
Abstract
One in three people with HIV (PWH) has hypertension. However, most hypertensive PWH in sub-Saharan Africa are unaware of their hypertension diagnosis and are not on treatment. To better understand barriers to hypertension care faced by PWH, we interviewed 15 medical providers who care for patients with HIV and hypertension in northern Tanzania. The data revealed barriers at the patient, provider, and system level and included: stress, depression, and HIV-related stigma; lack of hypertension knowledge; insufficient hypertension training; inefficient prescribing practices; challenges with counselling; capacity limitations in hypertension care; high costs of care; and lack of routine hypertension screening and follow-up. Opportunities for improvement focused on prioritizing resources and funding towards hypertension care. System-related challenges were the underlying cause of barriers at individual levels. Strategies that focus on strengthening capacity and utilize existing HIV platforms to promote hypertension care delivery are urgently needed to improve cardiovascular outcomes among PWH.
Background
Approximately 1 in 3 people with HIV (PWH) in sub-Saharan Africa (SSA) has hypertension, 1 a leading modifiable risk factor for cardiovascular disease and death.2-4 PWH have a heightened risk of cardiovascular disease including myocardial infarction, stroke, and sudden cardiac death compared to the general population.5,6 As PWH continue to age, the burden of hypertension and its associated cardiovascular related morbidity and mortality will rise, portending an impending public health crisis if not promptly addressed. 7
Despite this growing epidemic, most hypertensive PWH in SSA are unaware of their hypertension diagnosis and are not receiving hypertension treatment. 8 Clinical guidelines advise that antihypertensive treatment, including patient education, lifestyle modification, and pharmacologic therapy, should be initiated for all individuals with an elevated blood pressure. 9 However, a recent study in northern Tanzania examining a cohort of hypertensive patients enrolled in HIV care revealed that more than half of all participants had never had a previous blood pressure measurement, two-thirds were unaware of their diagnosis, 90% were not on antihypertensive treatment, and none had controlled blood pressure suggesting a discordance between real-world practice and treatment guidelines. 10
Challenges across the hypertension continuum of care among PWH in SSA are likely multifactorial.11-13 A qualitative study examining perspectives of hypertension care among hypertensive patients receiving HIV treatment in northern Tanzania identified poor patient knowledge as a predominant barrier to hypertension care. This same study also recognized that limitations in medical provider communication and counselling and lack of integrated HIV and hypertension care likely contributed to suboptimal clinical outcomes. 14 However, few studies have explored provider perspectives and experiences of hypertension care among PWH.15-18
In order to improve clinical outcomes among PWH, it is imperative to have a better understanding of the challenges faced across the hypertension care continuum. To better understand the barriers to hypertension care faced by PWH, we conducted a qualitative study exploring the perspectives and experiences of medical providers caring for patients with both HIV and hypertension.
Methods
This qualitative study involved in-depth interviews with 15 healthcare workers who provided care for patients with HIV and hypertension. To ensure rigor and reproducibility, the presentation of methods and results follows the Consolidated Criteria for Reporting Qualitative Research guidelines. 19
Setting
This study was conducted in the Moshi urban district of northern Tanzania, at 2 government-funded primary health centers, and 1 regional referral hospital. In northern Tanzania, the estimated prevalence of hypertension among patients enrolled in HIV care is 20%. 10 In all 3 study sites hypertension care is managed separately from HIV care (Table 1). In the 2 primary health centers, HIV care is delivered in the HIV Care and Treatment Centre, which is an HIV clinic, whereas hypertension care is either provided in the Outpatient Department (OPD), which is an urgent care clinic, or in the Hypertension Clinic. In the regional referral hospital, HIV care is provided in the Infectious Diseases Clinic, which is an HIV clinic, and hypertension care is delivered in the OPD. Standard of care for hypertension treatment follows the national standard treatment guidelines, and hypertension treatment protocols are not differentiated between PWH and the general population. 9
Characteristics of HIV and Hypertension Service Delivery Across Study Sites, Kilimanjaro Region, 2018 to 2019.

Abbreviations: OPD: Outpatient Department; CO: clinical officer; MD: medical doctor.
Study Population
Semi-structured interviews were conducted with 15 medical providers who provide care for patients with HIV and hypertension. Participants were eligible if they were actively practicing nurses, clinical officers (clinicians equivalent to a mid-level provider such as physician assistants in the United States), or physicians (medical doctors who completed a medical degree) who were working in the HIV Clinic, OPD or Hypertension Clinic at 1 of the 3 study sites. A total of 5 nurses, 5 clinical officers, and 5 physicians were recruited across the 3 sites. All physicians were trained as general internists. Participants were purposively selected to include a broad range of ages, number of years in practice, and training and experience in hypertension management.
