
Abstract
Background:
Characterizing viral response to lopinavir/ritonavir (LPV/r) monotherapy as second-line treatment may guide recommendations for resource-limited settings (RLS).
Methods:
We conducted a 48-week prospective, single-arm study of LPV/r monotherapy in patients failing first-line therapy in Nigeria. The primary outcome was sustained HIV-1 viral load (VL) <400 copies/mL at 48 weeks.
Results:
Of 30 enrolled patients, 28 (93%) achieved viral suppression on LPV/r, while 29 (96%) experienced low-level viremia. At 48 weeks, 9 (30%) met the primary outcome of sustained viral suppression; 14 (47%) patients were suppressed on LPV/r in a snapshot analysis. Detectable VLs at 12 and 24 weeks were strongly associated with treatment failure at 48 weeks. New resistance mutations were not detected. The trial was stopped early due to treatment failure.
Conclusion:
In this study, the rate of virologic failure among patients on a second-line lopinavir monotherapy regimen was relatively high and predicted by early detectable viremia. However, no LPV/r-associated resistance mutations were detected despite fluctuating low-level viremia, demonstrating the high genetic barrier to resistance of the protease inhibitor class which could be useful in RLS.
Keywords
Introduction
As of 2012, nearly 10 million people in resource limited settings (RLSs) had received antiretroviral therapy (ART), with an estimated 6% of patients failing first-line therapy each year. 1 Overall rates of failure of first-line therapy have been estimated at 13% to 32%. 2 –4 As second-line ART is significantly more expensive than first-line therapy, 5 defining the most efficacious and cost-effective second-line treatment strategy is of ever-growing importance. 6
First-line therapy in most RLS consists of dual nucleoside/nucleotide reverse transcriptase inhibitors (NRTI/NtRTIs) and one non-nucleoside reverse transcriptase inhibitor (NNRTI), with the recommended second-line therapy being 2 NRTI/NtRTIs plus a ritonavir-boosted protease inhibitor (PI). 7 However, due to cross-class NRTI resistance, the nucleoside backbone in second-line regimens may not retain activity particularly in those patients failing a thymidine analog-containing first-line regimen. Relying on NRTIs despite cross-class resistance unnecessarily exposes patients to potential drug toxicities and added costs and effectively results in PI monotherapy. In addition, many patients may be faced with dose-limiting NRTI toxicities, such as renal insufficiency, anemia, and peripheral neuropathies. Recently, the substitution of an integrase inhibitor for 2NRTIs in combination with a boosted PI did not result in significant improvements in second-line treatment outcomes. 8,9
What Do We Already Know about This Topic?
In clinical trials, treatment efficacy of boosted protease inhibitor monotherapy as second-line therapy has varied from 55% to 87%; yet little is known about who is likely to succeed or fail with this treatment strategy.
How Does your Research Contribute to the Field?
In this prospective open-label study, the rate of virologic failure at 48 weeks among patients on a second-line boosted lopinavir monotherapy regimen was relatively high and predicted by early detectable viremia at 12 and 24 weeks.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Lopinavir/ritonavir (LPV/r) monotherapy may have a role in certain patients but cannot be recommended as second-line therapy in patients without a compelling reason due to a significant risk of low-level viremia and subsequent virologic failure; clinically, patients virally suppressed at 24 weeks are likely to do well on LPV/r monotherapy.
Despite this concern, the role of PI-based monotherapy for second-line treatment in RLS remains undetermined, partially as a result of study design as well as varying definitions of treatment success: AIDS Clinical Trials Group 5230 concluded that lopinavir/ritonavir (LPV/r) Mt with treatment intensification was a promising strategy for durable viral suppression, 10 while the Europe-Africa Research Network for Evaluation of Second-Line Therapy (EARNEST) trial concluded that LPV/r monotherapy did not result in good HIV disease control. 8,10 Here, we report the viral dynamics of HIV in the setting of boosted PI monotherapy as second-line treatment.
Methods
Study Design and Location
A prospective, single-arm, nonrandomized, open-label, proof-of-concept study to evaluate the clinical safety and efficacy of LPV/r monotherapy over 48 weeks was conducted at 2 HIV treatment clinics in Jos, Nigeria: ECWA Evangel Hospital (now Bingham University Teaching Hospital) and Plateau State Specialist Hospital.
