
Abstract
We examined the relationship between depression (symptom type, diagnostic severity, and change over time) and adherence to HIV antiretroviral therapy (ART) with data from 3 longitudinal studies (N = 1021) of patients starting ART in Uganda. The Patient Health Questionnaire was used to assess depressive symptoms (total score; somatic and cognitive subscales) and categorize severity level. At baseline, 9% had major depression and 30% had minor depression; 82% were adherent (reported no missed ART doses in the past 7 days) at month 6 and 85% at month 12. Controlling for demographic and medical covariates, multivariate random-effects logistic regression models revealed that change in depression was not related to adherence; however, baseline total depression symptoms and cognitive symptoms in particular as well as major and minor depression were significant predictors of adherence. These findings highlight the need for early identification and aggressive treatment of depression to optimize ART adherence.
Access to lifesaving antiretroviral therapy (ART) has dramatically increased in sub-Saharan Africa (SSA) over the past 10 years. In Uganda alone, over 250 000 people were receiving ART as of 2011. 1 While advancements in ART have resulted in HIV becoming a manageable, chronic disease, its success requires lifelong treatment and high medication adherence. 2 –4 Research suggests that while ART adherence in SSA is generally good, 4 –7 there is evidence that adherence may decline over time 8 similar to what has been observed in the United States. 9 Studies of adherence determinants in SSA have identified structural (eg, drug availability and stock outs, distance to clinic and transportation costs) barriers to adherence, 10,11 but there has been much less investigation into psychosocial determinants of adherence compared to the research conducted in the Western world.
Depression is consistently found to be associated with ART nonadherence, 12 –14 but relatively few studies have examined this relationship in SSA 15 –17 ; even though in SSA, 30% to 50% of people living with HIV have elevated depressive symptoms and 10% to 20% have clinical depression. 17 –20 Most studies, including those in SSA, have examined ART adherence in relation to only global measures of depression (continuous variables representing depressive symptoms assessed by rating scales) or binary indicators of the presence of depression (assessed by a rating scale cutoff criterion or diagnostic interview), rather than specific aspects of depression that may have more or less effect on adherence.
Type of depressive symptom and diagnostic category of depression severity are the 2 aspects of depression that could differentially relate to medication adherence. Cognitive (and affective) depressive symptoms such as low mood and loss of interest can result in loss of motivation for daily activities including pill taking, 21,22 impaired problem solving can negatively affect adherence, 23 and poor concentration can manifest as forgetfulness, which is the most frequently cited reason by patients for missing ART doses. 22,24,25 Somatic symptoms such as sleep disturbance and fatigue can wreak havoc with structured daily routines including dosing regimens, 26 while loss of appetite can make it a challenge to eat the food needed to properly absorb medication and lead to patients skipping doses in an attempt to mitigate side effects intensified by poor dietary intake. Depression rating scales and diagnostic interviews provide a range of diagnostic levels of depression, from mild to moderate to severe depression, and it is possible that more or less severe depression impacts adherence differently. Yet we are unaware of published data that have carefully examined this potentially important distinction. Having a more nuanced understanding of the relationship between depression and adherence can inform how to measure and intervene on depression in order to improve ART adherence.
We have conducted 3 longitudinal studies of clients starting ART in Uganda over the past 5 years. In the analysis reported here, we combined data from these studies to examine self-reported ART adherence during the first year of treatment, and the role of depression as a determinant of adherence. More specifically, we assessed whether the influence of depression varied by depression severity (minor versus major depression) and symptom type (cognitive versus somatic) as well as whether change in depression was related to corresponding changes in adherence. If depression is found to play a role in ART adherence, this research will add to the growing evidence supporting the need for integrating depression treatment into HIV care in SSA.
