
Abstract
Beliefs that it is harmful to mix medications with alcohol (ie, interactive toxicity beliefs) are a known source of intentional antiretroviral therapy (ART) nonadherence. This study examined a serial process model of alcohol-ART interactive toxicity beliefs, alcohol-ART avoidance behaviors, and ART adherence in the association between alcohol use and HIV viral load. Participants were 198 patients receiving ART from a community clinic in the southeastern United States; 125 reported current alcohol use. Results showed that current alcohol use was associated with detectable HIV viral load, partially accounted for by alcohol-ART interactive toxicity beliefs, alcohol-ART avoidance behaviors, and ART adherence. There was a significant indirect effect of the serial chain of interactive toxicity beliefs—avoidance behaviors—adherence, indicating the 3 intermediating variables partially accounted for the relationship between alcohol use and HIV viral load. Addressing alcohol use as a barrier to ART adherence requires multipronged approaches that address intentional nonadherence.
What Do We Already Know about This Topic?
Alcohol is a robust barrier to HIV treatment adherence, and beliefs about mixing alcohol with medications further diminish adherence.
How Does Your Research Contribute to the Field?
Beliefs that it is hazardous to mix alcohol with antiretroviral medications are directly associated with behaviors aimed to avoid mixing alcohol and medications, leading to intentional nonadherence.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Interventions targeting alcohol use as a barrier to antiretroviral medication adherence should directly address alcohol-medication beliefs and behaviors to reduce intentional nonadherence.
Introduction
Antiretroviral therapy (ART) has transformed HIV infection from a nearly universally fatal disease to a manageable chronic illness. By suppressing HIV replication, ART dramatically slows the course of HIV infection and prevents the onset of AIDS. In addition, early treatment with ART preserves the immune system and reduces HIV infectiousness. 1 Advances in ART have lowered pill burden, reduced drug toxicities, and offer regimens that are more forgiving of nonadherence. 2 However, lower pill burden and effective drug dosing with even once-daily ART regimens have not always resulted in marked improvements in viral load relative to twice-daily regimens. 3,4 Previous estimates in what has become known as the HIV treatment cascade were that 1 in 5 people with HIV who are treated with ART have detectable HIV viral loads. 5 Recent research shows that these concerning estimates are actually overly optimistic, with more than 1 in 3 people (38%) receiving ART in clinical care not demonstrating durable control of HIV replication. 6 -8 Among the reasons for these missed opportunities are the challenges that many people living with HIV face in achieving and sustaining treatment retention and ART adherence. 9,10 Alcohol and other drug use are among the most common factors at the core of disparate HIV-related health outcomes. 11
Alcohol use, for example, effects memory, planning, organizational, and other cognitive functions that can result in missed medical appointments, prescription lapses, and missed medication doses. 12 Studies show temporal and dose–response relationships between alcohol consumption and missed ART, with drinkers missing more doses than nondrinkers and binge drinkers missing more doses than nonbinge drinkers. 13 The dose–response relationship between alcohol and ART adherence further shows that even limited or occasional use of alcohol impedes ART adherence. 14,15 Alcohol use itself can accelerate HIV disease progression both directly by decreasing CD4 cells 16 and indirectly by interfering with ART adherence. 13 More concerning than sporadic missed doses are prolonged treatment interruptions that can occur with drinking. 17 Among people living with HIV who drink alcohol, as many as half are nonadherent to ART and treatment interruptions when drinking are closely associated with overall nonadherence. 18 And while alcohol use can impede adherence by causing missed doses and unintentional lapses in medication taking, there is growing concern that beliefs regarding the hazards of mixing alcohol with ART can lead to intentional nonadherence. 18
Medication beliefs are potent determinants of adherence to medicines. 19,20 Specific beliefs about the risks for toxicity from mixing ART with alcohol, known as interactive toxicity beliefs, such as believing that alcohol and ART should never be mixed and that alcohol interferes with the effects of ART, have been shown to adversely impact ART adherence. 18 In the absence of co-occurring liver disease, there are no risks associated with moderate drinking and taking ART, and even heavy drinking poses limited risks with only certain classes of ART. 21,22 The association between mortality and alcohol use among people living with HIV who do not have liver complications is therefore attributable to the independent health effects of alcohol abuse and the impact of alcohol use on ART adherence. 23 Alcohol interactive toxicity beliefs are common among people living with HIV, including persons who continue drinking while taking ART. 24 Alcohol interactive toxicity beliefs may motivate some people to stop drinking when initiating ART. 18 However, among individuals who continue using alcohol after initiating ART, half report skipping their medications when drinking. 25 Furthermore, these associations are observed at the day level. Specifically, in studies that have monitored daily drinking and ART, results show that interactive toxicity beliefs predict nonadherence on days when drinking coincides with medications. 25 One study that monitored daily ART adherence and daily alcohol use over the course of 2565 patient-days found that alcohol interactive toxicity beliefs predicted ART nonadherence on days when drinking and not drinking, with interactive toxicity beliefs accounting for more variance in nonadherence than frequency of alcohol use, depression, and general medication concern beliefs. 26 And while interactive toxicity beliefs are found across cultures with similar impacts on ART nonadherence, 27 -30 the mechanisms by which interactive toxicity beliefs impede adherence have not yet been reported.