Study Eligibility
Adult patients experiencing treatment failure on their first-line regimen of NNRTI + 2NRTIs were recruited for the study. First-line treatment failure was defined as recurrence of previous opportunistic infection (OI), development of a new OI, a decline in absolute CD4+ T-cell count by 15% over 2 consecutive measurements, or a detectable VL >400 copies/mL after at least 24 weeks on the primary antiretroviral (ARV) regimen. In addition, treatment failure was confirmed with a VL >1000 copies/mL at the time of screening.
Patients were excluded from the study if they had laboratory or clinical evidence of advanced AIDS (CD4 < 50 cells/mm3), serious OI (defined as progressive multifocal leukoencephalopathy, cytomegalovirus disease, cryptococcus meningitis, cerebral toxoplasmosis, active tuberculosis, visceral Kaposi’s sarcoma, or at clinician discretion), malignancy, hepatitis, cirrhosis, poorly controlled diabetes, pregnancy or breastfeeding, or any other chronic illness or condition that may have posed a risk to the patient. They were also excluded if they had previously been treated with a PI or had a genotype demonstrating evidence of prior PI treatment.
Treatment Protocol
Following study entry, patients discontinued their previous ARV regimens and began taking LPV/r (Alluvia, supplied by Abbott Laboratories) in fixed-dose combination of lopinavir 133 mg/ritonavir 33 mg, given as 3 tablets by mouth twice a day. Patients had a separate visit focused on medication adherence. Patients completed a total of 15 visits over the 48-week study period. At each visit, patients underwent clinical assessment and screening for adverse events, as well as a symptom-directed physical exam. HIV-1 Viral loads were measured monthly. Hematologic and metabolic indices, including complete blood counts, creatine, aspartate aminotransferase, alanine aminotransferase, glucose, triglycerides, and total cholesterol, were repeated at weeks 24, 32, and 48. CD4 counts were repeated at weeks 12, 24, and 48. A random 10% of VL samples were sent to the University of Maryland’s clinical molecular laboratory for quality assurance purposes. Blood for genotype analysis was collected and stored at enrollment (baseline) and each subsequent visit. Patients that subsequently met criteria for virologic failure had genotype analysis from the baseline sample and at the time point of confirmed failure. Patients meeting criteria for virologic failure underwent treatment intensification with addition of a standardized regimen of tenofovir/emtricitabine (TDF/FTC).
Study End Points
The primary outcome was defined as achieving and maintaining viral suppression (defined as HIV-1 RNA < 400 copies/mL) until trial completion at 48 weeks. Virologic failure was defined as one of the following: (1) after achieving viral suppression, 2 consecutive VLs >400 copies/mL; or (2) failure to achieve viral suppression (<400 copies/mL) by week 24; or (3) failure to achieve 1.0 log VL decline from baseline by week 12. Immunologic failure was defined as 2 consecutive absolute CD4 counts >50% lower than the baseline absolute CD4 count.
Statistical Methods
The intention-to-treat (ITT) analysis compared viral suppression at 48 weeks among patients who remained on LPV/r monotherapy for the entire study, meeting all study requirements, to all patients who met any criteria for protocol failure. Due to delays in VL reporting, some patients remained on LPV/r monotherapy despite meeting protocol-defined failure; hence, we conducted an on-treatment (OT) analysis of all those who remained on LPV/r monotherapy through 48 weeks, regardless of study protocol status. Secondary analyses were also conducted of adverse events and toxicities, changes in virologic and immunologic measurements, metabolic indices, adherence reports, and evolution of resistance mutations. Univariate and multivariate logistic regression were used to calculate adjusted and unadjusted odds of treatment failure.
The sample size of 60 patients was calculated based on prior evidence demonstrating 75% viral suppression in ARV-naive patients on a 3-drug LPV/r-based regimen and an expected suppression rate of at least 60% in ARV-experienced patients. Therefore, using a one-sided alternative and a type I error rate of 0.05, a sample size of 60 patients would provide 72% power to detect a difference between the predicted success rate of LPV/r of 75% and the nominal success rate, 60%. Imputation was performed for missing VLs and CD4 counts by taking the mean of the previous and subsequent values. Statistical analysis was performed using Stata (version 13.1, StataCorp, College Station, Texas).
Role of the Funding Source
The funder played no role in the design, conduction, analysis, interpretation, manuscript development, or decision to submit the manuscript for publication.
