
Abstract
There is an urgent need to develop the HIV treatment cascade for men who have sex with men (MSM) and transgender individuals in rural Mpumalanga, South Africa. Mhealth tools such as smartphone applications have the potential to support HIV self-care behaviors. We conducted an exploratory study with HIV-positive community leaders to understand their current uses of cell phones and smartphones and to assess their interest in an HIV research study that utilized a smartphone application for HIV care support. A total of 18 community leaders were recruited to complete a questionnaire and focus group. We found that a large proportion of participants had smartphone access and were interested in a research study that utilized a smartphone application with secure access measures. We conclude that smartphone applications for HIV care research are feasible based on access and interest by MSM and transgender individuals in this rural setting.
Introduction
The HIV treatment cascade is underdeveloped for men who have sex with men (MSM) and transgender individuals in Mpumalanga. 1 The HIV treatment cascade outlines key steps for HIV care retention from HIV testing to linkage to care and treatment adherence that lead to lowered viral load and improve wellness. 2 In Mpumalanga, these steps have low retention for MSM. It is estimated that 16.3% to 20.6% of MSM have undiagnosed HIV infection in this setting, complementing different studies with MSM in other African communities that have shown similar high rates of undiagnosed HIV infection. 3 -5 In this rural setting, 1 in 2 MSM over the age of 25 years are HIV positive with only 18.3% linked to care and 13.6% taking antiretroviral treatment (ART). 3
Although we have good understanding of HIV risk for MSM in African settings, we have limited understanding of HIV risk factors and health-care needs for transgender individuals. 6 -9 In general, there have been few, and only recent, HIV prevention activities with rural MSM and transgender African communities. 10 As a result, most present late to clinic with HIV-related symptoms, and this delay in health-care access is also hindered by a history of MSM and transgender discrimination in the health-care setting. 10 -14 Men who have sex with men and transgender individuals have been designated a key population for HIV prevention in South Africa, which has led to increased testing and programs to improve clinical care. Yet, more research is needed to assess interventions that are designed to improve HIV self-care behaviors and support outside the clinic for these communities in rural settings. 15
Mhealth tools have the potential to support HIV self-care and improve HIV health outcomes for MSM and transgender individuals in African settings. 16,17 There is expanded, low-cost access to mobile technology including smartphones in low-resource settings that provide the potential for mhealth use in HIV self-care. 17,18 Mhealth tools include phone apps, tailored short messaging service (SMS), and online Websites that can be accessed by smartphones. These tools have been shown to improve various chronic conditions and health behaviors including ART adherence among HIV-positive individuals in low-resource settings. 19 -21 Also, mhealth tools have been effective in helping individuals navigate structural and social determinants of health to address individual HIV care and prevention behaviors. 22 However, there remains limited understanding of the feasibility of these mhealth tools for MSM and transgender individuals in African areas and how these tools can be integrated into HIV intervention research.
Therefore, we explored how MSM access and use smartphone technologies in their everyday lives in order to determine whether this technology is feasible for HIV care research interventions with this community in Mpumalanga. Participants outlined their current uses of smartphone technologies and considerations for research with specific implications for participant confidentiality.
Methods
The study utilized a quantitative and qualitative approach. 23 We administered a questionnaire asking participants to outline their uses and interest in smartphone and social networking technology. Afterward, participants completed a focus group to elaborate on their uses of smartphones and social networking technologies. Participants were recruited using a modified snowball sampling method where 4 (n = 2) community leaders were recruited who were asked to recruit an additional 10 (n = 10) community leaders to complete the study procedures. 24 We chose community leaders because they are the gatekeepers of various social networks and would endorse a study within their networks. All the community leaders were HIV positive, isiZulu, or isiSwati, and living in Mpumalanga, South Africa.
The questionnaire included demographic questions such as age, educational attainment, and employment as well as questions about sexuality and gender identity. Participants were asked if they use and own a cell phone or smartphone including how often they use these technologies including social networking technologies. Finally, participants were asked to measure their interest in participating in a study that involved various technologies. Univariate analysis was conducted in Statistics Analysis Software Package (SPSS) to describe general trends of technology use in this group. 25
The focus group discussions (FGDs) were conducted with 2 groups of MSM that lasted 2 hours in length for each. The first FGD had 12 participants, and the second FGD had 6 participants. A semistructured protocol was used that covered the areas: cell phone privacy, smartphone access and use including applications and social networking, considerations for smartphone use in a research study, and interest in regular HIV support groups that integrated smartphone apps. The FGDs were audio recorded, transcribed, and then analyzed using an open coding approach since the use of smartphones in Mpumalanga was relatively new with limited research about smartphone feasibility for HIV interventions in this setting. 26 -28
This study received human participants’ approval by institutional review boards at the University of California Los Angeles in the United States and the University of Witwatersrand in Johannesburg, South Africa. Participants completed written consent after learning about the study and prior to enrollment. In the qualitative data, we use “R” to designate the researcher and “P” to designate a participant.