Methods
Study Design
Data from 3 longitudinal studies were merged for the analysis. Studies A and B enrolled patients just entering HIV care, including those starting ART as well as those not yet eligible for ART, in order to examine the impact of ART on multiple health outcomes. Enrollment for study A was between January and September 2008, while study B enrolled patients from July 2008 to August 2009. Participants in study C had been in HIV care for variable lengths of time and were about to start ART at study enrollment (between January 2010 and February 2011). Study C was designed specifically to examine the role of depression and antidepressant therapy on the socioeconomic outcomes of ART; in addition to depression being assessed at each time point, antidepressants were prescribed to those who were clinically depressed. The analysis for this article included all participants in studies A and B who were starting ART at study baseline, and participants in study C who did not receive antidepressant therapy. Antidepressants were not used to treat depression as part of usual care at the clinics participating in each of the 3 studies. In all 3 studies, participants completed assessments at baseline and months 6 and 12.
Setting
Study A was conducted at 2 HIV clinics operated by Joint Clinical Research Center (JCRC) in Kampala and Kakira (a rural town approximately 100 km outside Kampala). Study B was conducted at 2 HIV clinics in Kampala, 1 operated by Reach Out Mbuya and 1 by Mulago-Mbarara Teaching Hospitals Joint AIDS Program. Study C was conducted at 4 HIV clinics operated by Mildmay Uganda in Kampala and the rural towns of Mityana, Naggalama, and Mukono (between 25 and 100 km outside Kampala). All sites serve clients who are generally in the lower socioeconomic strata. Adherence support mechanisms in place at these clinics as part of the usual care include the provision of ART-orientation training (typically provided over 2-3 clinic visits prior to ART being prescribed), and encouragement and education about adherence and ART provided in group talks and in consultation with providers. At each clinic, patients are routinely asked about any missed doses or adherence problems at each clinic visit.
Sample
Eligibility criteria to be enrolled in studies A and B included being of age 18 years or older, just started receiving care at the clinic, and completed evaluation for ART eligibility. In study C, participants needed to be 18 years of age or older, in care at the clinic for at least 6 months, and just been prescribed ART. In all studies, the primary eligibility criteria for the initiation of ART was having a CD4 count
Measures
All measures were administered in Luganda, the predominant language in this region of Uganda, by trained interviewers. The questionnaire was translated into Luganda using standard translation and back-translation methodology. All measures were administered at each of the 3 assessment time points.
Adherence
After a preamble in which the interviewer normalized nonadherence by indicating it was common for people to have challenges with always taking medication as directed, and emphasized the importance of the study and the clinic understanding the difficulties that people have in taking their medication, participants were asked, “How many doses of your HIV medication did you miss in the past 7 days?” Adherence self-efficacy was assessed by asking the respondent to rate their confidence in being able to “take all of your medication exactly as directed by your doctor” on a scale from 0 (cannot do at all) to 10 (am certain I can do).
Depression
The 9-item Patient Health Questionnaire (PHQ-9) 27 was used to measure the presence of depressive symptoms over the past 2 weeks. The PHQ-9 has been used successfully with HIV-infected individuals in other studies within SSA, 28 and the cross-cultural research of depression in Uganda suggests that convention measures developed in the Western world adequately represent how the illness is locally manifested and conceptualized. 29 Each of the 9 items corresponds to the symptoms used to diagnose depression according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria 30 ; responses to each item range from 0 (not at all) to 3 (nearly every day). Items were summed with a possible range of 0 to 27, with scores <5 representing no depression, 5 to 9 representing “mild” depression, 10 to 14 “moderate,” 15 to 19 “moderately severe,” and 20 to 27 “‘severe” depression. Scores greater than 9 correspond highly to major depression (88% specificity and sensitivity) when compared with a diagnostic clinical interview. 27 For our analysis, scores of 5 to 9 represented “minor depression” and scores greater than 9 represented “major depression.” We also divided the 9 items into 2 subscales, one representing somatic symptoms (4 items: fatigue, difficulty sleeping, poor appetite/overeating, and psychomotor retardation) and other cognitive and affective symptoms (5 items: depressed mood, loss of interest, feeling bad about oneself, trouble concentrating, and suicidal thoughts) to create somatic and cognitive subscales, with each subscale being the sum of the included items.
Demographic and medical characteristics
These included age, gender, education level (classified as a binary indicator of having at least some secondary education), and CD4 count abstracted from the client’s medical chart.