Results
One hundred five patients were screened for the study; 30 patients met inclusion criteria and were enrolled. Two patients were excluded for CD4 <50 cells/mm3 and 73 because of VLs <1000 copies/mL at screen. Seventeen of 506 data points were missing, resulting in only 3.4% of data being imputed. Study enrollment was halted at 30 when predetermined futility benchmarks were reached as well as per data and safety monitoring board recommendation.
Table 1 demonstrates the baseline characteristics of the participants. Twenty-five (83%) were women, with median age of 34.5 (interquartile range [IQR]: 31-40) years. At study entry, the median VL was 8302 (IQR: 1944-28 215) copies/mL and the median CD4 was 259 (IQR: 163-314) cells/mm3; median historic CD4 nadir was 143 (IQR: 81-190) cells/mm3. The median duration of prior ART was 29 (IQR: 23-36) months.
Baseline Characteristics of Study Participants.

Abbreviations: ART, antiretroviral therapy; CD4, CD4 + T-cell; IQR, interquartile range; LPV/r, lopinavir/ritonavir.
Table 2 displays the outcomes of study participants. Twenty-eight (93%) patients achieved viral suppression of any duration on LPV/r monotherapy with a median of 4 (IQR: 4-8) weeks to reach suppression; median total duration of viral suppression on LPV/r monotherapy was 22 (IQR: 12-36) weeks. No correlation was found between time to viral suppression and initial VL or initial CD4 count. Viral blips, defined as a detectable VL (>400 copies/mL) between 2 undetectable VLs, were experienced by 96% of the participants, with a median of 1 (IQR: 0-2) blip per patient over the course of the study; median VL recorded during a blip was 1692 (IQR: 940-3621) copies/mL. Seventy-three percent self-reported adherence of greater than 95% throughout the entire study period.
Results of 48 Weeks of LPV/r Monotherapy.

Abbreviations: ARV regime, antiretroviral regime; IQR, interquartile range; LPV/r, lopinavir/ritonavir; VL, viral load.
aRemained on LPV/r at end of study.
bAny other ARV regimen at end of study.
Safety parameters, including cholesterol, triglycerides, glucose, weight, and body mass index were assessed throughout the study and no significant differences were observed between baseline and end line values nor were any significant changes correlated to study success or failure (data not shown).
Figure 1 displays each patient over study time, with viral suppression and study status by line color and pattern. In the ITT analysis, 9 (30%) participants met the primary outcome of sustained viral suppression and 21 patients were ITT failures. Of ITT failures, 17 were virologic failures, 2 persons failed to achieve a 1-log reduction in VL by 12 weeks, and 1 person had not achieved virologic suppression by 24 weeks. One person was removed from the study due to new onset of diabetes. The median VL at the time of protocol failure was 1245 (IQR: 524-3215) copies/mL and the median week of study failure occurred at 20 (IQR: 12-28) weeks. One person was lost to follow-up after week 36 following virologic failure in week 20. The remaining 29 (97%) participants completed the trial.

Chart of each patient’s viral load and study status across study time. Each line represents a patient in the study with viral suppression indicated by line height, antiretroviral therapy by line pattern, and study status by line color. Intention-to-treat successes are represented by the lines in green at 48 weeks; on-treatment successes are represented by the lines that are solid (green or red) at 48 weeks. IQR indicates interquartile range; LPV/r, lopinavir/ritonavir; NRTI, nucleoside reverse transcriptase inhibitor; Pt, patient; TI, treatment intensification; VL, HIV viral load in copies/mL.
Due to a time delay in reporting VLs, all of the 17 ITT virologic failures continued for some period of time on LPV/r monotherapy. Twelve of the 17 subsequently resuppressed with no intervention and thus were allowed to continue on LPV/r monotherapy until some additional indication to intensify their regimen. Of these 12 patients, 7 remained on monotherapy until the end of the study; of those 7, 5 were virally suppressed at 48 weeks. These additional 5 patients were considered to have failed according to the study protocol definition, yet from a clinical perspective successfully remained on LPV/r monotherapy.
Therefore, an OT analysis was also performed, examining all patients who were still on LPV/r monotherapy regardless of ITT status. In the OT analysis, 16 (53%) patients completed the study while still on LPV/r monotherapy; of these, 14 (47%) were suppressed on LPV/r monotherapy at 48 weeks. Furthermore, of the 21 who failed per protocol, 11 (52%) patients resuppressed for at least some period of time while still on LPV/r monotherapy.