The current study was undertaken to examine interactive toxicity beliefs and associated behaviors as mechanisms in the association between alcohol use and poor clinical outcomes among people living with HIV who are receiving ART. We specifically tested 3 hypotheses in the context of a serial process model (see Figure 1) where the effects of alcohol use on HIV viral load (undetectable/detectable) would be partially accounted for by 3 serially positioned variables: interactive toxicity beliefs—alcohol-ART avoidance behaviors—ART adherence. First, we hypothesized there are direct effects of alcohol use on HIV load; greater alcohol consumption would be directly associated with greater likelihood of detectable HIV viral load. Second, we hypothesized serial direct effects of greater alcohol use on interactive toxicity beliefs, which would predict behaviors intended to avoid mixing alcohol and ART, and which in turn would predict poorer adherence, and ultimately detectable HIV viral load. Our third hypothesis concerned the indirect effects of alcohol use on HIV viral load through the serially related intermediating factors (beliefs-avoidance behaviors-nonadherence); alcohol’s indirect effect on viral load would be through the chain of all 3 intermediating factors.
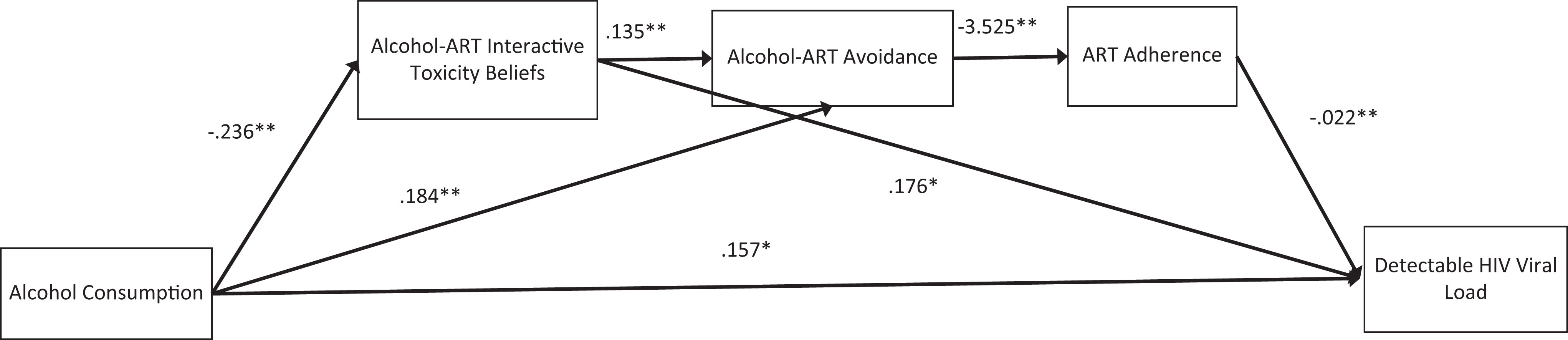
Serial process model predicting HIV viral load from alcohol use through interactive toxicity beliefs, alcohol-ART avoidance behaviors, and ART adherence. Note: *P < .05, **P < .01.