Procedures
Eligible participants were purposively selected by the research staff between September 1, 2018 and August 28, 2019. The in-depth interview guide was developed by an interdisciplinary team of social scientists, physicians and nurses, and reviewed by Tanzanian members of the research team to ensure appropriate language, terminology, and cultural saliency. The guide included open ended questions on key domains of interest (hypertension training, hypertension management and care experiences, HIV and hypertension perspectives, challenges to hypertension care, and improvements in care). Each question was followed by a list of possible follow-up probes to help guide the conversation. All interviews were conducted in a private room at the study site by either a physician researcher from the United States or a Tanzanian research assistant with experience in qualitative methodology. Both members of the research team were not involved in clinical care at any of the study sites. Interviews were conducted either in English or in Swahili, depending on the participant's preference. Interviews lasted between 20 and 60 min (mean of 35 min), were audio recorded with participant consent, and were transcribed in English. All participants received 5000 Tanzanian shillings (∼$2.20 US dollars) as reimbursement for their time.
Data Analysis
Data analysis was conducted using applied thematic analysis. 20 Transcripts were reviewed and after multiple readings, detailed memos were written for each transcript by a physician researcher from the United States to summarize and organize the content that emerged across the domains of interest. 21 Memos were constructed following a template of a priori domains, informed by the interview guide, to extract and synthesize core meaning from the text, and were reviewed by a Tanzanian research assistant to confirm completeness and rigor. Each transcript (7-16 pages of text) was condensed to a 4-12 page document memo, and through the memo writing process, emerging themes were identified which informed development of the codebook. The codebook consisted of 13 themes across 4 domains: barriers at the patient level, barriers at the provider level, barriers at the system level, and opportunities for improvement. Each document memo was then independently coded using NVivo 12 (QSR International, Melbourne, Australia) by a physician researcher from the United States to label the memo content to respective themes. A second physician researcher from the United States double-coded 20% of all memos and the 2 coders met to discuss coding and modify the codebook until consensus was reached. Coding queries were used to review text coded to themes and synthesize data. Representative quotes were reviewed throughout analysis and were selected to best capture the data.
Ethical Approval and Informed Consent
Study procedures were approved by Duke Health Institutional Review Board (Pro00091126), Kilimanjaro Christian Medical University College Research Committee (No. 2265), and the Tanzania National Institute for Medical Research Ethics Coordinating Committee (NIMR/HQ/R.8a/Vol. IX/2779). All participants provided written informed consent prior to enrolment.
Results
Characteristics
The characteristics of study participants are summarized in Table 2. Participants ranged in age from 29 to 60 years, with a median age of 42 (IQR 35-48) years. The sample included 8 women and 7 men. The number of years in clinical practice ranged from 2 to 35 years, with a median of 10 (IQR 7-20) years of clinical practice. A total of 12 participants reported receiving formal hypertension training during their schooling, and 5 participants reported receiving continuing medical education about hypertension at their place of work.