Data Analysis
Adherence data were converted into a dichotomous variable for analysis, representing whether all doses were taken in the past 7 days, because of highly skewed response distributions favoring no missed doses. Bivariate tests (2-tailed independent t tests, χ2 tests, analysis of variance) were used to assess for sample differences across the 3 studies and change in adherence over time (paired t tests and McNemar tests). Multivariate random-effects logistic regression models were used to examine the association between the depression measures and the binary indicator of adherence (whether the respondent reported any missed antiretroviral doses in the past 7 days) measured at months 6 and 12. We assumed a hierarchical structure with multiple assessments nested within participants and with participants nested within their study site. The model specification included a random intercept for each study site and participant to allow for differences in the outcome across sites as well as a different intercept for each participant. This approach produced adjusted standard errors to account for correlations among multiple assessments conducted with each person and due to clustering within study site. To account for dropout between baseline and month 12, we developed attrition weights to adjust or reweight the sample of study completers. To estimate the attrition weights, we used nonlinear generalized boosting models, 31 which required us to specify an inclusive list of baseline variables. All of the random-effects models with weights were fit using a maximum likelihood approach in XTMELOGIT in Stata (Version 12). 32
Model specification
Four models were estimated for adherence, with the goal of examining the potential role of depression in predicting adherence over the 12-month study period. The dependent variable in the models was change in the binary adherence variable from month 6 to month 12. Each model included time (representing the change in adherence from month 6 to month 12) and baseline demographic and medical characteristic covariates (age, gender, any secondary education, and CD4 count) as independent variables. What differed across the models were the depression-related independent variables. The regression effects of depression over time were decomposed into 2 parts: (i) level of depression at baseline and (ii) change in depression from baseline to month 12. The main effect of the baseline measure determined the cross-sectional association between depression at treatment onset and adherence, while the change variable in interaction with time determined whether changes in depression over time are associated prospectively with changes in adherence.
The first model included baseline depressive symptoms (PHQ-9 total score) and the interaction of time and change in depressive symptoms from baseline to month 12; a positive change score indicates a reduction in depressive symptoms, while a negative change score indicates increased symptoms. In order to assess the differential influence of cognitive versus somatic depressive symptoms, the second model replaced the PHQ-9 total score with its somatic and cognitive symptom subscales, both in terms of baseline measures and the change in these measures interacted with time. The third and fourth models assessed whether diagnostic levels of depression severity varied in their association with adherence. The third model included separate baseline indicators of having major depression (PHQ-9 score >9) and minor depression (PHQ-9 score between 5 and 9), and the interaction of time and change in depression symptoms (as measured by PHQ-9 total score and coded as in the first model). The last model included baseline indicators of major and minor depression, and 2 interaction terms for time by categorical improvement in depression severity (with the 3 categories being none, minor, or major depression) and time by worsening of depressive severity category, which separately estimated the change in consistent condom use among those who improved versus those who got worse with respect to depression. These indicators of categorical change in depression severity were binary; an indicator of 1 for improving severity indicated that someone went from major to minor or no depression or from minor to no depression, while an indicator of 1 for worsening severity indicated that someone went from no depression to minor or major depression or from minor to major depression.
Results
Sample Characteristics at Baseline
The merged sample consisted of 1021 participants, 289 from study A, 185 from study B, and 547 from study C. The baseline characteristics of the total sample, as well as by study, are presented in Table 1. The samples drawn from the 3 studies did not differ with regard to mean age and education level; however, study B had a higher proportion of men compared to study A (43.2% versus 32.2%; P = .043), and the mean CD4 count was significantly higher in study C (163) compared to both studies A (133) and B (143; P < .001). Study C had lower levels on each depression measure compared to those in studies A and B, because to clinically depressed patients in study C were given antidepressant therapy and as a result were excluded from this analysis. Overall retention at month 12 was 88.1%; retention was higher in study A (97.2%) compared to both study B (84.9%) and study C (84.3%; P < .001).
Baseline Characteristics of Total Sample and by Study.

Abbreviations: IQR, interquartile range; PHQ-9, The 9-item Patient Health Questionnaire.
a P < .05.
b P < .01.
c P< .001.
