
Abstract
The duration of macrocytosis after stopping zidovudine (ZDV) is unknown. Among 104 HIV-infected patients treated with ZDV for more than 1 year, 84 patients had macrocytosis at ZDV discontinuation. The median mean corpuscular volume (MCV) was 114.6 fL (range 100-128 fL). Patients were divided into 2 groups: those who did (resolved macrocytosis, n = 36) and did not (persistent macrocytosis, n = 48) normalize MCV at 3 to 6 months after ZDV discontinuation. Alcohol use (P = .02), smoking (P = .03), and lower (but within normal range) folic acid levels (P = .05) were related to the persistence of macrocytosis. A persistence of macrocytosis was observed in 57% at 3 to 6 months, 38% at 1 year and 37% at 2 years after ZDV therapy had stopped. Duration of ZDV therapy did not have an effect on the persistence of macrocytosis (P = .73). The median time for the MCV to normalize after stopping ZDV was 12.5 months.
Introduction
Macrocytosis, defined as mean corpuscular volume (MCV) ≥100 fL (normal 79-98 fL), is broadly categorized as megaloblastic (eg, associated with folate or cobalamin deficiency) or normoblastic (eg, associated with alcoholism, liver disease, and certain drugs including zidovudine [ZDV]). 1 Up to 88% of HIV-infected patients treated with ZDV are reported to have macrocytosis. 2,3 Zidovudine, a thymidine analogue nucleoside reverse transcriptase inhibitor, competes with natural deoxynucleoside triphosphates for binding to HIV reverse transcriptase as it converts HIV RNA into DNA. Competition with the latter can result in impaired synthesis of the erythrocyte precursor in the bone marrow, consequently resulting in macrocytosis. 4 The mechanism causing macrocytosis probably involves DNA biosynthetic changes 5 and changes in erythrocyte plasma membrane cholesterol and fatty acid and may be a manifestation of mitochondrial dysfunction. 4,6
Mean corpuscular volume increases by a mean of 3% at week 4 and 14% at 12 weeks after starting ZDV. Mean corpuscular volume can be used as a marker for adherence to ZDV containing therapy. 3 Some HIV-infected patients show persistence of macrocytosis with or without anemia after discontinuation of ZDV. There is limited literature on duration of persistence of macrocytosis after discontinuation of ZDV. This study characterizes the duration of macrocytosis after discontinuation of ZDV.
Methods
This is a retrospective cohort study approved by the University of Kentucky Institutional Review Board. We reviewed the clinical data of HIV-infected patients ≥18 years old obtained from the University of Kentucky clinic, with (1) continuous exposure to ZDV ≥1 year from January 01, 2004, to December 31, 2013, and (2) availability of the clinical laboratory data at least 3 months after discontinuation of ZDV. Zidovudine 300 mg twice daily as a fixed dose was prescribed to patients as Retrovir (GlaxoSmithKline), Combivir (GlaxoSmithKline), or Trizivir (ViiV Healthcare). Mean corpuscular volume and hemoglobin were recorded at the following time lines: 1 year prior to discontinuation, at discontinuation, 3 to 6 months later, and approximately 1 year and 2 years after discontinuation. Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were recorded at 3 to 6 months after discontinuation. Our data also included, if performed, hepatitis B surface antigen, hepatitis C antibody, thyroid-stimulating hormone (TSH), folic acid, vitamin B12 level, venous lactic acid level, and presence of fatty liver by ultrasound or computed tomography scan of abdomen performed at any time during the study period.
The stop date of ZDV was defined as 1 month after the last prescription date or the documented date of the clinic visit when ZDV was stopped. Suppressed viral load was defined as <200 copies/mL. Anemia was defined as hemoglobin <13.5 g/dL in males and <12 g/dL in females. There was no specific criterion for alcohol use or smoking.
Statistical Analysis
For the entire study sample, descriptive statistics were performed. Means, standard deviations, medians, ranges, and interquartile ranges (q1 and q3) were recorded for all continuous variables and frequencies and percentages for all categorical variables. For analysis of the relationships of variables between resolved macrocytosis (RM) group and persistent macrocytosis (PM) group, bivariate analyses were performed using the chi-square test or the Fisher exact test for categorical variables and the Wilcoxon tests for continuous variables. Kaplan-Meier curves were produced to determine median time to normalize macrocytosis, and log-rank tests were used to compare curves. To normalize macrocytosis analysis, participants with PM or those lost to follow up were censored. SAS version 9.4 (SAS Institute) was used for statistical analysis. The level of significance was defined as P < .05 (2 sided) unless otherwise specified.
Results
One hundred and four patients met the abovementioned criteria. The mean age was 46 years (standard deviation = 9.9 years), 83% were male, and 72% were white. The median treatment duration of ZDV was 4.6 years (range, 1-14 years). Eight (8%) patients were on ZDV ≥10 years, 30 (29%) patients between 5 and 10 years, and 66 (63%) patients <5 years. Macrocytosis was present in 81% (n = 84/104) 1 year prior to stopping ZDV and 86% (n = 89/104) at the time of stopping ZDV.