Methods
Setting and Participants
Patients were actively recruited from a publicly funded HIV clinic in central Georgia serving a small city and surrounding rural areas. More than 65% of people living with HIV in rural areas of the United States reside in southern states and more than half of people living with HIV in Georgia are in areas outside of major metropolitan areas. 31 The 13 counties served by the clinic have residents living in poverty at more than double the national rate. 32 A total of 124 men and 74 women completed the study measures between February and April 2016. Participants were receiving HIV treatment at the clinic site. None of the participants in this study had been diagnosed with significant liver disease.
Audio Computer-Assisted Self-Interviews
Demographic and Health Characteristics
We collected participant demographic characteristics (ie, gender, age, years of education, race, employment status, etc), history of incarceration, mental health treatment, and substance use services.
Alcohol and Other Drug Use
To assess alcohol use, we administered the Alcohol Use Disorders Identification Test (AUDIT), a 10-item scale designed to measure alcohol consumption and identify risks for alcohol abuse and dependence. 33 The first 3 items of the AUDIT represent quantity and frequency of alcohol use and the remaining 7 items concern problems incurred from drinking alcohol. The first 3 items of the scale were used to index quantity and frequency of alcohol use in the previous month, composing the AUDIT–Consumption (AUDIT-C) subscale. Scores on the AUDIT-C range from 0 to 12 with acceptable internal consistency 34 ; current study internal consistency, α = .90. We also asked participants whether they had used other drugs in the past month, including marijuana, cocaine/crack, inhalants (eg, poppers), and amphetamines.
Alcohol-ART Interactive Toxicity Beliefs
Participants completed 3 indicators of diverging beliefs about drinking alcohol and taking ART adapted from previous research. 18 These items represented beliefs and perceptions that it is hazardous to take HIV medications when drinking alcohol with reference to other persons and not asking about personal actions. The specific items were, “Alcohol and HIV medications should never be mixed,” “Alcohol breaks down HIV medications so they will not work right,” and “A person should stop taking their HIV medications if they are going to be drinking” responded to on 4-point ratings, strongly disagree = 1 to strongly agree = 4, and summed to create an overall index (α =.68).
Alcohol-ART Avoidance Behaviors
Participants completed 6 items to assess behaviors that explicitly refer to not taking ART when drinking alcohol. These behaviors were adapted from previous research on substance use–related intentional nonadherence. 35,36 The beliefs are shown in the Results section and were responded to regarding whether participants had personally performed each of the 6 actions, not practiced = 0, practiced = 1. We summed the number of behaviors endorsed to create the index of alcohol-related intentional nonadherence (α = .93).
Medication Adherence
We used a rating scale to assess ART adherence over the previous month. The adherence rating scale, often described as a visual analog scale, asks individuals to indicate the point along a continuum showing how much of their ART they have taken in the past month. For computerized administration, we adapted the response format by using a 100-point slide bar tool anchored by 0%, 50%, and 100%. The standard instructions are designed to counter socially desirable response biases by acknowledging that it can be difficult to take ART. 37 The instructions read, “We would be surprised if most people take 100% of their medications. Below, 0% means you have taken none of their HIV medications this past month, 50% means you have taken half of your HIV medications this past month, and 100% means you have taken every single dose this past month. What percent of your HIV medications did you take?” Participants indicated the percentage of medications taken by clicking their mouse anywhere on the 100-point slide bar continuum. The adherence rating scale used in this study has been found reliable and valid, 38 including significantly associated with HIV load. 39,40
HIV Viral Load and CD4 Count
Lab reports of blood plasma HIV viral load and absolute CD4 counts most proximal and within 3 months of the survey completion were abstracted from electronic medical records. In accordance with HIV treatment guidelines, 41 we define detectable viral load as >200 copies/mL—a threshold that nearly eliminates most cases of apparent viremia caused by viral load blips or assay variability. We used the clinically meaningful determination of detectable/undetectable viral load as the end point in our analytic models. We also collected absolute CD4 counts to describe participant health status; CD4 counts under 500 indicate immune system impairment and values under 200 cells/mm3 are diagnostic for AIDS.
Procedures
Participants were recruited through targeted convenience sampling. During a scheduled office visit, clinic patients were invited to participate in the study. A total of 257 patients were invited to complete the survey while waiting for their clinical appointment and 198 agreed, yielding a 77% response rate. Following informed consent, participants completed the audio computer-assisted self-interview and provided permission for the researchers to retrieve their electronic medical records. Participants were compensated for their time to complete the study measures with a US$15 cash (ATM) card. The university institutional review boards approved all procedures.