Treatment intensification with the addition of 2 NRTIs occurred at a median of 28 (IQR: 28-36) weeks; the median VL at intensification was 1805 (IQR: 0-28 449) copies/mL. From the time of ITT failure to treatment intensification, the median VL decreased by 463 (IQR: −2275-1421) copies/mL. Of the 14 patients receiving dual-NRTI intensification, 9 were suppressed at week 48. Thus at 48 weeks, 23 (76%) patients were suppressed (14/16 on monotherapy and 9/14 on LPV/r + 2NRTIs).
Baseline genotypes were performed on a selected subset of 8 patients and no PI resistance mutations were identified. By week 48, all patients who had had a genotype done had failed per protocol and were on a treatment-intensified regimen with 2NRTIs added to the PI. Six of 8 patients had VL <1000 by week 48; all 3 patients with WT virus at baseline, 2 patients with only M184V, and 1 of 3 patients with M184V + TAMs. Despite the presence of NRTI mutations, patients successfully resuppressed on 2NRTI treatment intensification following virologic failure of PI monotherapy.
Figure 2 panels, A and B, display the graphical trends of VLs over time (only VLs <10 000 copies/mL displayed to permit visualization of low-level viremia). Low-level viremia was present to some degree in all but one patient. Most patients achieved a rapid reduction in VL by week 4 regardless of their starting VL. This was followed by a “hectic” pattern, with high spikes in viral replication followed by different degrees of viral control, and only 3 patients losing complete viral control >10 000 copies. Those patients who required treatment intensification either lost viral control completely or were unable to regain viral control <1000 copies.

Patient viral loads across study time by treatment status at end of study. Display of all HIV viral loads less than 10 000 copies/mL for patients who successfully remained on lopinavir/ritonavir monotherapy at 48 weeks (Panel A, on-treatment successes) and those who failed lopinavir/ritonavir monotherapy by 48 weeks (Panel B, on-treatment failures).
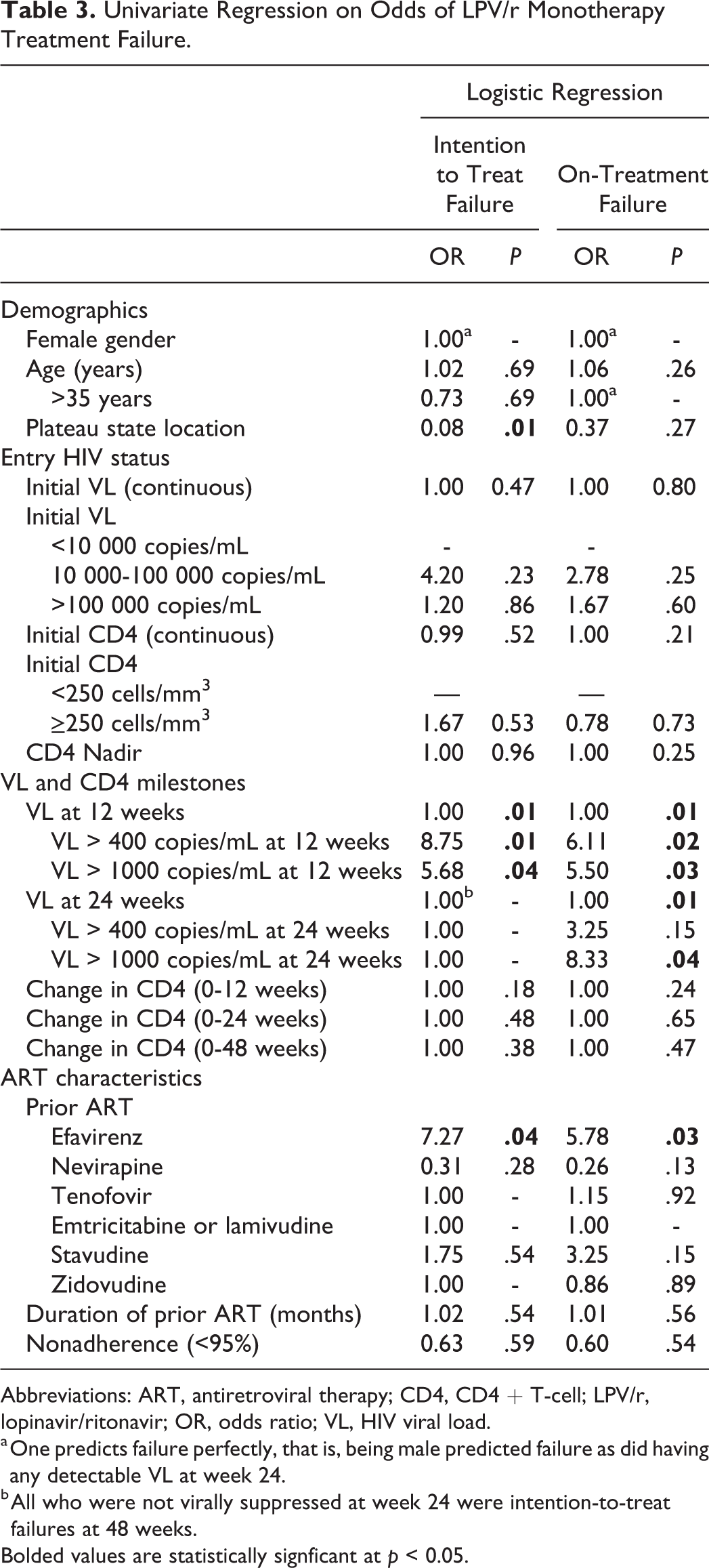
In comparison of ITT and OT success versus failure at 48 weeks, there were no statistically significant differences between groups in terms of baseline VL, CD4 count, historic CD nadir, or self-reported adherence (analysis not shown). Table 3 demonstrates the results of univariate logistic regression on the odds of ITT and OT failure. Female gender was associated with ITT and OT success, as all 5 males in the study failed LPV/r monotherapy (no P value due to collinearity).
Univariate Regression on Odds of LPV/r Monotherapy Treatment Failure.
Abbreviations: ART, antiretroviral therapy; CD4, CD4 + T-cell; LPV/r, lopinavir/ritonavir; OR, odds ratio; VL, HIV viral load.
a One predicts failure perfectly, that is, being male predicted failure as did having any detectable VL at week 24.
