidemiological Surveillance of HIV/AIDS, Madrid, Spain
6Red Cross, Madrid, Spain
7Social Services, Alcorcón City Council Icíar, Alcorcón, Spain
8Primary Care Centers, Alcorcón, Spain
9Rey Juan Carlos University, Madrid, Spain
10Fuenla Entiende LGTB, Madrid, Spain
11Local Police Alcorcón, Alcorcón, Spain
12Cadena SER, Madrid, Spain
13Kif-Kif NGO, Madrid
14LGTBIphobia Observatory Madrid, Madrid, Spain
15Sociedad Española Interdisciplinaria del SIDA (SEISIDA), Madrid, spain
16University of Alcalá, Madrid, Spain
17Apoyo Positivo, Madrid, Spain
18LGTBIPOL, Madrid, Spain
19Amar Dragoste, Madrid, Spain
Introduction: Alcorcón is a Spanish town of 170000 inhabitants, and one of the first five in Comunidad Madrid on HIV diagnoses. Joining FTC (2021), unanimously approved by the municipal plenary session, the strategy began, aligned with SDG 3.3
Description: The epidemiological situation, resources and vulnerability were assessed to develop collaborative actions aimed at specific groups in prevention, early diagnosis, training, awareness, sexual health, sexual diversity, vulnerability, stigmas, and community participation
Lesson Learned: HIV: Between 2012 and 2019 the incidence of diagnoses (x100,000 inh.) went from 14 to 7; late diagnosis went from 33% to 64%, being higher in immigrants (>50% vs < 30%), women (48.1% vs 38.4%) and >40 years (>40% vs < 40%). (See table.)
Factors of vulnerability and stigma detected/reported:
Diagnostic barriers associated with origin, gender, age, and social exclusion
Aging PLHIV (57.0% > 50 years)
Primary Care ignorance/reluctance about PrEP.
Sensitization about suspicion/detection/record of hate situations
Collaborative actions (>20 stakeholders) aimed at:
Professionals working with key populations: Training in sexual health/diversity/rights and awareness in incidents detection. Reached: Social Services, Addiction Center. Next: Police, Health Centers.
Youth: Education on sexual health and diversity. Reached: schools, university, NGOs.
LGTBQ + population: promotion of inclusion, awareness among professionals and population.
Vulnerable: coordination in a rapid circuit of recruitment-diagnosis-treatment.
Municipality: Actions and resources posted in town media. Testing Devices. Adherence to the Seville Declaration
Recommendations:
Late diagnosis: profile-driven testing, enhance fixed devices
Stigma and adherence: Assess including variables in the survey and assess the impact of long-acting treatment
Hate incidents: Sensitization in suspicion/detection and approach. Join the HIV Social Pact and the LGTBphobia Observatory. Coordination with organizations in gender violence
Older PLHIV: Assess frailty risk for inclusion in prevention program
PrEP training in healthcare centers
1311Leveraging Total Quality Leadership and Accountability (TQLA) Framework to Boost COVID-19 Vaccine Uptake Among People with HIV in Fast-Track City of Sinda, Zambia
Harsh Agarwal (presenting)1, Gabriel Kibombwe2, Thierry Malebe2, Harsh Agarwal2, Mbau Matuwa2, Mulenga Chilambwe2, Elliot Phiri2, Alan Kachuka3, Morai Morei Kasompola3, Mathias Simwinga4
1UNC Chapel Hill, Chapel Hill, NC, USA
2FHI 360, Lusaka, Zambia
3Petauke District Health Office, Petauke, Zambia
4Centre for Infectious Disease Research in Zambia (CIDRZ), Petauke, Zambia
Introduction: Covid-19 vaccinations are safe and critical for people with HIV (PWH) who could be vulnerable to worse outcomes of covid-19 from possible immunosuppression and high comorbidities. We found low Covid-19 vaccine coverage in Sinda (Zambia) for PWH receiving care through a PEPFAR program.
Description: We interviewed facility personnel to uncover factors driving low Covid-19 vaccinations; and implemented TQLA inspired adaptive strategies. We also used an interrupted time series (ITS) analysis to examine completion of cumulative annual target monthly.
Lesson Learned: Low vaccine uptake was attributed to reasons like client refusal because of uncertainty regarding vaccine efficiency, differentiated community delivery models and hence less footfall, unaccompanied adolescent and young people unable to legally consent to vaccinations, no proofs of first dosage, for clients already vaccinated through mobile vans but records not updated in COVID-19 Vaccines Global Access (COVAX) portal. Further, some PWH vaccinated and recorded in COVAX system were not updated in SmartCare (national electronic health record system for PWH), creating further bias in reporting.
We hence utilized our Monitoring and Evaluation Associates, Client Experience Associates, Covid champions to track appointments and line-listing the eligible PWH. PWH were contacted by phone and counseled, demystifying the Covid-19 vaccination. Supervised community follows up were conducted for those not reached by phone and SmartCare was triaged with COVAX tracker. We analyzed the pre (January 2022 to April 2022) and post intervention (May 2022 to April 2023) data. Following the intervention in May 22, we found over 2000% increase in average number of eligible PWH vaccinated for Covid-19, increasing from average of 23 PWH vaccinated per month to 554 (p = .01).
ITS analysis found a statistically significant difference in the slope for the monthly annual target status (p < .001), indicating a continual increase in pace towards completing the target post intervention.
Recommendations: We recommend closely monitoring vaccination uptake among PWH and practicing adaptive management to identify gaps, devise strategies, implement and learn cyclically to continuously optimize service delivery provisions.
1314Longitudinal Trajectories of Sexual Behavior and Incident HCV Re-Infection Among Men who Have Sex with Men with HIV in the Netherlands: Findings from an Observational Cohort Study
Kris Hage (presenting)1, Kalongo Hamusonde2, Anders Boyd1, Daniela Van Santen1, Astrid Newsum1, Marc van der Valk3, Kees Brinkman4, Arends Joop5, Fanny Lauw6, Bart Rijnders7, Arne van Eeden8, Luisa Salazar-Viscaya2, Janke Schinkel3, Maria Prins1
1Public Health Service of Amsterdam, Amsterdam, Netherlands
2University of Bern, Bern, Switzerland
3Amsterdam UMC, Amsterdam, Netherlands
4OLVG, Amsterdam, Netherlands
5UMC Utrecht, Utrecht, Netherlands
6MC Jan van Goyen, Amsterdam, Netherlands
7Erasmus UMC, Rotterdam, Netherlands
8DC Klinieken Lairesse, Amsterdam, Netherlands
Background: Men who have sex with men (MSM) remain a key population for hepatitis C virus (HCV) re-infection owing to sexual practices associated with HCV transmission. Little is known on how these behaviors evolve over time and whether they are associated with HCV re-infection. We aimed to identify subgroups of MSM with HIV with different patterns of HCV-related sexual behavior over time and assess re-infection risk within subgroups.
Method: We included MSM at risk for HCV re-infection following successful HCV treatment or spontaneous clearance using data from the Dutch observational MOSAIC study (2009–2018). HCV risk behavior was assessed using the validated HCV-MOSAIC score (range = 0.0–7.0); ≥ 2 indicating high re-infection risk. Subgroups were inferred using latent process mixed-effects, modelling HCV-MOSAIC score on age, group sex and casual partnership. HCV re-infection risk for each latent process was jointly modeled with a class-specific survival model.
Results: Analyses included 123 MSM. At first visit at risk for re-infection, median age was 45 years (IQR) = 41–50) and 113 persons had been treated for initial HCV infection, among which 59% were successfully treated with interferon-based regimen. Over a median follow-up of 2.7 years (IQR = 1,2–4,7), we identified two classes: one with lower HCV-MOSAIC scores (C1, n = 67), and one with higher HCV-MOSAIC scores with wider variation (C2, n = 56) (Figure 1A). In the first 3 years of follow-up, probabilities of not being HCV re-infected were similar between classes but diverged thereafter to 0.73 (CI = 0.61–0.87) in C1 and 0.47 (CI = 0.31–0.72) in C2 at year 5 (Figure 1B).