Characteristics of In-Depth Interview Participants, Kilimanjaro Region, 2018 to 2019 (n = 15).

Abbreviations: OPD: Outpatient Department.
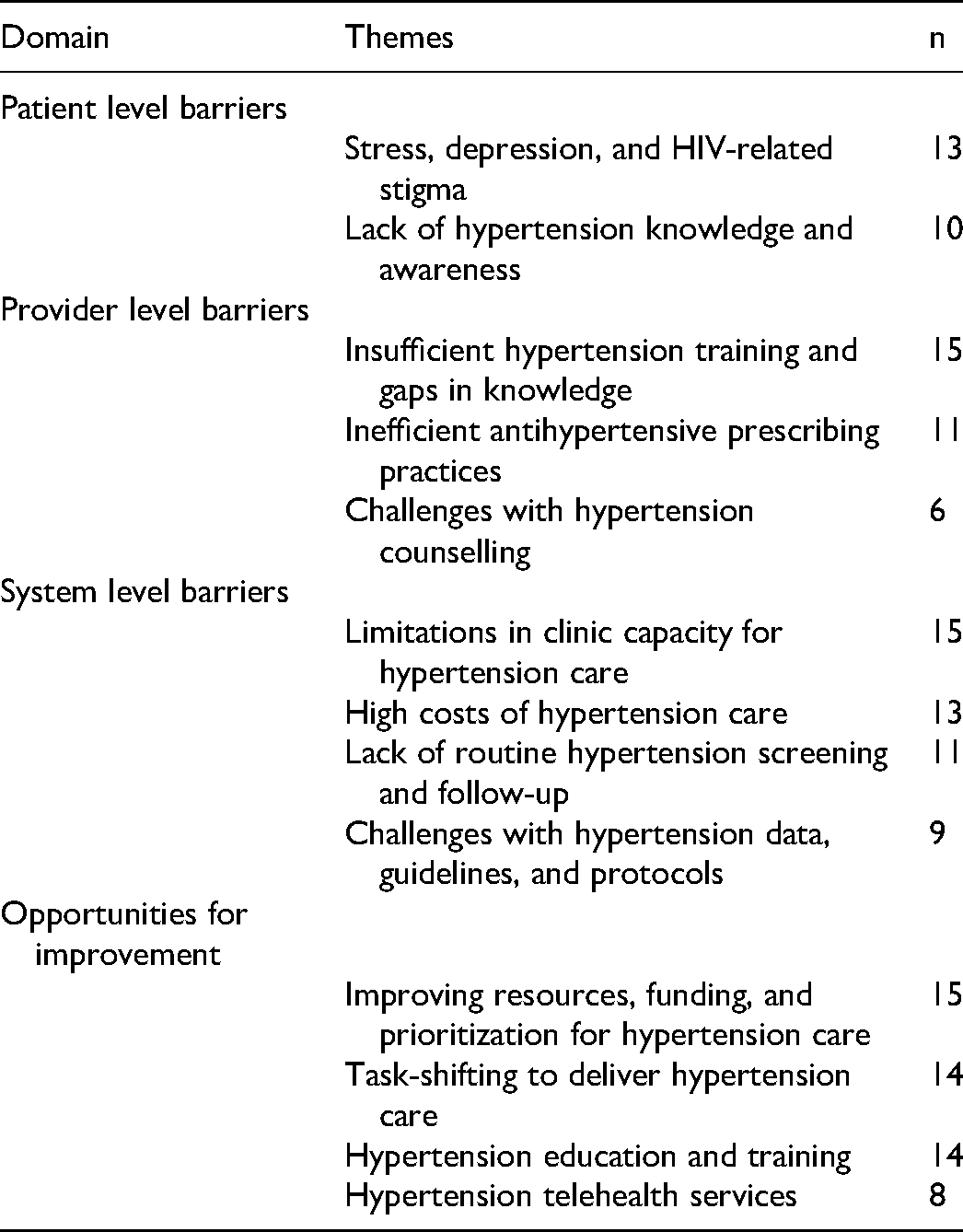
The data revealed a range of themes across the domains of barriers at the patient, provider, and system level and opportunities for improvement (Table 3).
Dominant Themes among Providers Regarding Hypertension Care Barriers and Opportunities for Improvement for People with HIV (n = 15).
Barriers at the Patient Level
Stress, Depression, and HIV-Related Stigma
Most providers described patients feeling overwhelmed from having multiple medical conditions, HIV and hypertension. Providers also acknowledged that antihypertensive drug nonadherence was in part due to patients feeling “burdened” from taking multiple medications. They believed that patients were “stressed” from their health issues and from challenging life circumstances, such as financial distress and conflicts within their family. Most providers raised concern that this stress could elevate blood pressure.
Some have already given up. They say, “Okay, I already have HIV and now I’m starting to have high blood pressure. I’d rather die”. (Nurse, Female, 40 years, HIV Clinic)
Some providers also suspected that patients with HIV frequently experienced depression and “hopelessness,” and that social stigma surrounding HIV remained a common occurrence.
The first challenge is that we provide care to people who have already lost hope. They are living a hopeless life already…Because remember that this person (with HIV) is living with death at the palm of their hand. So, the counselling that I provide should focus more on reviving the soul that has lost hope and is saddened. (Nurse, Female, 60 years, HIV Clinic)
Mental health issues and HIV-related stigma were viewed as common barriers that led to avoidance of the health care system.
They don't like to be treated in an area where they live or a health centre that is close to where they live. They like to be treated far from where they live, and transport is costly. So that's a problem. I think they still experience stigma. I think stigma around them still exists, so they fear that. (Physician, Male, 49 years, OPD and Hypertension Clinic)
Lack of Hypertension Knowledge and Awareness
Two-thirds of providers described patients’ low levels of hypertension knowledge as a major barrier to care. Providers reported patients were unaware that hypertension was an asymptomatic, chronic disease that required life-long treatment. They observed that patients typically adhered to antihypertensive medication when feeling ill and then stopped taking the drug when asymptomatic. Some providers stated that patients believed their hypertension was a temporary problem that could be cured through prayer, an alternative type of treatment, or temporary use of antihypertensive medication.
Most of them don't follow the instructions. When you tell them to use the medication for the rest of their life, they stop (the medication). Sometimes their blood pressure will increase suddenly because they used medication (temporarily) and then they stopped taking it…I think they have no idea about how to treat hypertension and they don't want to use drugs because they think using drugs daily is not a good habit, so they stop. When they feel okay, they just stop…They don't know how bad hypertension is, that's why. (Nurse, Female, 47 years, OPD, HIV and Hypertension Clinic)
Providers also noted that some patients questioned if their HIV or antiretroviral therapy (ART) caused their hypertension, leading to concerns of possible nonadherence to both antihypertensive and HIV treatment.