Data Analyses
For the purpose of descriptive analyses, we examined the demographic and health characteristics of the entire sample, with 124 persons reporting any current alcohol use and 74 reporting no current alcohol use. Descriptive analyses compared participants who were currently using alcohol as reported on the AUDIT-C to those not using alcohol. Comparisons used contingency table χ2 tests for categorical variables and independent t tests for continuous variables. We also conducted descriptive analyses to identify potential correlates of viral load (undetectable/detectable), using contingency table χ2 tests and independent t tests. In addition, we examined the frequencies of behavioral practices for avoiding mixing alcohol with medications for those participants reporting any alcohol use on the AUDIT-C. Descriptive correlational analyses were also performed with respect to the relationships among variables for all participants. Bivariate associations among continuous variables were examined with Pearson correlation coefficients and point biserial correlations for dichotomous viral load in relation to continuous measures.
Our main analyses tested the serial process model in Figure 1 that specifies multiple associations between alcohol use (AUDIT-C score) → Viral load, accounted for by Interactive Toxicity Beliefs → Avoiding ART when Drinking → ART Adherence. We used the SPSS IBM Process version 3.1 macro to test multiple factors using bootstrap statistical techniques. 42 Multiple intermediating variable models are appropriately analyzed using regression when data are cross-sectional. 43 The PROCESS macro estimates all paths designated in the model. Specifically, we used the model 6 template for multiple (3) variables in an x–y relationship. 42
PROCESS detects binary outcome variables, such as HIV viral load in this study, and estimates the direct and indirect effects, as well as the paths from the intermediating variables to the outcome using logistic regression. Thus, coefficients predicting the intermediating factors are estimated using ordinary least squares regression, and paths for the dichotomous outcome are estimated with maximum-likelihood based logistic regression. To control for duration of HIV diagnosis, years since testing HIV positive was included as a covariate. This model tests the effects of the predictor variable (alcohol use) on 3 intermediating variables (M1 = alcohol interactive toxicity beliefs, M2 = avoiding taking ART when drinking, and M3 = adherence; a paths), the direct effects of the intermediating variables on the outcome (viral load, b paths), and the effects of the predictor variable on the outcome (c path). We computed 95% confidence intervals (CI) for the indirect effects of alcohol use on viral load through alcohol-ART interactive toxicity beliefs, alcohol-ART avoidance behaviors, and adherence that were estimated from 5000 bootstrap resamples. All analyses used P < .05 as the criterion for statistical significance.
Results
Table 1 shows the demographic and health characteristics of the current sample partitioned by current alcohol use. Participants who drank alcohol were significantly more likely to report other drug use, were older, and were diagnosed with HIV infection fewer years. In terms of current health status, 12% of the sample showed evidence of advanced HIV disease with CD4 counts under 200 and 27% had detectable HIV viral loads, with drinkers more likely to have detectable HIV. Table 2 shows the descriptive analyses for comparisons of participants with undetectable and detectable viral loads. Results showed expected differences in ART adherence and CD4 counts, as well as age and a trend for years since testing HIV positive.
Demographic and Health Characteristics of Participants Who Did and Did Report Current Alcohol Use.

Abbreviations: ART, antiretroviral therapy; AUDIT, Alcohol Use Disorders Identification Test; N/A comparison invalid due to empty cells; M, mean; SD, standard deviation.
a P < .01.
b P < .05.
Demographic and Health Characteristics of Participants with Undetectable and Detectable HIV Viral Load.

Abbreviations: ART, antiretroviral; AUDIT, Alcohol Use Disorders Identification Test; M, mean; SD, standard deviation.
a p < .01.
b p < .05.
c p < .10.
Alcohol-ART Avoidance Behaviors
Table 3 shows the number and proportions of the subgroup of participants who drink alcohol as indexed on the AUDIT-C reporting intentional nonadherence behavior when drinking. The most frequently occurring behaviors were waiting to take ART after drinking (55%) and not mixing alcohol and HIV medications because it is not safe (40%). In addition, nearly 1 in 3 participants indicated that they wait to drink if they have taken their ART and 1 in 5 indicated that they stop taking ART when drinking alcohol.