Conclusion: Despite continuous high-risk behavior in half of MSM, HCV re-infection in this group only becomes more frequent after 3 years of follow-up which may imply waning immunity following previous HCV infection. To curb HCV transmission, continuous monitoring of sexual behavior and HCV-RNA is essential among MSM with HIV at high risk for HCV re-infection.
1325Fast Track's Catalyzed Decentralization of Medical Services and Innovations: Sustained HIV Response in Kyiv City in War Emergency Situations
Nataliya Salabai (presenting)1, Vitaliy Kazeka (presenting)2, Mykola Povoroznyk3, Valentyna Ginzburg4, Oksana Gorbachuk2
1UNAIDS, Kyiv, Ukraine
2Kyiv Municipal Hospital #5, Kyiv, Ukraine
3Kyiv City State Administration, Kyiv, Ukraine
4Health Care Department, Kyiv City Council, Kyiv, Ukraine
Introduction: At the beginning of 2022, ART in Kyiv was available for 12,920 people at 40 sites, including 12 municipal pharmacies and MAT – for 2877 people at 7 sites. After the full-scale invasion on February 24, 2022, the number of ART and MAT sites in Kyiv decreased to 10 and four respectively. The number of medical personnel who continued to work has halved. A curfew was introduced in the city, all the bridges were closed, and public commute was stopped. The main challenges at the most critical stage of warfare in Kyiv city were the retention of patients who were already on treatment and active enrollment of internally displaced representatives of key populations and PLH in preventive and treatment services.
Description: Remained sited served remained patients; drugs were dispensed through the pharmacies to 1350 people; telemedicine was actively applied, and 11,535 online consultations were conducted. Support of the non-governmental organizations in the delivery of drugs by taxi and mailing through post ensured ARV drugs reached 853 isolated people in the first, most difficult months of the war. Almost 90% of MAT patients were receiving 30-days take-home supply during the most critical months of war.
Lesson Learned: During the most difficult period of hostilities, thanks to the decentralization and innovations being implemented as part of the Fast-Track initiative, and the mobilization of support from the non-governmental sector, the continuation of ARV and MAT treatment was ensured almost without loss and to maintain access to testing for the population of Kyiv, including internally displaced persons.
Recommendations: Such measures of Fast-Track Strategy as treatment decentralization, multi-month dispensation of ART, telemedicine, pharmacy dispensing, support from NGOs in delivering drugs might be applied for maintaining response in the circumstances of emergency.
1331Addressing TB in Durban's High Risk Homeless and Drug User Population: A Mobile X-Ray Testing Initiative
Percy Gumede (presenting)1, Michael Wilson1, Amanda Brumwell1
1Advance Access & Delivery, Durban, South Africa
Introduction: Durban, in South Africa's KwaZulu-Natal province, faces urgent public health concerns with its large, unhoused population, including high rates of drug use, addiction, tuberculosis (TB), and HIV. South Africa has a significant HIV burden, affecting 18.8% of adults. Addressing the bidirectional relationship between HIV and TB requires prioritizing TB screening, diagnosis, and linkage. Durban's CBD has witnessed a substantial increase in homelessness, reaching an estimated 16,000 individuals in 2022 from 8000 in 2017.
Description: The Bellhaven Harm Reduction Centre, in collaboration with the Department of Health, and LTE Medical Solutions conducted a 12-day mobile x-ray testing initiative in Durban's CBD. Screening 435 individuals, 112 (26%) had abnormal x-rays, with 45 (40%) suggesting TB. The initiative targeted shelters, hostels, and frequented spaces to provide rapid diagnostics and healthcare access.
Lesson Learned: The mobile x-ray testing initiative identified a significant number of potential TB cases (9%), emphasizing the urgent need to address TB in people living with HIV. Challenges arose in ensuring clinical evaluation for those with abnormal x-ray results, but collaborative efforts and comprehensive screening methods helped overcome them. Notably, 6 individuals (13%) had abnormal x-ray findings but tested negative for TB using Gene Xpert, highlighting the importance of employing multiple diagnostic tools.
Recommendations: Based on findings and lessons learned, we recommend a multi-faceted approach to address TB and HIV among Durban's homeless population. This includes targeted resources, enhanced stakeholder collaboration, and innovative strategies for holistic care. Allocating sufficient resources for prevention, screening, and treatment programs tailored to the homeless is crucial.
1337Tests on Bergamo Population: The Experience of Bergamo Leaves No One Behind and of Checkpoint
Davide Meli (presenting)1, Ilaria Mercurio (presenting)2, Paolo Meli3, Caterina Pellegris2, Franco Maggiolo4
1Cooperativa Don Giuseppe Monticelli, Bergamo, Italy
2Bergamo Fast-Track City, Bergamo, Italy
3Associazione Comunità Emmaus, Bergamo, Italy
4ASST Papa Giovanni XXIII, Bergamo, Italy
Background: On 2019 Bergamo become Fast Track City accordingly a checkpoint was opened on June 2020 and offer tests for HIV HCV and Syphilis one day for week. On June 2022 the project Bergamo Leaves No One Behind (BGLNOB) started with the purpose to screen people who live in situations of poverty and to help in the eventual linkage to care
Method: Test Data were collected with the Cobatest questionnaire.
Results: Tests are offered at the Checkpoint or during target events. In BGLNOB tests are offered in six NGOs workplaces that deal with poor people. In four years, we made:
5786 HIV test, founding 21 new infections: incidence is 0,36%;
5202 HCV test, founding 29 new infections: incidence is 0,56%;
5081 Syphilis test, founding 25 new infections: incidence is 0,49%

From September 2022 to May 2023 BG Checkpoint tested 1817 people: 2 positives for HIV (0,1%) 3 positives for HCV (0,1%) 5 positives for Syphilis (0,3%). All positivity had been linked to care.
During the same period in BGLNOB have been tested 280 people. The new diagnosis has been: 7 for HIV (2,5%) with 5 linked to care; 8 for HCV (2,8%) with 5 linked to care; 5 for Syphilis (1,8%), all linked to care. (figure 1)
The totality of data recorded that 60% of population is less then 30 years old, most male, many people were on their first test especially under 30 years old. (figures 2 and 3)
Conclusion: The results of BGLNOB project show the importance of increasing Test and Help for targeted key populations.
Otherwise, the work at the checkpoint underlines the importance to offer tests among general population, with regard to young people, that has also an educational role, allow to reduce stigma e generates awareness.
1344Analyzing the Implementation of Tuberculosis Preventive Therapy with the 3HP Regimen in Urban Maputo
Yolanda Manuel (presenting)1, Eveza Obra Bires1, Belia Xirinda2, Luis Elias3
1IAPAC, Maputo, Mozambique
2Maputo City Municipality, Maputo, Mozambique
3Fast-Track Cities Institute, Maputo, Mozambique
Background: Tuberculosis Preventive Therapy (TPT) is a priority in achieving targets outlined in WHO END TB Strategy, especially in high-burden countries like Mozambique. Scaling up shorter TPT, such as once weekly isoniazid–rifapentine (3HP) taken for three months, was adopted in Mozambique as one of the critical strategies. The 3HP was experimentally introduced in 2022, and Maputo city was one of the two selected cities to administer this prophylaxis.
Method: Data were available on an electronic database, collected at 26 health facilities (HF) in Maputo. The 3HP was administrated to all adults – 15 years old or older – starting on ART and those identified as TB contacts from March 2021 to June 2022, with the assessment of the end of their TPT by October 2022.