The problem with clients who have HIV and hypertension is that they may think that their ART is causing their blood pressure to be high…They say, “Since I have started taking these drugs (ART), I’m not feeling well”. So, there is a danger of not adhering to ART. That is a very big concern to me. (Clinical Officer, Male, 48 years, HIV Clinic)
Other providers believed that while patients considered HIV to be a serious disease, they did not view hypertension as a serious medical problem mainly due to their lack of knowledge about hypertension.
Barriers at the Provider Level
Insufficient Hypertension Training and Gaps in Knowledge
Hypertension knowledge among healthcare providers varied by level of training. Of the 3 levels of providers, physicians reported having the most training on hypertension management and were also the most knowledgeable. Most providers reported only receiving hypertension training during their schooling. A few nurses described only receiving “on the job” training. One clinical officer stated she received no formal hypertension training and explained that she gained knowledge about hypertension primarily from reading on her own and through her clinical practice. Another clinical officer noted that while he received hypertension training during his schooling, many years had passed, and he acknowledged forgetting much of what he previously learned. He also believed that most healthcare providers in Tanzania lacked hypertension knowledge due to limitations in continuing medical education and training.
Training per say? No. That doesn't exist here. We just use the knowledge from the education we received at the university (during medical school) and you get management experience from treating hypertensive patients. Training as the way we receive training for HIV? They do ignore hypertension so much. I have never seen that thing. (Physician, Male, 35 years, OPD and Hypertension Clinic)
Hypertension knowledge was very good overall. All providers were aware of the modifiable lifestyle factors that contributed to hypertension (eg, an unhealthy diet, high salt intake, alcohol and tobacco use, a sedentary lifestyle, and obesity). All providers were also aware of the importance of antihypertensive drugs and the lifelong duration of treatment and they aimed to follow the national standard treatment guidelines for selection of antihypertension agents. However, all nurses and about half of all clinical officers believed that stress was the most common cause of hypertension among PWH, and that stress reduction through counselling was effective primary treatment. Some providers explained that the lack of prioritization and funding towards noncommunicable diseases (NCDs) led to knowledge gaps in hypertension, especially in comparison to diseases that receive substantial financial support, like HIV.
You know many healthcare workers deal with diseases such as HIV and so forth, but they ignore hypertension…They see that there isn't much funding placed towards this disease. So, they don't think it's a hot issue…When you call people to listen to new findings on HIV, a lot of people will come because they think that's something that touches many people. But when you want to present findings for hypertension, very few people will attend. People forget that this (hypertension) is a burning issue and it touches a lot of people, and they act as if this problem doesn't even exist. (Physician, Male, 35 years, OPD and Hypertension Clinic)
Inefficient Antihypertensive Prescribing Practices
Providers reported that they typically gave patients a one-month supply or less of antihypertensive medication. Some providers acknowledged that they prescribed antihypertensive medication a week at a time in order to try and promote frequent follow-up. Providers explained that they often asked patients to come to the clinic multiple times over the course of a month or a week for blood pressure measurements and would then provide prescriptions for antihypertensive drugs accordingly. These practices may have led to nonadherence due to logistic limitations for the patient.
After diagnosing the patient with high blood pressure, most of the time we write a month prescription and then they should come back for a check-up. But if you are not sure of the diagnosis, then we prescribe for two weeks, one week or even 5 days for some patients and then you tell them to come back. (Clinical Officer, Male, 45 years, OPD)
Challenges With Hypertension Counselling
More than half of all providers acknowledged the importance of counselling and communication in hypertension management, including counselling about lifestyle modification, medication use, and duration of treatment. Participants believed that counselling was imperative for treatment adherence, and explained that patients were often nonadherent to antihypertensive drug therapy when they were not adequately counselled about potential side effects or the required duration of treatment. Providers believed that because patients were adherent to their HIV treatment, they would also be adherent to their hypertension treatment, but only if they received proper counselling. However, due to high patient volumes, providers described lack of time to adequately counsel patients on medication adherence, potential side effects, drug-drug interactions, and appropriate follow-up and next steps in treatment. As a result, this lack of guidance may have led patients to have suboptimal antihypertensive medication adherence.