Depression
Mean PHQ-9 at baseline was 4.11 (standard deviation = 3.92), with 8.9% having major depression (scored >9 on PHQ-9) and 29.1% having minor depression (scored between 5 and 9 on PHQ-9). Depression declined dramatically over the course of 12 months of ART. Mean PHQ-9 total score declined from 4.18 at baseline to 0.81 at month 12 (P < .001), rates of major depression declined from 9.0% at baseline to 1.4% at month 12 (P < .001), and rates of minor depression dropped from 30.3% at baseline to just 2.9% at month 12 (P < .001), among the 899 participants with data at both assessments.
Adherence
All participants were on nonnucleoside reverse transcriptase inhibitor (NNRTI)-based ART regimens during the course of the study, with efavirenz (EFV) or nevirapine (NVP) being the most commonly prescribed NNRTI; 94.5% were prescribed regimens that called for antiretroviral medications to be taken twice daily. Of the 950 participants who completed the month 6 assessment, 82.8% reported no missed doses in the past 7 days. Similarly, at month 12, 84.0% of the 899 respondents reported no missed doses in the past 7 days. Within-respondent comparisons revealed rather stable adherence; among the 811 participants with adherence data at both months 6 and 12, 79.3% were either adherent (no missed doses; 73.0%) or nonadherent (6.3%) at both assessments, while 9.0% were adherent at month 6 but not month 12, and 11.7% were adherent at month 12 but not month 6.
Relationship between Depression and Adherence
In bivariate comparisons, participants who reported being adherent (no missed doses) at both months 6 and 12 had lower depressive symptoms (PHQ-9 total score) at baseline (mean = 3.58) than those who had reported nonadherence at either assessment (mean = 5.32; P < .001) as well as lower rates of major depression (5.9% versus 15.2%; P < .001) and minor depression (27.2% versus 36.0%; P = .007). These group differences generally remained with regard to depression measures at month 6, with those who reported being adherent at both assessments having lower depressive symptoms (1.66 versus 2.17; P = .048) and lower rates of major depression (1.7% versus 5.8%; P = .002), but there was no difference with regard to minor depression (10.8% versus 8.4%; P = .310). The 2 groups did not differ significantly with regard to any of the month 12 depression measures. This pattern of results was similar when examining the depression correlates of adherence at months 6 and 12 separately.