Results: 1.691 individuals were identified as TB contacts, and 91% have started the TPT. 41.3% of the TB contacts were eligible and initiated the 3HP. Almost 30% have completed this once-a-week treatment to prevent TB. Patients who started the ART were also evaluated on their eligibility for TPT. Of the 23.199 patients initiated on ARV during the evaluation period, 98% were screened for TB. Half of the patients screened have started the TPT, with 94% eligible for prophylaxis with 3HP. Of those, only 13% have completed TPT.
Conclusion: PLHIV starting ART, are being routinely screened for TB, and those eligible received TPT. However, treatment completion is not as high as expected, even using a shorter TPT regimen such as the 3HP, probably due to weak counseling on TPT adherence/completion by the healthcare providers; weak monitoring of 3HP adherence; and the monthly absenteeism from work, to collect the 3HP at the HF. There is a need to increase literacy about the importance of TPT; build capacity to monitor TPT adherence; and implement tailored strategies to target known barriers to completing TPT.
1347Quality of Care Survey Among PLHIV in Maputo: Poor Understanding of Undetectable Viral Load as a Challenge to Actioning the “Undetectable = Untransmissible” Message
Imane Sidibe (presenting)1, Yolanda Manuel (presenting)2, Savaiva Munguambe2, Karen Chale3, Mariam Diallo1, José M. Zuniga1
1IAPAC, Washington, DC, USA
2IAPAC, Maputo, Mozambique
3IAPAC, Lusaka, Zambia
Background: HIV care and treatment literacy, especially around the importance of adhering to ART to achieve viral suppression, is key in improving health outcomes. Poor understanding among PLHIV regarding the therapeutic and preventative benefits of achieving an undetectable viral load is a key challenge in actioning the “Undetectable = Untransmittable” (U = U) messaging.
Method: A 36-question survey was fielded in Maputo to assess the quality of care (QoC) provided to PLHIV. The survey assessed QoC across eight domains: HIV understanding, HIV counseling, linkage to HIV care, engagement in HIV care, ART literacy and ART adherence, secondary HIV prevention, whole person care, and interpersonal communication. Approval from the Mozambique Biomedical Research Ethics Committee for Health (CNBS) was obtained, and the survey was fielded across 21 health facilities in the city of Maputo.
Results: Among the 422 survey respondents, 64% identified at the time of the survey as female and 35% as male. The majority of respondents in the survey fell between the age ranges of 30–49 (67%).
In terms of HIV knowledge, 32% correctly answered the definition of viral load as being the amount of HIV in the blood, but 73% did not know what an undetectable viral load meant which is a challenge for actioning the U = U message. Most respondents (93%) agreed completely or somewhat that they would like to know more about HIV and ART. In relation to counseling, 89% and 96% of respondents, respectively, reported they received counseling from their health care providers on HIV transmission modes and ART adherence in the past 12 months. However, 32% responded that they had not received any counselling about U = U within the same timeframe.
Conclusion: Survey results highlight the importance of providing services that ensure PLHIV are effectively linked to care and mechanisms are put into place to retain them in care. Reinforcing counseling efforts on the implications of a sustained undetectable viral load remains critical to reducing new infections and decreasing AIDS-related mortality among PLHIV.
1348Classes and Correlates of HIV Risk Among Those Seeking Sexual Health Services in Miami-Dade County: A Latent Class Analysis
Ariana Johnson (presenting)1, Susanne Doblecki-Lewis1
1University of Miami Miller School of Medicine, Miami, FL, USA
Background: Understanding characteristics of HIV risk among sub-groups can allow tailoring of prevention intervention strategies. Latent class analysis (LCA) can identify and describe classes or sub-groups of individuals with different typologies of risk.
Method: We applied LCA to 2036 individuals seeking sexual health services through the University of Miami PrEP program. Variables included were history of bacterial sexually transmitted infection (STI), transactional sex, anonymous sex, sex with an HIV positive sexual partner, sex with a person who injects drugs, use of injection drugs, and condomless sex. The timeframe measures were past 12 months. Chi Square, Fisher's Exact, and t- test analyses were used to examine the correlates of class membership.
Results: Mean age was 37.2 years (SD = 12.5). Participants were predominantly male sex assigned at birth (70.4%), White (56%), Hispanic (62.7%), and foreign born (54.7%). Four distinct profiles of HIV risk were identified: (1) Low risk – probabilities 0–0.32% for each variable; (2) Low/moderate risk –anonymous sex (30.9%), sex with people who are HIV positive (5.2%), STI (9.2%); (3) Moderate risk – anonymous sex (87%), STI (80.5%), transactional sex (84.2%); (4) Higher risk –risk probabilities 45% – 100% for each variable. Class 1, low risk, highest percentage of participants who were foreign born (69.5%) and had health insurance (25.4%). Class 4, high risk, participants were largely male sex at birth (87.6%), Hispanic/Latino (72.9%), and self-reported their HIV risk as low (43.6%).
Conclusion: Our analysis found low risk perception among those in the highest HIV risk class. Additionally, a history of an STI was important to risk stratification between classes 2 and 3. Interventions focused on HIV risk perception and identifying those with a recent STI may help to focus prevention efforts.
1349Addressing Stigma and Discrimination Towards HIV Positive Mothers During the War in City of Dnipro
Tetyana Martynenko (presenting)
1
1Municipality of Dnipro City, Dnipro, Ukraine
Introduction: Despite Russia's full-scale military invasion of Ukraine, millions of refugees and IDPs, continuing shelling and damage to health care infrastructure, city of Dnipro manage to preserve effective mother to child HIV prevention programme.
Description: In 2022 city of Dnipro managed to ensure HIV testing for 97% of pregnant women, ART for 98%, of those, who received positive test result, and 98% of preventive treatment for infants. However, stigma and discrimination towards people living with HIV was a significant obstacle for internally displaced pregnant women to seek care. That is why Municipal health care department together with social protection department and the Dnipro city network of people living with HIV run the information campaign and establish the chain of continuing HIV services and support to HIV positive pregnant women, mothers, and their children.
Lesson Learned: Establishing a nondiscriminatory environment and continuum of integrated services is a key to success and it is possible even in severe circumstances related to war. Internally displaced pregnant women and mothers living with HIV require housing, basic humanitarian support, legal services, psychosocial support, medical services, and it is not the end of the list. Some of these women are using drugs, some of them have co-morbidities. Joint and well-coordinated efforts of social protection system, health care system, community support is a necessary condition to ensure continuum of care and support.
Recommendations: The example of Dnipro city demonstrates how HIV programmes can be resilient, sustainable and even more efficient in humanitarian context.
1353Patterns of HIV Risk Behavior and the Self-Perception of HIV Risk Among Adolescent Men Who Have Sex with Men and Transgender Women in Brazil: A Latent Class Analysis
Fabiane Soares (presenting)1, Laio Magno2, Beo Oliveira Leite1, Jony Arrais Pinto-Junior3, Leila Amorim1, Alexandre Grangeiro4, Dirceu Greco5, Ines Dourado1
1Universidade Federal da Bahia, Salvador, Brazil
2Universidade do Estado da Bahia, Salvador, Brazil
3Universidade Federal Fluminense, Niterói, Rio de Janeiro, Brazil
4Universidade de São Paulo, São Paulo, Brazil
5Universidade Federal de Minas Gerais, Minas Gerais, Brazil
Background: Self-perception of HIV risk is an important indicator of HIV prevention choices. We aimed to identify patterns of HIV risk behavior among adolescent men who have sex with men and transgender women (aMSM/aTGW) in Brazil.
Method: PrEP1519 was a prospective, multicenter, PrEP demonstration cohort study among aMSM/aTGW aged 15–19 in Brazil. For this cross-sectional analysis, we included 1441 adolescents enrolled from February 2019-February 2023. Latent class analysis (LCA) grouped adolescents with similar patterns of HIV-preventive behaviors and determined which group were associated with self-perception of HIV risk. The indicator variables for LCA were condom use, lubricants, use of post-exposure prophylaxis (PEP), HIV testing between partners, and non-penetrative sex.