b All who were not virally suppressed at week 24 were intention-to-treat failures at 48 weeks.
Bolded values are statistically signficant at p < 0.05.
Detectable VL (>400) at 12 weeks was strongly indicative of treatment failure at 48 weeks, with odds of either ITT failure (odds ratio [OR] = 8.75, P = .01) or OT failure (OR = 6.11, P = .02), as compared to those who were undetectable at 12 weeks. HIV-1 viral loads at 24 weeks were also strongly predictive of treatment failure at 48 weeks. Of those who had a detectable VL at 24 weeks, all went on to be ITT failures (P value not calculated due to collinearity). Detectable VL at 24 weeks showed a nonsignificant trend toward OT failure (OR = 3.25, P = .15); however, this became statistically significant when the VL cutoff was increased to 1000 copies/mL (OT failure: OR = 8.33, P = .04).
Characteristics of prior ARV treatment were examined for potential association with treatment failure. Prior treatment with efavirenz (EFV) was significantly associated with failure; those who had been on a prior EFV-based regimen had a 7.27-fold higher odds of ITT failure (P = .04) and 5.78 higher odds of OT failure (P = .03), as compared to those who had not been exposed to EFV. Self-reported adherence of <95% was not associated with odds of treatment failure.
Multivariate logistic regression (not displayed) was also performed to assess adjusted odds of treatment failure; however, due to low study numbers and collinearity, ORs were frequently inestimable. Intention-to-treat failure was perfectly associated with male gender and detectable VL at 24 weeks, demonstrating that the ITT successes all occurred among women and among those who were suppressed at 24 weeks. Intention-to-treat outcomes were also strongly associated with study location and history of prior EFV treatment, as per the univariate regression. On-treatment failure was also strongly predicted by detectable VL at 24 weeks, male gender, and prior EFV use.
Discussion
In this prospective open-label study, we evaluated the efficacy of second-line ART with LPV/r monotherapy to maintain viral suppression below 400 copies. By strict ITT criteria, LPV/r monotherapy maintained sustained viral suppression in only 9 (30%) patients. Of 30 patients, 28 (93%) suppressed for some period of time on LPV/r monotherapy. In a 48-week snapshot analysis, 14 (47%) patients were virally suppressed among those who remained on LPV/r monotherapy for the duration regardless of loss of viral control during the study. Across the study, low-level viremia was prevalent and lack of viral suppression at 12 weeks was a strong predictor of subsequent failure. Of note, we found no adverse hematologic or metabolic effects associated with LPV/r monotherapy use and no PI resistance mutations emerged during monotherapy use.
