
Abstract
Background:
With the wide usage of highly active antiretroviral therapy, the morbidity and mortality due to HIV have declined gradually. The aim of our study was to determine the cause of mortality among HIV-infected patients and the factors causing early death.
Methods:
Using medical records of 73 inpatients who are dead, data were collected and analyzed using SPSS version 19 (IBM SPSS Statistics). Chi-square test was performed to determine the factors contributing to early death. A P value <.05 was considered significant.
Results:
Among 73 deaths, 50 (68.5%) were AIDS related and 23 (31.5%) were non-AIDS related. The most common opportunistic infection causing death was Pneumocystis carinii pneumonia. Early deaths were strongly attributed to low CD4 counts at admission (<100 cells), antiretroviral therapy-naive status, late presentation, and fewer admissions (P value <.05).
Conclusion:
Although AIDS-defining illness remains the main cause of death in HIV, there is significant number of deaths due to non–HIV-related causes.
Introduction
HIV has emerged as a global pandemic since 1981. In the early era, it was considered as a deadly illness. With the discovery of highly active antiretroviral therapy (HAART), HIV has become a manageable chronic illness. 1 Studies have shown that adherence to antiretroviral therapy (ART) has not only improved life expectancy of patients but also helped to reduce the incidence of comorbidities in HIV-infected patients. 2 –5
Many research that were carried out in the past has shown that the main cause of death among HIV-infected patients are attributed to AIDS-defining illnesses. 6 –8 But, after the wide usage of HAART globally, the incidence of opportunistic infections and malignancies associated with AIDS has gradually declined and so the mortality rate.
However, as HIV-infected patients live longer with less risks of acquiring AIDS-defining illnesses, the cause of death is believed to show a changing trend. The incidence of non–AIDS-defining illnesses and cardiometabolic diseases has been reported to increase in HIV-infected patients. A similar study across Europe observed that the proportion of deaths following HIV-related disease decreased by 25% annually, while there was an increment of 32% yearly in the proportion of deaths due to non HIV-related disease. 9 Therefore, meticulous study on the cause of death among HIV-infected patients is of great importance to understand the changing pattern of mortality. This study will be useful in future to prioritize measures in the prevention and management of comorbidities in HIV infection.
India has 2.1 million people living with HIV (PLHIV), by the year 2015. Of this, Karnataka is the state with third highest PLHIV. The annual death rates in Karnataka has been reported to decline by 7% to 81% from year 2007 to 2015. This decline is consistent with the dramatic expansion of ART centers in the country. 10 Many studies have been conducted in India regarding HIV, but not many has spoken about the causes of mortality in HIV. This study is the first of its kind dealing in detail with this aspect.
Materials and Methods
Research protocol was submitted to Institutional Ethical Committee, Kasturba Medical College, Mangalore, and ethical clearance was obtained.
Study Setting, Design, and Population
A hospital-based retrospective study was carried out in Kasturba Medical College Hospital. Kasturba Medical College Hospital is a tertiary-care center that has been actively treating HIV-infected patients since 1998. It has an ART centre to provide medical care, counseling, and drugs to patients from all over Karnataka state and also receive referral cases from the neighboring states. All the 73 HIV-infected patients who died in the hospital between years 2010 and 2016 were included in our study.
Definitions
Highly active antiretroviral therapy was defined as the use of 3 full-dose antiretroviral drugs. AIDS-defining illness was defined as death attributable to a category C disease listed by the Centers for Disease Control and Prevention and death due to an HIV-associated disease defined as an immunodeficiency-related disease (eg, bacterial pneumonia caused by Streptococcus pneumoniae, chronic diarrhea). A cause of death not attributable to an AIDS-defining or HIV-related illness was characterized as “non-HIV related” (eg, trauma, suicide, and liver disease). 11 Treatment failure definition used in this study is according to World Health Organization (WHO) definitions and is divided into 3 subtypes: (1) Clinical failure is defined as the appearance or reappearance of WHO clinical stage III or stage IV events after 24 weeks on ART. (2) Immunological failure is when after 24 weeks on ART the CD4 count falls to the pretherapy baseline, falls to 50% from the peak treatment value, or the CD4 count is persistently below 100 cells/mm3. (3) Virological failure is when plasma viral load >5000 after 24 weeks on ART.