Results: Two distinct groups came out and were characterized by preventive behaviors: (1) high HIV risk behavior (N = 1108; 76.9%), characterized by less frequent use of these methods: condom (6.6%), HIV test with a partner (6.4%), non-penetrative sex (15.1%), and PEP use (16.0%), but more frequent use of lubricant (36.9%)*; and (2) *low HIV risk behavior (N = 333; 23.1%), characterized by more frequent use of these methods: condom (40.3%), HIV test with a partner (12.7%), non-penetrative sex (27.5%), and PEP use (0.0%) but less frequent use of lubricants (28.3%). Those who perceived themselves at higher HIV risk were 7.5 times more likely to have actual high HIV risk behavior (OR: 7.5; 95% CI: 2.0–27.6), adjusted for age, gender, education, and race.
Conclusion: HIV risk perception was associated with the actual risk of adolescents and, therefore, this indicator can be used for detecting adolescents at greater risk of infection to connect them to preventive health services.
1359Ensuring Effective and Sustainable PrEP Care Through Practice-Based Adaptive Responses: A Qualitative Multiple Case Study of PrEP Service Delivery in Belgian HIV Clinics
Jef Vanhamel (presenting)1, Thijs Reyniers1, Anke Rotsaert1, Bea Vuylsteke1, Steven Callens2, Karina Kielmann1
1Institute of Tropical Medicine Antwerp, Antwerpen, Belgium
2Ghent University Hospital, Ghent, Belgium
Background: In Belgium, oral HIV pre-exposure prophylaxis (PrEP) has been publicly available since 2017, with services delivered through specialized HIV clinics. Interactions between healthcare providers, health system resources and care components in PrEP service delivery models are complex, yet poorly understood. This study aimed to increase insight into providers’ adaptive responses during PrEP care implementation under real-world conditions.
Method: We conducted a qualitative multiple case study on PrEP care implementation in eight specialized HIV clinics. We conducted 34 semi-structured interviews with a purposive sample of PrEP care providers (physicians, nurses, psychologists), supplemented by 50 h of observations of healthcare settings and 17 unstructured interviews with PrEP care providers. Field notes from observations and verbatim interview transcripts were thematically analyzed using extended Normalization Process Theory as a guiding framework.
Results: Increased workload, due to a growing PrEP client cohort, was a common driver for local PrEP care adaptations. Yet, we observed large variations in the nature and extent of implemented adaptive strategies, due to differences in system “hardware” (eg, infrastructure, organizational structure and client volume) and “software” (eg, leadership style, organizational culture and interactions between health professionals) across settings. Providers negotiated clinical care norms (eg, on PrEP eligibility, required visit frequency and addressing mental health needs of PrEP clients) in the context of evolving clinical experience, rigid reimbursement rules and individual client needs. These adaptations were strongly interrelated with emergent organizational restructuring to balance delivery quality with efficiency. Notably, shifting time-intensive routine care aspects from specialist physicians to nurses was facilitated by co-location, allowing immediate feedback during training and supervision.
Conclusion: Implementing PrEP care is a complex intervention that demands considerable adaptive capacity to ensure effective integration within the real-world constraints of healthcare systems. Adaptive response and flexibility should be incorporated in policy and guidelines governing PrEP roll-out, and in evaluation of PrEP implementation studies.
1369Evaluation of the Test and Treat Strategy for HIV Management in the eThekwini Metro of KwaZulu-Natal, South Africa Using Fast-Track Cities Quality of Care Survey Data: Are We Winning?
Somasundram Pillay (presenting)1, Chalone Savant2, Nceba Gqaleni1, Imane Sidibe3, Nombulelo Magula1
1University of KwaZulu-Natal, Durban, South Africa
2IAPAC, Durban, South Africa
3International Association of Providers of AIDS Care, Washington, DC, USA
Background: Using Fast Track Cities Quality of Care (QoC) Survey data, this study aimed to assess the implementation consistency of South Africa's Test and Treat (T&T) policy of HIV testing and immediate initiation of ART.
Method: The QoC survey employed an observational, cross-sectional design, targeting PLHIV in 30 healthcare facilities with high HIV burden in eThekwini, South Africa. Data was collected over a two- to three-month period in 2022–2023. Participants were categorized into four groups based on time since their HIV diagnosis: < 1 year, 1–4 years, 5–9 years, and 10 + years.
Results: Of 564 respondents, most were females, aged 30–49 years, aware of HIV status, and on ART for 1–4 years. Adherence to ART was high, with 83.2% reporting compliance. Patients without an early first clinical visit increased across the four time-based groups (38.9% for less than 1 year, 29.6% for 1–4 years, 38.3% for 5–9 years, and 55.6% for 10 or more years). Similarly, the percentage of patients initiating ART on day of diagnosis increased across the groups (22.27% for less than 1 year, 32.2% for 1–4 years, 46.7% for 5–9 years, and 62% for 10 or more years). Reasons for delayed initiation included patient choice, stigma, clinician decision, and CD4 count (pre-T&T era). Notably, 11.1% of participants diagnosed within the past year were not on ART, while an additional 5.6% had waited 1–3 months for ART initiation.
Conclusion: Despite improvements over the four time periods regarding first clinical visit and early ART initiation, many patients were not within T&T policy. Immediate ART initiation remains crucial for reducing HIV-related morbidity and mortality, preventing HIV transmission, and enhancing quality of life.
1377Developing Tools and Strategies to Expand the Implementation of Advanced Clinic Care Clinics at Primary Healthcare Facilities in a Resource-Limited Setting
Melanie Collins (presenting)
1
1Johannesburg Health District, Johannesburg, South Africa
Introduction: Johannesburg has the highest number of PLHIV in South Africa, estimated at 730,000; 95% access services through primary healthcare (PHC) facilities. Up to 35% of patients present with advanced HIV disease (AHD), necessitating Advanced Clinical Care (ACC) at PHC. Sub-district G is particularly impacted as patients referred to the hospital for ACC travel up to 60 km at substantial personal cost.
Description: Despite the need for ACC services, uptake has been slow. PHC facility managers were unconvinced about the potential benefit and clinicians (largely nurse-led services) required additional training and mentoring to manage AHD. Poor booking systems and uncertainty around ACC criteria resulted in inefficient use of experienced clinicians’ time, and allocation of PHC clinicians for mentoring needed to be strengthened to ensure transfer of skills for sustainability. Lastly, data collection was required to measure impact.
Two tools were developed to address the identified challenges. First, an electronic file audit tool (in Excel) to identify gaps in clinical management and monitor outcomes following implementation. Second, a clinic register included identified dates, ACC criteria and contact information for tele-mentoring. The register also serves as a portfolio of evidence for mentoring at each clinic date and collects vital data elements for monitoring.
Medical officer support for the ACC clinics will be phased out over 18 months. (See figure.)

Lesson Learned: Standardizing implementation of ACC clinics and implementing tools such as a file audit tool and register can improve the uptake of ACC clinics in PHC facilities. As a result, ACC clinics have been expanded from 1 to 5 facilities from April to June 2023.
Recommendations: Phased support and standardized tools should be used to strengthen nurse-led ACC care in low resource settings. Current ACC clinics will run until December 2023, followed by an evaluation of clinician confidence and patient outcomes.
1384A Community-Led Assessment of the HIV Treatment Cascade in Jamaica's Western Region
1, Carla Roye1, Jumoke Patrick1, Andwayne Davis1
1Jamaican Network of Seropositives, Kingston CSO, Kingston, Jamaica
Background: This study aimed to assess the HIV treatment cascade in the Western Region of Jamaica, with a focus on identifying areas for improvement and ending AIDS by 2030.