Boosted-PI monotherapy trials in naive patients or first-line deintensification trials have achieved treatment efficacy ranging from 70% to 88% 11 –26 ; however, the MONotherapy AntiRetroviral Kaletra (MONARK) trial demonstrated only 47% viral suppression for naive patients at 96 weeks. 27 These trials, primarily completed in Europe and the United States, provided the basis for second-line treatment trials of LPV/r monotherapy in RLS. These second-line treatment trials had treatment efficacy rates of 60% to 65%, 28,29 though the ACTG trial demonstrated efficacy of 87% at 24 weeks. 10 Notably, a recent trial evaluating LPV/r monotherapy deintensification as a second-line treatment strategy in sub-Saharan Africa demonstrated efficacy of only 55%. 8 A recent meta-analysis by Arribas et al 20 assessed efficacy of boosted PI monotherapy versus triple therapy in 2303 patients in 13 randomized trials. They found viral suppression in 73.9% (629/851) of patients on boosted PI monotherapy in the primary switch-equals-failure analysis as compared to 82.0% (710/865) of patients on triple ART (absolute risk difference of 8.3%, 95% confidence interval: 4.8%-11/9%, P < .0001). However, when treatment intensification was included, there was no significant difference between the 2 therapies (87% versus 85%). 20
Working under an FDA IND, our trial was required to monitor VLs every 4 weeks, which offered an opportunity to examine the viral kinetics of HIV in a previously treated population under LPV/r monotherapy. We observed that low-level viremia is pervasive and more frequent than previously described with 96% of patients experiencing viremia after suppression. In the Bamrasnaradura Infectious Diseases Institute MONOtherapy (BIDI-MONO) trial, which assessed VLs every 3 months, 24% had viral blips and 10% had persistent viremia. 11 Manosuthi et al checked VLs at weeks 48, 96, and 144 and found low-level viral rebound in 10% to 15% of patients. 28 In a 2009 systematic review of LPV/r monotherapy, Bierman et al found that only 10% of patients have viral rebound. 30 However, the Second-line Anti-Retroviral therapy in Africa (SARA) trial which assessed efficacy of LPV/r monotherapy following a 24-week induction with combined LPV/r + 2NRTIs found that 40% of monotherapy patients had VLs greater than 50 copies/mL and 14% over 1000 copies/mL at 24 weeks; 5% of the monotherapy group had major PI mutations. 31
Critically, we observed no major PI resistance mutations in our patients. Other studies have similarly found a very low risk of treatment-emergent resistance mutations or loss of future treatment options with boosted PI monotherapy. 18 –20,22,23,32,33
Low-level viremia in PI monotherapy has been attributed to higher adherence requirements given the short half-life of boosted PIs, and nonadherence is a possible explanation for the viremia seen in our patients, particularly those with high spikes and subsequent resuppression in the absence of TI. However, the pattern of viral replication seen in our patients does not suggest poor adherence. The patients were carefully screened for a history of good adherence, had a comprehensive adherence intervention prior to starting second-line, and maintained high levels of self-reported adherence and compliance with study visits. Furthermore, we found no statistical association between viral suppression and adherence. Finally, and most convincingly, the successful viral suppression following treatment intensification with 2 NRTIs without additional adherence interventions suggests that adherence is not the only factor for failure. A similar pattern of successful viral suppression following treatment intensification following boosted PI monotherapy is seen in other trials. 20,33
Protease inhibitors target postintegration, viral translational amplification. This might allow for a state of cellular activation and increased potential for viral replication which monotherapy PI treatment cannot reliably prevent. Increased environmental stimuli for immune activation experienced in RLS could also potentially increase viral replication, further exposing the limitations for complete viral control on boosted PI monotherapy.
The long-term success of LPV/r monotherapy for any given patient is difficult to predict and precludes guideline recommendation of PI monotherapy as second-line treatment. However, there will be patients in need of second-line therapy who are intolerant to NRTIs, resistant to all NNRTIs and without access to integrase inhibitors. Moreover, boosted PI monotherapy has consistently been demonstrated to be a cost-effective treatment strategy compared to triple therapy, 33 –35 a key consideration for RLS. All studies, including ours, point to a reasonable expectation that LPV/r monotherapy would be effective in some patients. We found that detectable VLs at 12 and 24 weeks were strongly indicative of treatment failure at 48 weeks. Patients who had detectable VL at 12 weeks were 8.75 times more likely to fail at 48 weeks (P = .01) and all patients who had a detectable VL at 24 weeks would go on to fail by ITT protocol. These VL milestones offer a clinically useful tool: a VL can be checked 6 months after starting LPV/r monotherapy, and if VL is detectable >400 copies, there may not be utility in continuing treatment without intensification.