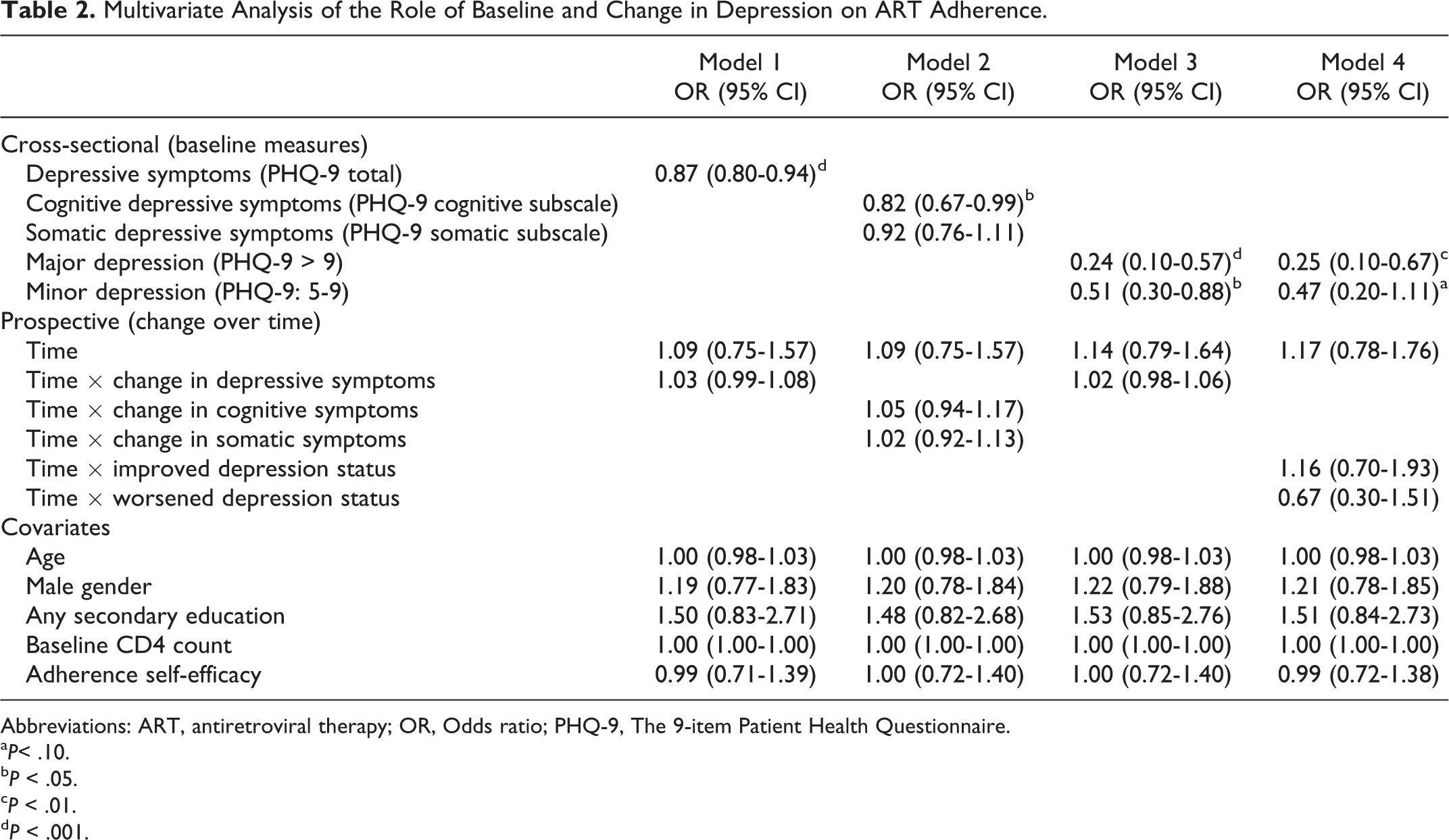
In the multivariate models (see Table 2), the time coefficient was not significantly related to adherence in any of the models, indicating that adherence remained stable from month 6 to month 12. The interactions of time with measures of depression were also not significantly related to adherence. However, each model did reveal baseline measures of depression to be predictive of adherence levels across months 6 and 12. In model 1, baseline depression as measured by the PHQ-9 total score was significantly associated with adherence, with each unit increase in depression associated with a 13% reduction in the odds of adherence. Model 2 revealed that cognitive depressive symptoms at baseline were predictive of adherence but not somatic depressive symptoms; each unit increase in cognitive depressive symptoms was associated with an 18% reduction in the odds of adherence. Major depression was predictive of nonadherence in both models 3 and 4, as it was associated with 76% and 75% lower odds of adherence in these models, respectively. Minor depression was a significant predictor of nonadherence in model 3, in which it was associated with a 49% reduction in the odds of adherence, but in model 4 it was only marginally associated with adherence. None of the baseline covariates predicted adherence.
Multivariate Analysis of the Role of Baseline and Change in Depression on ART Adherence.
Abbreviations: ART, antiretroviral therapy; OR, Odds ratio; PHQ-9, The 9-item Patient Health Questionnaire.
a P< .10.
b P < .05.
c P < .01.
d P < .001.
Discussion
This study is one of the few to examine the relationship between depression and ART adherence using measures that go beyond global depression to include symptom type and categorical severity, in a large, longitudinal sample in SSA. Like other studies, our data show that a global measure of depression is associated with lower adherence, 12 –17 but our findings also suggest that cognitive depressive symptoms at the start of ART are predictive of adherence, unlike somatic symptoms and that moderate to severe forms of depression (as represented by major depression in our study) impede adherence somewhat more so than milder forms of depression (minor depression).