Method: The methodology involved training stakeholders in establishing a Community Treatment Observatory (CTO), data collection, analysis, and advocacy. Interviews with 158 recipients of care, 12 healthcare workers, and 17 focus group discussions were conducted between September and December 2022 in six treatment sites.
Results: The study indicated that as of October 2022, 3839 people living with HIV (PLHIV) were registered in healthcare facilities, indicating successful linkage to care. Among PLHIV who had been on antiretroviral therapy (ART) for 12 months or more, 93% had undergone viral load testing. However, 43% of them did not receive the test results within six months. Overall, 70% of PLHIV linked to care were found to be virally suppressed.
Men aged 25–34 had the highest rate of loss to follow-up, while women aged 18–24 had the lowest rate of viral load suppression. Retention in care was negatively impacted by long waiting times and challenges related to employment and medical appointments, with 29% of participants missing appointments due to work obligations.
The findings suggest that targeted interventions would address the vulnerabilities of specific age and gender groups in the treatment cascade. Efforts to reduce waiting times and improve appointment scheduling would improve adherence. Respondents reported positive experiences with confidentiality, stigma, discrimination, and service availability across facilities.
Conclusion: The pilot phase of the CTO highlighted specific areas for improvement in the Western Region's HIV treatment cascade. Addressing the needs of vulnerable populations; wait times and appointment scheduling challenges could contribute to better outcomes and progress towards achieving the 2025 targets and ending AIDS as a public health concern.
1391Advancing Public Health: A Pioneering Case Study of Decentralized Services in Almada, Portugal – Results of the Integrated Center for Social and Health Responses
Inês Correia (presenting)1, Fatima Gomes1, Bruno Pinto1, Joeli Souza1, Joelsy Pacheco1, Cátia Pires1, Mariana Vicente1, Luís Mendão1, Daniela Lages2, Paula Brito2, João Alves2, Frederico Bonito2, Nuno Silva Marques2, Alexandre Tomás3, Rita Cunha4, Ricardo Fernandes4
1Grupo de Ativistas em Tratamentos, Almada, Portugal
2Hospital Garcia de Orta, Almada, Portugal
3ACES Almada-Seixal, Almada, Portugal
4Câmara Municipal de Almada, Almada, Portugal
Introduction: The “Almada Municipality without AIDS” initiative launched the Integrated Center for Social and Health Responses (ICSHR) in September 2021 as part of the Fast Track Cities Initiative. This collaboration between the Municipality of Almada, Almada-Seixal Health Center Group, Garcia de Orta Hospital, and the Group of Activists in Treatment aims to address HIV prevention and response, and other sexually transmitted infections (STIs), viral hepatitis (VH), and tuberculosis. The partners share responsibilities and resources through a collaboration protocol.
Description: ICSHR provides screening, medical consultations, nursing services, referrals to the National Health Service (NHS), social support, peer assistance, and materials for STI prevention and safer drug consumption.
The partnership led to the implementation of Portugal's first decentralized PrEP consultation in September 2021. By July 2022, the center expanded to offer decentralized VH and STI treatment consultations.
A retrospective data analysis from September 2021 to May 2023 revealed a total of 1170 PrEP appointments, 65 VH treatment appointments, and 258 STI treatment appointments.
ICSHR conducted 3309 screening tests for HIV, Hepatitis B and C, and Syphilis. They facilitated 49 referrals to hospital appointments and provided 681 social support appointments. Material distribution included 44574 external condoms, 926 internal condoms, and 21635 packages of lubricant for STI prevention.
Lesson Learned: This collaborative approach demonstrated the effectiveness of bringing together municipalities, formal healthcare services, and community-based interventions. It removed barriers to prevention, diagnosis, and treatment adherence, resulting in tailored healthcare responses for individuals living with or at risk of these infections.
Recommendations: The success of partnerships between municipalities, the NHS, and civil society organizations with shared objectives highlights their potential for replication at regional and national levels. Collaborative approaches can enhance healthcare services and improve health outcomes for communities.
1392Achieving Virological Control and Engagement Through Tailored Peer Mentoring: Successful Conclusions of a Collaborative Project Supported by the Fast-Track Cities (FTC) Initiative
Harry Coleman (presenting)1, Jaime Sylla (presenting)2, Kajann Kantha3, Joel Robinson2, Elizabeth Dale3, Elizabeth Hamlyn3, Hannah Alexander1, Kate Childs3, Goli Haidari1
1Guy's and St. Thomas’ NHS Trust, London, England, United Kingdom
2METRO Charity, London, England, United Kingdom
3King's College Hospital, London, England, United Kingdom
Introduction: Incomplete adherence to anti-retroviral therapy (ART) and challenges in engaging with healthcare services pose significant challenges to achieving optimal health outcomes for people living with HIV (PLWH). We addressed barriers to engagement through a tailored peer mentor project. Individuals with a viral load (VL) of >200 copies/ml were eligible for referral. They included some of the most complex patients within the services.
We aimed for 60% of patients who engaged with the peer mentor to achieve a VL <200 copies/ml within 12 months.
We present outcomes of a three-year FTC funded peer mentor project, the lessons learnt and the future plans.
Description: The mentor was embedded in two London HIV clinics, supported by Metro charity and FTC. The mentor provided sessions to referred clients covering motivation, HIV knowledge, beliefs and barriers to adherence – promoting patient agency.
Lesson Learned: 116 patients were referred. 46/116 (40%) engaged with the mentor. The median age of those engaged was 39 (range 20–61). 29/46 (63%) were male. 23/46 (50%) were GBMSM. The Median CD4 count at referral was 187 cells/ml (range 8–1147 cells/ml) and median VL 81,500 copies/ml. 45/46 (98%) patients engaged with the peer mentor achieved a VL <200 copies/ml at some point. (See figure.)
Recommendations: The project's success stems from integrating the mentor into the clinical team, where they actively participated in ward rounds and outpatient clinics. The project fostered extensive information sharing, facilitating the development of personalised care plans. Improvements include: recruiting further mentors, providing supervision for the mentor, and establishing a closure process for the mentor-mentee relationship.
We recommend embedding peer mentors in all clinics to enable PLWH to achieve an undetectable VL. The project plans to expand with more mentors to ensure diversity and representation for patients, providing enhanced support for patients.
1402Reduced Pre-Exposure Prophylaxis (PrEP) Interruption with a Tech-Based Continuous Quality Improvement Intervention for Men Having Sex with Men (MSM) in Fast-Track Cities of Austin and Dallas
Harsh Agarwal (presenting)1, Mark Erwin2, Sanford Scott Lyles2
1UNC Chapel Hill, Chapel Hill, NC, USA
2Centre for Health Empowerment, Austin, TX, USA
Introduction: Oral PrEP is an effective HIV prevention strategy for vulnerable groups like MSM. However, in the USA, even for those MSM who are keen to use it, PrEP access and retention is obstructed by insurance and processes level challenges. We adopted a continuous quality improvement (CQI) framework to identify gaps and used tech-innovative strategies to reduce drops.
Description: Our automated technology-workflows examined retention trends, identifying clients falling out of care or experiencing delays. PrEP navigators reached out to such clients for structured interviews.
We found that clients falling out of care had common challenges: rejection of PrEP insurance claims without prior authorizations, (lack of) timeliness of shipping-authorizations and uptake of habit formation. We hypothesized that if we address bureaucratic challenges and customized client outreach, especially earlier in the retention lifecycle, drop rates would diminish.
Lesson Learned: We developed 340 bWell software that created automatic alerts if prescriptions were not filled within a certain period, and we coordinated between the clients and stakeholders to troubleshoot problems. To examine the effect of the intervention, we evaluated data 6 months pre (N = 119, May-Oct in 2022) and post (N = 131, Nov 2022 to June 2023) intervention.