They will (take antihypertensive medication) if you counsel them well. You tell them the advantages of using antihypertensive medication and disadvantages of stopping it and the advantages of using HIV medicines and disadvantage of stopping it. And if you sit with them for a long time, telling them, they will use the medication. The problem is when you are counselling them, you have to take time. For every clinic appointment they attend, you have to talk, to repeat yourself. The problem is having a high burden of patients and a few health workers. You see there is a queue; there are many patients. You can't spend a lot of time with one patient so you hurry so that you can finish with them. (Clinical Officer, Female, 53 years, OPD)
Barriers at the System Level
Limitations in Clinic Capacity for Hypertension Care
All providers discussed multiple limitations in clinical capacity as the predominant barrier to hypertension care. Limitations in capacity that affected both PWH and those without HIV included staff shortages, lack of available antihypertensive medication, and insufficient laboratory facilities. All providers stated that due to the high volume of patients, shortages in prescribing providers and specialists were a major issue that impacted the quality of care received. Providers also described lack of available antihypertensive medications in the pharmacy as a common barrier. Providers explained that well tolerated, first line, medications were often not available, and so antihypertensive medications known to cause side effects were prescribed, which may have led to nonadherence. Ill equipped laboratory facilities were another barrier commonly described by providers who practiced in the primary health centers. Providers from these centers often referred their patients to larger hospitals for laboratory investigations. However, once referred, challenges with transportation and cost would prevent patients from acquiring the laboratory studies.
Some capacity related barriers were described as more specific to PWH and included limitations in blood pressure equipment, privacy, and integrated care. Lack of physical space and a subsequent loss of privacy and confidentiality were commonly reported barriers that affected PWH.
If a patient comes to the HIV clinic…we cannot communicate (confidentially) with them. We can communicate with the group (of patients) but not with just one patient. It's a problem here in the HIV clinic…because of the small space. (Nurse, Male, 29 years, HIV Clinic)
Providers described lack of blood pressure equipment in the HIV clinic as another challenge to hypertension care. One clinical officer noted that functioning blood pressure machines were not readily available in the HIV clinic.
What we need is a blood pressure machine that is well functioning, because some of the blood pressure machines, they will have abnormal results. Like the one there (in the HIV clinic), before you even record it, it already reports it's been recording for five minutes. So, whenever you give the patient their results, it is not accurate. (Clinical Officer, Male, 48 years, HIV Clinic)
A few providers believed that the lack of integration between HIV and hypertension care was a challenge for hypertensive patients with HIV due to the inefficiency and inconvenience of having to attend 2 separate clinics.
It is very difficult for a patient to be here at the HIV clinic and then referred to the OPD. The patients have been waiting a long time, they are tired and want to go home. If you refer them to the OPD, they say “Ah! Why me? I’m tired” So, it's not good. It's better to also have (hypertension care) here in the HIV clinic. (Nurse, Female, 44 years, HIV Clinic)
Some providers believed that while integration of hypertension and HIV care would be ideal, restrictions in capacity such as staff shortages and space constraints would make integration difficult.
Sometimes the doctor is not available. Only the nurse is available, and if she checks the blood pressure (and it is high), there is no doctor to prescribe medication. So, she has to refer the patient to the OPD. (Clinical Officer, Female, 42 years, HIV Clinic)
High Costs of Hypertension Care
All but 2 providers reported that the high costs were significant barriers to hypertension care. Costs for hypertension care included the costs for medications, clinic visits, transportation to and from the clinic, laboratory investigations, and referrals for specialists and higher levels of care. In addition, while providers mentioned that coverage of hypertension services was available through health insurance, they also expressed concern that the insurance premiums were expensive and unaffordable for many patients with HIV, who may have a lower socioeconomic status. Nonadherence to antihypertensive treatment was frequently attributed to the high costs of hypertension care. In contrast, providers noted that that HIV care was completely free, ART was readily available, and that adherence to HIV treatment was very good.
Everything trickles to how much someone can actually afford in terms of medication. I think a good number of patients with HIV do not have stable jobs or a stable income. Some of them are struggling to even come to the clinic to collect their ART. So, on top of that, when you give them a prescription to go and buy a month supply of antihypertensives that costs 30,000 Tanzanian shillings (approximately 13 US dollars), they can't afford it. (Physician, Male, 42 years, OPD)
Lack of Routine Hypertension Screening and Follow-up
Most providers reported that while routine hypertension screening was done in the OPD, it was not performed in the HIV clinic, where blood pressure was typically only measured upon patient request or if a patient described feeling ill. Even in these scenarios, the patient typically required referral from the HIV clinic to the OPD for blood pressure measurement and further evaluation.
We don't measure the blood pressure of the patient here (in the HIV clinic), but when we ask our patients questions, “How do you feel? Do you have a history of high blood pressure in your family?” When you get a patient who says, “Yes”, we refer them to the OPD to get their blood pressure checked. But it is not done routinely in the HIV clinic. (Nurse, Female, 44 years, HIV Clinic)
Providers explained that staffing limitations, high patient volumes, and lack of provider awareness and functional blood pressure equipment prevented the implementation of routine hypertension screening within the HIV clinic.