Data Collection and Analysis
After obtaining permission from medical records department of the hospital, medical records of patients who died, death certificates, and laboratory data were collected. Utmost care was taken to maintain anonymity and confidentiality of information taken. Data were collected using a proforma consisting of demographic details, clinical history, admission records, laboratory parameters, and death information. All the data were presented as proportions and analyzed using SPSS version 19 (IBM SPSS Statistics). Chi-square test was done for factors contributing to early deaths among HIV-infected patients. A P value <.05 is considered as statistically significant.
Results
A total number of 872 PLHIV were registered under the study hospital from year 2010 to 2016, and 73 in-hospital deaths were reported during this duration. When analyzing annual deaths, we did not obtain a steady declining pattern. However, annual deaths have decreased from 13 to 6 (by 53.8%) from year 2015 to 2016.
The total of 73 deaths that occurred in the hospital between the year 2010 and 2016 was included in this study. Table 1 shows the baseline characteristics of the study populations; 45 (61.64%) were males and 28 (38.36%) were females. The majority (54.79%) of deaths were from age-group of 41 to 60 years, followed by the age group of 20 to 40 years (39.73%), and only 5.5% of the deaths were attributed to the HIV-infected patients aged older than 60. The mean age at death was 43 ± 9 years. Of 73 patients who died, 48 had received ART, while 25 did not receive ART. The total number of admissions in the hospital following the diagnosis of HIV was also obtained (median admission = 3; interquartile range [IQR]: 1-7): 31.5% of the study population was admitted only once in the hospital; 56.2% of people were admitted between 2 and 10 times; and 12.3% had more than 10 admissions. The last CD4 count prior to death was categorized as 0 to 100 for 35 (48%) patients, 101 to 350 for 25 (34.2%) patients, 351 to 500 for 8 (11%) patients, and more than 500 for a minority of 5 (6.8%) patients. The median CD4 count prior to death was 111 (IQR: 38-281.50); 31.5% presented late to the hospital with advanced disease, and the remaining 68.5% were early presenters.
Baseline Characteristics of HIV-Infected Patients Who Died between the Year 2010 and 2016.a

Abbreviation: ART, antiretroviral therapy.
aN = 73.
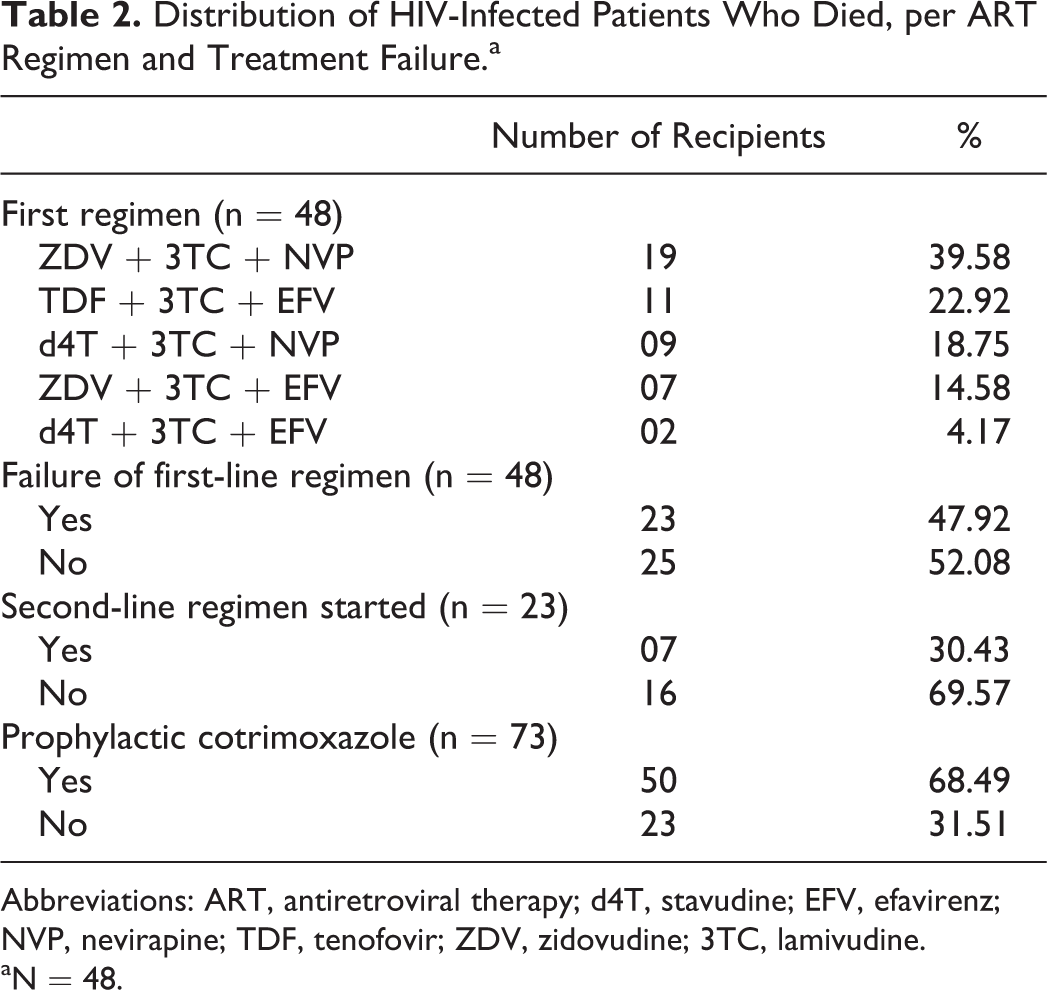
Table 2 shows the ART profile of the patients who died. Among the 73 inpatients who died, only 48 of them had received ART. The most common first-line regimen that was received is ZLN (zidovudine [ZDV] + lamivudine [3TC] + nevirapine [NVP]) combination, which was received by 19 (39.58%) patients. The TLE (tenofovir [TDF] + lamivudine [3TC] + efavirenz [EFV]) combination received by 11 (22.92%) patients is the latest regimen that are also prescribed to newer patients. Per WHO 2006 Global guidelines, 23 (47.92%) reported failure . Only 7 (30.43%) among the first-line regimen failure proceeded to receive the second-line regimen, while 16 (69.6%) did not. Of all the patients who died, 50 (68.49%) received cotrimoxazole as prophylaxis against Pneumocystis carinii pneumonia (PCP) regardless of the ART status.