We compared pre and post data descriptively and ran a two-sample t-test. In both pre and post intervention samples, most participants were from Dallas and Travis country. The intervention reduced the drop by 23%, reducing drops from 31% (N = 37) to 8% (N = 12) after intervention (p < .001). At the same time, it was worth noting that while there were more white MSM than black MSM in post-intervention group, proportion of MSM dropping out of care was higher among black man in both pre (46%) and post (41%) groups as compared to white MSM.
Recommendations: Technology driven CQI approach can facilitate identification of systemic gaps and facilitate problem resolution in real time, helping improve critical outcomes like PrEP retention. Such interventions can be leveraged in similar settings with low PrEP retention.
1412Improvement of HCV Screening and Linkage to Care Through Implementation Science in Madeira, Portugal
Elisa Xavier (presenting)1, Vítor Magno Pereira (presenting)1, Luís Jasmins1, Ana Paula Reis1, Nancy Faria1, Nuno Ladeira2, Madalena Pestana2, Bruno Freitas1, Nuno Canhoto1, Diogo Medina3, Alba Carrodeguas3
1Serviço de Saúde da Região Autónoma da Madeira, Madeira, Portugal
2Hospital Central do Funchal, Funchal, Portugal
3Gilead Sciences, Madrid, Spain
Background: Hepatitis C (HCV) is a curable chronic viral infection, however, there is still a high proportion of undiagnosed cases. In 2016, WHO announced the goal of HCV elimination until 2030. SESARAM manages 47 primary care centers, 3 hospitals, and 1 emergency department (ED) that serve 254,000 residents in the Portuguese Autonomous Region of Madeira. All facilities share the same laboratory.
In line with WHO, we implemented systematic, opportunistic HCV screening in 2020. We optimized existing infrastructure and staff, assisted by electronic health record algorithms to identify patient eligibility and automate the laboratory requests orders with oral opt-out consent. We used reflex testing for the first time in Portugal, wherein positive HCV antibody tests trigger HCV core antigen confirmation on the same specimen without physician or patient initiation. Eligible patients included those aged between 18–70, without known HCV diagnosis or testing in the previous year, who required blood work for any reason. We integrated the HCV screening from January 2020 in wards, followed by emergency department in July 2020 and primary care in January 2021.
We screened 35376 patients for HCV between January 2022 to May 2023. We found 0.5% antibody prevalence and 0.14% viremia diagnosing 52 new cases of HCV. An analysis of the quarterly moving averages of antibody and RNA prevalence in the population reveals a decreasing trend over time, crossing zero between 2024 and 2026. Linkage to care was complete at 94%.
Opportunistic screening grounded in Implementation Science and Information Technology is feasible and effective at improving timely HCV diagnosis gaps and achieving elimination.
1414Implication of Self-Stigma on PLHIV in Jamaica
Jumoke Patrick (presenting)1, Jaemar Johnson1, Andwayne Davis1, Dane Lewis1
1Jamaica Network of Seropositives (JN+), Kingston, Jamaica
Background: This study with 267 PLHIV examined self-stigma among people living with HIV (PLHIV) in Jamaica, focusing on its prevalence, associated factors, and consequences.
Method: A mixed-methods approach was employed, utilizing questionnaires and focus group discussions. The data were analyzed using cross-tabulations and chi-square analysis.
Results: The study revealed that 61% experienced guilt and 51% felt shame due to their HIV status. The experience of guilt and shame was significantly associated with age and duration of HIV diagnosis. Individuals aged 18–44 reported higher levels of guilt, while those aged 45–54 reported lower levels. Moreover, 78% of respondents reported negative impacts on their lives, primarily affecting self-confidence. Males exhibited greater negative impacts on self-confidence, while younger age and shorter duration of HIV diagnosis were linked to lower self-respect.
Sadness (39%) and low self-esteem (20.3%) were the most common emotions associated with guilt, with women reporting more sadness and men reporting more low self-esteem. Participants with shorter durations of HIV diagnosis reported higher levels of sadness and low self-esteem. Regarding disclosure, 70% disclosed their status to healthcare professionals, and 68% to family members.
Approximately 26% had their status disclosed without their consent, primarily by family and friends. However, guilt and shame were found to have little impact on medication collection and adherence, with the majority maintaining consistent adherence.
Regarding sexual relationships (66%) reported guilt and shame did not affect their negotiation of condom use within relationships.
52% believed they were solely responsible for practising safe sex due to their HIV status.
Conclusion: The study demonstrates that self-stigma affects PLHIV in various aspects of their lives, particularly within the first 10 years of diagnosis. Recommendations to address self-stigma should include expanding peer support groups, mental health interventions, empowering women socioeconomically, addressing GBV, and promoting mechanisms for reporting and addressing discrimination complaints.
1418Sexual Minority Stress Processes Are Associated with Lower PrEP Engagement Among Men Who Use Stimulants
Renessa Williams (presenting)1, Leah Davis-Ewart (presenting)1, Ariana Johnson (presenting)1, Nicole O'Dell1, Sidney Carr1, Samantha Dilworth2, Christian Grov3, Adam Carrico1
1University of Miami, Coral Gables, FL, USA
2University of California San Francisco, San Francisco, CA, USA
3CUNY School of Public Health, New York, NY, USA
Background: Sexual minority men (SMM), experience significant stress because of stigma and discrimination. This cross-sectional study sought to (1) identify the profiles of sexual minority stress specific to SMM who use stimulants (2) examine associations with measures relevant to engagement in the pre-exposure prophylaxis (PrEP) care continuum.
Method: A national US sample of 105 cis-gender SMM who currently were not taking PrEP were included in the analysis. We utilized a latent profile analysis to characterize underlying patterns of sexual minority stress to identify ‘profiles’ or sub-groups of participants. Participants completed self-report measures of sexual minority stress including internalized homophobia, concealment of sexuality, and prejudice events. ANOVA and Chi Square analysis were used to examine the correlates of profile membership.
Results: Participants were on average 39.4 years old (SD = 9.13) self-identified as gay (75%), predominantly White (70%) and non-Hispanic (79%). Four distinct profiles of sexual minority stress were identified: (1) Assimilation – low internalized stigma with moderate concealment and prejudice events; (2) Marginalization – high internalized stigma and concealment with low prejudice events; (3) Integration – low internalized stigma and low concealment with high prejudice events; and (4) Separation – moderate internalized stigma and concealment with high prejudice events. The Assimilation profile had significantly higher proportions of men without health insurance (p = 0.03), who were mostly White (83%), and the lowest average intentions to use PrEP (8.54; SD = 2.30). The Separation profile, characterized by the highest probability of experiencing a prejudice event compared to the other profiles, had the most difficulty with PrEP self-efficacy (p < 0.01; mean efficacy scores 26.6 (SD = 3.81)).
Conclusion: Findings underscore the importance of understanding the full spectrum of sexual minority stress to optimize PrEP engagement in SMM who use stimulants.
1424Constructing Social and Healthcare Responses Centered on the Needs of People Who Use Drugs in the Municipality of Amadora, Portugal
Joana Pires (presenting)1, Joana Silva1, Andreia Leite1, Ana Rita Goes1
1NOVA National School of Public Health, Amadora, Lisbon, Portugal
Background: Drug use in public spaces has been identified as a major concern in Amadora (Lisbon, Portugal), among the people in homeless situation. Local knowledge of the territory is required for the design of any intervention to address this public health problem. Participatory co-design methods bring diverse understandings of a problem, allowing the construction of holistic responses with all key actors, such as the field teams. Selecting the main needs and responses for the PWUD, it becomes fundamental to think about the construction and development of responses at a local level, taking into account practices and patterns of consumers and consumption.
Method: The goal was to identify the needs and perceptions of workers from field teams, about what and how the responses to the PWUD should be constructed in Amadora. The research team conducted three in-depth workshops with the field teams who work directly with PWUD in the city of Amadora. Qualitative data were collected during the workshops with the team workers. The approach to analysis was informed by iterative categorization and reflexive thematic analysis methods.