Other factors predictive of ITT success were female gender and treatment at Plateau State Hospital, whereas ITT failure was associated with prior EFV treatment. The association with EFV treatment likely represents confounding with male gender, as EFV was not prescribed to women of childbearing age; EFV could also be associated with prior history of TB treatment. The difference in boosted PI monotherapy success by gender is interesting and to our knowledge has not been described previously. This may represent a difference in adherence, though to date there is conflicting evidence as whether adherence differs by gender. 36 –38 Of note, in our study, initial VL and CD4 count did not predict treatment success nor did historic CD4 nadir or self-reported adherence. In other studies of boosted PI monotherapy, such factors were correlated with treatment outcomes. 10,13,16,18,21,22,27,39 –42
The primary weakness of this trial is the small sample size. The trial was halted early, and only half of the estimated needed participants were recruited. The frequency of VL monitoring, while a key strength of this study, is also one of its major weaknesses. Such frequent monitoring is neither representative of clinical practice nor of clinical treatment trials. Had we pursued less frequent VL monitoring we likely would have had rates of failure similar to other studies.
In conclusion, low-level viremia is extremely common in patients on LPV/r monotherapy in RLS, with 96% of patients in this study experiencing at least 1 blip. Lopinavir/ritonavir monotherapy may have a role in certain patients but cannot be recommended as second-line therapy in patients without a compelling reason due to a significant risk of low-level viremia and subsequent virologic failure. For clinical purposes, patients who are not virally suppressed by 24 weeks should not continue on LPV/r monotherapy.
Footnotes
Authors’ Note
C.W.C. performed the data analysis, conducted the literature review, and wrote the manuscript. D.K. performed the initial data cleaning and analysis, assisted with the literature review, and helped write the first draft of the manuscript. C.N. provided clinical oversight of the study in Nigeria. A.A. managed the laboratory components of the study in Nigeria, including measurement of plasma HIV RNA concentrations and related analyses. D.S. was the study coordinator and oversaw the daily study operations, patient enrollment, and study monitoring. M.O. provided the overall administrative leadership and programmatic support necessary to conduct the trial in Nigeria. B.G. helped to conceive of and design the study and provided independent review and editing particularly in regard to data interpretation for primary end point. A.A. conceived of and designed the study, developed the study protocol, oversaw the study, supervised the data analysis, assisted in writing the manuscript, and was the overall principal investigator. All authors provided input to the article and approved the final version. The Institutional Review Boards of both University of Maryland and Jos University Teaching Hospital approved the study, as did the ethics committees of the 2 study sites, ECWA Evangel Hospital (now Bingham University Teaching Hospital) and Plateau State Specialist Hospital.
This study was approved by the institutional review board of University of Maryland, Baltimore (study no. HP-00040700), the institutional review board of Jos University Teaching Hospital, and the ethics committees of each of the 2 study sites. The study was also approved as a Food and Drug Administration (FDA) Investigational New Drug (IND) application (approval no. 74,245) and the Nigerian National Agency for Food and Drug Administration and Control (NAFDAC).
All participants provided written informed consent prior to enrolment in the study. Informed consent was provided in both English and Hausa, and oral translation was provided for other languages as needed. In addition, HIV viral loads (VLs) were assessed monthly as required by the FDA IND and NAFDAC.
Acknowledgements
The authors wish to thank Nathan Jensen, PhD, Marie Diener-West, PhD, Colleen Hanrahan, PhD, David Riedel, MD, MPH, and Kristen Stafford, PhD, for their valuable assistance with statistical analysis in this paper. Finally, the authors would like to thank the patients of Jos who participated in the study and all the study staff who helped make it possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The initial funding for the study was provided through an investigator-initiated study grant awarded to AA by Abbott Laboratories. These funds importantly allowed for the employment and training of study personnel, laboratory costs, and international travel for a study auditing team. Abbott Laboratories also supplied and shipped the lopinavir/ritonavir (Alluvia) used in the study. Additional funding to complete the study was provided by the Institute of Human Virology.