Alcohol-ART Avoidance Behaviors among HIV-Positive Drinkers.a
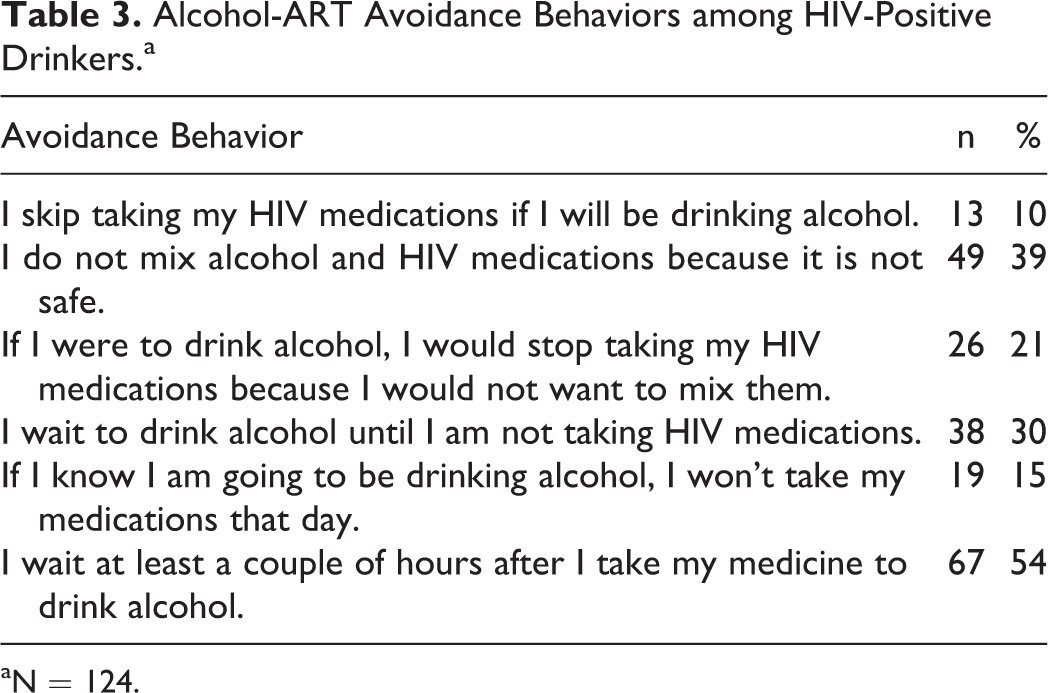
aN = 124.
Bivariate Correlations among Model Variables
Alcohol Use Disorders Identification Test–Consumption-C scores were significantly inversely related to interactive toxicity beliefs, positively related to alcohol-ART avoidance behaviors, and positively related to detectable viral load (see Table 4). Interactive toxicity beliefs were also associated with alcohol-ART avoidance behaviors in the expected direction; greater interactive toxicity beliefs were associated with engaging in avoidance behaviors. In addition, alcohol-ART avoidance behaviors were significantly inversely related to ART adherence and adherence was inversely related to detectable viral load. This pattern of associations was consistent with the proposed process model.