Results: The health needs identified, and corresponding responses are centered on safe consumption spaces, facilitated access to primary and mental healthcare, and access to low-threshold opiate agonist treatment. At the social level, sheltering, employment, and social insertion are urgently needed as structuring responses. The results indicate the importance of designing responses that are centered on the needs and circumstances of PWUD, thinking in an integrative and intersectional way and providing services using a “one-stop-shop” approach. The need for inclusive and dignifying spaces and practices was also emphasized.
Conclusion: The increasing access and availability to continuum responses, considering holistic, intersectional, individual needs and preferences, are crucial. A person-centered and context-specific approaches are indispensable for defining services.
1426Improving Viral Load Suppression in Pediatric and Adolescent Patients Using National Health Laboratory Service Reports in Johannesburg, South Africa
Melanie Collins (presenting)1, Kate Rees2
1Johannesburg Health District, Johannesburg, South Africa
2Anova Health Institute, Johannesburg, South Africa
Background: Viral load (VL) suppression in children and adolescents living with HIV remains a challenge in South Africa. The management of complex clinical and psychosocial factors that lead to high viral loads is confounded by a lack of efficient systems to timeously identify patients with a high VL, limited capacity to address the identified challenges, and clinicians’ lack of confidence managing children.
Method: The National Health Laboratory Service (NHLS) generates weekly reports of all patients with an abnormal VL result in the preceding week. These reports were used to identify patients with a VL ≥ 1000 copies/ml for urgent clinical and psychosocial intervention. Clinical interventions included clinical assessment, health education, regimen simplification and optimization, managing opportunistic infections and potential drug-drug interactions, switching to second line regimens, as well as genotyping, when required. Psychosocial services included adherence counselling, disclosure support, referral to community-based organizations (CBOs) and recruitment to adherence clubs.
Results: At the time of data review, 272 patients with a previous VL ≥1000 copies/ml had been managed using this process and had a follow up VL result. Of these, 196 (72%) had a follow up VL <1000 copies/ml, including 107 (39%) with a VL <50 copies/ml. (See figure.)

Conclusion: Close to three quarters of children in this high-risk group re-suppressed after intervention. This process can be used to timeously identify paediatric and adolescent patients with a high VL and provide comprehensive clinical and psychosocial services. Scaling is feasible and should be considered in high burden areas to improve VL suppression.
1429Evaluation Voluntary Assisted Partner Notification Modalities for Active HIV Case Finding in Kigali, Rwanda
Semakula Muhammed (presenting)
1
1Rwanda MoH/RBC, Kigali, Rwanda
Background: Voluntary assisted partner notification (VAPN) services that use contract, provider, or dual referral modalities may efficiently identify individuals with undiagnosed HIV infection. We aimed to assess the relative effectiveness of VAPN modalities in identifying undiagnosed HIV infections. VAPN was piloted in 23 health facilities in Kigali, Rwanda.
Method: We identified individuals with a new HIV diagnosis before antiretroviral therapy initiation or individuals on antiretroviral therapy (index cases), who reported having had sexual partners with unknown HIV status, to assess the association between referral modalities and the odds of identifying HIV-positive partners using a Bayesian hierarchical logistic regression model. We adjusted our model for important factors identified through a Bayesian variable selection.
Results: Between October 2018 and December 2019, 6336 index cases were recruited, leading to the testing of 7690 partners. The HIV positivity rate was 7.1% (546/7690). We found no association between the different referral modalities and the odds of identifying HIV-positive partners. Notified partners of male individuals (adjusted odds ratio 1.84; 95% credible interval: 1.50 to 2.28) and index cases with a new HIV diagnosis (adjusted odds ratio 1.82; 95% credible interval: 1.45 to 2.30) were more likely to be infected with HIV.
Conclusion: All 3 VAPN modalities were comparable in identifying partners with HIV. Male individuals and newly diagnosed index cases were more likely to have partners with HIV. HIV-positive yield from index testing was higher than the national average and should be scaled up to reach the first UNAIDS-95 target by 2030.
1432Effects of Using Key Population (KP) Peer Educators at Health Facilities to Identify, Attract, and Retain Other KP into HIV Care and Treatment (C&T) Continuum in Maputo City
Vanda Zitha (presenting)1, Sheila Lobo de Castro (presenting)2, Alice Abreu3, Belia Xirinda4, Laison Daniel5
1Serviços de Saúde da Cidade de Maputo, Maputo, Mozambique
2Maputo City Health Service, Maputo City, Mozambique
3Maputo City Council, Maputo, Mozambique
4Maputo City Municipality, Maputo, Mozambique
5CCS, Maputo, Mozambique
Introduction: Maputo City has a 16,5% HIV prevalence among people aged 15 years and older. More than a quarter (28.7%) of new infections in this age group are attributed to key populations (KP), including female sex workers (FSW), men who have sex with men (MSM), incarcerated or recently released individuals (PIP), and people who use injectable drugs (PWID). KP face significant barriers to accessing health services due to stigma and discrimination. On the other hand, a significant proportion of KP living with HIV (88%) is identified in the community, which limits their follow-up and retention in C&T at the health facilities (HF), given the providers’ difficulty to identify and reach them.
Description: In 2019, Maputo engaged KP in care provision by:
Identifying and hiring KP individuals to work as peer educators;
Training them (KP) with healthcare providers in strategies to identifying, welcoming, and attracting KP to seek care at HFs;
Allocating KP peer educators in higher volume HF of Maputo;
Lesson Learned:
Using KP peer educators in the HFs, has increased the number of KP living with HIV identified at the HF from 12% to 79%;
KP tested, aware of their HIV status and integrated into HIV C&T have increased by over 30 times in HFs, in less than 4 years (Figure 1);
The Ministry of Health and other implementing partners (IP) have accepted well the initiative and are supportive;
Health providers are still resistance to the initiative and need to show empathy and Camaraderie for KP peer educators.
Recommendations:
Health authorities need to raise awareness of health providers to the importance of being inclusive and the need to integrate other competencies through teamwork to improve their health results;
There is a need to improve the working environment of the peers, eliminating all forms of stigma and discrimination started by the health providers. (See figure.)

1437Missed Opportunities for PrEP Uptake: Insights from a London E-Service
Vanessa Apea (presenting)1, Sara Day2, Efejiro Ashano1
1Preventx, Sheffield, England, United Kingdom
2Chelsea and Westminster Hospital NHS Foundation Trust, London, England, United Kingdom
Background: There is clear inequity in PrEP awareness, perceived candidacy and uptake, with predominant users in the UK being White men who have sex with men (MSM). Racially minoritized MSM and Black women (BW) are two key groups in which to maximize uptake to achieve 2030 targets. Users of an STI screening e-service, collaboratively funded by 30/33 London local authorities, are triaged to assess current PrEP use, HIV risk and PrEP eligibility. If deemed eligible they are signposted to PrEP advice. We sought to quantify and characterize PrEP users (PU) and non-PrEP users (NPU).
Method: We conducted a retrospective analysis of a London e-service, between April 2022 and April 2023, to explore the demographics of PU and NPU, focusing on MSM and BW, stratifying by age, ethnicity and HIV, Neisseria Gonorrhea (GC) and Chlamydia Trachomatis (CT) positivity.
Results: 100786 users who accessed the e-service for HIV testing were MSM; 47% (n = 47568) were PU. Of the 53218 NPU, 55% were signposted to PrEP advice. HIV positivity among NPU was slightly higher than PU, 0.32% versus 0.23%; the highest being among those of Latin American and other Black background. GC and CT positivity in PU were 8.3% and 7.49%, respectively, as compared to 4.9% and 4.39% in NPU. 64005 users were BW; only 38 were PU. Of the 63967 NPU, 30% were signposted to PrEP. HIV positivity among NPU was 0.29%; the highest among those of Black African background and those aged 25–34. GC and CT positivity in NPU were 0.5% and 3.51%, respectively.