At the Time of ZDV Discontinuation
Among the 104 patients who met the abovementioned criteria, 89 HIV-infected patients had macrocytosis. Of the 89 patients, 5 were excluded in the analysis due to their detectable viral load ≥200 copies/mL with normal MCV at the time of ZDV discontinuation, suggesting noncompliance. Fifty-nine (70%) of 84 patients were switched to tenofovir (TDF)–emtricitaine-based regimens, 21 (25%) to abacavir (ABC)–lamivudine (3TC )-based regimens, 3 patients to nucleoside reverse transcriptase inhibitor (NRTI)-sparing regimens. One patient did not continue HIV medication after stopping ZDV. The mean MCV was 115 fL at the time of ZDV discontinuation, 103 fL at 3 to 6 months, 99 fL at 1 year, and 98 fL at 2 years after ZDV discontinuation.
Among 84 patients with viral load <200 copies/mL after ZDV discontinuation, 57% (48 of 84) had macrocytosis at 3 to 6 months, 38% (31 of 81) at 1 year, and 37% (29 to 79) at 2 years. Of the 44 patients with MCV ≥ 115 fL at the time of stopping ZDV, macrocytosis persisted in 73% (32 of 44) at 3 to 6 months, 45% (20 of 44) at 1 year, and 47% (20 to 43) at 2 years. Of the 40 patients with an MCV <115 fL, macrocytosis persisted in 40% (16 of 40) at 3 to 6 months (P = .003 compared to MCV > 115 fL), 30% (11 of 37) at 1 year (P = 0.15), and 25% (9 of 36) at 2 years after stopping ZDV (P = .048).
The median MCV of 84 HIV-infected patients with macrocytosis at the time of ZDV discontinuation was 114.6 (range 100-128 fL). Of the 84 patients, 16% (n = 14) had anemia, 12% (n = 10) had chronic hepatitis B infection, 8% (n = 7) had chronic hepatitis C infection, and 1 patient had coinfection with chronic hepatitides B and C. In 2 patients, the venous lactic acid levels at the time of ZDV discontinuation were within the normal range. Among 8 patients on ZDV ≥ 10 years, 2 had normal MCV at the time of discontinuation and 6 had normal MCV at 3 to 6 months after ZDV discontinuation.
At 3 to 6 Months after ZDV Discontinuation
Eighty-four virologcially suppressed HIV-infected patients with macrocytosis at the time of ZDV discontinuation were divided into 2 groups, the groups that did (RM, n = 36) and did not (PM, n = 48) normalize their increased MCV at 3 to 6 months. Comparison of the 2 groups is shown in Table 1.
Comparison of Resolved Macrocytosis (RM) Group and Persistent Macrocytosis (PM) Group at 3 to 6 Months after Stopping ZDV.a

Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; SD, standard deviation; TSH, thyroid-stimulating hormone; ZDV, zidovudin.
aN = 84.
HIV-infected patients in the PM group were more likely to use alcohol (50% versus 25%, P = .02), smoke (69% versus 44%, P = .03), and have lower folic acid levels (median = 13.5 versus 18.1, P = .05) compared to the HIV-infected patients in the RM group. The presence of coinfection with hepatitis B, hepatitis C, elevated transaminases (AST > 40 and ALT > 41), a fatty liver, and decreased vitamin B12 levels were not statistically significant between the 2 groups.
At 1 Year and 2 Years after ZDV Discontinuation
At 1-year follow-up after discontinuation of ZDV, macrocytosis persisted in 38% (31 of 81) of enrolled patients, 19% (6 of 31) of those with macrocytosis at 1 year had anemia. Of the patients, 66% (31 of 47) from the PM group had macrocytosis at 1 year, whereas no patient from the RM group had PM at 1 year (P < .001).
At the 2-year follow-up, 37% (29 of 79) of patients had macrocytosis. Seven (24%) of 29 patients had anemia. Of those patients, 55% (26 of 47) with macrocytosis at 3 to 6 months (PM group) had macrocytosis at 2 years after stopping ZDV, whereas 9% (3 of 32) of those who had previously RM (RM group) had macrocytosis at 2 years (P < .0001). Overall, the median time for MCV to normalize was 12.3 months (95% confidence interval: 7.6-14.4; see Figure 1). Time to normalization was longer for smokers compared to nonsmokers (P = .005; Figure 2).

Time to resolution of macrocytosis (normalization); overall median time to resolution was 12.3 months.