Our finding that cognitive depressive symptoms (eg, depressed mood and loss of interest in activities that normally are pleasurable), not somatic symptoms, predict adherence suggests that pill-taking behavior and decisions may be more influenced by emotional and cognitive processes—how people think and feel emotionally, as opposed to physical symptoms that one may experience. Indeed, studies have shown that cognitive behavioral interventions that target maladaptive attitudes and beliefs regarding HIV treatment and adherence can be effective in improving ART adherence. 33 The absence of a relationship between somatic depressive symptoms (eg, poor appetite, insomnia, fatigue) and adherence may relate to the overlap of these symptoms with those of medical illness and which are common among people living with HIV 34 ; therefore, the presence of such symptoms may be due to HIV or antiretroviral side effects and thus relate to adherence less robustly than cognitive symptoms of depression.
Perhaps as expected, the presence of major depression was more strongly predictive of nonadherence compared to minor depression, but our data provide evidence that the latter is also associated with lapses in adherence. These findings suggest that adherence is negatively affected not only when depressive symptoms become relatively severe and presumably disruptive to overall functioning, rather even milder forms of depression may adversely affect pill-taking behavior, suggesting the need for frequent screening of depression and aggressive, early intervention. Routine screening of depression can be implemented with little need for limited clinic resources as several self-administered depression measures have been validated and successfully used with HIV-positive patients. 28,35
With evidence of depression at the outset of HIV treatment being predictive of ART adherence during the first year of treatment, one would expect that changes in depression, whether it be an increase or decrease, would correspond to a like change in adherence. Yet we found no relationship between change in depression and change in ART adherence during the first year of treatment. A possible explanation for this negative finding may be related to the restricted range of depression and adherence found in our sample; relatively few participants had moderate to severe depression at baseline, depression levels became markedly lower at months 6 and 12 as patients went on ART and very few remained or became depressed, and adherence levels were highly stable. Despite the absence of a relationship between change in depression and adherence in our data, other studies have documented such a relationship. 36 Also, a number of studies have found depression treatment to result in improved ART adherence, 37 –39 although not all. 40 It would be informative to know whether adherence benefits of depression treatment accrue even more among patients who had more severe depression. Furthermore, while depression is commonly thought of as an antecedent to nonadherence, the relationship between depression and adherence may be bidirectional, as poor adherence and associated effects on physical health may increase the risk for depression. 41 Studies evaluating adherence interventions should examine whether improved adherence has beneficial effects on depression and psychological well-being.
In addition to a limited range in the severity of depression and nonadherence observed in our sample, a key limitation to our analysis is our reliance on self-report measures of both adherence and depression. Self-report measures of adherence are widely conceded to overestimate actual ART pill-taking behavior 42 ; although the validity of self-reported adherence is substantiated by studies showing a significant relationship between such measures and virological suppression, 43 objective measures of adherence (eg, electronic monitoring) have been shown to more strongly correlate with HIV viral load. 42,44 Similarly, the use of a structured diagnostic interview to diagnose depression would have enabled us to better distinguish between mild and major depression; however, the PHQ-9 has been shown to have good criterion validity with regard to major depression 27 and has been used successfully in people living with HIV, in SSA. 28 Also, our analysis and measurement focused solely on unipolar depression and did not include bipolar depression, which may affect adherence differently. HIV viral load assays are not a part of usual care at the study sites because of cost, so we were not able to include this clinical outcome measure in our analysis, which limited our ability to confirm the validity of the self-report measure as well as assess the relationship between adherence and HIV treatment outcome. Finally, our findings are not generalizable to all ART clients, as clients who opt not to participate in research could differ on variables that relate to adherence and therefore affect the relationships we observed.
In conclusion, these findings provide support for the relationship between depression at the outset of ART and poor treatment adherence in the first year of treatment, with cognitive depressive symptoms and more severe levels of depression posing particular challenges to adherence, although minor depression was also associated with nonadherence. Mental health services are largely absent from HIV care programs in Uganda and across SSA, 45 yet our findings, together with evidence in the literature supporting the adherence benefits of depression treatment, suggest that integrating routine screening, early detection, and aggressive treatment of depression into HIV care programs may be important for optimizing treatment adherence and HIV clinical outcomes in this setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: Funding for this research was contributed from grants from the National Institute of Mental Health (1R01MH083568), the National Institute for Child Health and Development (1R24HD056651) and Rockefeller Foundation (HE007).