Bivariate Correlations among Model Variables.a
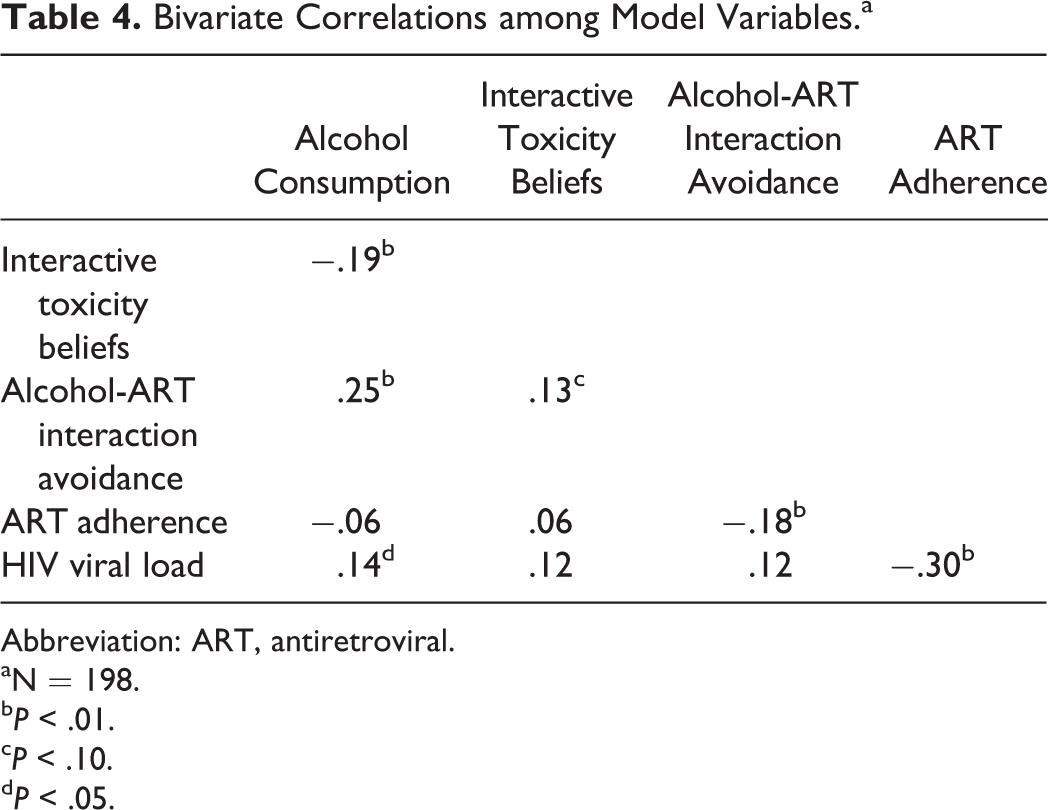
Abbreviation: ART, antiretroviral.
aN = 198.
b P < .01.
c P < .10.
d P < .05.
Alcohol Use and HIV Viral Load Serial Process Model
We tested the serial process model using multiple regression analyses that included alcohol use (independent variable), HIV viral load (dichotomous undetectable/detectable, dependent variable), and alcohol interactive toxicity beliefs, alcohol-ART avoidance behaviors, and ART adherence (intermediate variables). Results of the serial process model are shown in Figure 1. Years since testing HIV positive was included in the model and was not significant in any paths. The full model was significant in predicting HIV viral load, model χ2 = 23.64, P < .001, using McFadden estimated R 2, the model accounted for 11.1% of the variance in viral load.
For tests of direct effects, results confirmed the first hypothesis showing that AUDIT-C scores significantly predicted detectable HIV viral load, b = .157 (se = .073), P < .05, 95% CI: .014 to .300. In the test of the second hypothesis, the direct effect of alcohol use predicting alcohol interactive toxicity beliefs was significant, b = −.236, t = 3.09, P < .01, and alcohol-ART avoidance behaviors, b = .184, t = 4.11, P < .01, but not ART adherence, b = .179, t = −.21, P > .1. Alcohol interactive toxicity beliefs were directly related to HIV viral load, b = .176, z = 2.34, P < .01. Alcohol interactive toxicity beliefs significantly predicted alcohol-ART avoidance behaviors, b = .135, t = 3.16, P < .01, and alcohol-ART avoidance behaviors in turn predicted ART adherence, b = −3.52, t = −2.57, P < .01, and ART adherence predicted HIV viral load, b = −.022, z = −3.60, P < .01.
In the test of our third hypothesis, the indirect effects of the 3 serially positioned factors were tested using 5000 bootstrap resamples. The indirect effect of alcohol use on HIV viral load through the 3 serially aligned factors (Interactive Toxicity Beliefs → Avoiding ART when Drinking → ART Adherence) was significant, b = −.002, se = .002, 95% CI: −.0009 to −.0003. The indirect effect of alcohol use on viral load through interactive toxicity beliefs was also significant, b = −.0041, se = .026, 95% CI: −.1241 to −.0085. All other possible paths were included in the model and none of the other indirect effects were significant.