I think it's just routine (that blood pressure is not measured in the HIV clinic) because we’re used to checking for opportunistic infections, but, not for NCDs. We don't deal with them (NCDs) that much. But we are supposed to screen….It's just because it's not taken seriously…I think we need to raise awareness on the importance of screening for high blood pressure in our clinics. (Physician, Female, 29 years, HIV Clinic and OPD)
In addition to challenges in hypertension screening, providers also reported that patients with HIV often lack routine follow-up for their hypertension.
We counsel them to take the (antihypertensive) medication and we just tell them, “If you feel bad on any day, you can come back.” Actually, there is no real protocol for following them up. (Nurse, Female, 40 years, HIV Clinic)
Challenges With Hypertension Data, Guidelines, and Protocols
Most physicians reported that hypertension management protocols were available at the OPD and they tended to use the national guidelines from the Ministry of Health for hypertension treatment. However, while protocols were often available at the OPD, they were not accessible in the HIV clinic and some providers acknowledged they were not aware of hypertension protocols at their facility. In addition, some providers explained that they did not know that hypertension was a problem among PWH due to the lack of data on hypertension and PWH in SSA.
I don't have data because I just treat them without following them up. I don't have data. I think it (hypertension among PWH) is a problem, but without data we don't talk about anything. (Nurse, Female, 47 years, OPD, HIV and Hypertension Clinic)
Opportunities for Improvement
Improving Resources, Funding, and Prioritization for Hypertension Care
Universally, all providers believed that capacity development and resource allocation towards hypertension care was critical in improving hypertension outcomes among PWH. Suggestions for improvements included integration of HIV and hypertension care to address the lack of routine screening and follow-up, universal health care coverage for NCD care to address the high costs of care, increasing the number of clinical staff to address human resource limitations, increasing the physical space of health facilities to address infrastructure constraints and confidentiality issues, and prioritizing national funding and allocation of resources towards hypertension and other NCDs.
One physician believed that expansion of primary care health services was crucial for improving hypertension outcomes among PWH, and described that while there is a high demand for primary care, patients are often not able to obtain these services at medical facilities due to challenges with cost and access to care.
People are afraid to come to the hospital because of the cost. Now there is this push towards universal health care coverage so that every citizen will have health insurance. Maybe, that is the only thing that is going to get us out of trouble! Because if you announce that there is going to be a two-day health screening at a health fair, you will get so many people beyond your imagination! At the very same time, people are not coming to the hospital! They’d rather go to a tent at the health fair to get their blood and urine tested. That speaks volumes about the inaccessibility of health services like primary care within our own communities. (Physician, Male, 42 years, OPD)
A few providers believed that the same prioritization, financing, and resources allocated towards HIV care was necessary for NCD and hypertension care.
I think the same strength placed in HIV should be placed in hypertension and diabetes because they are the leading conditions that are causing a lot of challenges. Also, most of the patients that are diagnosed are not well off. Their socioeconomic status is not good, and our patients end up getting renal failure and they cannot afford dialysis, so they end up dying. We need to put the same strength that we put into HIV, into other co-morbidities such as hypertension. (Physician, Female, 29 years, OPD and HIV Clinic)
Task-Shifting to Deliver Hypertension Care
The delivery of hypertension care through task-shifting approaches, utilizing a nurse or community health worker instead of a physician for the delivery of care, was discussed with providers. Providers believed this model of care could be a potential solution to address staff shortages, high patient volumes, and time restraints. Most providers thought that a nurse or community health worker could help with patient navigation, blood pressure screening, patient education, and lifestyle modification counselling. Some providers referenced existing HIV programs that utilized community health workers as an example of a successful task-shifting model of care.
(A community health worker) would be helpful. The same way we have been screening our patients for HIV in the community, I think it would also be very good to have healthcare providers who screen patients in the community to rule out hypertension, and then make sure all patients found to be hypertensive are brought to medical attention. (They could) also train the community on the importance of investigating NCDs, including hypertension. They could raise awareness of hypertension and the ways to prevent it, and screen to get an earlier diagnosis in our communities. That will be very helpful. (Physician, Female, 29 years, HIV Clinic and OPD)
However, almost all providers stated that there would be limitations to the care a community health worker could provide and that strict boundaries regarding roles and responsibilities should be enforced.
Hypertension Education and Training
Most providers also believed that implementing hypertension education for patients in the community and in the clinic, similar to large-scale HIV educational campaigns, was of utmost importance.
I think the best (way to improve hypertension care) is to give them (patients) education. Maybe a brochure should be available at the health centre with simple language and information on how to maintain blood pressure and how to prevent hypertension. Maybe having a routine health campaign would be helpful? I have never heard about campaigns (for hypertension). Maybe distributing posters and brochures to the community could help. (Nurse, Female, 44 years, HIV Clinic)
In addition, providers requested more opportunities for NCD and hypertension training for healthcare workers in order to increase awareness of hypertension and cardiovascular diseases in PWH.