Distribution of HIV-Infected Patients Who Died, per ART Regimen and Treatment Failure.a
Abbreviations: ART, antiretroviral therapy; d4T, stavudine; EFV, efavirenz; NVP, nevirapine; TDF, tenofovir; ZDV, zidovudine; 3TC, lamivudine.
aN = 48.
The causes of death were certain in all 73 (shown in Table 3). These data were obtained from the death certificate and confirmed by clinical and laboratory findings. Most of the deaths (50 [68.49%]) were attributed to AIDS-defining illnesses consisting mostly of various opportunistic infections attributed to AIDS.
Causes of Death among the Study Population Who Died.a

aN = 73.
bSingle cases of acute intestinal obstruction leading to circulatory failure and pulmonary embolism.
Table 4 shows all the individual causes in AIDS-related deaths. Among them, PCP remains as the most common cause of mortality as demonstrated by several previous studies and literatures. Of the 73 (23.3%) patients, 17 died due to PCP causing respiratory failure, despite taking prophylactic medications such as cotrimoxazole. Other important AIDS-defining illness were tuberculosis in various forms and pulmonary and extrapulmonary disease that affected 9 (12.3%) deaths followed by central nervous system toxoplasmosis for 7 (9.6%) deaths. Non–Hodgkin lymphoma was the most important AIDS-related malignancy causing death among 5 (6.8%) patients.
Specific Causes of AIDS-Related Deaths.a

Abbreviation: CNS, central nervous system.
an = 50.
Table 5 depicts the non–HIV/AIDS-related deaths. Four deaths are due to antiretroviral drug toxicity. Stavudine (d4T) was the cause of 3 cases, and TDF caused 1 case of proximal renal tubular acidosis with Fanconi syndrome. Four other deaths caused by cardiovascular diseases was due to acute coronary syndrome and acute pulmonary edema. Three patients died due to liver cirrhosis, of which 2 cases were Hepatitis B virus surface antigen (HBsAg) and Hepatitis C Virus (HCV) positive.
Specific Causes of Non–HIV/AIDS-Related Deaths.a

an = 23.
Important laboratory parameters of the patients who died are revealed in Table 6. Most of the patients had anemia (mean value = 10.0 g/dL) during the last hospital admission. Hyponatremia was seen in 53.4% of patients. In terms of potassium, most patients were within the normal range. Random blood sugar was normal in most of them (72.6%), and only 19.2% had hypoglycemia. Erythrocyte sedimentation rate was markedly elevated in most patients. Many patients (35.6%) showed leukocytosis, explaining acute infection and sepsis in late stages.