Discussion
The current study found that 62% of people receiving ART reported current alcohol use. We found that alcohol drinkers were more likely to report other drug use, were older, and were diagnosed with HIV a shorter time than nondrinkers. Current alcohol use was also related to detectable HIV viral load. Among participants who reported current alcohol use, more than half endorsed at least one behavior associated with intentionally avoiding taking ART when drinking. Thirty-nine percent of participants who reported drinking alcohol indicated that they do not mix alcohol and ART because it is not safe and 21% stated that they would stop taking their ART when drinking. We also found that alcohol interactive toxicity beliefs were associated with drinking less and level of drinking was positively related to engaging in alcohol-ART avoidance behaviors. These findings are consistent with past research on alcohol interactive toxicity beliefs 24,25,27 and affirm the current model of underlying mechanisms in the association between alcohol consumption and HIV viral load.
We found support for the 3 study hypotheses that link alcohol interactive toxicity beliefs, alcohol-ART avoidance, and ART adherence in the association between alcohol use and detectable HIV viral load. Alcohol use demonstrated direct effects on viral load and direct effects on alcohol-ART avoidance behaviors, while alcohol-ART interactive toxicity beliefs had a direct effect on viral load. We also found that the indirect effect of the 3 serially aligned variables, interactive toxicity beliefs—avoidance behaviors—adherence, was also significant. These findings show that interactive toxicity beliefs and associated behaviors indicative of intentional nonadherence partially account for the association between alcohol use and viral load. Additionally, the indirect effect of alcohol use on unsuppressed HIV through alcohol interactive toxicity beliefs suggests a unique role of interactive toxicity beliefs on HIV treatment outcomes beyond any specific avoidance and adherence behaviors. It should be noted that our model only accounted for 11% of the variance in HIV viral load, suggesting that additional factors, including unmeasured beliefs and unintentional nonadherence, should be examined in future research. Alcohol interactive toxicity beliefs may impact treatment outcomes as part of a broader spectrum of medication concerns that are known to impede medication adherence. 44,45
Results of the current study should be interpreted in light of its methodological limitations. We sampled participants receiving services from a publicly funded HIV care provider and our sample was one of convenience. Thus, our participants cannot be considered representative of people living with HIV. In addition, the study was conducted in just one state in the southeastern United States and is therefore also geographically constrained. The limitations of self-reported drinking are well-known and likely underestimated alcohol use. We also relied on self-reported measures for all of the other social and behavioral variables in this study. Although we used state-of-the-science measures delivered by computerized interviews, the results are still subject to reporting biases. For example, we did not observe an expected association between alcohol use and ART adherence, and this lack of association may have resulted from the restricted range of drinking reported on the AUDIT-C. Finally, the study design was cross-sectional and therefore does not allow for directional or causal inferences. With these limitations in mind, we believe that the current findings add to the existing literature and have implications for designing interventions aimed to address intentional nonadherence among people receiving ART who drink alcohol.
Interventions to improve ART adherence have typically concentrated on implementing reminders and memory aids, improving medication adherence skills, managing structural barriers to adherence, and resolving other sources of unintentional nonadherence. 46 -48 With respect to alcohol use and adherence, most approaches have either tried to reduce drinking or used strategies for remembering to take medications when drinking. Although sources of alcohol-related unintentional nonadherence remain important targets for interventions, fully addressing the influence of alcohol on ART adherence will require attending to intentional nonadherence as well. Interventions should aim to both reduce missed doses of ART that result from unintentional nonadherence and address interactive toxicity beliefs associated with intentional nonadherence. Clinical assessments of alcohol use should directly assess patient beliefs about drinking and taking ART. It is also important to note that for patients who are diagnosed with liver disease, drinking is highly hazardous, and concerns about mixing alcohol and ART are well-founded. 49,50 Any reassurance that mixing alcohol and ART is safe, therefore, does not apply to patients with co-occurring liver disease.
Believing that it is better to not take ART than mix ART with alcohol should be addressed directly with corrective information. However, disputing erroneous interactive toxicity beliefs should take care not to inadvertently increase alcohol use because reducing alcohol consumption remains an important goal for improving the health of people living with HIV and maximizing HIV treatment outcomes. We therefore suggest taking a broader health literacy approach to correcting interactive toxicity beliefs as opposed to challenging any one given belief. 51 Clear messages with accurate information should be delivered in routine clinical care with the aim of replacing false assumptions and folklore regarding alcohol use and medications.
Footnotes
Authors’ Note
The study was approved by the University of Connecticut Institutional Review Board Protocol H14-184GDPH and all participants gave written informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by National Institute of Alcohol Abuse and Alcoholism Grant R01-AA023727.