Conclusion: The data offers insight into the potential magnitude and demographics of missed opportunities within HIV prevention. Future initiatives should further explore how to maximize PrEP uptake via digital PrEP pathways.
1453FINISHING HIV: An EHE Model for Latinos Integrating One-Stop-Shop PrEP Services, a Social Network Support Program, and a National Pharmacy Chain
Mariano Kanamori (presenting)
1
1University of Miami, Miami, FL, USA
Introduction: PrEP services are not being sufficiently accessed by Latino MSM (LMSM) in Miami, the epicenter of the HIV epidemic in the US.
Description: FINISHING HIV is a hybrid 1 implementation-effectiveness randomized controlled trial of an implementation strategy bundle of a social network support component and a one-stop-shop PrEP component to improve PrEP initiation of LMSM. Our implementation partners are Latinos Salud (a local HIV agency for LMSM) and CVS Health (a national pharmacy chain). Penetration at pharmacies and social events leads to random assignment to either a social network support component + one-stop-shop PrEP component (N = 24 seeds and 288 LMSM friends) or to standard health promotion (N = 312). Participants are assessed at baseline and receive follow ups and dried blood spots collection at 6 and 12 months to quantify tenofovir diphosphate concentrations. For implementation (Aim 1), we use RE-AIM framework to evaluate Reach (the extent to which high risk persons initiate participation in the program), and Implementation (the extent to which implementation strategies are delivered as designed). We use Consolidated Framework for Implementation Science Research to examine contextual factors associated with Reach and Implementation. We are comparing effectiveness (Aim 2) in PrEP initiation (primary outcome), as well as PrEP knowledge, retention, and adherence (secondary outcomes).
Lesson Learned: Our logic model makes explicit our determinants, strategies, mechanisms, and outcome measures (Figure 1). Table 1 includes CFIR constructs/sub-constructs with greatest perceived strengths based on 20 interviews with Latinos Salud staff. Photovoice with 24 participants showed that LMSM would start PrEP not just to protect themselves, but to also protect their community. Religion is a guiding force for initiating PrEP.

Recommendations: Our use of social network support, one-stop-shop PrEP, and community and national pharmacy chain partners is a promising model that can be replicated in other EHE priority areas.
1455Online HIV Self-Test Giveaway Service in Kazakhstan: Key Findings and Implications
Zhanar Tatkeyeva (presenting)1, Mira Sauranbayeva1, Viktor Ivakin1, Anna Deryabina1
1ICAP at Columbia University, Almaty, Kazakhstan
Background: In February 2022, ICAP launched an online HIV self-test (HIVST) giveaway service in Almaty, Kazakhstan
Method: Information about the HIVST service is disseminated through social media targeting key populations (KP). HIVSTs are ordered using an ICAP-developed platform. Clients can collect their HIVST at 24/7 automated parcel lockers, pharmacies, AIDS Center, community-based organizations, or by courier delivery. After order placement, clients are offered a risk assessment. Information on pre-exposure prophylaxis (PrEP) and other HIV prevention is displayed to clients reporting high-risk behaviors. HIVST kits also include information on HIV prevention, treatment, and partner testing. Clients report results to the AIDS Center coordinator, who supports those reporting reactive tests to complete confirmatory testing and treatment initiation
Results: By April 2023, 1819 HIVSTs were delivered to 1234 clients who reported themselves as men, 568 as women, 8 as nonbinary, 8 as transgender, and 1 did not report gender. The median age was 25 years (IQR 22-31). 47% (885) reported their results, including 21 reactive results. Twelve people were confirmed as HIV-positive and initiated on ART. Most clients collected their HIVST at parcel lockers (56%) and pharmacies (33%). Of 1799 people who reported their HIV testing history, 603 (33%) were first-time testers, 455 (25%) tested more than 12 months ago. 54% (985) completed the risk assessment. Of those, 228 (23%) reported themselves as men who have sex with men (MSM), 19 (2%) as clients of sex workers (SWs), 10 (1%) as sex partners of people who use drugs, 9 (1%) as sex partners of people living with HIV, 8 (1%) as SWs, 8 (1%) as transgender individuals, 702 (71%) did not consider themselves as KP
Conclusion: An online HIVST service is effective in reaching people who otherwise might not get tested, especially younger people and MSM
1456Social Network Strategy as an Effective Approach to Engage People Who Inject Drugs in HIV Testing
Zhanar Tatkeyeva (presenting)1, Mira Sauranbayeva1, Anna Deryabina1
1ICAP at Columbia University, Almaty, Kazakhstan
Background: Almaty has one of the highest numbers of people who inject drugs (PWID) living with HIV in Kazakhstan. Since 2019, as part of Almaty Model for Epidemic Control, ICAP jointly with NGO Revansh implements community-based HIV testing among PWID using traditional outreach. In 2021, to improve HIV case-finding, ICAP supported the launch of a social network-based recruitment strategy (SNS).
Method: As part of SNS, PWID were provided with coupons and incentivized to invite other PWID to come to Revansh for testing. To assess effectiveness of HIV testing efforts, we compared HIV testing coverage, HIV case finding, and participants’ characteristics identified through SNS and the outreach-based testing among PWID. Routinely collected aggregate program data collected by an NGO “Revansh” from September 1, 2021, to May 31, 2023, were used for analysis.
Results: A total of 3465 people were tested for HIV, including 1534 (1188 men and 346 women) who were referred for testing through SNS and 1931 (1237 men and 694 women) through traditional outreach. The median age of PWID tested was 37 years (IQR: 37–38) for SNS and 39 years (IQR: 37–40) for outreach. SNS resulted in higher positivity yields compared to traditional outreach (3.4% vs 1.7%, the p = 0.0009). SNS also accounted for a higher proportion of self-reported first-time testers (52%) versus traditional outreach (16%, p-value < 0.00001).
Conclusion: The results of the study demonstrate that both testing approaches are effective at engaging PWID in HIV testing with SNS resulting in higher HIV testing yield and larger proportions of first-time testers.
1458Making PrEP Equity Local: Examining PrEP Equity Metrics in U.S. Cities
Patrick Sullivan (presenting)1, Kamaria Dyan Brisco1, Gordon Le1, Stephanie DuBose1, Sindhu Ravishankar2, Daniel Murdock1, Vatsana Chanthala3, Lorene Maddox4, Colby Cohen4, José M. Zuniga2
1Emory University, Atlanta, GA, USA
2IAPAC, Washington, DC, USA
3Office of Health Policy and AIDS Funding, New Orleans, LA, USA
4Florida Department of Health Bureau of Communicable Diseases, Tallahassee, FL, USA
Background: It is critical to monitor not only the number of US PrEP users, but also whether PrEP use is equitable along critical dimensions (eg, age, sex). The PrEP-to-Need Ratio (PnR) is a PrEP equity metric that has been evaluated in US regions, states, and counties, but has not been promoted for monitoring PrEP uptake in US cities.
Method: Using county data as a surrogate for city data for two select cities for which county boundaries approximate city boundaries, we compared PnR by sex and age in city/state pairs: Miami (approximated by data from Dade County) and Florida, and New Orleans (approximated by data from Orleans Parish) and Louisiana.
Results: Overall, PnRs were higher in the two cities than in their host states for women and men, and for all age groups with the exception of men and those 35–44 and >55 years of age in Miami/Florida. (See figure.)

Conclusion: Even considering that Miami and New Orleans have more people with PrEP indications than do other parts of their states, these cities generally outperform their states in terms of equitable PrEP access. The differences might be attributable to social determinants, such as a higher density of PrEP providers and corresponding lower commute times to PrEP care in cities. PrEP equity metrics should be promoted as critical components of prevention effort evaluation. Additionally, further evaluation should be conducted to identify why PrEP equity is higher in these cities than in their host states and what city strategies might be exportable to state programs.