Important Laboratory Parameters during the Last Admission Prior to Death.a

Abbreviation: ESR, erythrocyte sedimentation rate.
an = 73.
We compared the several variables and the time to death of HIV-infected patients to identify the factors contributing to early death (shown in Table 7). Early death was defined as death that occurred within the same year of diagnosis, which accounted for 29 patients. CD4 count of patients who died early fell below 350 cells/cu3, and only 1 was above 350 cells/cu3 among them (P value = .009). Nineteen patients died early due to late presentation. We also found that these patients presented in stage 4 AIDS with multiple opportunistic infections. Early presenters (around 40 of them) survived longer, and the data were highly significant (P value ≤ .001). Of all the early deaths, 19 (65.5%) had only single admission in the hospital; probably they presented late with stage 4 disease. Late deaths (40 of them) had more hospital admissions. Among those who died early, only 11 patients received ART, while 37 patients who received ART died later.
Factors Contributing to Early Mortality among HIV-Infected Individuals.

Discussion
Our study included 73 deaths that occurred during the span of 7 years (2010-2016). AIDS-defining illness remains the main cause of mortality among HIV-infected individuals, accounting for 68.5% of the deaths. Among AIDS-defining illness, the major cause of death was found to be PCP (22%). This is in concordance with the studies done by Jain et al 12 and Gill et al, 13 where PCP has been reported to be the leading cause of death. Despite administration of prophylactic medication against PCP as soon as HIV diagnosis is made, many patients still acquired this infection. Following PCP, tuberculosis is the second most common opportunistic infection causing death (12.3%), while toxoplasmosis contributes to about 9.6% deaths. AIDS-related malignancy happened to cause 9.6% deaths, where non–Hodgkin lymphoma is identified as the most common cause.
Twenty-three (31.5%) patients in this study died due to non–AIDS-defining illness. Among the various causes, 4 deaths are related to cardiovascular diseases that were identified to be acute pulmonary edema secondary to left ventricular failure, hypertrophic obstructive cardiomyopathy, and acute myocardial infarction. Another 4 (5.48%) deaths were due to drug toxicity caused by d4T leading to lactic acidosis. Lewden et al 6 in a similar study involving 964 deaths among 185 participating wards stated that 7% of deaths were attributed to cardiovascular diseases and 1% of the death was due to ART-induced lactic acidosis.
The number of deaths reduced by 62.5% in 2016 compared to 2010. But there is no obvious declining trend in the annual number of deaths as shown by Krentz et al. 14
Ghate et al 15 observed that older age, lower CD4 counts at baseline, presence of tuberculosis at any study time point, and ART-naive status were highly associated with mortality. In our observation, we found factors causing early death in HIV. Low CD4 counts (<100 cells), ART-naive status, late presentation, and fewer admissions significantly contributed to early deaths. This has clearly shown us that ART contributes to better prognosis and longer survival of the patients. Patients who present early to the hospital have higher chance of receiving thorough investigations to reveal underlying opportunistic infections and other comorbidities allowing prompt treatment to be initiated at the earliest.
The prognosis of HIV in India is still worse compared to Western countries despite all the same measures taken to curb the disease progress. This is mainly because of the social stigma and poor health-seeking behavior among HIV-infected patients. Despite having multiple ART centers that offer counseling and free treatment, patients still default the treatment and reappear to us with advanced disease. This study clearly shows patients who present to us early, start ART at the earliest, and come for regular follow-ups have a better longevity. It also indirectly enlightens us that the usage of HAART improves survival rate and improves immunity among these patients.
Our study has some limitations. The number of deaths that occurred in the hospital is only the tip of the iceberg. Many deaths that occurred at home were not reported to the hospital. Some patients who were initially regular in checkups abscond during the critical stage of their illness. Also, the adherence of these patients could not be captured. Our results are not generalizable to the deaths of HIV-infected patients.
Conclusion
Patients should be educated, and more awareness creating initiatives should be conducted in order to reduce early deaths among HIV-infected patients. All patients should be held within the health care system to follow up and monitor them regularly. Early deaths can be surely avoided with cooperation from both patients and health care system to establish early diagnosis, regular follow-ups, and adequate measures to prevent and treat opportunistic infections.
Footnotes
Acknowledgement
The authors would like to thank Dr. TMA Pai Endowment Chair in HIV and Opportunistic infections.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.