Results
We present the results of the questionnaire and FGDs with community leaders in Mpumalanga. Leaders lived in 2 districts of Mpumalanga. Twelve leaders lived in Ehlenzeni and 6 lived in Gert Sibande. Among the participants, the average length of time they have been living with HIV is 4.5 years with a range of 1 to 17 years. Tables 1 to 3 show basic classification of the questionnaire responses, and Table 4 outlines the focus group themes.
Demographics.
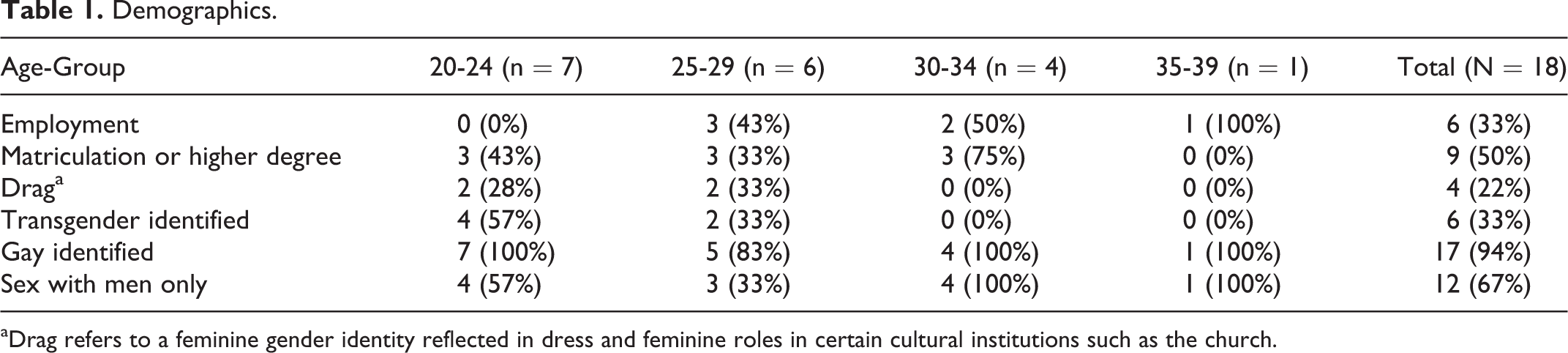
aDrag refers to a feminine gender identity reflected in dress and feminine roles in certain cultural institutions such as the church.
Access to Cell Phones and Social Networking Technology.

Interest in HIV Research Using Smartphone and Social Networking Technology.

Abbreviations: MSM, men who have sex with men; SMS, short messaging service.
Smartphone Use and Feasibility for HIV Care.a

Abbreviations: BMI, body mass index; TB, tuberculosis.
a“R ”designates the researcher and “P” designates a participant.
In Table 1, we outline our demographic findings by age range. Most of the participants were unemployed (67%); all those under the age of 24 years were unemployed. Only half (50%) of the participants had a matriculation degree, and more than one-third (33%) of the participants had sex with only men. Nearly all the participants identified as gay (94%), a small proportion did drag (22%), while some participants identified as transgender (33%). All those who did drag or identified as transgender were limited to 29 years of age or younger. Most of the participants who identified as transgender also identified as gay. Drag identity involves integrating feminine dress into one’s life, either regularly or semiregularly, but it remains a different identity from transgender identity in this setting.
There is considerable access to cell phones among the participants (Table 2). Most participants own their own cell phone (94%), while a high proportion of them have a smartphone (67%). Few share their cell phone with others (22%), and many participants regularly use online social networking, such as Facebook (94%) and WhatsApp (83%).
Participants were asked if they would be willing to use smartphone applications or online social networking technology while enrolled in a research study (Table 3). Most participants were willing to use SMS functions including receiving messages and responding to these within a research study (83% for all), and all participants were willing to use a smartphone application for HIV care and MSM identity support. A lower proportion of participants were interested in sending SMS photos of HIV clinical outcomes (61%) or engaging in an online social networking site for HIV support (56%). Monthly in-person HIV support groups, with SMS reminders to attend these groups, were of interest to 94% of the participants.
Through the FGDs, we outlined 3 main themes that described how participants used their smartphones and the feasibility of using these for research purpose (Table 4). These themes are described next with quotes represented in Table 4.
Sharing and Managing Privacy
Participants described sharing their phones regularly with others including friends and family, but they limited access to other so they don’t see private content such as photos and SMS conversations. Most stated that friends could access their phones and all the phone content, but their partners were not allowed access because, as 1 participant stated, “he will see things he isn’t meant to see and read….” Participants restricted their partner’s access to their phones because the partner may find private photos or conversations with other partners, which would lead to a fight. Furthermore, irrespective of who was using their phone, all participants described watching the person carefully to manage what they saw and used on the phone, and when it came to family, participants with more than 1 phone gave the “saved” phone to their family member. The “saved” phone was a Christianity metaphor, referring to the phone without MSM-related content. However, only 6 participants stated that they had more than 1 phone for this purpose.