I think capacity building through provider training (is important). You know when we are trained, we get empowered and we can work efficiently for our patients. (Physician, Male, 49 years, OPD and Hypertension Clinic)
Hypertension Telehealth Services
The use of telehealth technology via telephone calls and text messaging was also discussed with some providers. Overall, providers believed that text messaging and phone calls would help build rapport between patients and providers and could be used for appointment reminders and medication adherence monitoring. Some providers also believed that since telehealth strategies have been successful with HIV care it would also be helpful in NCD management.
We have seen that (telehealth services) have been very successful with HIV and they are now doing it for tuberculosis…It's very good. It's also encouraging to remind these patients of their clinic appointments…and it keeps you close to the patients. Sometimes we just prescribe medications to patients but if we were closer to them, we would be able to treat them in many other ways far from medication alone. (Physician, Male, 35 years, OPD and Hypertension Clinic)
However, providers brought up a number of limitations with telehealth services including lack of access to telephones and mobile service, electricity outages, illiteracy, and confidentiality issues.
Discussion
In this study, healthcare workers described their perspectives and experiences caring for patients with both HIV and hypertension in northern Tanzania. Participants in our study revealed multiple, intersecting barriers to hypertension care at the patient, provider and system-level. Notably, system-related challenges were the most dominant and were the underlying cause of almost all barriers observed at the individual level. These findings suggest that strengthening of NCD health systems is critical for overcoming barriers to hypertension care, and that evidence-based interventions that focus on developing infrastructure and healthcare capacity are urgently needed to improve cardiovascular outcomes among PWH in SSA.
HIV-related stigma, stress and mental health conditions, such as depression, were identified as significant barriers to hypertension care at the patient level. Participants in our study suggested that HIV-stigma led to increased stress and depression, which may have led to disengagement and avoidance of the medical system and subsequent antihypertensive nonadherence. HIV-related stigma is known to negatively impact HIV-care engagement and ART adherence. 22 Evidence also suggests that HIV-stigma is associated with disengagement and poor clinical outcomes for other chronic diseases. 23 Given the increasing prevalence of cardiovascular disease among PWH, these findings highlight the need to address stigma and mental health in order to improve engagement for NCD care. In addition, further research investigating the associations between HIV-related stigma, mental health, and NCD outcomes among PWH in Tanzania and similar settings are needed.
Gaps in NCD training, inefficient prescribing practices and challenges with counselling were major obstacles reported at the provider level in our study. However, limitations at the system-level were the underlying cause of all provider-related barriers. Providers aimed to adhere to the national treatment guidelines for hypertension care; 9 however, clinician shortages and high patient volumes led to insufficient time to work with patients to provide individualized, patient-centered care. These time restrictions often resulted in suboptimal counselling, substandard prescribing practices, and lack of guidance regarding patient follow-up. In addition, gaps in NCD training and, consequently, in NCD management skills were attributed to lack of NCD prioritization at a national level. Similar studies in SSA have found an association between inadequate healthcare infrastructure and shortcomings in provider knowledge and practices.24-26 Therefore, prioritizing NCD care and increasing human resource capacity may be fundamental strategies to improve provider related barriers and hypertension outcomes among PWH.
Providers universally reported that system-related barriers were the most significant obstacles to hypertension care. System-level challenges included staff shortages, high costs of hypertension care, ill-equipped facilities for hypertension management, lack of routine hypertension screening, and a paucity of funding for NCDs. These findings are consistent with data exploring barriers to hypertension care faced by the general population in SSA.27-29 Our findings also suggest that system-level challenges were the underlying cause of most obstacles at the patient and provider level. For example, clinician shortages in combination with high patient volumes led to restrictions in hypertension screening, management and follow-up practices. These shortcomings then impacted patients’ levels of hypertension knowledge and led to issues surrounding treatment adherence. Furthermore, the majority of barriers depicted were specific to hypertension and were not encountered in HIV care: the high cost of hypertension care is a barrier unique to NCDs as all HIV-related services in Tanzania are free, 30 patient and provider-directed HIV educational and training programs are robust in contrast to those targeting NCDs, and HIV screening is widely implemented in comparison to screening for NCDs. 31 HIV care in Tanzania and similar settings have overcome many of these health system barriers, in part, by creating a heavily invested, parallel system of healthcare delivery that offers long-term care and treatment.32,33 This siloed approach has led to successful and efficient delivery of HIV care, but has also created challenges for the management of chronic diseases beyond HIV. For example, participants in our study described lack of integration between hypertension and HIV care as a major obstacle in hypertension care that is unique for PWH. The growing burden of NCDs among PWH in SSA has the potential to overwhelm this siloed and strained health system if limitations at the system level are not promptly addressed.