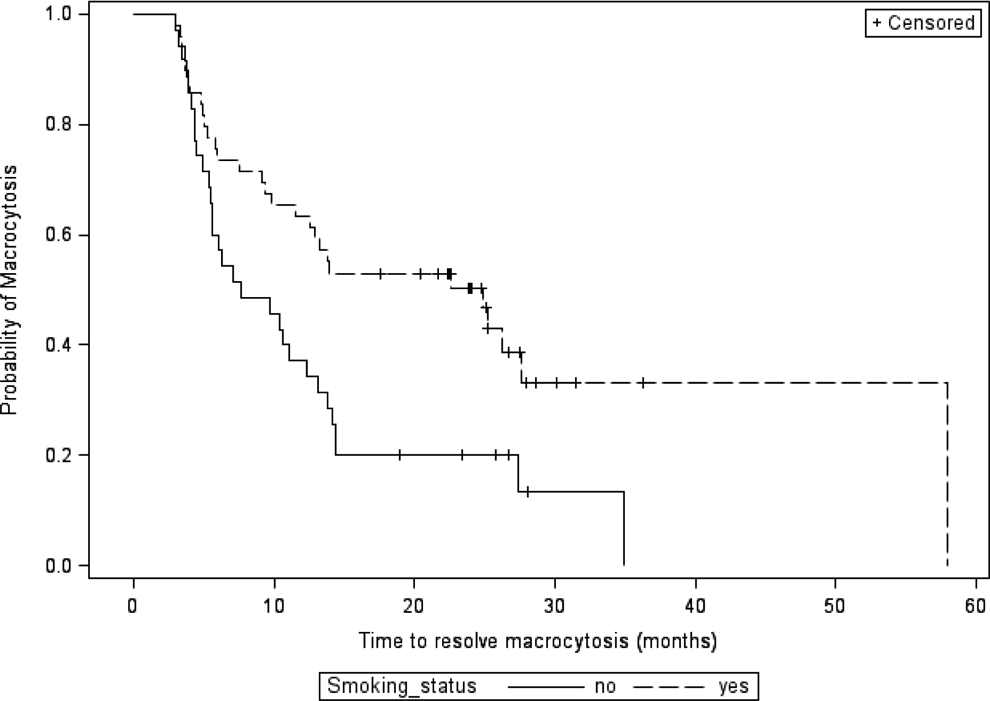
Time to resolution of macrocytosis stratified by smoking status.
Discussion
Zidovudine was initially synthesized as a potential antineoplastic agent in 1964. 7 It was never approved for use in humans as cancer chemotherapy. Zidovudine was used as monotherapy for HIV treatment in the 1980s. 8 It has continued as combination regimens for HIV treatment and in the prevention of perinatal HIV transmission. 9,10 It is still used as a first-line antiretroviral regimen in resource-constrained setting. 10 Apart from macrocytosis and bone marrow toxicity, ZDV can cause lipodystrophy, lactic acidosis, myopathy, and liver toxicity. 9–11 Zidovudine can cause mitochondrial toxicity that can lead to several mitochondrial disorders. It is known that mitochondrial genetic polymorphisms can lead to individual NRTI toxicity. 12 Macrocytosis may be a marker of treatment-related mitochondrial dysfunction in persons on ZDV. 4 Persistent macrocytosis after ZDV treatment may be a marker for the presence of such mitochondrial DNA mutations; as such, it might elicit concern for more severe mitochondrial dysfunction with the use of other NRTIs.
To our knowledge, this is the first study to review the risk factors associated with the persistence of macrocytosis after discontinuation of ZDV.
The median treatment duration of ZDV in our study population was 4.6 years (range, 1-14 years). Macrocytosis was present in 86% (n = 89 of 104) at the time of stopping ZDV. Of the patients, 14% did not develop macrocytosis despite long-term ZDV. The MCV decreased by a mean of 11% at 3 to 6 months, 14% at 1 year, and 15% at 2 years after ZDV discontinuation. The duration of ZDV did not seem to affect the persistence of the macrocytosis (P = .73). Eight patients who were on ZDV ≥ 10 years normalized MCV within 3 to 6 months after stopping ZDV. The patients with an MCV > 115 fL at discontinuation of ZDV were more likely to have PM up to 2 years later. The patients in this cohort were switched from ZDV to different NRTI-based regimens, and these new treatments could have had an unidentified effect on their MCV. Alcohol use, smoking, and lower (but within normal limit) folic acid levels (median 11.1 ng/mL) appeared significant for persistence of macrocytosis. However, there were no patients with folic acid deficiency in the PM group. The duration of ZDV, anemia, smoking, TSH, and vitamin B12 levels, elevated transaminases, and presence of fatty liver were not statistically significant. Five patients with a normal MCV had abnormal TSH levels (2 low and 3 high, normal 0.-4 µIU/mL).
Limitations of this study include the small number of study patients, only a single center, a retrospective study, and a study in which the laboratory data were not obtained at regular intervals. Also there was no quantification for alcohol use, smoking, or bone mineral density testing after ZDV was stopped. Changes in bone density have been suggested a marker for mitochondrial toxicity for those taking an NRTI. 13
In conclusion, we found a PM in 57% of 84 HIV-infected patients at 3 to 6 months, 38% of 81 patients at 1 year, and 37% of 79 patients at 2 years after ZDV therapy had stopped. Duration of ZDV therapy did not appear to have an effect on the persistence of macrocytosis (P = .73). The median time for the MCV to normalize after ceasing ZDV was 12.5 months. The higher the MCV, the longer it took to normalize. Alcohol use, smoking, and lower folic acid levels were related to persistence of macrocytosis. Of the patients, 55% continued to have PM 2 years after stopping ZDV if their MCV did not normalize by 3 to 6 months after discontinuing ZDV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.