Phones Are an Extension Life
Participants valued their phones since these served as a key resource for them socially and economically. They described the phone as an extension of their lives since it allowed them to search for jobs and participate on social networking sites such as Facebook. As 1 participant stated, “we use it [smartphone] to find agents for job hunting purposes….” Most jobs are posted online, and smartphones allowed them to search for positions efficiently. When discussing the possibility of using smartphones to support their HIV health, participants who identified as transgender saw this as an opportunity to reduce the effects of stigma they experience in the clinic. As 1 participant stated, “The files are going to stigmatize us because then I have to take a male file even though I feel like a female.” Transgender participants saw the smartphone as a way of reducing their time in the clinic. If they could manage their HIV disease on a more daily basis and on their own, then they are expected to go to the clinic less often because they would be healthier, which would simultaneously support their transgender identity because they wouldn’t be forced into the wrong gender assignment in the clinic.
HIV Care Smartphone Applications Have Potential
Participants were asked to discuss what they thought of a hypothetical smartphone application for HIV care, and if they would participate in a study that used it. We explained that the initial idea for the smartphone application would be to create a basic tool for people to monitor their ART, clinical measures, and clinical visits, provide them access to general HIV information, and receive SMS reminders about taking their medication. Participants were very interested in such an application. They saw that the application would be especially beneficial to them when they are working and can’t make it to the clinic before closing time. As 1 participant stated, “we wouldn’t have to go far for information,” since they can access the information they needed about their HIV care or receive general HIV information on their smartphone.
However, participants wanted to customize the application with 2 components. First, they wanted the application to be password protected, so they could still share their phone with others. Second, they wanted the application to have more than just HIV care information but include other general wellness information. They discussed that the application could include the capacity to monitor their body mass index or other clinical conditions such as tuberculosis treatment and diabetes care. This second component was intended, in part, to prevent unexpected HIV status disclosures to others. However, participants did discuss wellness in reference to their HIV care, which suggests they want this application to do more than monitor HIV but also help them manage their health in general.
Discussion
This exploratory study was conducted to understand the uses of smartphones and the feasibility of using this technology in an HIV research study with MSM and transgender individuals in rural Mpumalanga, South Africa. 8,9 We recruited community leaders to complete a questionnaire and participate in an FGD to elaborate on the role of smartphones in their lives and research. The community leaders included a diverse group of individuals representing younger and older age ranges for this setting, and it included those who identified as transgender. To our knowledge, this is the first time HIV-positive transgender individuals openly discussed their health needs in a qualitative study in Mpumalanga, and this necessitates the need for additional research with this group especially with regard to HIV prevention. 8,9
For the primary purposes of this study, we found that cell phones and smartphones are used daily by both MSM and transgender individuals in this setting. This finding correlates with other studies that show increased smartphone access and use in African communities. 17,20 Participants described their smartphones as a necessary tool in order to access information for all aspects of their lives from social networking to jobs to celebrity gossip and indicated having their smartphones with them throughout the day and evening. Most owned their phones, and these findings suggest high rates of smartphone access to support feasibility.
Also, we found that participants were interested in participating in a study that used an HIV care smartphone application, but this interest was based on a few conditions to support their confidentiality around their HIV-positive status, which aligns with mhealth research ethics. 18,29 Although most participants responded in the questionnaire that they didn’t share their phones, one of the main themes from the FGDs was that participants did, in fact, share their phones with many different people including family, friends, and partners. Similarly, they provided detailed examples of this sharing and how they managed others when they used their phone, which suggests that the focus group responses were a more accurate description of phone sharing in this setting. Even though they shared their phones, they were interested in participating in a study that used a smartphone application, if the application was password protected and included other wellness measures like diabetes self-care. Since participants shared their phones and content, they wanted the application to be secured to limit access. Their suggestion to add other health content to the application was based on the idea that they believed it would allow them to hide the HIV content while also supporting their general wellness. We concluded that an HIV care smartphone application was feasible for a research study based on interest in this community.
Limitations
We didn’t discuss smartphone costs with participants. Most of the participants had a smartphone, yet few had regular employment. More research is needed to understand how participants maintain the cost of their smartphones while unemployed and how this may have implications for HIV care and intervention development.
Conclusion
HIV prevention for rural-living MSM is expanding and should now consider and investigate the specific needs for transgender individuals as well. Also, given the high HIV prevalence rate in Mpumalanga, it is critical that the HIV treatment cascade is addressed for MSM and transgender individuals. The treatment cascade is dependent not only on trained health-care professionals but on an individual’s ability to self-manage their HIV health; and mhealth tools, like smartphone applications, are feasible for research and may be assessed in order to understand the effectiveness of these for HIV care in this setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Center for HIV Identification, Prevention, and Treatment National Institutes of Mental Health grant MH58107, UCLA Center for AIDS Research grant 5P30AI028697, and the T32 Post-Doctoral Training Program in Global HIV/AIDS Prevention at UCLA T32MH080634.