HIV care and treatment programs in SSA, including Tanzania, have been successful largely due to enormous efforts in global and national campaigns, financing, and resource strengthening.34,35 These investments have positively impacted clinical outcomes along the HIV treatment cascade: among those aware of their HIV diagnosis in Tanzania, 92% are on treatment and 87% have achieved virologic suppression. 35 In contrast, previous research in northern Tanzania revealed that among hypertensive PWH, 10% are on antihypertensive treatment and none have achieved blood pressure control. 10 In order to address the barriers faced along the hypertension treatment cascade, prioritization, funding, and strengthening programs at a national level, similar to those performed for HIV must be conducted for other chronic diseases. Moreover, the success of HIV clinical programs in SSA could be translated to other chronic diseases affecting PWH. Integrating NCD care into HIV clinical programs is one approach that has shown promise in improving hypertension outcomes among PWH; this approach utilizes existing infrastructure and avoids additional burden on an already taxed system.36,37 Furthermore, the harnessing of strengths of HIV programs towards NCD management is in line with national goals. In 2016, the Ministry of Health in Tanzania created guidelines supporting the integration of HIV and NCD services in order to address the barriers to linkage, initiation, and retention to care for comorbidities afflicting PWH. 31 The findings from our study support these guidelines; however, successful integration of HIV and other chronic diseases will require a provision of resources directed towards NCD care to overcome the numerous limitations in clinical capacity.
Actionable ideas to improve hypertension outcomes among PWH were described by participants in our study. These include task-shifting strategies to address clinician shortages, phone-based services to address treatment adherence, educational campaigns to address limitations in patient knowledge, and skill building programs to address gaps in provider training. However, universally, all providers believed that capacity building of the broader health system was fundamental for improving hypertension outcomes among PWH in Tanzania. Capacity building strategies included universal coverage for NCD care and treatment, increasing the clinician to patient ratio, and allocating funds and clinical resources for NCD care. In 2010, the WHO created a call to action for the prioritization of NCDs globally, including in SSA. 38 The Tanzanian Ministry of Health has recognized this call to action, and in 2016 developed a strategic plan to strengthen health systems and national capacity for NCD prevention and control in the general population and in PWH. 39 Our findings are in line with these goals, and support the further study, development, and implementation of evidence-based interventions to address the rising burden of NCDs among PWH.
This study had several limitations. First, social desirability bias may have influenced participants’ responses; specifically, participants may have felt pressure to appear competent and may have minimized concerns or challenges which may have been exacerbated by one of the interviewers being a physician. Second, our recruitment strategy only included medical providers from an urban area in northern Tanzania. Therefore, the findings may not be generalizable to all providers in this geographic region. Finally, we recognize that the relatively small sample size may not have allowed for making a robust comparison of themes across the different provider levels of training. Additional research is needed to explore hypertension care perspectives from a larger sample of medical providers. In addition, patient perspectives from both urban and rural areas in SSA are needed to better understand the barriers to hypertension care faced by PWH.
Conclusions
In conclusion, healthcare workers who care for patients with both HIV and hypertension described multiple, intersecting barriers to hypertension care at the patient, provider, and system level. However, system-related challenges were the most dominant and were the underlying cause of most barriers seen at the individual level. Strategies that focus on strengthening capacity and utilize existing HIV platforms to expand NCD care delivery are urgently needed to address the growing burden of NCDs among PWH in SSA. As PWH continue to age, and are further affected by chronic diseases beyond HIV, it will become increasingly imperative to develop evidence-based interventions that address the challenges impeding high-quality NCD care.
Footnotes
Acknowledgments
We would like to thank the health care providers who participated in the study for their time and for sharing their perspectives and experiences. We appreciate support from the Duke Global Health Institute and the Duke Hubert-Yeargan Centre for Global Health for this research. We would like to thank the staff from the Kilimanjaro Clinical Research Institute and the KCMC-Duke Collaboration for all their efforts and support for this study.
Authors’ Contributions
PM, NMT, and MHW conceived the study; PM, NMT, and MHW designed the study protocol; PM, BTM, and MHW implemented and supervised the study; PM and LW collected the study data; PM, LW, and SWG performed the data analysis; PM drafted the manuscript; PM, LW, SWG, NMT, BTM, and MWH critically revised the manuscript for content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethics approval was obtained by the Duke Health Institutional Review Board (Pro00091126), Kilimanjaro Christian Medical University College Research Committee (No. 2265), and the Tanzania National Institute for Medical Research Ethics Coordinating Committee (NIMR/HQ/R.8a/Vol. IX/2779). All participants provided written informed consent prior to study participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the US National Institutes of Health Fogarty International Centre (grant number D43TW009337) and by the National Institutes of Health Ruth L. Kirschstein National Research Service Award (grant number T32AI007392). The funders had no role in study design, data collection, analysis, interpretation, or in writing the manuscript.